Interleukin-6 and Lymphocyte Count Associated and Predicted the Progression of Frailty Syndrome in Prostate Cancer Patients Undergoing Antiandrogen Therapy


 ,
, 
Abstract
:1. Introduction
2. Results
2.1. Characteristics of the Study Population
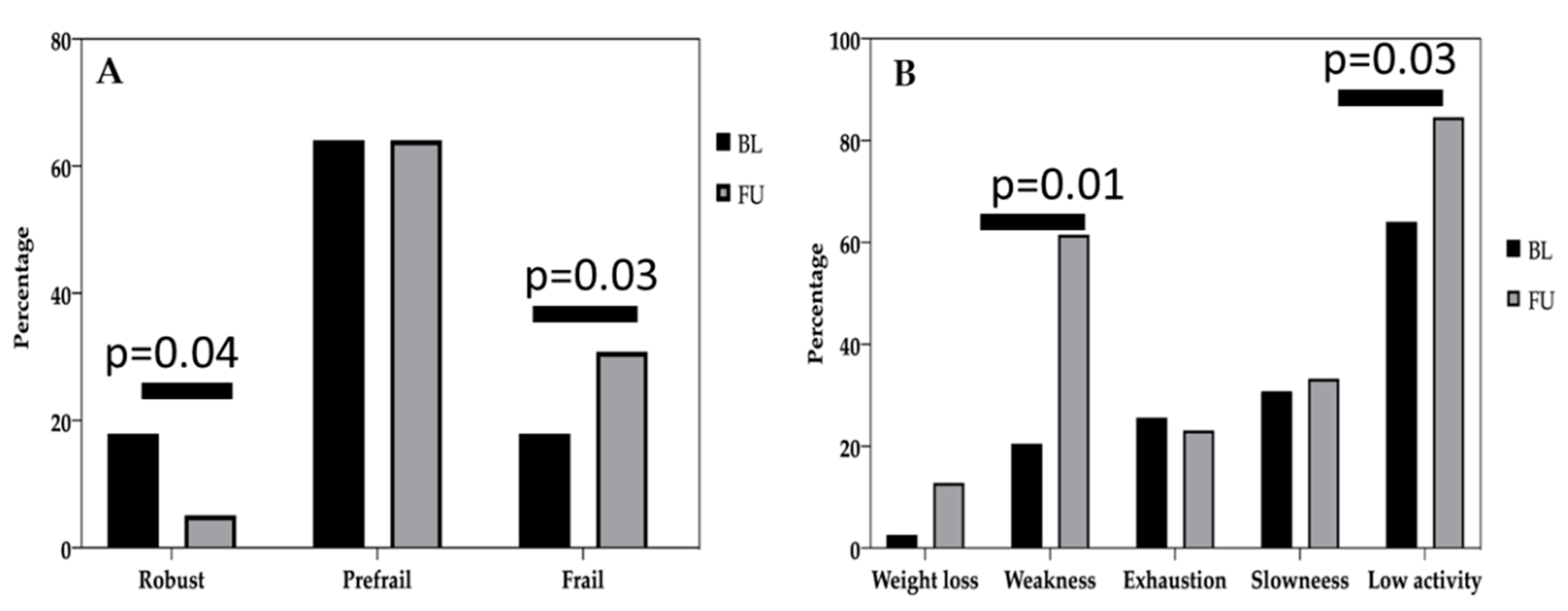
2.2. Evaluation of Frailty Syndrome in the Study Sample
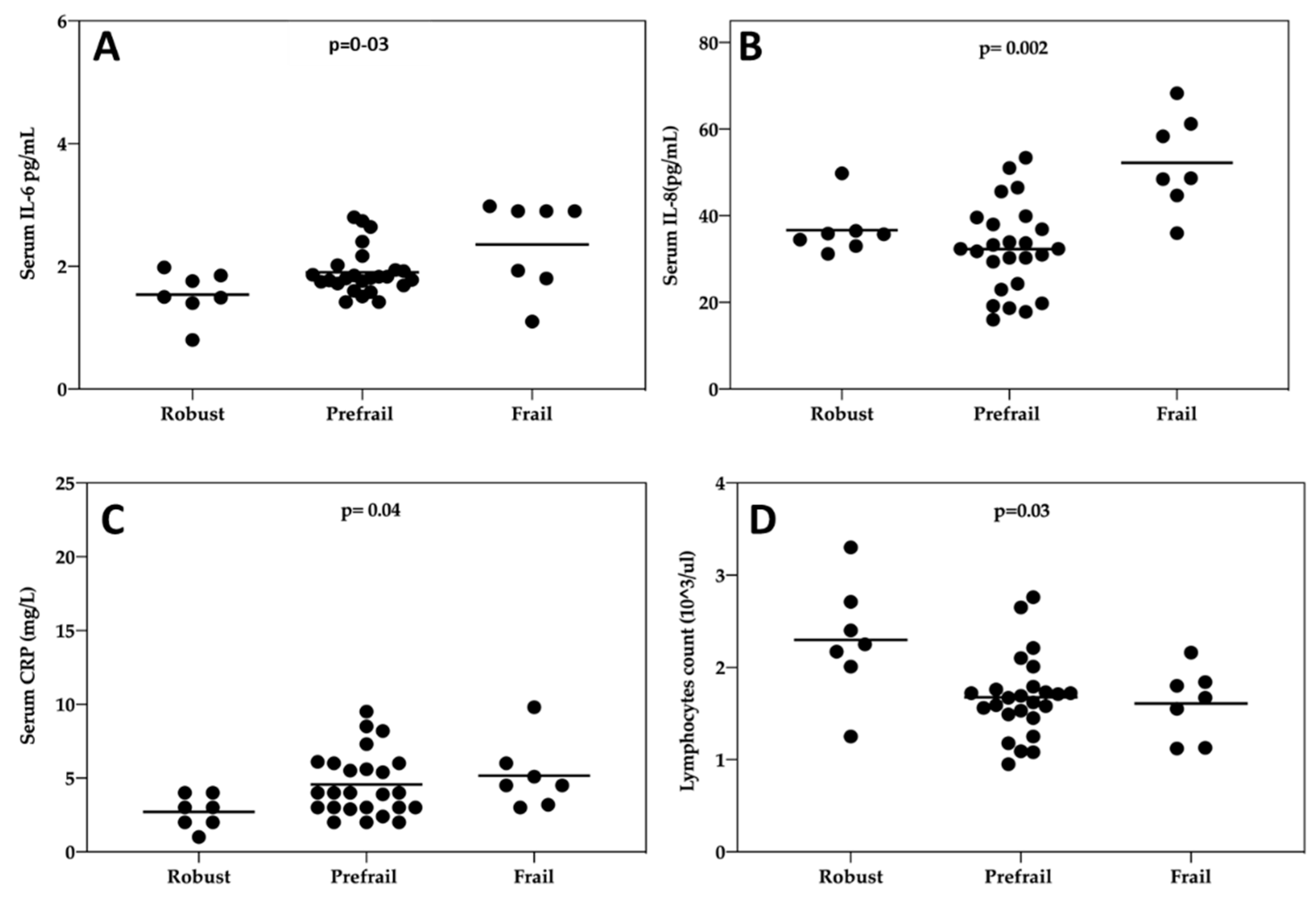
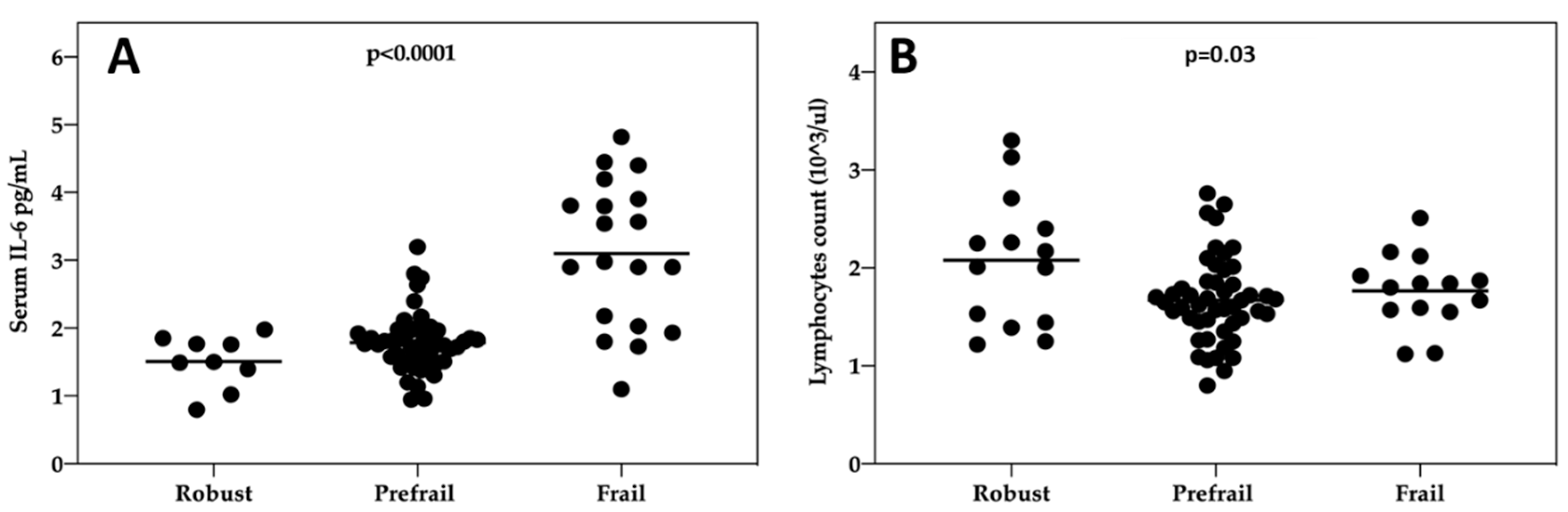
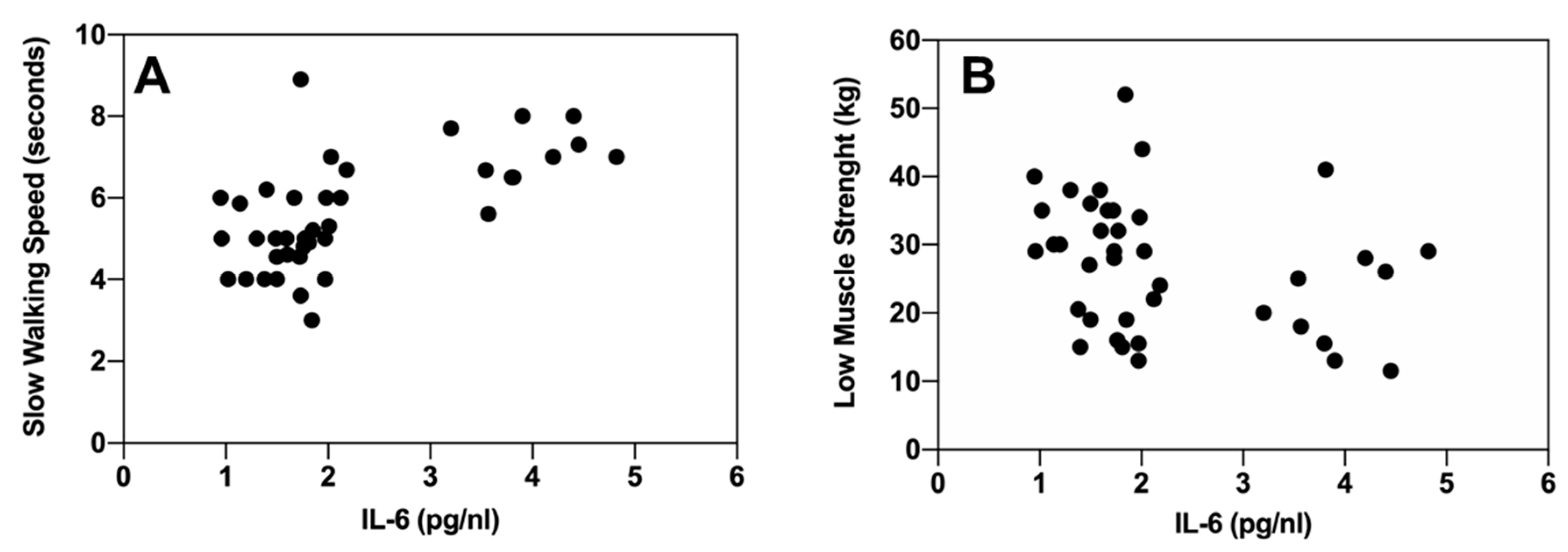
2.3. Association Between Inflammatory Markers and Frailty Syndrome
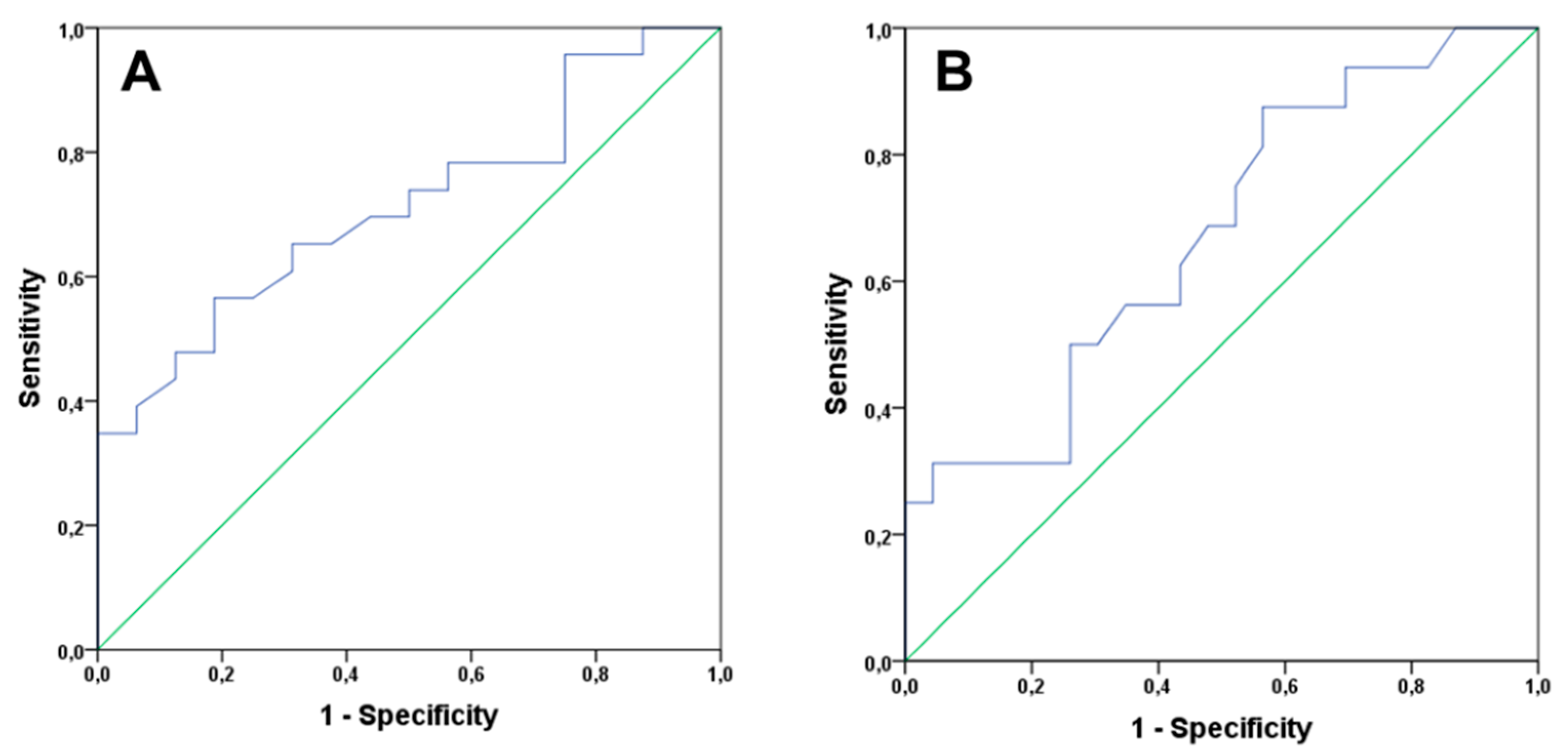
2.4. Analysis of Clinical Variables and Inflammatory Markers as Predictors of Progression of Frailty Syndrome
3. Discussion
4. Materials and Methods
4.1. Measurement of Inflammatory Markers
4.2. Measurement of Hematological and Biochemical Markers
4.3. Sociodemographic and Clinical Variables
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer Incidence and Mortality Patterns in Europe: Estimates for 40 Countries and 25 Major Cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef] [PubMed]
- Caumont, F.; Conti, G.; Hurwitz, L.M.; Kuo, C.; Levie, K.E.; Badiozamani, K.; Frankel, J.K.; Flores, J.P.; Brand, T.C.; Chaurasia, A.; et al. A prospective analysis of health-related quality of life in intermediate and high-risk prostate cancer patients managed with intensity modulated radiation therapy, with vs. without hormonal therapy. In Urologic Oncology: Seminars and Original Investigations; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar] [CrossRef]
- Kim, D.; Lee, J.; Kim, K.; Hong, N.; Kim, J.; Hah, Y.; Koo, K.; Kim, J.; Cho, K. Effect of androgen-deprivation therapy on bone mineral density in patients with prostate cancer: A systematic review and meta-analysis. J. Clin. Med. 2019, 8, 113. [Google Scholar] [CrossRef] [Green Version]
- Cornford, P.; Bellmunt, J.; Bolla, M.; Briers, E.; De Santis, M.; Gross, T.; Henry, A.M.; Joniau, S.; Lam, T.B.; Mason, M.D.; et al. EAU-ESTRO-SIOG guidelines on prostate cancer, part II: Treatment of relapsing, metastatic, and castration-resistant prostate cancer. Eur. Urol. 2017, 71, 630–642. [Google Scholar] [CrossRef] [PubMed]
- Dellis, A.; Zagouri, F.; Liontos, M.; Mitropoulos, D.; Bamias, A.; Papatsoris, A.G. Management of advanced prostate cancer: A systematic review of existing guidelines and recommendations. Cancer Treat. Rev. 2019, 73, 54–61. [Google Scholar] [CrossRef] [PubMed]
- Chang, D.; Joseph, D.J.; Ebert, M.A.; Galvão, D.A.; Taaffe, D.R.; Denham, J.W.; Newton, R.U.; Spry, N.A. Effect of androgen deprivation therapy on muscle attenuation in men with prostate cancer. J. Med. Imag. Radiat. Oncol. 2014, 58, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Winters-Stone, K.M.; Moe, E.; Graff, J.N.; Dieckmann, N.F.; Stoyles, S.; Borsch, C.; Alumkal, J.J.; Amling, C.L.; Beer, T.M. Falls and frailty in prostate cancer survivors: Current, past and never users of androgen deprivation therapy. J. Am. Geriatr. Soc. 2017, 65, 1414–1419. [Google Scholar] [CrossRef]
- Bylow, K.; Mohile, S.G.; Stadler, W.M.; Dale, W. Does androgen-deprivation therapy accelerate the development of frailty in older men with prostate cancer? A conceptual Review. Cancer 2007, 110, 2604–2613. [Google Scholar] [CrossRef]
- Hsu, B.; Cumming, R.G.; Handelsman, D.J. Testosterone, frailty and physical function in older men. Expert Rev. Endocrinol. Metab. 2018, 13, 159–165. [Google Scholar] [CrossRef]
- Cheung, A.S.; Hoermann, R.; Dupuis, P.; Joon, D.L.; Zajac, J.D.; Grossmann, M. Relationships between insulin resistance and frailty with body composition and testosterone in men undergoing androgen deprivation therapy for prostate cancer. Eur. J. Endocrinol. 2016, 175, 229–237. [Google Scholar] [CrossRef] [Green Version]
- Chiang, J.M.; Kaysen, G.A.; Segal, M.; Chertow, G.M.; Delgado, C.; Johansen, K.L. Low testosterone is associated with frailty, muscle wasting and physical dysfunction among men receiving hemodialysis: A longitudinal analysis. Nephrol. Dial. Transplant. 2019, 34, 802–810. [Google Scholar] [CrossRef]
- Saad, F.; Röhrig, G.; Von Haehling, S.; Traish, A. Testosterone deficiency and testosterone treatment in older men. Gerontology 2017, 63, 144–156. [Google Scholar] [CrossRef] [PubMed]
- Molina-Garrido, M.J.; Guillén-Ponce, C. Use of geriatric assessment and screening tools of frailty in elderly patients with prostate cancer. Review. Aging Male 2017, 20, 102–109. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2004, 59, M255–M263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Mareschal, J.; Weber, K.; Rigoli, P.; Biason, E.; Frambati, L.; Gotteland, C.; Zilli, T.; Pichard, C.; Miralbell, R. The ADAPP trial: A two-year longitudinal multidisciplinary intervention study for prostate cancer frail patients on androgen deprivation associated to curative radiotherapy. Acta Oncol. 2017, 56, 569–574. [Google Scholar] [CrossRef]
- Droz, J.-P.; Albrand, G.; Gillessen, S.; Hughes, S.; Mottet, N.; Oudard, S.; Payne, H.; Puts, M.; Zulian, G.; Balducci, L.; et al. Management of prostate cancer in elderly patients: Recommendations of a task force of the international society of geriatric oncology. Eur. Urol. 2017, 72, 521–531. [Google Scholar] [CrossRef]
- Breul, J.; Lundström, E.; Purcea, D.; Venetz, W.P.; Cabri, P.; Dutailly, P.; Goldfischer, E.R. Efficacy of testosterone suppression with sustained-release triptorelin in advanced prostate cancer. Adv. Ther. 2017, 34, 513–523. [Google Scholar] [CrossRef] [Green Version]
- Klotz, L.; Breau, R.H.; Collins, L.L.; Gleave, M.E.; Pickles, T.; Pouliot, F.; Saad, F. Maximal testosterone suppression in the management of recurrent and metastatic prostate cancer. J. Can. Urol. Assoc. 2017, 11, 16–23. [Google Scholar] [CrossRef]
- Perachino, M.; Cavalli, V.; Bravi, F. Testosterone levels in patients with metastatic prostate cancer treated with luteinizing hormone-releasing hormone therapy: Prognostic significance? BJU Int. 2010, 105, 648–651. [Google Scholar] [CrossRef]
- Mohamad, N.V.; Wong, S.K.; Wan Hasan, W.N.; Jolly, J.J.; Nur-Farhana, M.F.; Ima-Nirwana, S.; Chin, K.Y. The Relationship between circulating testosterone and inflammatory cytokines in men. Aging Male 2019, 22, 129–140. [Google Scholar] [CrossRef]
- Maggio, M.; Basaria, S.; Ceda, G.P.; Ble, A.; Ling, S.M.; Bandinelli, S.; Valenti, G.; Ferrucci, L. The relationship between testosterone and molecular markers of inflammation in older men. J. Endocrinol. Invest. 2005, 28, 116–119. [Google Scholar] [PubMed]
- Fahey, J.L.; Schnelle, J.F.; Boscardin, J.; Thomas, J.K.; Gorre, M.E.; Aziz, N.; Sadeghi, H.; Nishanian, P. Distinct categories of immunologic changes in frail elderly. Mech. Ageing Dev. 2000, 115, 1–20. [Google Scholar] [CrossRef]
- Franceschi, C.; Bonafè, M.; Valensin, S. Human immunosenescence: The prevailing of innate immunity, the failing of clonotypic immunity, and the filling of Immunological space. Vaccine 2000, 18, 1717–1720. [Google Scholar] [CrossRef]
- Monti, D.; Ostan, R.; Borelli, V.; Castellani, G.; Franceschi, C. Inflammaging and human longevity in the omics era. Mech. Ageing Dev. 2017, 165, 129–138. [Google Scholar] [CrossRef]
- Al Saedi, A.; Feehan, J.; Phu, S.; Duque, G. Current and emerging biomarkers of frailty in the elderly. Clin. Interv. Aging 2019, 14, 389–398. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Liu, S.; Leng, S.X. Chronic low-grade inflammatory phenotype (CLIP) and senescent immune dysregulation. Clin. Ther. 2019, 41, 400–409. [Google Scholar] [CrossRef] [Green Version]
- Kane, A.E.; Sinclair, D.A. Frailty biomarkers in humans and rodents: Current approaches and future advances. Mech. Ageing Dev. 2019, 180, 117–128. [Google Scholar] [CrossRef]
- Soysal, P.; Stubbs, B.; Lucato, P.; Luchini, C.; Solmi, M.; Peluso, R.; Sergi, G.; Isik, A.T.; Manzato, E.; Maggi, S.; et al. Inflammation and frailty in the elderly: A systematic review and meta-analysis. Ageing Res. Rev. 2016, 31, 1–8. [Google Scholar] [CrossRef]
- Velissaris, D.; Pantzaris, N.; Koniari, I.; Koutsogiannis, N.; Karamouzos, V.; Kotroni, I.; Skroumpelou, A.; Ellul, J. C-reactive protein and frailty in the elderly: A literature review. J. Clin. Med. Res. 2017, 9, 461–465. [Google Scholar] [CrossRef] [Green Version]
- Ershler, W.B.; Keller, E.T. Age-associated increased interleukin-6 gene expression, late-life diseases, and frailty. Annu. Rev. Med. 2000, 51, 245–270. [Google Scholar] [CrossRef]
- Nguyen, D.P.; Li, J.; Tewari, A.K. Inflammation and prostate cancer: The role of interleukin 6 (IL-6). BJU Int. 2014, 113, 986–992. [Google Scholar] [CrossRef] [PubMed]
- Rani, A.; Dasgupta, P.; Murphy, J.J. Prostate cancer: The role of inflammation and chemokines. Am. J. Pathol. 2019, 189, 2119–2137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Royuela, M.; Rodríguez-Berriguete, G.; Fraile, B.; Paniagua, R. TNF-Alpha/IL-1/NF-KappaB transduction pathway in human cancer prostate. Histol. Histopathol. 2008, 23, 1279–1290. [Google Scholar] [CrossRef]
- Xu, H.; Ding, Q.; Jiang, H.W. Genetic polymorphism of interleukin-1A (IL-1A), IL-1B, and IL-1 receptor antagonist (IL-1RN) and prostate cancer risk. Asian Pacific J. Cancer Prev. 2014, 15, 8741–8747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Waugh, D.J.J.; Wilson, C. The interleukin-8 pathway in cancer. Clin. Cancer Res. 2008, 14, 6735–6741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pirtskhalaishvili, G.; Nelson, J.B. Endothelium-derived factors as paracrine mediators of prostate cancer progression. Prostate 2000, 44, 77–87. [Google Scholar] [CrossRef]
- Gillessen, S.; Attard, G.; Beer, T.M.; Beltran, H.; Bjartell, A.; Bossi, A.; Briganti, A.; Bristow, R.G.; Chi, K.N.; Clarke, N.; et al. Management of patients with advanced prostate cancer: Report of the advanced prostate cancer consensus conference 2019. Eur. Urol. 2020, 77, 508–547. [Google Scholar] [CrossRef]
- Rhee, H.; Gunter, J.H.; Heathcote, P.; Ho, K.; Stricker, P.; Corcoran, N.M.; Nelson, C.C. Adverse effects of androgen-deprivation therapy in prostate cancer and their management. BJU Int. 2015, 115, 3–13. [Google Scholar] [CrossRef]
- Cardoso, A.L.; Fernandes, A.; Aguilar-Pimentel, J.A.; de Angelis, M.H.; Guedes, J.R.; Brito, M.A.; Ortolano, S.; Pani, G.; Athanasopoulou, S.; Gonos, E.S.; et al. Towards frailty biomarkers: Candidates from genes and pathways regulated in aging and age-related diseases. Ageing Res. Rev. 2018, 47, 214–277. [Google Scholar] [CrossRef]
- Calvani, R.; Marini, F.; Cesari, M.; Tosato, M.; Picca, A.; Anker, S.D.; von Haehling, S.; Miller, R.R.; Bernabei, R.; Landi, F.; et al. Biomarkers for physical frailty and sarcopenia. Aging Clin. Exp. Res. 2017, 29, 29–34. [Google Scholar] [CrossRef]
- Fernández-Garrido, J.; Ruiz-Ros, V.; Buigues, C.; Navarro-Martinez, R.; Cauli, O. Clinical features of prefrail older individuals and emerging peripheral biomarkers: A systematic review. Arch. Gerontol. Geriatr. 2014, 59, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Trigunaite, A.; Dimo, J.; Jørgensen, T.N. Suppressive effects of androgens on the immune system. Cell Immunol. 2015, 294, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Roved, J.; Westerdahl, H.; Hasselquist, D. Sex differences in immune responses: Hormonal effects, antagonistic selection, and evolutionary consequences. Horm. Behav. 2017, 88, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Bruunsgaard, H.; Pedersen, M.; Pedersen, B.K. Aging and proinflammatory cytokines. Curr. Opin. Hematol. 2001, 8, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Lehrer, S.; Diamond, E.J.; Mamkine, B.; Droller, M.J.; Stone, N.N.; Stock, R.G. C-Reactive protein is significantly associated with prostate-specific antigen and metastatic disease in prostate cancer. BJU Int. 2005, 95, 961–962. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Russell, M.R.; Shahriari, K.; Jernigan, D.L.; Lioni, M.I.; Garcia, F.U.; Fatatis, A. Interleukin-1β promotes skeletal colonization and progression of metastatic prostate cancer cells with neuroendocrine features. Cancer Res. 2013, 73, 3297–3305. [Google Scholar] [CrossRef] [Green Version]
- Fulop, T.; Witkowski, J.M.; Olivieri, F.; Larbi, A. The integration of inflammaging in age-related diseases. Semin. Immunol. 2018, 40, 17–35. [Google Scholar] [CrossRef]
- Banzola, I.; Mengus, C.; Wyler, S.; Hudolin, T.; Manzella, G.; Chiarugi, A.; Boldorini, R.; Sais, G.; Schmidli, T.S.; Chiffi, G.; et al. Expression of indoleamine 2,3-dioxygenase induced by IFN-γ and TNF-α as potential biomarker of prostate cancer progression. Front. Immunol. 2018, 9. [Google Scholar] [CrossRef] [Green Version]
- Culig, Z.; Puhr, M. Interleukin-6 and prostate cancer: Current developments and unsolved questions. Mol. Cell. Endocrinol. 2018, 462, 25–30. [Google Scholar] [CrossRef]
- Baylis, D.; Bartlett, D.B.; Syddall, H.E.; Ntani, G.; Gale, C.R.; Cooper, C.; Lord, J.M.; Sayer, A.A. Immune-endocrine biomarkers as predictors of frailty and mortality: A 10-year longitudinal study in community-dwelling older people. Age 2013, 35, 963–971. [Google Scholar] [CrossRef]
- Leng, S.X.; Xue, Q.L.; Tian, J.; Huang, Y.; Yeh, S.H.; Fried, L.P. Associations of neutrophil and monocyte counts with frailty in community-dwelling disabled older women: Results from the Women’s Health and Aging Studies, I. Exp. Gerontol. 2009, 44, 511–516. [Google Scholar] [CrossRef] [PubMed]
- Murphy, A.J.; Watsford, M.L. The effect of walking training on respiratory function and performance in older females. Int. Sport. J. 2005, 6, 171–184. [Google Scholar]
- Lin, E.Y.; Pollard, J.W. Tumor-associated macrophages press the angiogenic switch in breast cancer. Cancer Res. 2007, 67, 5064–5066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavassani, K.A.; Meza, R.J.; Habiel, D.M.; Chen, J.F.; Montes, A.; Tripathi, M.; Martins, G.A.; Crother, T.R.; You, S.; Hogaboam, C.M.; et al. Circulating monocytes from prostate cancer patients promote invasion and motility of epithelial cells. Cancer Med. 2018, 7, 4639–4649. [Google Scholar] [CrossRef] [PubMed]
- Langmann, G.A.; Perera, S.; Ferchak, M.A.; Nace, D.A.; Resnick, N.M.; Greenspan, S.L. Inflammatory markers and frailty in long-term care residents. J. Am. Geriatr. Soc. 2017, 65, 1777–1783. [Google Scholar] [CrossRef]
- Li, H.; Manwani, B.; Leng, S.X. Frailty, inflammation, and immunity. Aging Dis. 2011, 2, 466–473. [Google Scholar]
- Darvin, K.; Randolph, A.; Ovalles, S.; Halade, D.; Breeding, L.; Richardson, A.; Espinoza, S.E. Plasma protein biomarkers of the geriatric syndrome of frailty. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2014, 69, 182–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semmarath, W.; Seesen, M.; Yodkeeree, S.; Sapbamrer, R.; Ayood, P.; Malasao, R.; Siviroj, P.; Limtrakul, P. The association between frailty indicators and blood-based biomarkers in early-old community dwellers of Thailand. Int. J. Environ. Res. Public Health 2019, 16, 3457. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Maxwell, C.A.; Yu, F. Biological processes and biomarkers related to frailty in older adults: A state-of-the-science literature review. Biol. Res. Nurs. 2019, 21, 80–106. [Google Scholar] [CrossRef]
- Fougère, B.; Boulanger, E.; Nourhashémi, F.; Guyonnet, S.; Cesari, M. Chronic inflammation: Accelerator of biological aging. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2017, 72, 1218–1225. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Liu, Z.; Wang, Y.; Wang, Z.; Shi, J.; Xie, X.; Jin, L.; Chu, X.; Wang, X. C-reactive protein, frailty and overnight hospital admission in elderly individuals: A population-based study. Arch. Gerontol. Geriatr. 2016, 64, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Evans, W.J.; Paolisso, G.; Abbatecola, A.M.; Corsonello, A.; Bustacchini, S.; Strollo, F.; Lattanzio, F. Frailty and muscle metabolism dysregulation in the elderly. Biogerontology 2010, 11, 527–536. [Google Scholar] [CrossRef] [PubMed]
- Marzetti, E.; Calvani, R.; Bernabei, R.; Leeuwenburgh, C. Apoptosis in skeletal myocytes: A potential target for interventions against sarcopenia and physical frailty—A mini-review. Gerontology 2012, 58, 99–106. [Google Scholar] [CrossRef]
- Marcos-Pérez, D.; Sánchez-Flores, M.; Maseda, A.; Lorenzo-López, L.; Millán-Calenti, J.C.; Gostner, J.M.; Fuchs, D.; Pásaro, E.; Laffon, B.; Valdiglesias, V. Frailty in older adults is associated with plasma concentrations of inflammatory mediators but not with lymphocyte subpopulations. Front. Immunol. 2018, 9, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Núñez, J.; Sastre, C.; D’Ascoli, G.; Ruiz, V.; Bonanad, C.; Miñana, G.; Valero, E.; Garcia-Blas, S.; Mollar, A.; Villaescusa, A.; et al. Relation of low lymphocyte count to frailty and its usefulness as a prognostic biomarker in patients >65 years of age with acute coronary syndrome. Am. J. Cardiol. 2020, 125, 1033–1038. [Google Scholar] [CrossRef]
- Binkley, N.; Krueger, D.; Buehring, B. What’s in a name revisited: Should osteoporosis and sarcopenia be considered components of ‘dysmobility syndrome? ’ Osteoporos. Int. 2013, 24, 2955–2959. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Porter Starr, K.N.; McDonald, S.R.; Bales, C.W. Obesity and physical frailty in older adults: A scoping review of lifestyle intervention trials. J. