Nivolumab plus Ipilimumab versus Existing Immunotherapies in Patients with PD-L1-Positive Advanced Non-Small Cell Lung Cancer: A Systematic Review and Network Meta-Analysis

 , , ,
, , , 
Abstract
:1. Introduction
2. Methods
2.1. Systematic Review
2.2. Quality Assessment
2.3. Inclusion and Exclusion Criteria (Predefined PICOS)
2.3.1. Patients
2.3.2. Interventions/Comparisons
2.3.3. Outcomes
2.3.4. Study Design
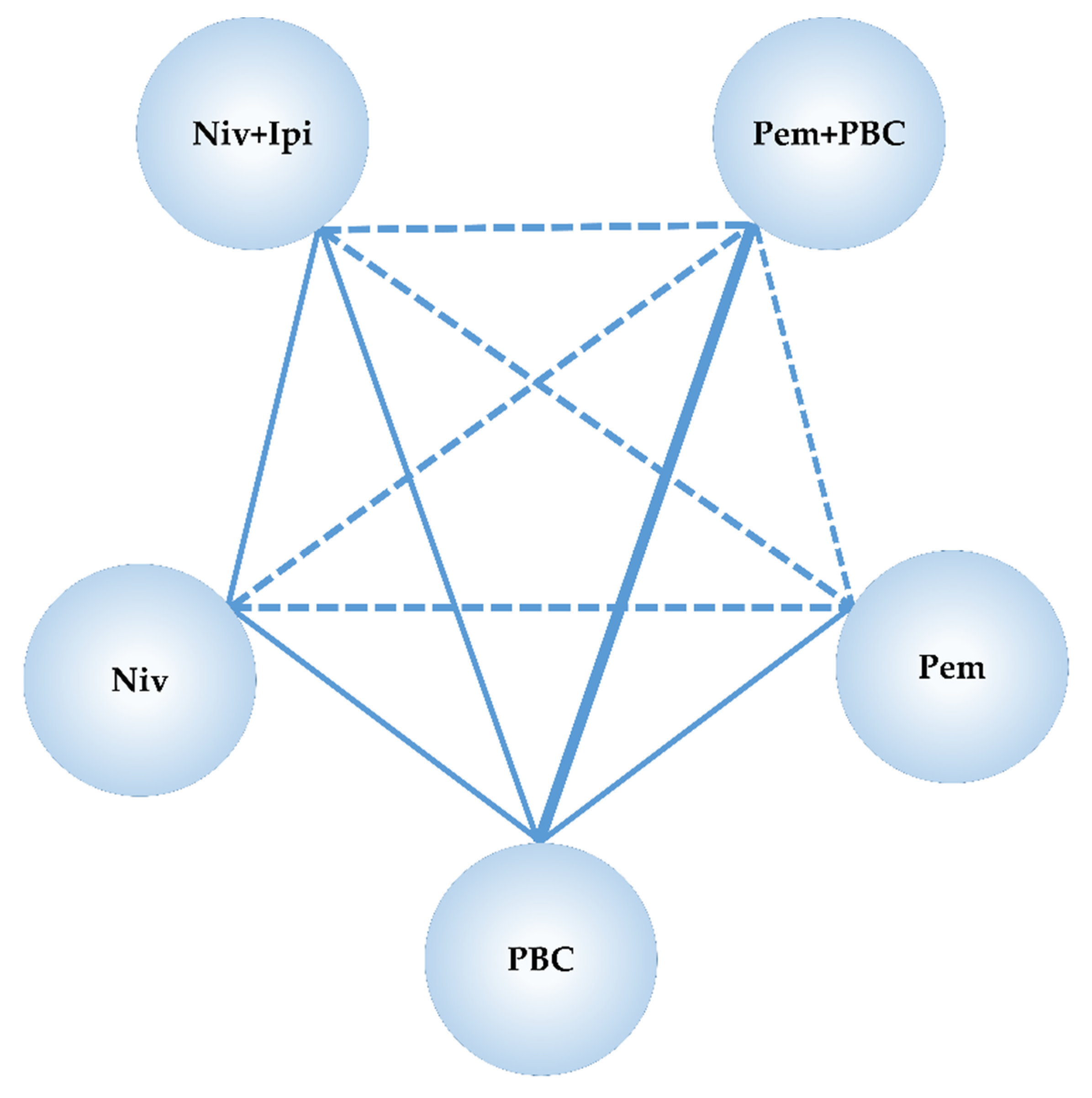
2.4. Statistical Method of Network Meta-Analysis
2.5. Ethical Aspects
3. Results
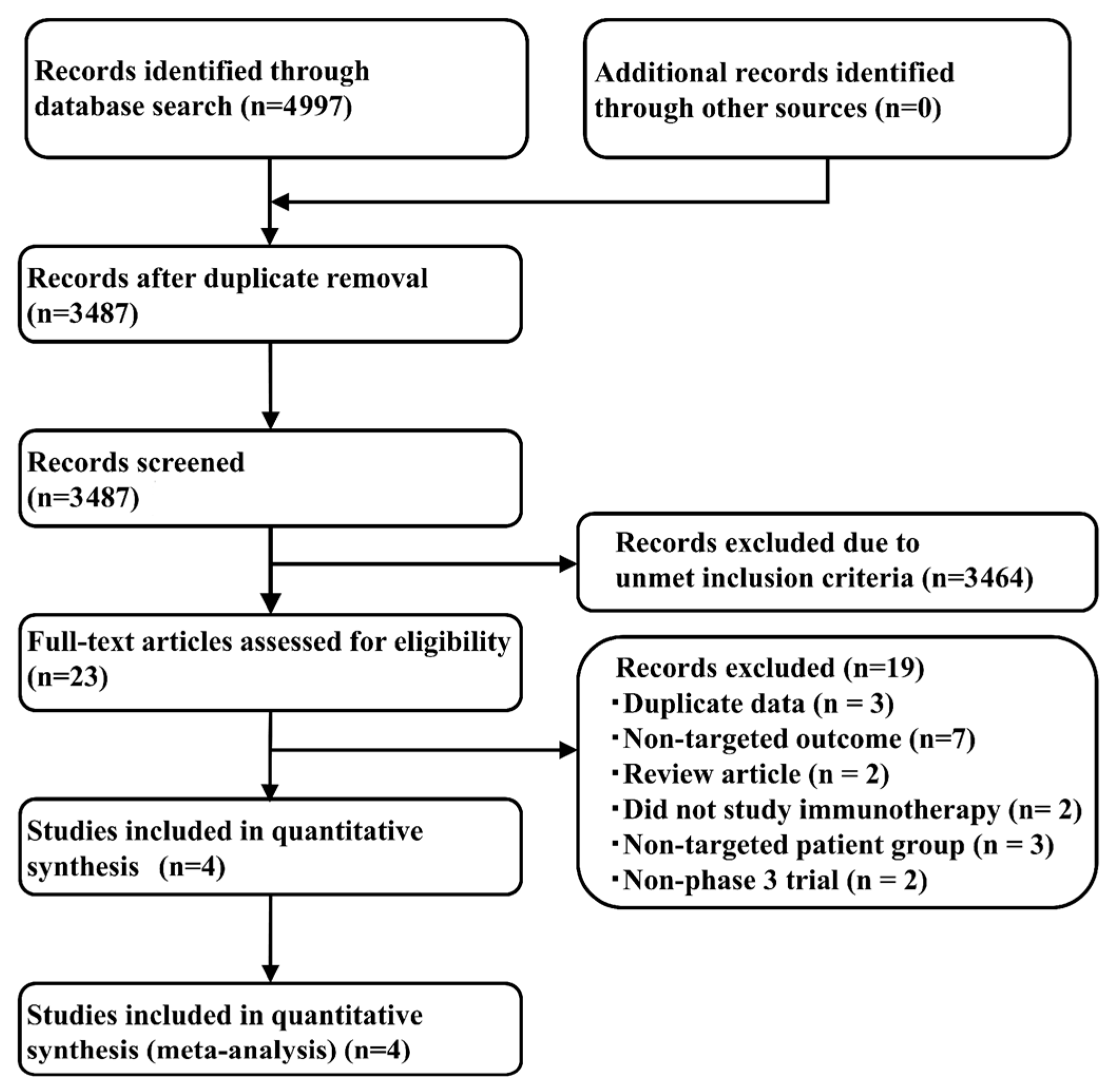
3.1. Systematic Review
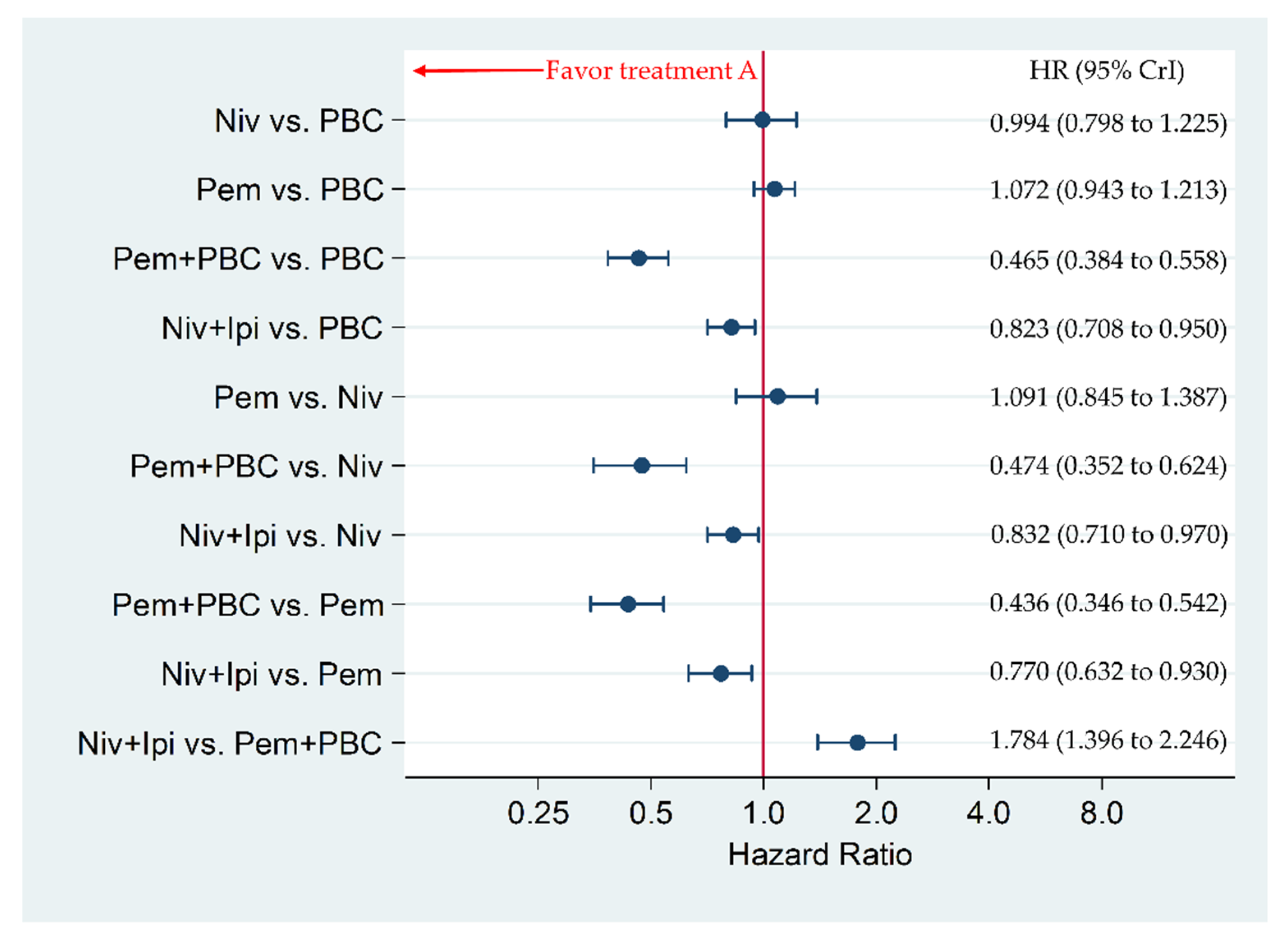
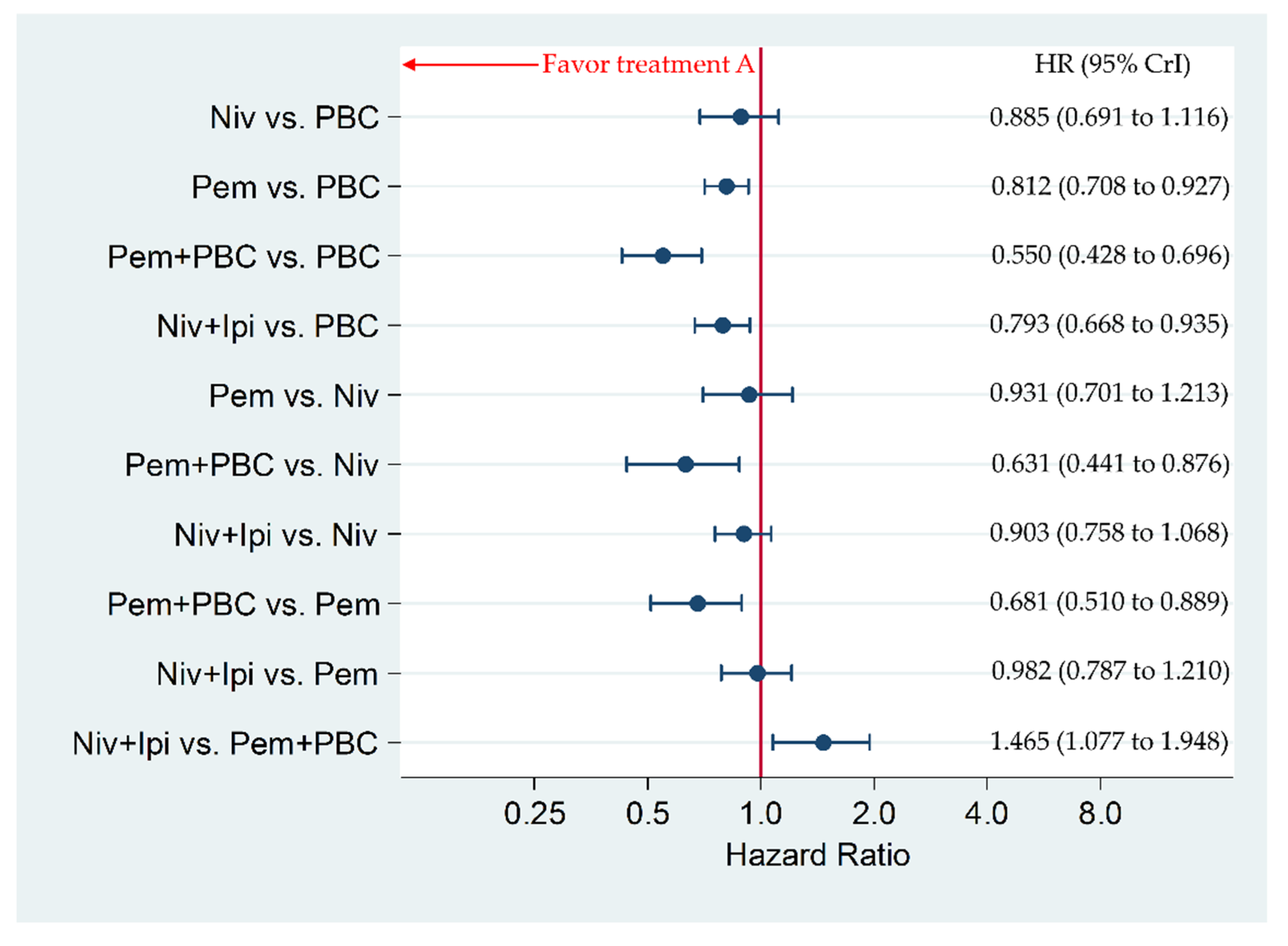
3.2. Primary Efficacy Endpoint: Progression-Free Survival in Patients with a PD-L1 Expression of 1% or More
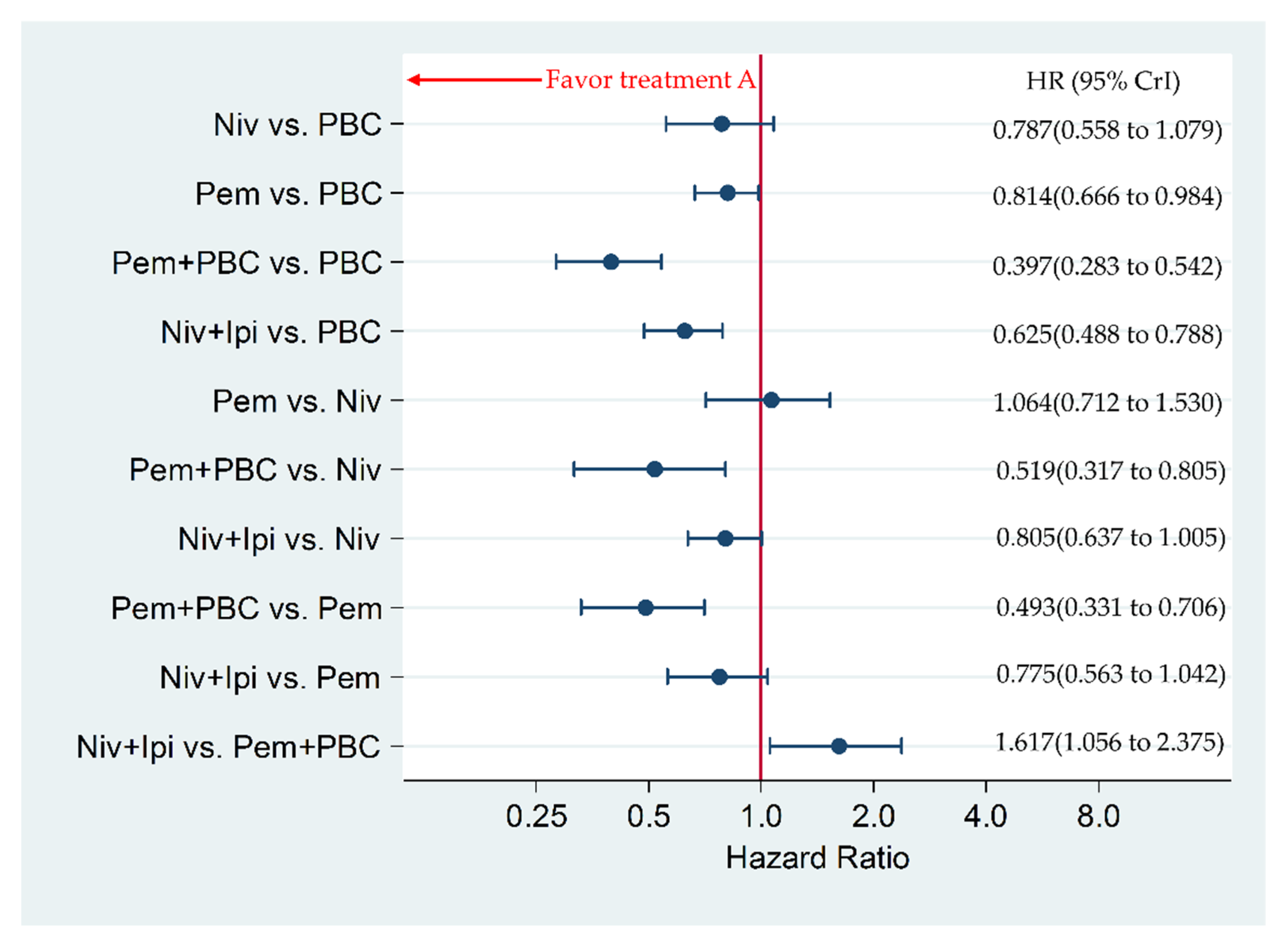
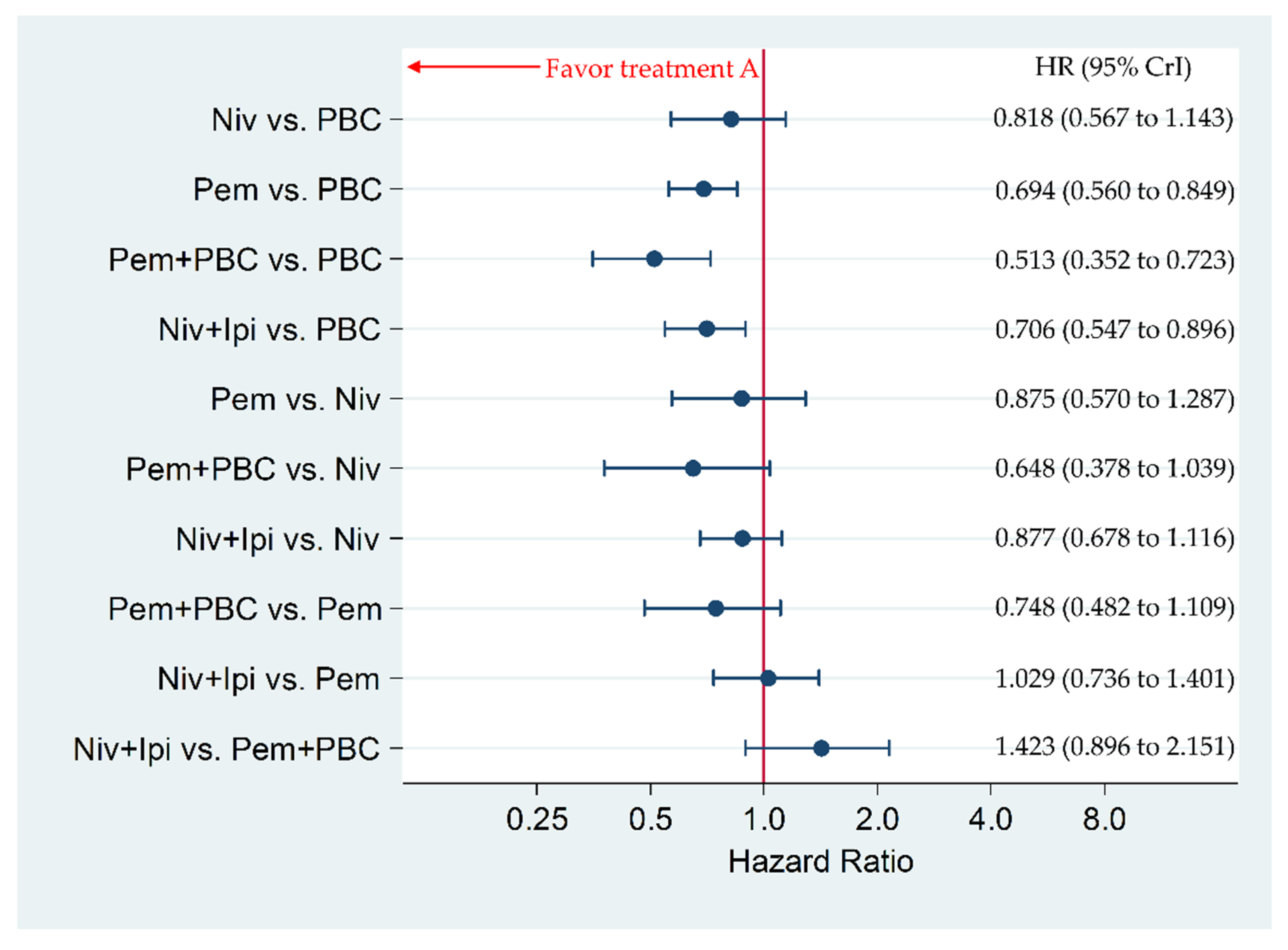
3.3. Secondary Efficacy Endpoint: Progression-Free Survival in Patients with a PD-L1 Expression of 50% or More
3.4. Secondary Efficacy Endpoint: Overall Survival in Patients with a PD-L1 of 1% or More
3.5. Secondary Efficacy Endpoint: Overall Survival in Patients with PD-L1 of 50% or More
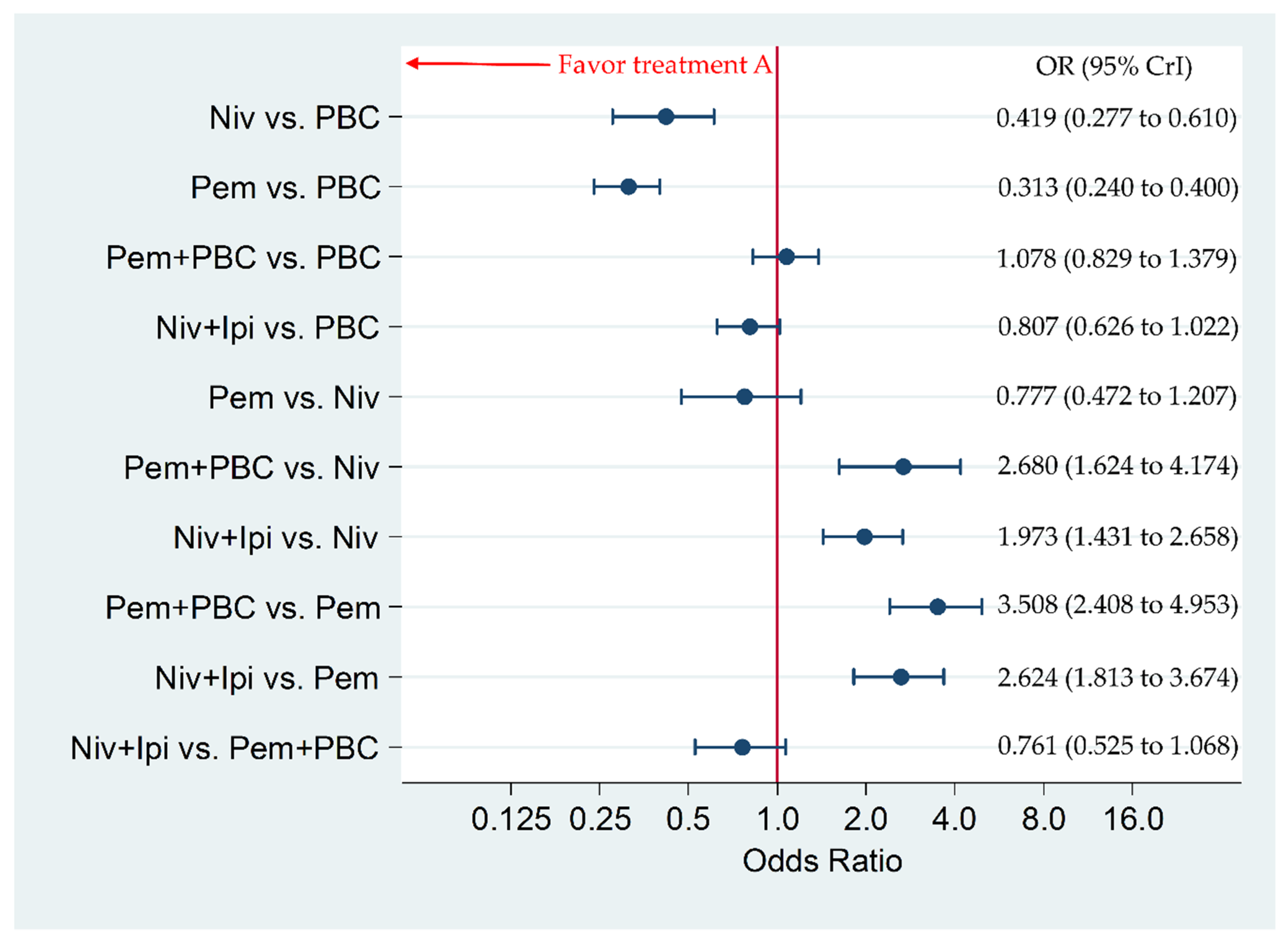
3.6. Primary Safety Endpoint: Incidence of G3–5AEs in the Overall Population
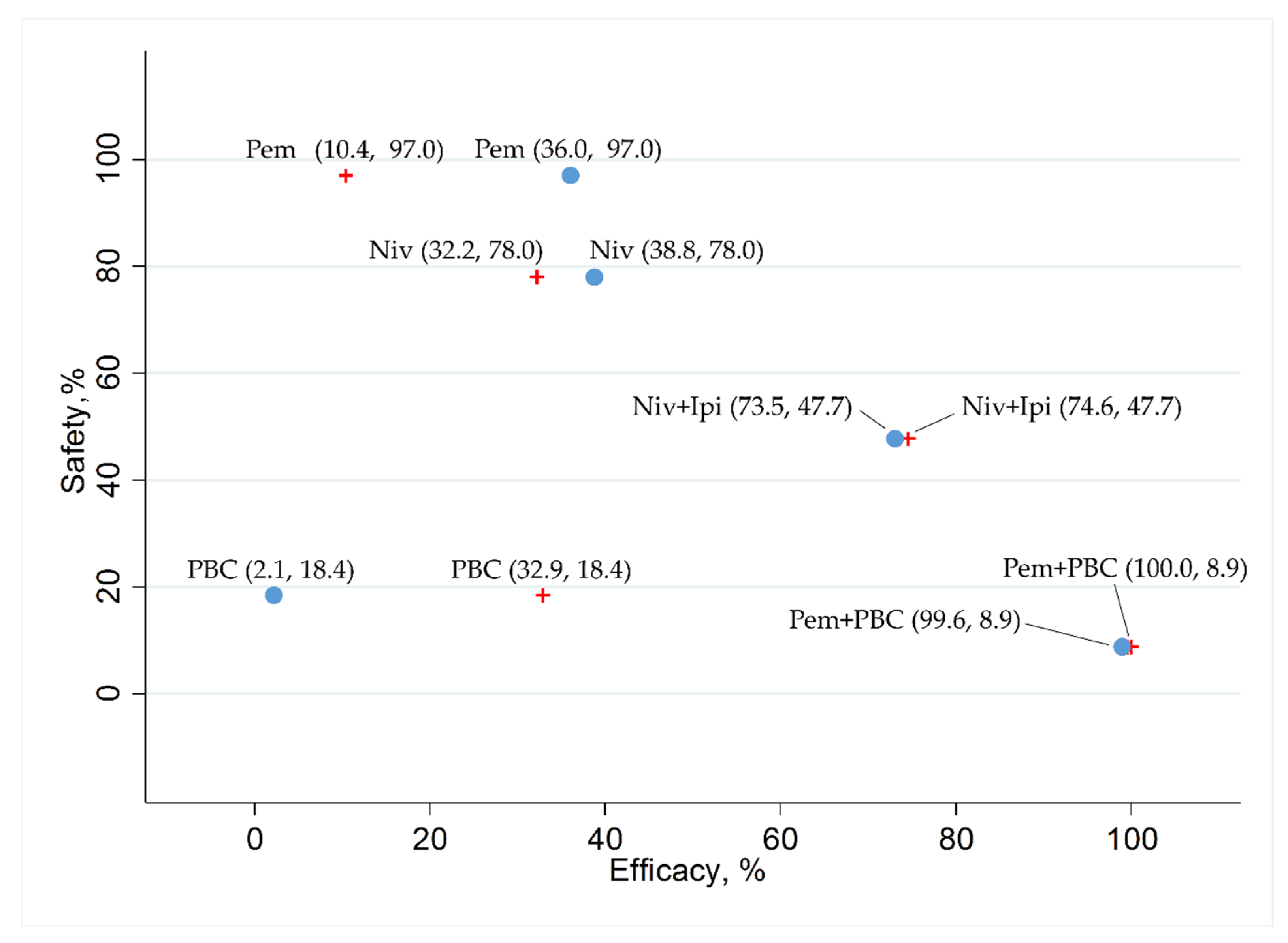
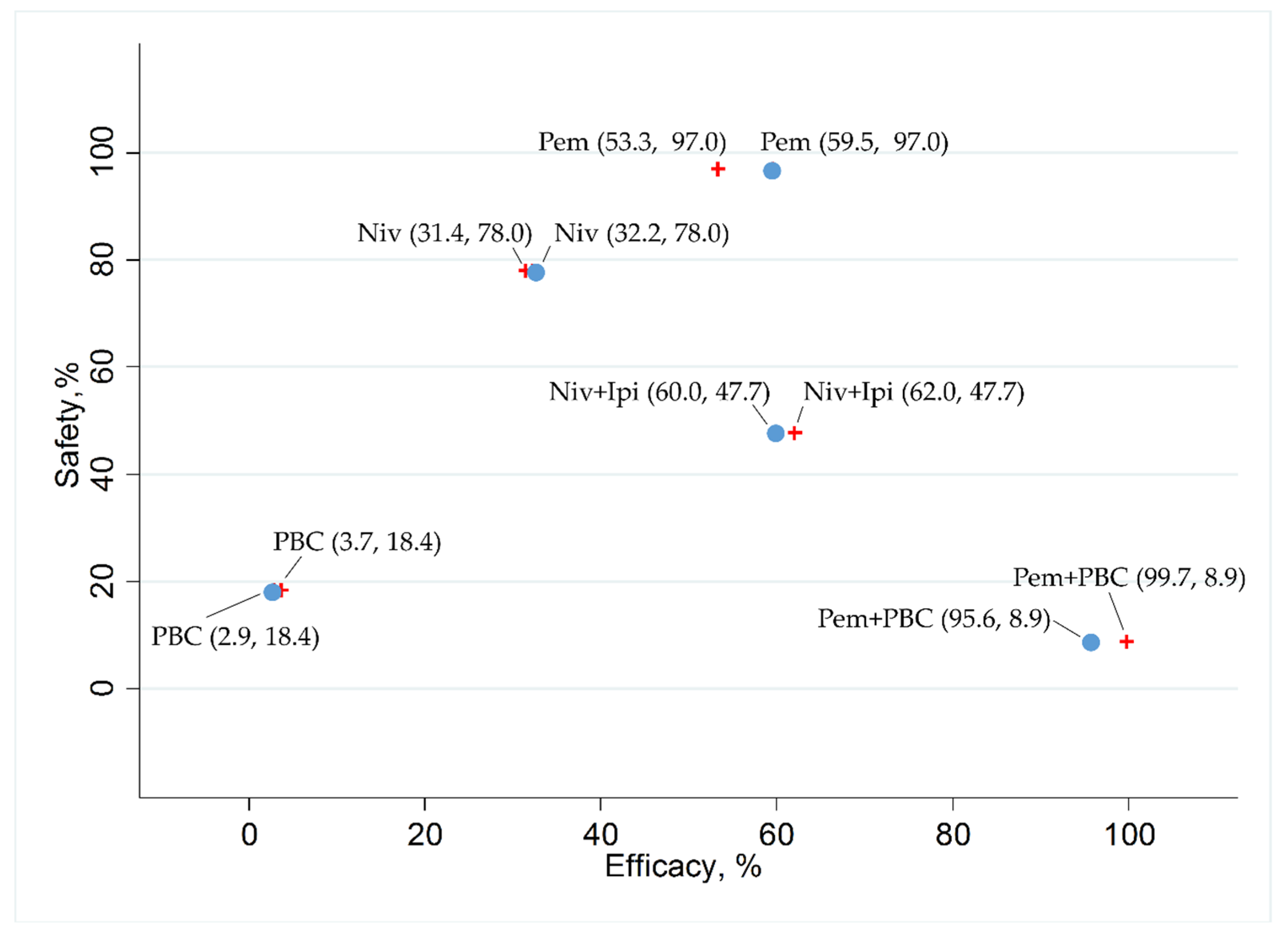
3.7. Ranking Assessment
3.8. Bias Assessment
3.9. Sensitivity Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A
Search Strategies in Pubmed (Searched on Mar 13, 2020)
References
- Nasim, F.; Sabath, B.F.; Eapen, G.A. Lung cancer. Med. Clin. N. Am. 2019, 103, 463–473. [Google Scholar] [CrossRef] [PubMed]
- Arbour, K.; Riely, G.J. Systemic therapy for locally advanced and metastatic non-small cell lung cancer: A review. JAMA 2019, 322, 764–774. [Google Scholar] [CrossRef] [PubMed]
