
Prediction of Microvascular Invasion in Hepatocellular Carcinoma via Deep Learning: A Multi-Center and Prospective Validation Study

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
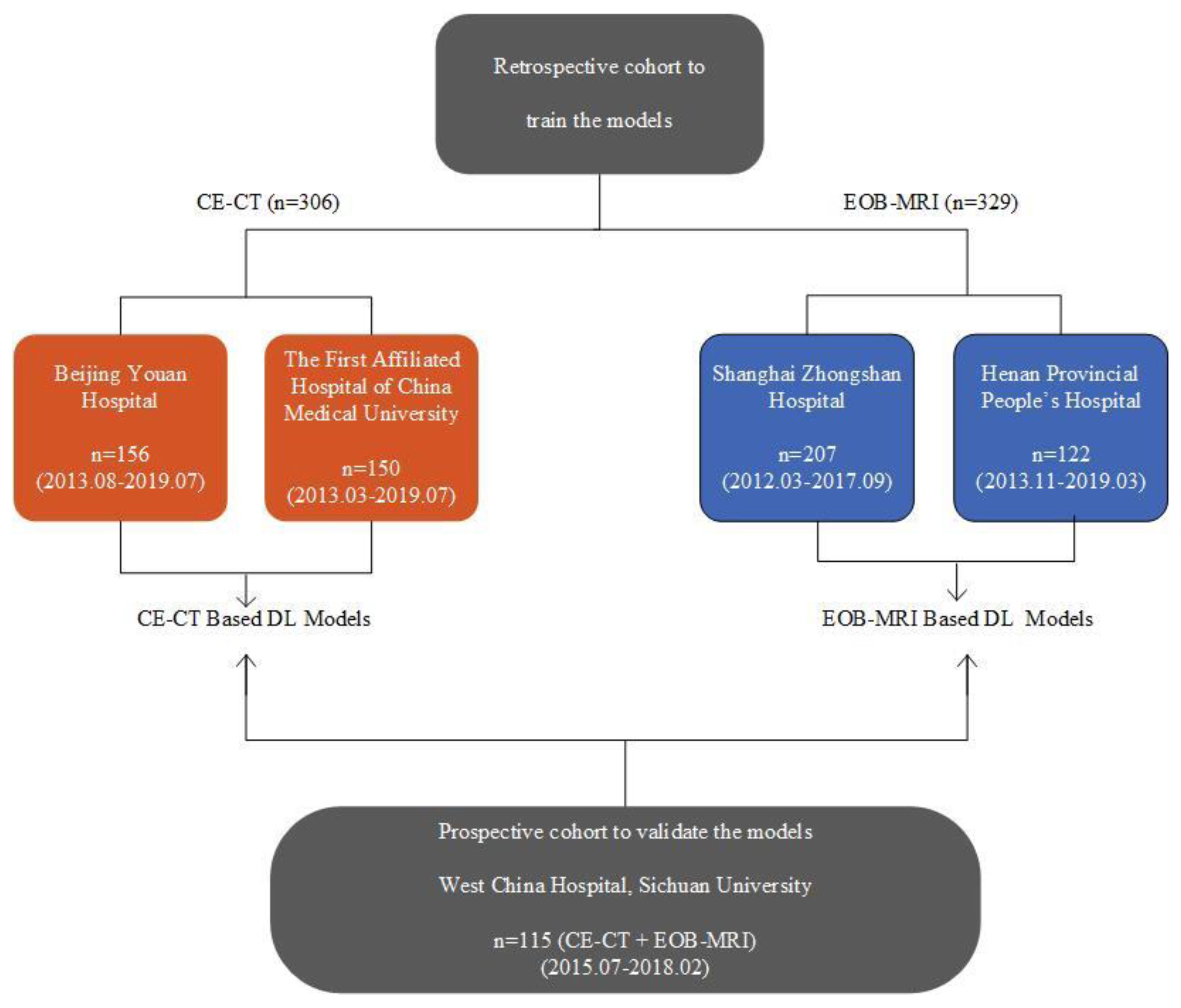
2.1. Patients
2.2. Histopathologic Diagnosis of MVI
2.3. Imaging Acquisition
2.4. Image Analysis
2.5. Development of DL Models
2.6. Model Assessment and Inter-Modality Comparison
2.7. Visualization and Confirmation of the MVI High-Risk Areas
2.8. Prognostic Power Evaluation
2.9. Statistical Analysis
3. Results
3.1. Baseline Characteristics
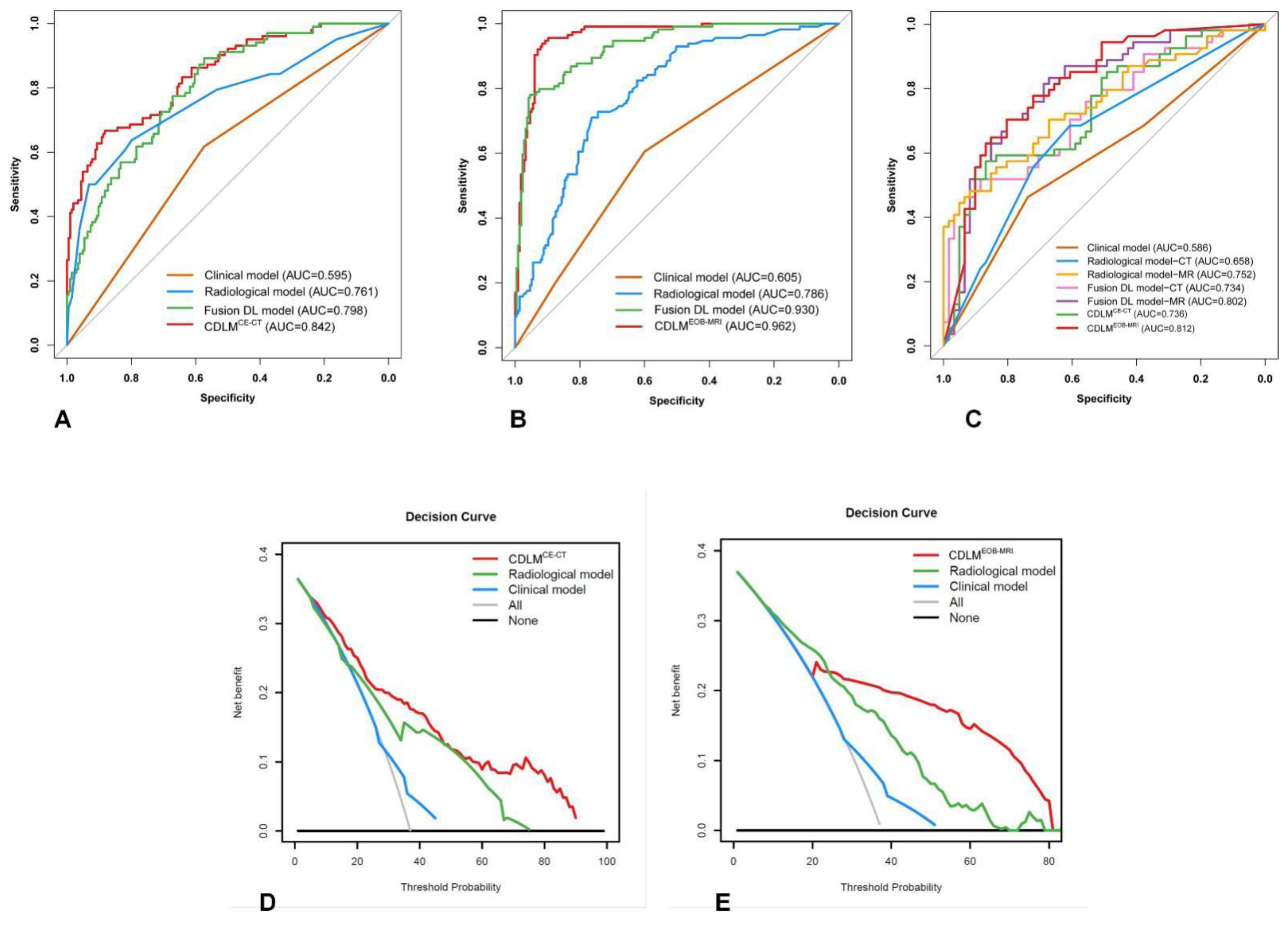
3.2. Predictive Performances of Clinical and Qualitative Radiological Models
3.3. Predictive Performances of CDLMs
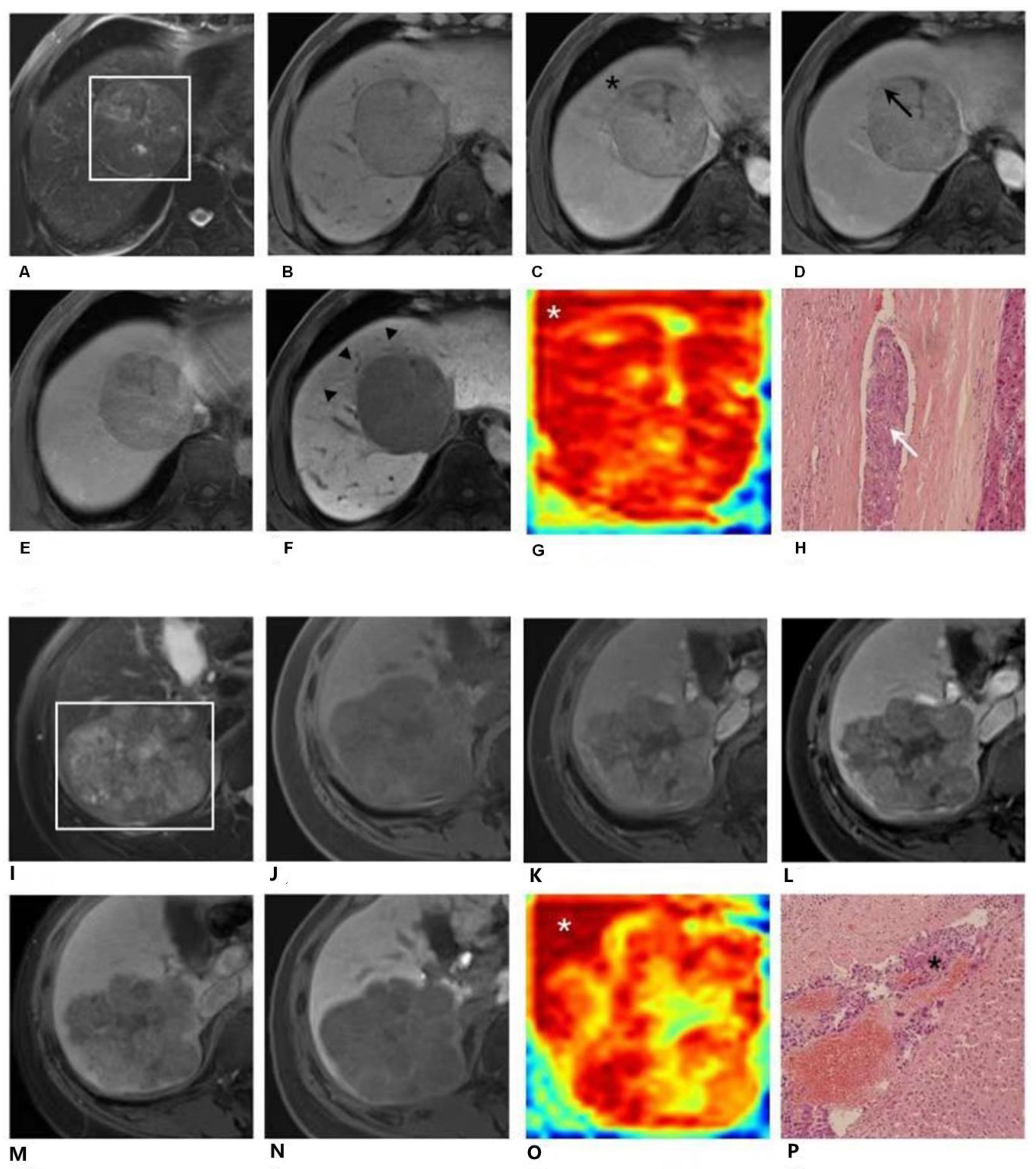
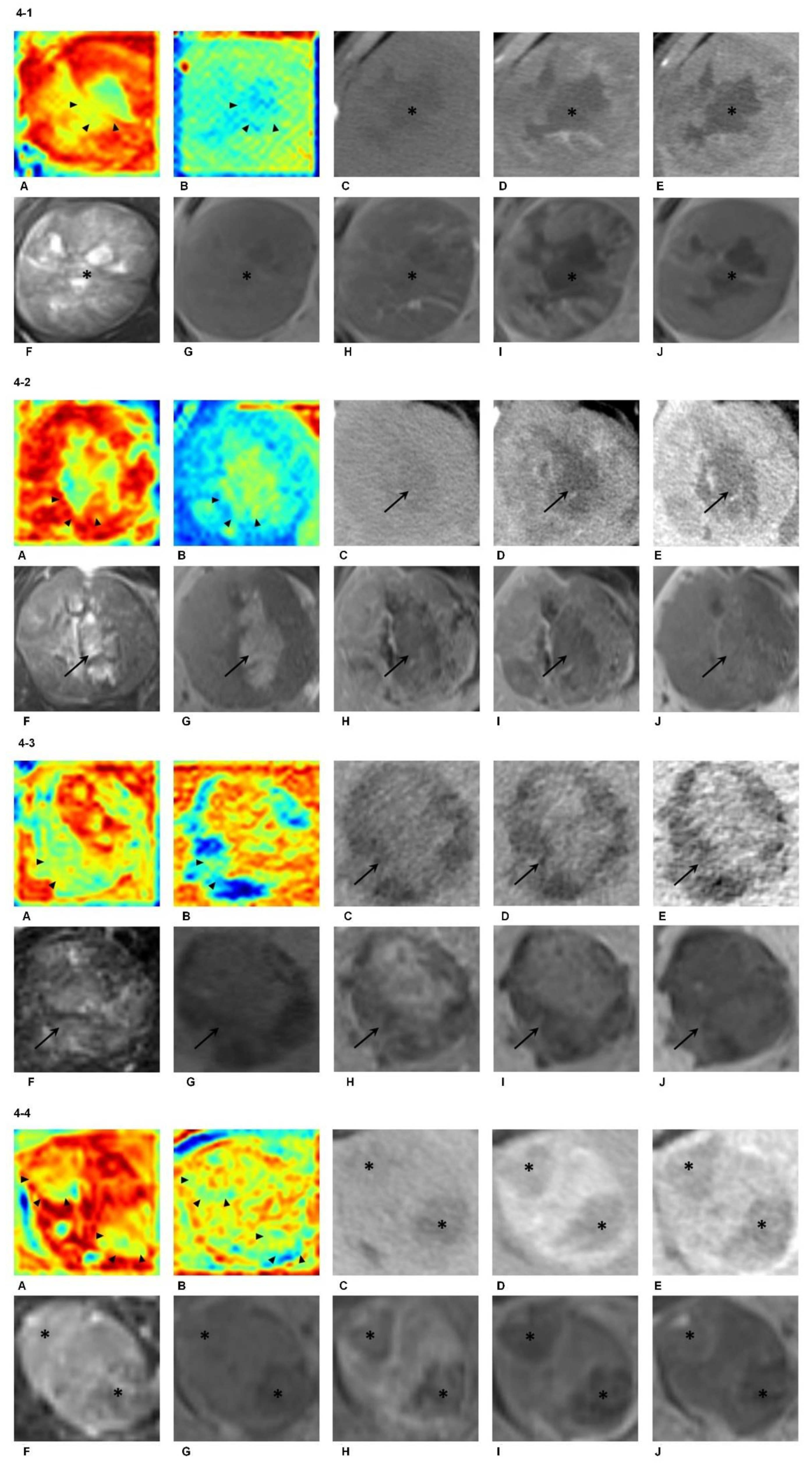
3.4. Identification and Confirmation of the MVI High-Risk Areas
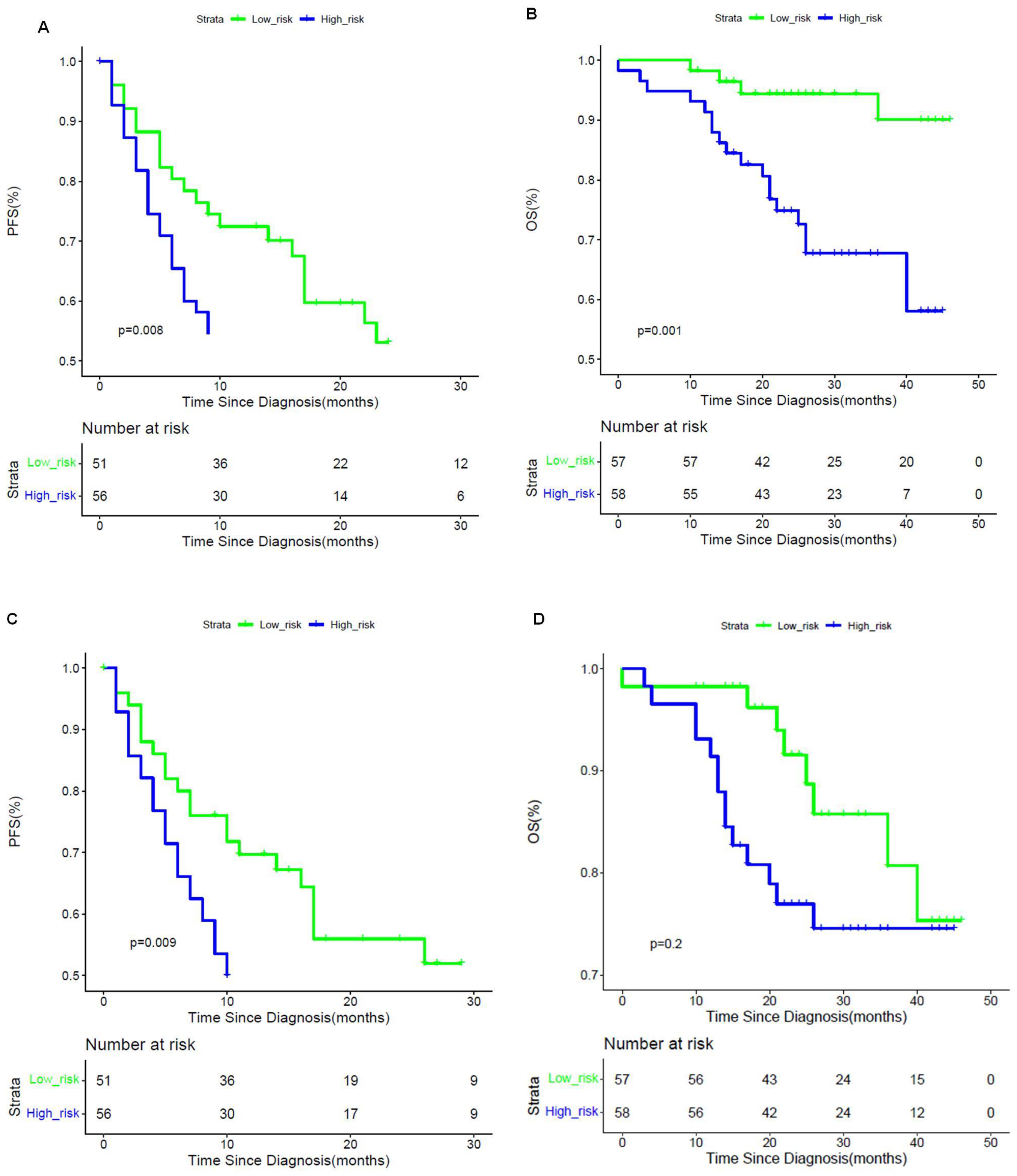
3.5. Prognostic Implications of CDLMs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Forner, A.; Reig, M.; Bruix, J. Hepatocellular carcinoma. Lancet 2019, 391, 1301–1314. [Google Scholar] [CrossRef]
- Tabrizian, P.; Jibara, G.; Shrager, B. Recurrence of hepatocellular cancer after resection: Patterns, treatments, and prognosis. Ann. Surg. 2015, 261, 947–955. [Google Scholar] [CrossRef] [PubMed]
