
Meta-Analysis of the Accuracy of Abbreviated Magnetic Resonance Imaging for Hepatocellular Carcinoma Surveillance: Non-Contrast versus Hepatobiliary Phase-Abbreviated Magnetic Resonance Imaging

 , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Eligible Criteria
2.3. Data Extraction
2.4. Evaluation of Study Quality
2.5. Summary estimates synthesis
3. Results
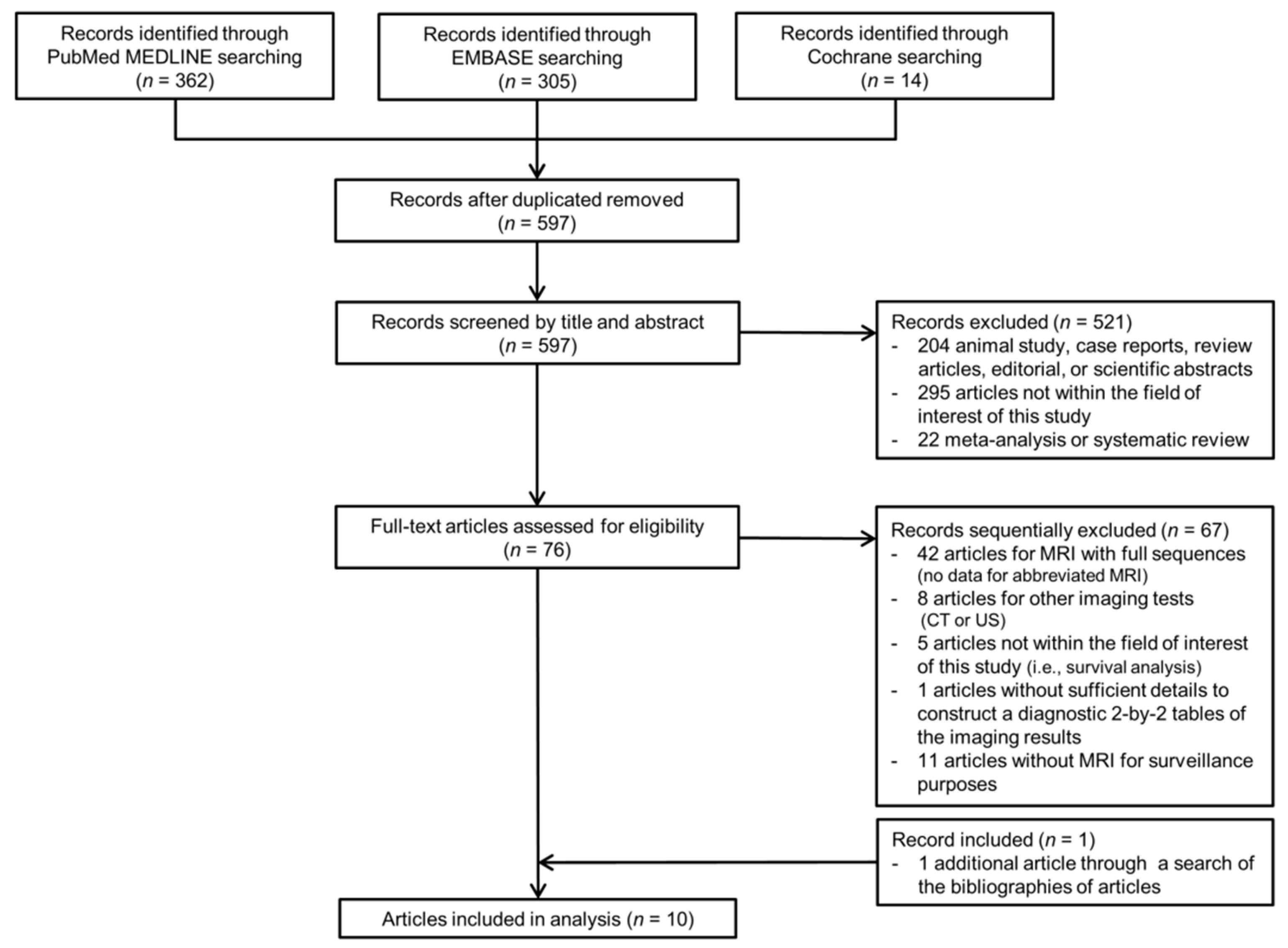
3.1. Literature Search
3.2. Quality Assessment
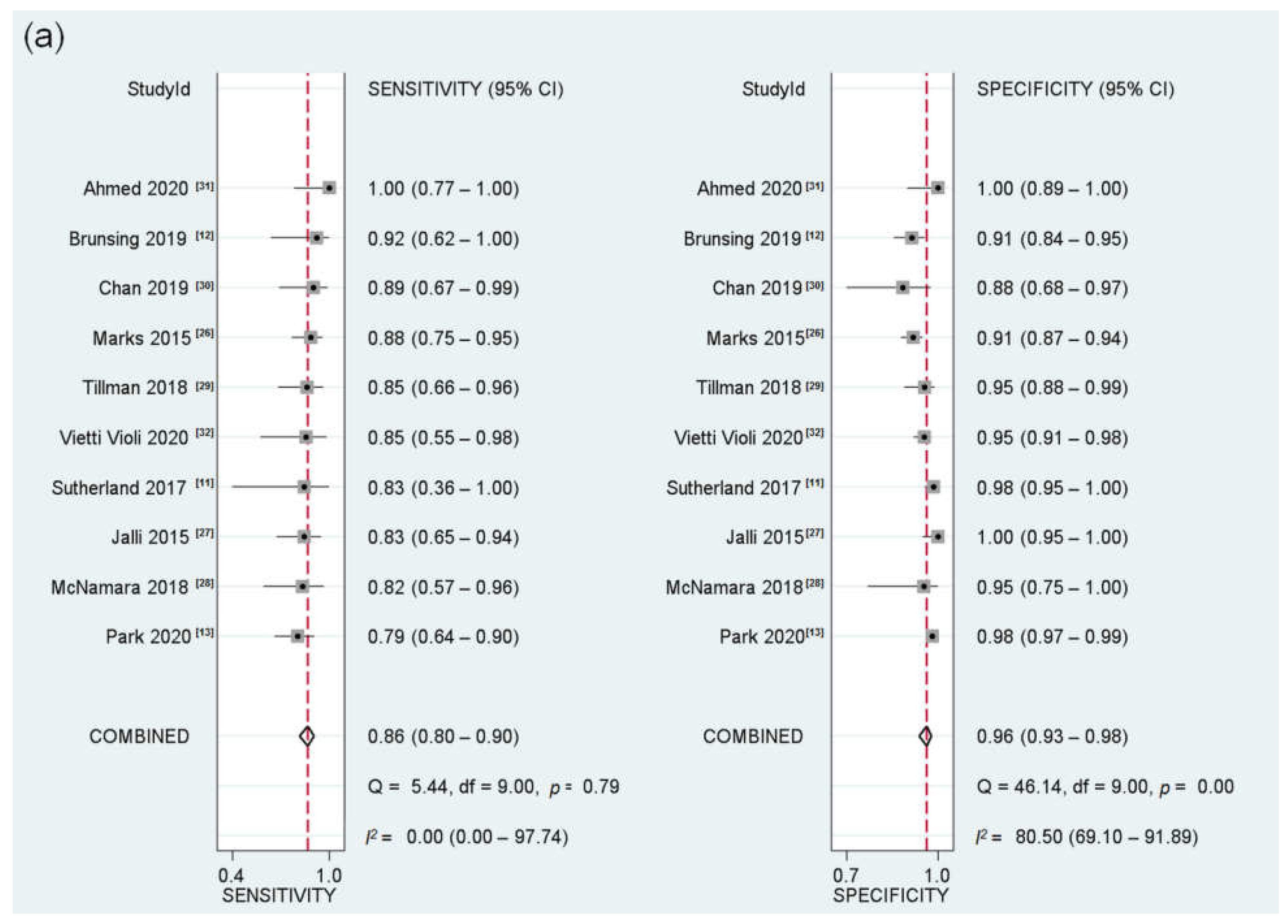
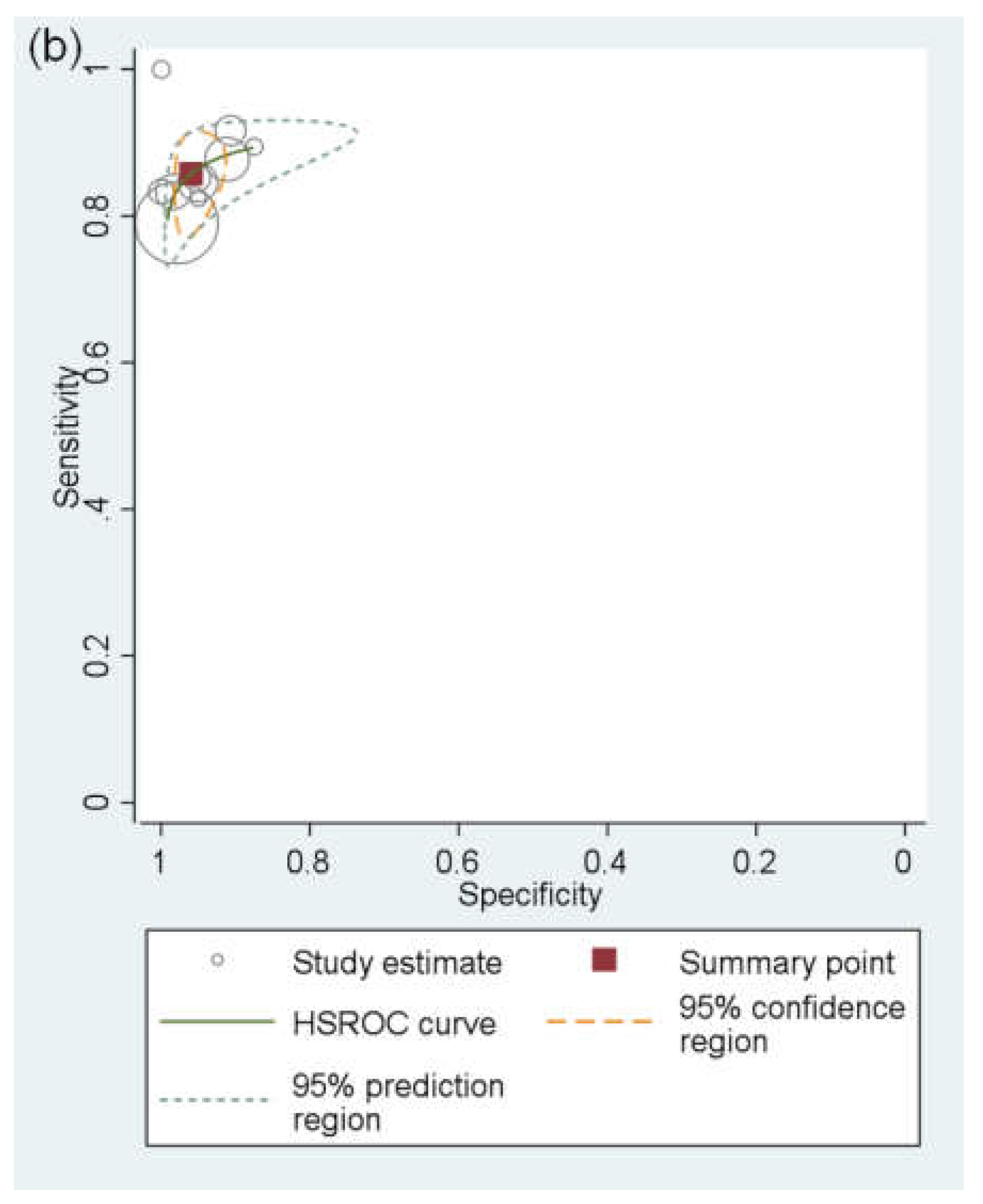
3.3. Performance of AMRI for Detecting HCC
3.4. HBP-AMRI vs. NC-AMRI for Detecting HCC
3.5. Meta-regression Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fujiwara, N.; Friedman, S.L.; Goossens, N.; Hoshida, Y. Risk factors and prevention of hepatocellular carcinoma in the era of precision medicine. J. Hepatol. 2018, 68, 526–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serper, M.; Taddei, T.H.; Mehta, R.; D’Addeo, K.; Dai, F.; Aytaman, A.; Baytarian, M.; Fox, R.; Hunt, K.; Goldberg, D.S.; et al. Association of Provider Specialty and Multidisciplinary Care With Hepatocellular Carcinoma Treatment and Mortality. Gastroenterology 2017, 152, 1954–1964. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, B.H.; Lim, Y.S.; Kim, E.Y.; Kong, H.J.; Won, Y.J.; Han, S.; Park, S.; Hwang, J.S. Temporal improvement in survival of patients with hepatocellular carcinoma in a hepatitis B virus-endemic population. J. Gastroenterol. Hepatol. 2018, 33, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, Staging, and Management of Hepatocellular Carcinoma: 2018 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Management of hepatocellular carcinoma. J. Hepatol. 