- Duma, N.; Santana-Davila, R.; Molina, J.R. Non- small cell lung cancer: Epidemiology, screening, diagnosis, and treatment. Mayo Clin. Proc. 2019, 94, 1623–1640. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Shroff, G.S.; Viswanathan, C.; Carter, B.W.; Benveniste, M.F.; Truong, M.T.; Sabloff, B.S. Staging lung cancer: Metastasis. Radiol. Clin. N. Am. 2018, 56, 411–418. [Google Scholar] [CrossRef] [PubMed]
- Bironzo, P.; Di Maio, M. A review of guidelines for lung cancer. J. Thorac. Dis. 2018, 10 (Suppl. 13), S1556–S1663. [Google Scholar] [CrossRef] [Green Version]
- Torre, L.A.; Siegel, R.L.; Jemal, A. Lung cancer statistics. Adv. Exp. Med. Biol. 2016, 893, 1–19. [Google Scholar]
- Low, J.L.; Walsh, R.J.; Ang, Y.; Chan, G.; Soo, R.A. The evolving immuno-oncology landscape in advanced lung cancer: First-line treatment of non-small cell lung cancer. Ther. Adv. Med. Oncol. 2019, 11, 1758835919870360. [Google Scholar] [CrossRef]
- Ackermann, C.J.; Reck, M.; Paz-Ares, L.; Barlesi, F.; Califano, R. First-line immune checkpoint blockade for advanced non-small-cell lung cancer: Travelling at the speed of light. Lung Cancer 2019, 134, 245–253. [Google Scholar] [CrossRef]
- Hellmann, M.D.; Paz-Ares, L.; Bernabe Caro, R.; Zurawski, B.; Kim, S.W.; Carcereny Costa, E.; Park, K.; Alexandru, A.; Lupinacci, L.; de la Mora Jimenez, E.; et al. Nivolumab plus ipilimumab in advanced non-small-cell lung cancer. N. Engl. J. Med. 2019, 381, 2020–2031. [Google Scholar] [CrossRef] [PubMed]
- Remon, J.; Esteller, L.; Taus, A. Nivolumab plus ipilimumab combination therapy for the first-line treatment NSCLC: Evidence to date. Cancer Manag. Res. 2019, 11, 4893–4904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- White, I.R. Network meta-analysis. Stata J. 2015, 15, 951–985. [Google Scholar] [CrossRef] [Green Version]
- Jansen, J.P.; Crawford, B.; Bergman, G.; Stam, W. Bayesian meta-analysis of multiple treatment comparisons: An introduction to mixed treatment comparisons. Value Health 2008, 11, 956–964. [Google Scholar] [CrossRef] [Green Version]