- Marrero, J.A.; Kulik, L.M.; Sirlin, C.B.; Zhu, A.X.; Finn, R.S.; Abecassis, M.M.; Roberts, L.R.; Heimbach, J.K. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American Association for the Study of Liver Diseases. Hepatology 2018, 68, 723–750. [Google Scholar] [CrossRef] [Green Version]
- Imamura, H.; Matsuyama, Y.; Tanaka, E.; Ohkubo, T.; Hasegawa, K.; Miyagawa, S.; Sugawara, Y.; Minagawa, M.; Takayama, T.; Kawasaki, S.; et al. Risk factors contributing to early and late phase intrahepatic recurrence of hepatocellular carcinoma after hepatectomy. J. Hepatol. 2003, 38, 200–207. [Google Scholar] [CrossRef]
- Lim, K.C.; Chow, P.K.H.; Allen, J.C. Microvascular invasion is a better predictor of tumor recurrence and overall survival following surgical resection for hepatocellular carcinoma compared to the Milan criteria. Ann. Surg. 2011, 254, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Sumie, S.; Nakashima, O.; Okuda, K.; Kuromatsu, R.; Kawaguchi, A.; Nakano, M.; Satani, M.; Yamada, S.; Okamura, S.; Hori, M.; et al. The significance of classifying microvascular invasion in patients with hepatocellular carcinoma. Ann. Surg. Oncol. 2014, 21, 1002–1009. [Google Scholar] [CrossRef] [PubMed]