2018, 69, 182–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Omata, M.; Cheng, A.L.; Kokudo, N.; Kudo, M.; Lee, J.M.; Jia, J.; Tateishi, R.; Han, K.H.; Chawla, Y.K.; Shiina, S.; et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: A 2017 update. Hepatol. Int. 2017, 11, 317–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tzartzeva, K.; Obi, J.; Rich, N.E.; Parikh, N.D.; Marrero, J.A.; Yopp, A.; Waljee, A.K.; Singal, A.G. Surveillance Imaging and Alpha Fetoprotein for Early Detection of Hepatocellular Carcinoma in Patients With Cirrhosis: A Meta-analysis. Gastroenterology 2018, 154, 1706–1718. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.Y.; An, J.; Lim, Y.S.; Han, S.; Lee, J.Y.; Byun, J.H.; Won, H.J.; Lee, S.J.; Lee, H.C.; Lee, Y.S. MRI with Liver-Specific Contrast for Surveillance of Patients with Cirrhosis at High Risk of Hepatocellular Carcinoma. JAMA Oncol. 2017, 3, 456–463. [Google Scholar] [CrossRef]
- Kim, H.L.; An, J.; Park, J.A.; Park, S.H.; Lim, Y.S.; Lee, E.K. Magnetic Resonance Imaging Is Cost-Effective for Hepatocellular Carcinoma Surveillance in High-Risk Patients with Cirrhosis. Hepatology 2019, 69, 1599–1613. [Google Scholar] [CrossRef]
- Sutherland, T.; Watts, J.; Ryan, M.; Galvin, A.; Temple, F.; Vuong, J.; Little, A.F. Diffusion-weighted MRI for hepatocellular carcinoma screening in chronic liver disease: Direct comparison with ultrasound screening. J. Med. Imaging Radiat. Oncol. 2017, 61, 34–39. [Google Scholar] [CrossRef] [Green Version]
- Brunsing, R.L.; Chen, D.H.; Schlein, A.; Wolfson, T.; Gamst, A.; Mamidipalli, A.; Violi, N.V.; Marks, R.M.; Taouli, B.; Loomba, R.; et al. Gadoxetate-enhanced Abbreviated MRI for Hepatocellular Carcinoma Surveillance: Preliminary Experience. Radiol. Imaging Cancer 2019, 1, e190010. [Google Scholar] [CrossRef]
- Park, H.J.; Jang, H.Y.; Kim, S.Y.; Lee, S.J.; Won, H.J.; Byun, J.H.; Choi, S.H.; Lee, S.S.; An, J.; Lim, Y.S. Non-enhanced magnetic resonance imaging as a surveillance tool for hepatocellular carcinoma: Comparison with ultrasound. J. Hepatol. 