- Lumley, T. Network meta-analysis for indirect treatment comparisons. Stat. Med. 2002, 21, 2313–2324. [Google Scholar] [CrossRef]
- Tonin, F.S.; Rotta, I.; Mendes, A.M.; Pontarolo, R. Network meta-analysis: A technique to gather evidence from direct and indirect comparisons. Pharm. Pract. 2017, 15, 943. [Google Scholar] [CrossRef] [Green Version]
- Lu, G.; Ades, A. Combination of direct and indirect evidence in mixed treatment comparisons. Stat. Med. 2004, 23, 3105–3124. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: New York, NY, USA, 2011. [Google Scholar]
- Paz-Ares, L.; Luft, A.; Vicente, D.; Tafreshi, A.; Gümüş, M.; Mazières, J.; Hermes, B.; Çay Şenler, F.; Csőszi, T.; Fülöp, A.; et al. Pembrolizumab plus chemotherapy for squamous non-small-cell lung cancer. N. Engl. J. Med. 2018, 379, 2040–2051. [Google Scholar] [CrossRef]
- Jansen, J.P.; Fleurence, R.; Devine, B.; Itzler, R.; Barrett, A.; Hawkins, N.; Lee, K.; Boersma, C.; Annemans, L.; Cappelleri, J.C. Interpreting indirect treatment comparisons and network meta-analysis for health-care decision making: Report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: Part 1. Value Health 2011, 14, 417–428. [Google Scholar] [CrossRef] [Green Version]
- Hoaglin, D.C.; Hawkins, N.; Jansen, J.P.; Scott, D.A.; Itzler, R.; Cappelleri, J.C.; Boersma, C.; Thompson, D.; Larholt, K.M.; Diaz, M.; et al. Conducting indirect-treatment-comparison and network-meta-analysis studies: Report of the ISPOR Task Force on Indirect Treatment Comparisons Good Research Practices: Part 2. Value Health 2011, 14, 429–437. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bucher, H.C.; Guyatt, G.H.; Griffith, L.E.; Walter, S.D. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J. Clin. Epidemiol. 1997, 50, 683–691. [Google Scholar] [CrossRef]
- Miwa, H.; Igarashi, A.; Teng, L.; Uda, A.; Deguchi, H.; Tango, T. Systematic review with network meta-analysis: Indirect comparison of the efficacy of vonoprazan and proton-pump inhibitors for maintenance treatment of gastroesophageal reflux disease. J. Gastroenterol. 2019, 54, 718–729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, H.; Chi, H.; You, H.; Wang, M.; Zhang, G.; Yang, H.; Li, Q. Indirect-comparison meta-analysis of treatment options for patients with refractory Kawasaki disease. BMC Pediatr. 2019, 19, 158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Busse, W.; Chupp, G.; Nagase, H.; Albers, F.C.; Doyle, S.; Shen, Q.; Bratton, D.J.; Gunsoy, N.B. Anti-IL-5 treatments in patients with severe asthma by blood eosinophil thresholds: Indirect treatment comparison. J. Allergy Clin. Immunol. 2019, 143, 190–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ando, K.; Tanaka, A.; Sagara, H. Comparative efficacy and safety of dupilumab and benralizumab in patients with inadequately controlled asthma: A systematic review. Int. J. Mol. Sci. 2020, 21, 889. [Google Scholar] [CrossRef] [Green Version]
- Dias, S.; Welton, N.J.; Sutton, A.J.; Caldwell, D.M.; Lu, G.; Ades, A.E. Evidence synthesis for decision making 4: Inconsistency in networks of evidence based on randomized controlled trials. Med. Decis. Mak. 2013, 33, 641–656. [Google Scholar] [CrossRef] [Green Version]
- Dias, S.; Welton, N.J.; Sutton, A.J.; Caldwell, D.M.; Lu, G.; Ades, A.E. Evidence synthesis for decision making 3: Heterogeneity–subgroups, meta-regression, bias, and bias-adjustment. Med. Decis. Mak. 2013, 33, 618–640. [Google Scholar] [CrossRef] [Green Version]
- Dias, S.; Sutton, A.J.; Ades, A.E.; Welton, N.J. Evidence synthesis for decision making 2: A generalized linear modeling framework for pairwise and network meta-analysis of randomized controlled trials. Med. Decis. Mak. 2013, 33, 607–617. [Google Scholar] [CrossRef] [Green Version]