- Erstad, D.J.; Tanabe, K.K. Prognostic and therapeutic implications of microvascular invasion in hepatocellular carcinoma. Ann. Surg. Oncol. 2019, 26, 1474–1493. [Google Scholar] [CrossRef]
- Mazzaferro, V.; Llovet, J.M.; Miceli, R. Predicting survival after liver transplantation in patients with hepatocellular carcinoma beyond the Milan criteria: A retrospective, exploratory analysis. Lancet Oncol. 2009, 10, 35–43. [Google Scholar] [CrossRef]
- Piardi, T.; Gheza, F.; Ellero, B.; Woehl-Jaegle, M.L.; Ntourakis, D.; Cantu, M.; Marzano, E.; Audet, M.; Wolf, P.; Pessaux, P. Number and tumor size are not sufficient criteria to select patients for liver transplantation for hepatocellular carcinoma. Ann. Surg. Oncol. 2012, 19, 2020–2026. [Google Scholar] [CrossRef]
- Iguchi, T.; Shirabe, K.; Aishima, S. New pathologic stratification of microvascular invasion in hepatocellular carcinoma: Predicting prognosis after living-donor liver transplantation. Transplantation 2015, 99, 1236–1242. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Perálvarez, M.; Luong, T.V.; Andreana, L.; Meyer, T.; Dhillon, A.P.; Burroughs, A.K. A systematic review of microvascular invasion in hepatocellular carcinoma: Diagnostic and prognostic variability. Ann. Surg. Oncol. 2013, 20, 325–339. [Google Scholar] [CrossRef]