2020, 72, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Gupta, P.; Soundararajan, R.; Patel, A.; Kumar-M, P.; Sharma, V.; Kalra, N. Abbreviated MRI for hepatocellular carcinoma screening: A systematic review and meta-analysis. J. Hepatol. 2021, in press. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Bru, C.; Bruix, J. Prognosis of hepatocellular carcinoma: The BCLC staging classification. Semin. Liver Dis. 1999, 19, 329–338. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferro, V.; Regalia, E.; Doci, R.; Andreola, S.; Pulvirenti, A.; Bozzetti, F.; Montalto, F.; Ammatuna, M.; Morabito, A.; Gennari, L. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N. Engl. J. Med. 1996, 334, 693–699. [Google Scholar] [CrossRef]
- Kim, Y.K.; Park, H.J.; Park, M.J.; Park, M.J.; Lee, W.J.; Choi, D. Noncontrast MRI with diffusion-weighted imaging as the sole imaging modality for detecting liver malignancy in patients with high risk for hepatocellular carcinoma. Magn. Reson. Imaging 2014, 32, 610–618. [Google Scholar] [CrossRef] [PubMed]
- Besa, C.; Lewis, S.; Pandharipande, P.V.; Chhatwal, J.; Kamath, A.; Cooper, N.; Knight-Greenfield, A.; Babb, J.S.; Boffetta, P.; Padron, N.; et al. Hepatocellular carcinoma detection: Diagnostic performance of a simulated abbreviated MRI protocol combining diffusion-weighted and T1-weighted imaging at the delayed phase post gadoxetic acid. Abdom. Radiol. 2017, 42, 179–190. [Google Scholar] [CrossRef]
- Han, S.; Choi, J.I.; Park, M.Y.; Choi, M.H.; Rha, S.E.; Lee, Y.J. The Diagnostic Performance of Liver MRI without Intravenous Contrast for Detecting Hepatocellular Carcinoma: A Case-Controlled Feasibility Study. Korean J. Radiol. 2018, 19, 568–577. [Google Scholar] [CrossRef]
- Khatri, G.; Pedrosa, I.; Ananthakrishnan, L.; de Leon, A.D.; Fetzer, D.T.; Leyendecker, J.; Singal, A.G.; Xi, Y.; Yopp, A.; Yokoo, T. Abbreviated-protocol screening MRI vs. complete-protocol diagnostic MRI for detection of hepatocellular carcinoma in patients with cirrhosis: An equivalence study using LI-RADS v2018. J. Magn. Reson. Imaging 2020, 51, 415–425. [Google Scholar] [CrossRef]
- Kim, J.S.; Lee, J.K.; Baek, S.Y.; Yun, H.I. Diagnostic performance of a minimized protocol of non-contrast MRI for hepatocellular carcinoma surveillance. Abdom. Radiol. 2020, 45, 211–219. [Google Scholar] [CrossRef]
- Park, S.H.; Kim, B.; Kim, S.Y.; Choi, S.J.; Huh, J.; Kim, H.J.; Kim, K.W.; Lee, S.S. Characterizing Computed Tomography-Detected Arterial Hyperenhancing-Only Lesions in Patients at Risk of Hepatocellular Carcinoma: Can Non-Contrast Magnetic Resonance Imaging Be Used for Sequential Imaging? Korean J. Radiol. 2020, 21, 280–289. [Google Scholar] [CrossRef]
- Whang, S.; Choi, M.H.; Choi, J.I.; Youn, S.Y.; Kim, D.H.; Rha, S.E. Comparison of diagnostic performance of non-contrast MRI and abbreviated MRI using gadoxetic acid in initially diagnosed hepatocellular carcinoma patients: A simulation study of surveillance for hepatocellular carcinomas. Eur. Radiol. 2020, 30, 4150–4163. [Google Scholar] [CrossRef] [PubMed]
- Marks, R.M.; Ryan, A.; Heba, E.R.; Tang, A.; Wolfson, T.J.; Gamst, A.C.; Sirlin, C.B.; Bashir, M.R. Diagnostic per-patient accuracy of an abbreviated hepatobiliary phase gadoxetic acid-enhanced MRI for hepatocellular carcinoma surveillance. AJR Am. J. Roentgenol. 2015, 204, 527–535. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalli, R.; Jafari, S.H.; Sefidbakht, S.; Kazemi, K. Comparison of the Accuracy of DWI and Ultrasonography in Screening Hepatocellular Carcinoma in Patients with Chronic Liver Disease. Iran. J. Radiol. 2015, 12, e12708. [Google Scholar] [CrossRef] [Green Version]
- McNamara, M.M.; Thomas, J.V.; Alexander, L.F.; Little, M.D.; Bolus, D.N.; Li, Y.E.; Morgan, D.E. Diffusion-weighted MRI as a screening tool for hepatocellular carcinoma in cirrhotic livers: Correlation with explant data-a pilot study. Abdom. Radiol. 2018, 43, 2686–2692. [Google Scholar] [CrossRef] [PubMed]