- Brooks, S.P.; Roberts, G.O. Convergence assessment techniques for Markov chain Monte Carlo. Stat. Comput. 1998, 8, 319–335. [Google Scholar] [CrossRef]
- Brooks, S.P.; Gelman, A. General methods for monitoring convergence of iterative simulations. J. Comput. Graph. Stat. 1998, 7, 434–455. [Google Scholar]
- Salanti, G.; Ades, A.E.; Ioannidis, J.P. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: An overview and tutorial. J. Clin. Epidemiol. 2011, 64, 163–171. [Google Scholar] [CrossRef]
- Mok, T.; Wu, Y.L.; Kudaba, I.; Kowalski, D.M.; Cho, B.C.; Turna, H.Z.; Castro, G.; Srimuninnimit, V., Jr.; Laktionov, K.K.; Bondarenko, I.; et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised, open-label, controlled, phase 3 trial. Lancet 2019, 393, 1819–1830. [Google Scholar] [CrossRef]
- Gandhi, L.; Rodríguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef]
- Leach, D.R.; Krummel, M.F.; Allison, J.P. Enhancement of antitumor immunity by CTLA-4 blockade. Science 1996, 271, 1734–1736. [Google Scholar] [CrossRef] [Green Version]
- Cameron, F.; Whiteside, G.; Perry, C. Ipilimumab: First global approval. Drugs 2011, 71, 1093–1104. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Hammers, H.; Lipson, E.J. Nivolumab: Targeting PD-1 to bolster antitumor immunity. Future Oncol. 2015, 11, 1307–1326. [Google Scholar] [CrossRef]
- Fulchiero, E.; Jimeno, A. Nivolumab. Drugs Today 2014, 50, 791–802. [Google Scholar] [CrossRef]
- Gunturi, A.; McDermott, D.F. Nivolumab for the treatment of cancer. Expert Opin. Investig. Drugs 2015, 24, 253–260. [Google Scholar] [CrossRef]
- Rajan, A.; Kim, C.; Heery, C.R.; Guha, U.; Gulley, J.L. Nivolumab, anti-programmed death-1 (PD-1) monoclonal antibody immunotherapy: Role in advanced cancers. Hum. Vaccin. Immunother. 2016, 12, 2219–2231. [Google Scholar] [CrossRef] [Green Version]
- Barbee, M.S.; Ogunniyi, A.; Horvat, T.Z.; Dang, T.O. Current status and future directions of the immune checkpoint inhibitors ipilimumab, pembrolizumab, and nivolumab in oncology. Ann. Pharmacother. 2015, 49, 907–937. [Google Scholar] [CrossRef]