- Renzulli, M.; Brocchi, S.; Cucchetti, A. Can current preoperative imaging be used to detect microvascular invasion of hepatocellular carcinoma? Radiology 2015, 279, 432–442. [Google Scholar] [CrossRef]
- Kim, K.A.; Kim, M.J.; Jeon, H.M. Prediction of microvascular invasion of hepatocellular carcinoma: Usefulness of peritumoral hypointensity seen on gadoxetate disodium-enhanced hepatobiliary phase images. J. Magn. Reson. Imaging 2012, 35, 629–634. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Kim, S.H.; Lee, J.E. Preoperative gadoxetic acid–enhanced MRI for predicting microvascular invasion in patients with single hepatocellular carcinoma. J. Hepatol. 2017, 67, 526–534. [Google Scholar] [CrossRef]
- Lei, Z.; Li, J.; Wu, D.; Xia, Y.; Wang, Q.; Si, A.; Wang, K.; Wan, X.; Lau, W.Y.; Wu, M.; et al. Nomogram for preoperative estimation of microvascular invasion risk in hepatitis B virus–related hepatocellular carcinoma within the milan criteria. JAMA Surg. 2016, 151, 356–363. [Google Scholar] [CrossRef]
- Yasaka, K.; Akai, H.; Abe, O. Deep learning with convolutional neural network for differentiation of liver masses at dynamic contrast-enhanced CT: A preliminary study. Radiology 2017, 286, 887–896. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.; Lu, X.; Zhou, H. Deep learning Radiomics of shear wave elastography significantly improved diagnostic performance for assessing liver fibrosis in chronic hepatitis B: A prospective multicentre study. Gut 2019, 68, 729–741. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Gu, D.; Wei, J. A Radiomics Nomogram for Preoperative Prediction of Microvascular Invasion in Hepatocellular Carcinoma. Liver Cancer 2019, 8, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Wei, J.; Gu, D. Preoperative radiomics nomogram for microvascular invasion prediction in hepatocellular carcinoma using contrast-enhanced CT. Eur. Radiol. 2019, 29, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Zhang, H.-L.; Liu, Q.-P.; Sun, S.-W.; Zhang, J.; Zhu, F.-P.; Yang, G.; Yan, X.; Zhang, Y.-D.; Liu, X.-S. Radiomic analysis of contrast-enhanced CT predicts microvascular invasion and outcome in hepatocellular carcinoma. J. Hepatol. 2019, 70, 1133–1144. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S. Deep residual learning for image recognition. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 July 2016; pp. 770–778. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Selvaraju, R.R.; Cogswell, M.; Das, A. Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar]
- Kotikalapudi, R. Keras-Vis. GitHub. Available online: https://github.com/raghakot/keras-vis (accessed on 10 May 2021).
- Banerjee, S.; Wang, D.S.; Kim, H.J.; Sirlin, C.B.; Chan, M.G.; Korn, R.L.; Rutman, A.M.; Siripongsakun, S.; Lu, D.; Imanbayev, G.; et al. A computed tomography radiogenomic biomarker predicts microvascular invasion and clinical outcomes in hepatocellular carcinoma. Hepatology 2015, 62, 792–800. [Google Scholar] [CrossRef]
- Cucchetti, A.; Piscaglia, F.; Grigioni, A.D.E. Preoperative prediction of hepatocellular carcinoma tumour grade and micro-vascular invasion by means of artificial neural network: A pilot study. J. Hepatol. 2010, 52, 880–888. [Google Scholar] [CrossRef]
- Renzulli, M.; Buonfiglioli, F.; Conti, F.; Brocchi, S.; Serio, I.; Foschi, F.G.; Caraceni, P.; Mazzella, G.; Verucchi, G.; Golfieri, R.; et al. Imaging features of microvascular invasion in hepatocellular carcinoma developed after direct-acting antiviral therapy in HCV-related cirrhosis. Eur. Radiol. 2018, 28, 506–513. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.T.; Yang, L.; Yang, Z.X. Assessment of microvascular invasion of hepatocellular carcinoma with diffusion kurtosis imaging. Radiology 2017, 286, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Chernyak, V.; Fowler, K.J.; Kamaya, A.; Kielar, A.Z.; Elsayes, K.M.; Bashir, M.R.; Kono, Y.; Do, R.K.; Mitchell, D.G.; Singal, A.G.; et al. Liver Imaging Reporting and Data System (LI-RADS) version 2018: Imaging of hepatocellular carcinoma in at-risk patients. Radiology 2018, 289, 816–830. [Google Scholar] [CrossRef] [PubMed]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Prospective Cohort. | Retrospective Cohort (EOB-MRI or CE-CT) |
|---|---|
| Inclusion Criteria | |
| 1. Age ≥ 18 years | 1. Age ≥ 18 years |
| 2. High risk for HCC (cirrhosis and/or chronic hepatitis B virus infection) | 2. Patients with surgically confirmed HCC |
| 3. No previous treatment for hepatic lesions | 3. Histopathological examination with proven MVI status recorded |
| 4. Patients with Child-Pugh class A liver function | 4. Preoperative EOB-MRI or CE-CT were performed within one month prior to surgery |
| Exclusion Criteria | |
| 1. Non-HCC patients | 1. Patients without important clinical data |
| 2. Patients with any previous antitumoral treatment | 2. Patients with any previous antitumoral treatment |
| 3. Patients with any contraindication of gadoxetate disodium-enhanced MRI | 3. Patients without conclusive histopathological confirmation of MVI status |
| 4. Patients with insufficient image quality to perform reliable qualitative or radiomics analysis | 4. Patients with unequivocal macrovascular invasion |
| 5. Patients without conclusive histopathological confirmation of MVI status | 5. Patients with insufficient image quality to perform reliable qualitative or radiomics analysis |
| 6. Patients with unequivocal macrovascular invasion | |
| 7. The time interval between preoperative EOB-MRI and surgery exceeded one month | |
| CE-CT Cohort | ||||||
| Characteristics | Training Dataset (n = 306) | Validation Dataset (n = 115) | ||||
| MVI Present | MVI Absent | p Value | MVI Present | MVI Absent | p Value | |
| Age (years) | 55 ± 11 | 59 ± 9 | 0.544 | 48 ± 11 | 52 ± 11 | 0.288 |
| Gender | 0.630 | 0.140 | ||||
| Male | 77 (75.5) | 159 (77.9) | 39 (72.2) | 51 (83.6) | ||
| Female | 25 (24.5) | 45 (22.1) | 15 (27.8) | 10 (16.4) | ||
| Etiology of liver disease | 0.850 | 0.286 | ||||
| HBV | 95 (93.1) | 191 (93.6) | 53 (98.1) | 61 (100) | ||
| HCV | 3 (2.9) | 4 (2.0) | 1 (1.9) | 0 | ||
| None or other | 4 (3.9) | 9 (4.4) | 0 | 0 | ||
| Total bilirubin | 0.05 | 0.926 | ||||
| <20.4 μmol/L | 52 (51.0) | 128 (62.7) | 43 (79.6) | 49 (80.3) | ||
| >20.4 μmol/L | 50 (49.0) | 76 (37.3) | 11 (20.4) | 12 (19.7) | ||
| Alanine aminotransferase | 0.515 | 0.485 | ||||
| <40 U/L | 42 (41.2) | 92 (45.1) | 32 (59.3) | 40 (65.6) | ||
| >40 U/L | 60 (58.8) | 112 (54.9) | 22 (40.7) | 21 (34.4) | ||
| Aspartate aminotransaminase | 0.001 | 0.019 | ||||
| <35 U/L | 25 (24.5) | 90 (44.1) | 20 (37.0) | 36 (59.0) | ||
| >35 U/L | 77 (75.5) | 114 (55.9) | 34 (63.0) | 25 (41.0) | ||
| Platelet | 0.001 | 0.067 | ||||
| <125 × 109/L | 14 (13.7) | 63 (30.9) | 5 (9.3) | 1 (1.6) | ||
| >125×109/L | 88 (86.3) | 141 (69.1) | 49 (90.7) | 60 (98.4) | ||
| α-fetoprotein | 0.007 | 0.067 | ||||
| <20 ng/mL | 39 (38.2) | 117 (57.4) | 17 (31.5) | 23 (37.7) | ||
| 20–400 ng/mL | 32 (31.4) | 44 (21.6) | 12 (22.2) | 22 (36.1) | ||
| >400 ng/mL | 31 (30.4) | 43 (21.1) | 25 (46.3) | 16 (26.2) | ||
| Edmondson–Steiner grade * | 0.356 | 0.002 | ||||
| Grade I | 4 (9.5) | 24 (15.3) | 0 | 5 (8.2) | ||
| Grade II | 21 (50.0) | 86 (54.8) | 29 (53.7) | 44 (72.1) | ||
| Grade III | 17 (40.5) | 47 (29.9) | 25 (46.3) | 12 (19.7) | ||
| CT imaging features | ||||||
| Cirrhosis of background liver | 0.001 | 0.902 | ||||
| Absent | 31 (30.4) | 30 (14.7) | 18 (33.3) | 21 (34.4) | ||
| Present | 71 (69.6) | 174 (85.3) | 36 (66.7) | 40 (65.6) | ||
| Number of tumors | <0.001 | 0.210 | ||||
| Solitary | 70 (68.6) | 181 (88.7) | 33 (61.1) | 44 (72.1) | ||
| Multiple | 32 (31.4) | 23 (11.3) | 21 (38.9) | 17 (27.9) | ||
| Tumor size (cm) | 5.8 ± 4.3 | 4.0 ± 3.6 | <0.001 | 7.6 ± 3.3 | 4.7 ± 2.0 | <0.001 |
| Tumor margin | 0.019 | 0.014 | ||||
| Smooth margin | 29 (28.4) | 86 (42.2) | 25 (46.3) | 42 (68.9) | ||
| Non-smooth margin | 73 (71.6) | 118 (57.8) | 29 (53.7) | 19 (31.1) | ||
| Peritumoral enhancement | 0.001 | 0.003 | ||||
| Absent | 49 (48.0) | 139 (68.1) | 24 (44.4) | 44 (72.1) | ||
| Present | 53 (52.0) | 65 (31.9) | 30 (55.6) | 17 (27.9) | ||
| Enhancement pattern | <0.001 | 0.851 | ||||
| Typical | 77 (75.5) | 113 (55.4) | 51 (81.9) | 56 (87.2) | ||
| Atypical | 25 (24.5) | 91 (44.6) | 3 (18.1) | 5 (12.8) | ||
| Radiologic capsule | 0.931 | 0.512 | ||||
| Absent | 32 (31.4) | 65 (31.9) | 13 (24.1) | 18 (29.5) | ||
| Present | 70 (68.6) | 139 (68.1) | 41 (75.9) | 43 (70.5) | ||
| EOB-MRI Cohort | ||||||
| Characteristics | Training Dataset (n = 329) | Validation Dataset (n = 115) | ||||
| MVI Present | MVI Absent | p Value | MVI Present | MVI Absent | p Value | |
| Age (years) | 55 ± 10 | 54 ± 10 | 0.544 | 48 ± 11 | 52 ± 11 | 0.567 |
| Gender | 0.331 | 0.140 | ||||
| Male | 97 (85.1) | 188 (87.4) | 39 (72.2) | 51 (83.6) | ||
| Female | 17 (14.9) | 27 (12.6) | 15 (27.8) | 10 (16.4) | ||
| Etiology of liver disease | 0.637 | 0.286 | ||||
| HBV | 103 (90.4) | 200 (93.0) | 53 (98.1) | 61 (100) | ||
| HCV | 5 (4.4) | 8 (3.7) | 1 (1.9) | 0 | ||
| None or other | 6 (5.3) | 7 (3.3) | 0 | 0 | ||
| Total bilirubin | 0.358 | 0.926 | ||||
| <20.4 μmol/L | 98 (86.0) | 180 (83.7) | 43 (79.6) | 49 (80.3) | ||
| >20.4 μmol/L | 16 (14.0) | 35 (16.3) | 11 (20.4) | 12 (19.7) | ||
| Alanine aminotransferase | 0.293 | 0.485 | ||||
| <40 U/L | 76 (66.7) | 151 (70.2) | 32 (59.3) | 40 (65.6) | ||
| >40 U/L | 38 (33.3) | 64 (29.8) | 22 (40.7) | 21 (34.4) | ||
| Aspartate aminotransaminase | 0.095 | 0.019 | ||||
| <35 U/L | 74 (64.9) | 156 (72.6) | 20 (37.0) | 36 (59.0) | ||
| >35 U/L | 40 (35.1) | 59 (27.4) | 34 (63.0) | 25 (41.0) | ||
| Platelet | 0.262 | 0.067 | ||||
| <125 × 109/L | 56 (49.1) | 115 (53.5) | 5 (9.3) | 1 (1.6) | ||
| >125 × 109/L | 58 (50.9) | 100 (46.5) | 49 (90.7) | 60 (98.4) | ||
| α-fetoprotein | 0.002 | 0.067 | ||||
| <20 ng/mL | 45 (39.5) | 129 (60.0) | 17 (31.5) | 23 (37.7) | ||
| 20–400 ng/mL | 46 (40.4) | 59 (27.4) | 12 (22.2) | 22 (36.1) | ||
| >400 ng/mL | 23 (20.2) | 27 (12.6) | 25 (46.3) | 16 (26.2) | ||
| Edmondson–Steiner grade | <0.001 | 0.002 | ||||
| Grade I | 1 (0.9) | 16 (7.4) | 0 | 5 (8.2) | ||
| Grade II | 58 (50.9) | 140 (65.1) | 29 (53.7) | 44 (72.1) | ||
| Grade III | 55 (48.2) | 59 (27.4) | 25 (46.3) | 12 (19.7) | ||
| MR imaging features | ||||||
| Cirrhosis of background liver | 0.720 | 0.902 | ||||
| Absent | 37 (32.5) | 74 (34.4) | 18 (33.3) | 21 (34.4) | ||
| Present | 77 (67.5) | 141 (65.6) | 36 (66.7) | 40 (65.6) | ||
| Number of tumors | <0.001 | 0.210 | ||||
| Solitary | 75 (65.8) | 178 (82.8) | 33 (61.1) | 44 (72.1) | ||
| Multiple | 39 (34.2) | 37 (17.2) | 21 (38.9) | 17 (27.9) | ||
| Tumor size (cm) | 4.1 ± 3.0 | 2.3 ± 1.5 | <0.001 | 7.6 ± 3.3 | 4.7 ± 2.0 | <0.001 |
| Tumor margin | <0.001 | 0.014 | ||||
| Smooth margin | 34 (29.8) | 110 (51.2) | 25 (46.3) | 42 (68.9) | ||
| Non-smooth margin | 80 (70.2) | 105 (48.8) | 29 (53.7) | 19 (31.1) | ||
| Peritumoral enhancement | <0.001 | 0.021 | ||||
| Absent | 61 (53.5) | 170 (79.1) | 22 (40.7) | 38 (62.3) | ||
| Present | 53 (46.5) | 45 (20.9) | 32 (59.3) | 23 (37.7) | ||
| Enhancement pattern | <0.001 | 0.190 | ||||
| Typical | 50 (43.9) | 141 (65.6) | 43 (79.6) | 54 (88.5) | ||
| Atypical | 64 (56.1) | 74 (34.4) | 11 (20.4) | 7 (11.5) | ||
| Radiologic capsule | 0.370 | 0.743 | ||||
| Absent | 34 (29.8) | 59 (27.4) | 6 (11.1) | 8 (13.1) | ||
| Present | 80 (70.2) | 156 (72.6) | 48 (88.9) | 53 (86.9) | ||
| Tumor hypointensity on HBP | <0.001 | 0.550 | ||||
| Absent | 53 (46.5) | 152 (70.7) | 3 (5.6) | 2 (3.3) | ||
| Present | 61 (53.5) | 63 (29.3) | 51 (94.4) | 59 (96.7) | ||
| Peritumoral hypointensity on HBP image | <0.001 | <0.001 | ||||
| Absent | 80 (70.2) | 194 (90.7) | 11 (20.4) | 36 (59.0) | ||
| Present | 34 (29.8) | 20 (9.3) | 43 (79.6) | 25 (41.0) | ||
| Developed Models | Retrospective Training Cohort (EOB-MRI n = 329; CE-CT n = 306) | Prospective Validation Cohort 2 (n = 115) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| SEN | SPE | ACC | AUC (95% CI) | SEN | SPE | ACC | AUC (95% CI) | ||
| Clinical model | CE-CT | 61.8% | 57.4% | 58.8% | 0.595 (0.533–0.657) | 68.5% | 37.7% | 52.2% | 0.586 (0.485–0.686) |
| EOB-MRI | 60.5% | 60.0% | 60.2% | 0.605 (0.546–0.664) | 68.5% | 37.7% | 52.2% | 0.586 (0.485–0.686) | |
| Radiological model | CE-CT | 63.7% | 79.9% | 74.5% | 0.761 (0.700–0.822) | 68.5% | 57.4% | 62.6% | 0.658 (0.561–0.754) |
| EOB-MRI | 71.1% | 76.3% | 74.5% | 0.786 (0.736–0.836) | 88.9% | 31.2% | 58.3% | 0.752 (0.662–0.842) | |
| Single CT-phase-based signature | Arterial phase | 68.6% | 73.5% | 71.9% | 0.742 (0.690–0.789) | 44.4% | 86.9% | 67.0% | 0.703 (0.619–0.779) |
| Venous phase | 75.5% | 69.6% | 71.6% | 0.785 (0.738–0.828) | 75.9% | 62.3% | 68.7% | 0.723 (0.642–0.799) | |
| Plain phase | 67.6% | 72.1% | 70.6% | 0.759 (0.716–0.805) | 66.7% | 63.9% | 65.2% | 0.689 (0.602–0.771) | |
| Single MR-sequence-based signature | Arterial phase | 71.1% | 87.9% | 82.1% | 0.865 (0.824–0.905) | 74.1% | 75.4% | 74.8% | 0.780 (0.695–0.865) |
| Venous phase | 70.2% | 70.2% | 70.2% | 0.766 (0.712–0.820) | 61.1% | 72.1% | 67.0% | 0.699 (0.604–0.795) | |
| Transitional phase | 68.4% | 70.2% | 69.6% | 0.746 (0.690–0.803) | 66.7% | 67.2% | 67.0% | 0.672 (0.573–0.772) | |
| T2WI | 78.9% | 64.7% | 69.6% | 0.775 (0.723–0.827) | 77.8% | 62.3% | 69.6% | 0.732 (0.639–0.824) | |
| HBP T1WI | 64.0% | 79.1% | 73.9% | 0.768 (0.714–0.822) | 63.0% | 75.4% | 69.6% | 0.710 (0.614–0.806) | |
| Fusion DL model | CE-CT | 89.2% | 57.4% | 68.0% | 0.798 (0.753–0.840) | 51.9% | 88.5% | 71.3% | 0.734 (0.654–0.806) |
| EOB-MRI | 78.1% | 95.3% | 89.4% | 0.930 (0.902-0.957) | 70.4% | 80.3% | 75.7% | 0.802 (0.720–0.885) | |
| CDLM | CDLMCE-CT | 66.7% | 88.2% | 81.0% | 0.842 (0.803–0.883) | 57.4% | 86.9% | 73.0% | 0.736 (0.662–0.805) |
| CDLMEOB-MRI | 93.9% | 91.6% | 92.4% | 0.962 (0.857–0.927) | 70.4% | 80.3% | 75.7% | 0.812 (0.721–0.880) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wei, J.; Jiang, H.; Zeng, M.; Wang, M.; Niu, M.; Gu, D.; Chong, H.; Zhang, Y.; Fu, F.; Zhou, M.; et al. Prediction of Microvascular Invasion in Hepatocellular Carcinoma via Deep Learning: A Multi-Center and Prospective Validation Study. Cancers 2021, 13, 2368. https://doi.org/10.3390/cancers13102368
Wei J, Jiang H, Zeng M, Wang M, Niu M, Gu D, Chong H, Zhang Y, Fu F, Zhou M, et al. Prediction of Microvascular Invasion in Hepatocellular Carcinoma via Deep Learning: A Multi-Center and Prospective Validation Study. Cancers. 2021; 13(10):2368. https://doi.org/10.3390/cancers13102368
Chicago/Turabian StyleWei, Jingwei, Hanyu Jiang, Mengsu Zeng, Meiyun Wang, Meng Niu, Dongsheng Gu, Huanhuan Chong, Yanyan Zhang, Fangfang Fu, Mu Zhou, and et al. 2021. "Prediction of Microvascular Invasion in Hepatocellular Carcinoma via Deep Learning: A Multi-Center and Prospective Validation Study" Cancers 13, no. 10: 2368. https://doi.org/10.3390/cancers13102368