- Tillman, B.G.; Gorman, J.D.; Hru, J.M.; Lee, M.H.; King, M.C.; Sirlin, C.B.; Marks, R.M. Diagnostic per-lesion performance of a simulated gadoxetate disodium-enhanced abbreviated MRI protocol for hepatocellular carcinoma screening. Clin. Radiol. 2018, 73, 485–493. [Google Scholar] [CrossRef]
- Chan, M.V.; McDonald, S.J.; Ong, Y.Y.; Mastrocostas, K.; Ho, E.; Huo, Y.R.; Santhakumar, C.; Lee, A.U.; Yang, J. HCC screening: Assessment of an abbreviated non-contrast MRI protocol. Eur. Radiol. Exp. 2019, 3, 49. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, N.N.A.; El Gaafary, S.M.; Elia, R.Z.; Abdulhafiz, E.M. Role of abbreviated MRI protocol for screening of HCC in HCV related cirrhotic patients prior to direct-acting antiviral treatment. Egypt. J. Radiol. Nucl. Med. 2020, 51, 102. [Google Scholar] [CrossRef]
- Vietti Violi, N.; Lewis, S.; Liao, J.; Hulkower, M.; Hernandez-Meza, G.; Smith, K.; Babb, J.S.; Chin, X.; Song, J.; Said, D.; et al. Gadoxetate-enhanced abbreviated MRI is highly accurate for hepatocellular carcinoma screening. Eur. Radiol. 2020, 30, 6003–6013. [Google Scholar] [CrossRef] [PubMed]
- Goossens, N.; Singal, A.G.; King, L.Y.; Andersson, K.L.; Fuchs, B.C.; Besa, C.; Taouli, B.; Chung, R.T.; Hoshida, Y. Cost-Effectiveness of Risk Score-Stratified Hepatocellular Carcinoma Screening in Patients with Cirrhosis. Clin. Transl. Gastroenterol. 2017, 8, e101. [Google Scholar] [CrossRef]
- Lima, P.H.; Fan, B.; Berube, J.; Cerny, M.; Olivié, D.; Giard, J.M.; Beauchemin, C.; Tang, A. Cost-Utility Analysis of Imaging for Surveillance and Diagnosis of Hepatocellular Carcinoma. AJR Am. J. Roentgenol. 2019, 213, 17–25. [Google Scholar] [CrossRef]
- Brunsing, R.L.; Fowler, K.J.; Yokoo, T.; Cunha, G.M.; Sirlin, C.B.; Marks, R.M. Alternative approach of hepatocellular carcinoma surveillance: Abbreviated MRI. Hepatoma Res. 2020, 6, 59. [Google Scholar] [CrossRef]
- Levine, D.; McDonald, R.J.; Kressel, H.Y. Gadolinium Retention After Contrast-Enhanced MRI. JAMA 2018, 320, 1853–1854. [Google Scholar] [CrossRef]
- Reiter, T.; Ritter, O.; Prince, M.R.; Nordbeck, P.; Wanner, C.; Nagel, E.; Bauer, W.R. Minimizing risk of nephrogenic systemic fibrosis in cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2012, 14, 31. [Google Scholar] [CrossRef] [Green Version]
- Saito, K.; Moriyasu, F.; Sugimoto, K.; Nishio, R.; Saguchi, T.; Akata, S.; Tokuuye, K. Histological grade of differentiation of hepatocellular carcinoma: Comparison of the efficacy of diffusion-weighted MRI with T2-weighted imaging and angiography-assisted CT. J. Med. Imaging Radiat. Oncol. 2012, 56, 261–269. [Google Scholar] [CrossRef]
- Chandarana, H.; Taouli, B. Diffusion and perfusion imaging of the liver. Eur. J. Radiol. 2010, 76, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Cerny, M.; Bergeron, C.; Billiard, J.S.; Murphy-Lavallée, J.; Olivié, D.; Bérubé, J.; Fan, B.; Castel, H.; Turcotte, S.; Perreault, P.; et al. LI-RADS for MR Imaging Diagnosis of Hepatocellular Carcinoma: Performance of Major and Ancillary Features. Radiology 2018, 288, 118–128. [Google Scholar] [CrossRef] [Green Version]
- Kang, J.H.; Choi, S.H.; Byun, J.H.; Kim, D.H.; Lee, S.J.; Kim, S.Y.; Won, H.J.; Shin, Y.M.; Kim, P.N. Ancillary features in the Liver Imaging Reporting and Data System: How to improve diagnosis of hepatocellular carcinoma ≤ 3 cm on magnetic resonance imaging. Eur. Radiol. 2020, 30, 2881–2889. [Google Scholar] [CrossRef] [PubMed]
- Macaskill, P.G.C.; Deeks, J.J.; Harbord, R.M.; Takwoingi, Y. Chapter 10: Analysing and Presenting Results. In Cochrane Handbook for Systematic Reviews of Diagnostic Test Accuracy; Deeks, J.J., Bossuyt, P.M., Gatsonis, C., Eds.; Version 1.0.; The Cochrane Collaboration: London, UK, 2010; Available online: http://srdta.cochrane.org/ (accessed on 29 February 2021).
- Soher, B.J.; Dale, B.M.; Merkle, E.M. A review of MR physics: 3T versus 1.5T. Magn. Reson. Imaging Clin. N. Am. 2007, 15, 277–290. [Google Scholar] [CrossRef] [PubMed]
- Boll, D.T.; Merkle, E.M. Imaging at higher magnetic fields: 3 T versus 1.5 T. Magn. Reson. Imaging Clin. N. Am. 2010, 18, 549–564. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Study Location (Period) | No. of Patients (% Male) | Cirrhosis Patients (% Cirrhosis) | Most Common Underlying Liver Disease (%) | No. of Patients with HCC (%) | % of HCC < 2 cm | Patient Age, Years * | MRI Magnet | MRI Sequences | AMRI Protocol | Reference Standards for HCC (%) | Interpretation of AMRI |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Marks (2015) [26] | Retrospective | United States (2008–2012) | 298 (56.4) | Cirrhosis (NR) or other risk factors for HCC † | Hepatitis C virus (50.7) | 49 (16.4) | 28.6 | 55.9 ± 10.9 | 1.5 or 3.0-T | T2WI, HBP, DWI | HBP-AMRI | Pathology, multiphase CT, or MRI | Simulation |
| Jalli (2015) [27] | Retrospective | Iran (2011–2013) | 96 (NR) | Cirrhosis only (100) | NR | 30 (31.3) | NR | NR | 1.5-T | T2WI, T1 Dual-GRE, DWI | NC-AMRI | Pathology (100) | Simulation |
| Sutherland (2017) [11] | Prospective | Australia (NR) | 192 (72.4) | Cirrhosis (NR) or other risk factors for HCC | Hepatitis B virus (56.3) | 6 (3.1) | 57.1 | 58 (22–80), mean (range) | NR | DWI | NC-AMRI | Pathology, multiphase CT, or MRI | Clinical practice |
| McNamara (2018) [28] | Retrospective | United States (2009–2013) | 37 (67.6) | Cirrhosis only (100) | NR | 17 (45.9) | NR | 21–70, range | 1.5 or 3.0-T | DWI | NC-AMRI | Pathology (100) | Simulation |
| Tillman (2018) [29] | Retrospective | United States (2008–2014) | 79 (53.2) | Cirrhosis (64.6) or other risk factors for HCC | Hepatitis B virus (41.8) | 13 (16.5) | 44.4 | 57.5 ± 13.7 | 1.5 or 3.0-T | T2WI, HBP | HBP-AMRI | Pathology (59.3), multiphase CT, or MRI (40.7) | Simulation |
| Brunsing (2019) [12] | Retrospective | United States (2014–2016) | 141 (54.6) | Cirrhosis (92.9) or other risk factors for HCC | Hepatitis C virus (37.9) | 12 (8.5) | 66.7 | 59.1 ± 11.5 | 1.5 or 3.0-T | T2WI, HBP, DWI | HBP-AMRI | Pathology, multiphase CT, or MRI | Clinical practice |
| Chan (2019) [30] | Retrospective | Australia (2015–2018) | 44 (49.5) | Cirrhosis only (100) | Hepatitis B virus (14.9) | 20 (45.5) | 40.5 | 63 ± 13 | 3.0-T | T2WI, DWI, T1 Dual-GRE | NC-AMRI | Multiphase MRI (100) | Simulation |
| Ahmed (2020) [31] | Prospective | Egypt (2018–2019) | 41 (53.7) | Cirrhosis only (100) | Hepatitis C virus (100) | 10 (24.4) | NR | 53.4 ± 9.2 | 1.5-T | T2WI, DWI | NC-AMRI | Multiphase MRI (100) | NR |
| Park (2020) [13] | Retrospective | Korea (2011–2014) | 382 (56.8) | Cirrhosis only (100) | Hepatitis B virus (72.3) | 43 (11.3) | 83.3 | 56.4, median | 1.5-T | T2WI, DWI | NC-AMRI | Pathology (46.5) or multiphase CT (53.5) | Simulation |
| Vietti Violi (2020) [32] | Retrospective | United States (2017) | 237 (58.6) | Cirrhosis (87.3) or other risk factors for HCC | Hepatitis C virus (25.7) | 13 (5.5) | NR | 58 ± 11.9 | 1.5 or 3.0-T | T2WI, HBP, DWI | HBP-AMRI and NC-AMRI | Pathology (7.7), multiphase CT, or MRI (92.3) | Simulation |
| Any Stage HCC | |||||
| HBP AMRI | NC AMRI | ||||
| Study | Sensitivity (95% CI) | Specificity (95% CI) | First author | Sensitivity (95% CI) | Specificity (95% CI) |
| Marks [26] | 88% (75,95) | 91% (87,94) | Jalli [27] | 83% (65,94) | 100% (95,100) |
| Tillman [29] | 85% (66,96) | 95% (88,99) | Sutherland [11] | 83% (36,100) | 98% (95,100) |
| Brunsing [12] | 92% (62,100) | 91% (84,95) | McNamara [28] | 82% (57,96) | 95% (75,100) |
| Vietti Violi [32] * | 85% (55,98) | 95% (91,98) | Chan [30] | 89% (67,99) | 88% (68,97) |
| Ahmed [31] | 100% (77,100) | 100% (89,100) | |||
| Park [13] | 79% (64,90) | 98% (97,99) | |||
| Vietti Violi [32] * | 62% (32,86) | 96% (92,98) | |||
| Pooled estimates | 87% (81,94) | 93% (91,95) | 82% (76,89) | 98% (96,99) | |
| Early-stage HCC | |||||
| HBP AMRI | NC AMRI | ||||
| Study | Sensitivity (95% CI) | Specificity (95% CI) | First author | Sensitivity (95% CI) | Specificity (95% CI) |
| Brunsing [12] | 87% (65,100) | 91% (86,96) | Sutherland [11] | 80% (28,99) | 98% (95,100) |
| McNamara [28] | 81% (54,96) | 95% (76,100) | |||
| Park [13] | 79% (63,90) | 98% (97,99) | |||
| Pooled estimates | 87% (65,100) | 91% (86,96) | 79% (69,89) | 98% (97,99) | |
| Summary Estimate | ||||
|---|---|---|---|---|
| Variables | Subgroup | Sensitivity (95% CI) | Specificity (95% CI) | p-Value |
| Study design | Prospective (n = 2) | 95% (86,100) | 99% (97,100) | 0.05 |
| Retrospective (n = 8) | 85% (80,90) | 95% (93,97) | - | |
| Study location * | Western (n = 7) | 87% (81,92) | 94% (92,97) | 0.06 |
| Eastern (n = 2) | 81% (72,90) | 98% (97,100) | - | |
| Study quality | Low/unclear risk of bias (n = 5) | 82% (74,89) | 98% (97,98) | 0.01 |
| High risk of bias (n = 5) | 89% (84,95) | 92% (90,94) | - | |
| Cirrhosis | Exclusively enrolling cirrhosis patients (n = 5) | 85% (78,92) | 98% (96,99) | 0.34 |
| Others † (n = 5) | 86% (79,93) | 95% (92,97) | - | |
| Most common underlying liver disease * | Hepatitis C (n = 4) Hepatitis B (n = 4) | 90% (83,96) 83% (76,91) | 93% (91,96) 97% (96,99) | 0.13 |
| HCC prevalence in each study | <20% (n = 6) >20% (n = 4) | 85% (78,91) 88% (80,96) | 96% (93,98) 97% (94,100) | 0.53 |
| MRI magnet field strength * | Only 1.5T (n = 3) | 84% (76,92) | 98% (97,99) | <0.01 |
| 3.0T or both 1.5 and 3.0T (n = 6) | 87% (81,93) | 93% (91,95) | - | |
| Number of surveillance rounds | Single (n = 8) | 87% (81,92) | 96% (94,99) | 0.80 |
| Multiple (n = 2) | 83% (72,94) | 96% (92,100) | - | |
| Interpretation of AMRI * | Clinical practice (n = 2) | 88% (73,100) | 96% (91,100) | 0.91 |
| Simulation (n = 7) | 85% (79,90) | 96% (93,98) | - | |
| Reference standard for HCC | Pathology-only (n = 2) | 83% (72,94) | 99% (96,100) | 0.36 |
| Pathology or imaging (n = 8) | 86% (81,92) | 95% (93,98) | - | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, D.H.; Choi, S.H.; Shim, J.H.; Kim, S.Y.; Lee, S.S.; Byun, J.H.; Choi, J.-I. Meta-Analysis of the Accuracy of Abbreviated Magnetic Resonance Imaging for Hepatocellular Carcinoma Surveillance: Non-Contrast versus Hepatobiliary Phase-Abbreviated Magnetic Resonance Imaging. Cancers 2021, 13, 2975. https://doi.org/10.3390/cancers13122975
Kim DH, Choi SH, Shim JH, Kim SY, Lee SS, Byun JH, Choi J-I. Meta-Analysis of the Accuracy of Abbreviated Magnetic Resonance Imaging for Hepatocellular Carcinoma Surveillance: Non-Contrast versus Hepatobiliary Phase-Abbreviated Magnetic Resonance Imaging. Cancers. 2021; 13(12):2975. https://doi.org/10.3390/cancers13122975
Chicago/Turabian StyleKim, Dong Hwan, Sang Hyun Choi, Ju Hyun Shim, So Yeon Kim, Seung Soo Lee, Jae Ho Byun, and Joon-Il Choi. 2021. "Meta-Analysis of the Accuracy of Abbreviated Magnetic Resonance Imaging for Hepatocellular Carcinoma Surveillance: Non-Contrast versus Hepatobiliary Phase-Abbreviated Magnetic Resonance Imaging" Cancers 13, no. 12: 2975. https://doi.org/10.3390/cancers13122975