- Reck, M.; Borghaei, H.; O’Byrne, K.J. Nivolumab plus ipilimumab in non-small-cell lung cancer. Future Oncol. 2019, 15, 2287–2302. [Google Scholar] [CrossRef]
- Selby, M.J.; Engelhardt, J.J.; Johnston, R.J.; Lu, L.S.; Han, M.; Thudium, K.; Yao, D.; Quigley, M.; Valle, J.; Wang, C.; et al. Preclinical development of ipilimumab and nivolumab combination immunotherapy: Mouse tumor models, in vitro functional studies, and Cynomolgus macaque toxicology. PLoS ONE 2016, 11, e0161779. [Google Scholar]
- Carreau, N.A.; Pavlick, A.C. Nivolumab and ipilimumab: Immunotherapy for treatment of malignant melanoma. Future Oncol. 2019, 15, 349–358. [Google Scholar] [CrossRef]
- Gao, X.; McDermott, D.F. Ipilimumab in combination with nivolumab for the treatment of renal cell carcinoma. Expert Opin. Biol. Ther. 2018, 18, 947–957. [Google Scholar] [CrossRef]
- Spain, L.; Larkin, J. Combination immune checkpoint blockade with ipilimumab and nivolumab in the management of advanced melanoma. Expert Opin. Biol. Ther. 2016, 16, 389–396. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Names | Key Inclusion Criteria |
|---|---|
| KEYNOTE-189 | 18 years of age or older |
| Metastatic non-squamous NSCLC with at least one measurable lesion Without a EGFR sensitive mutation or ALK fusion gene translocation | |
| No previous systemic anticancer treatment | |
| Performance status rank of 0 or 1 | |
| KEYNOTE-407 | 18 years of age or older |
| Stage IV squamous cell carcinoma with at least one measurable lesion | |
| No previous systemic anticancer treatment | |
| Performance status rank of 0 or 1 | |
| KEYNOTE-042 | 18 years of age or older |
| Locally advanced or metastatic NSCLC with at least one measurable lesion Without a EGFR sensitive mutation or ALK fusion gene translocation | |
| No previous systemic anticancer treatment | |
| Performance status rank of 0 or 1 | |
| Having a PD-L1 expression proportion of 1% or greater. | |
| CheckMata 227 | 18 years of age or older |
| Squamous or non-squamous Stage IV or recurrent NSCLC Without a EGFR sensitive mutation or ALK fusion gene translocation | |
| No previous systemic anticancer treatment | |
| Performance status rank of 0 or 1 |
| Study Name (Year of Publication) | Treatment Arms | N | Age—yrs. Median (range) | Female Sex No. (%) | ECOG PS No. (%) | Histologic Type No. (%) | PD-L1 Status |
|---|---|---|---|---|---|---|---|
| KEYNOTE-189 (2018) | Pembrolizumab 200 mg/body e3w plus platinum-based chemotherapy | 410 | 65 (34–84) | 156 (38.0) | PS0: 186 (45.4) PS1: 221 (53.9) PS2: 1 (0.2) Missing: 2 (0.5) | Adenocarcinoma 394 (96.1) | ≥1% 260 (63.4) |
| Other 16 (3.9) | ≥50% 132 (32.2) | ||||||
| Platinum-based chemotherapy | 206 | 63.5 (34–84) | 97 (47.1) | PS0: 80 (38.8) | Adenocarcinoma 198 (96.1) | ≥1% 128 (62.1) | |
| PS1: 125 (60.7) | Other 8 (3.6) | ≥50% 70 (34.0) | |||||
| Missing: 1 (0.5) | |||||||
| Total, 616 | |||||||
| KEYNOTE-407 (2018) | Pembrolizumab 200 mg/body e3w plus platinum-based chemotherapy | 278 | 65 (29–87) | 58 (20.9) | PS0: 73 (26.3) | Squamous: 272 (97.8) | ≥1% 176 (63.3) |
| PS1: 205 (73.7) | Adenosquamous: 6 (2.2) | ≥50% 73 (26.3) | |||||
| Platinum-based chemotherapy | 281 | 65 (36–88) | 46 (16.4) | PS0: 90 (32.0) | Squamous: 274 (97.5) | ≥1% 177 (63.0) | |
| PS1: 191 (68.0) | Adenosquamous: 7 (2.5) | ≥50% 73 (26.0) | |||||
| Total, 559 | |||||||
| Pembrolizumab 200 mg/body e3w | 637 | 63.0 (57.0–69.0) | 187 (29%) | PS0: 198 (31) | Squamous: 243 (38) | ≥1% 637 (100) | |
| PS1: 439 (69) | Non-squamous: 394 (62) | ≥50% 299 (46.9) | |||||
| Platinum-based chemotherapy | 637 | 63.0 (57.0–69.0) | 185 (29%) | PS0: 192 (30) | Squamous: 249 (39) | ≥1% 637 (100.0) | |
| PS1: 445(70) | Non-squamous: 388(61) | ≥50% 300 (47.1) | |||||
| Total, 1274 | |||||||
| CheckMate 227 (2019) | Nivolumab 3 mg/kg e2w plus ipilimumab 1 mg/kg e6w | 583 | 64 (26–87) | 190 (32.6) | PS0: 204 (35.0) | Squamous: 163 (28.0) | ≥1% 396 (67.9) |
| PS1: 377 (64.7) | Non-squamous: 419 (71.9) | ≥50% 205 (35.2) | |||||
| Other or missing: 2 (0.3) | Missing data: 1 (0.2) | ||||||
| Nivolumab 240 mg/body e2w | 396 | 64 (27–85) | 124 (31.3) | PS0: 142 (35.9) | Squamous: 117 (29.5) | ≥1% 396 (100.0) | |
| PS1: 252 (63.6) | Non-squamous: 279 (70.5) | ≥50% 214 (54.0) | |||||
| Other or missing: 2 (0.5) | Missing data: 0 (0) | ||||||
| Platinum based chemotherapy | 583 | 64 (29–87) | 198 (34.0) | PS0: 191 (32.8) | Squamous: 162 (27.8) | ≥1% 397 (68.1) | |
| PS1: 386 (66.2) | Non-squamous: 421 (72.2) | ≥50% 192 (32.9) | |||||
| Other or missing: 6 (1.0) | Missing data: 0 (0) | ||||||
| Total, 1562 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ando, K.; Kishino, Y.; Homma, T.; Kusumoto, S.; Yamaoka, T.; Tanaka, A.; Ohmori, T.; Ohnishi, T.; Sagara, H. Nivolumab plus Ipilimumab versus Existing Immunotherapies in Patients with PD-L1-Positive Advanced Non-Small Cell Lung Cancer: A Systematic Review and Network Meta-Analysis. Cancers 2020, 12, 1905. https://doi.org/10.3390/cancers12071905
Ando K, Kishino Y, Homma T, Kusumoto S, Yamaoka T, Tanaka A, Ohmori T, Ohnishi T, Sagara H. Nivolumab plus Ipilimumab versus Existing Immunotherapies in Patients with PD-L1-Positive Advanced Non-Small Cell Lung Cancer: A Systematic Review and Network Meta-Analysis. Cancers. 2020; 12(7):1905. https://doi.org/10.3390/cancers12071905
Chicago/Turabian StyleAndo, Koichi, Yasunari Kishino, Tetsuya Homma, Sojiro Kusumoto, Toshimitsu Yamaoka, Akihiko Tanaka, Tohru Ohmori, Tsukasa Ohnishi, and Hironori Sagara. 2020. "Nivolumab plus Ipilimumab versus Existing Immunotherapies in Patients with PD-L1-Positive Advanced Non-Small Cell Lung Cancer: A Systematic Review and Network Meta-Analysis" Cancers 12, no. 7: 1905. https://doi.org/10.3390/cancers12071905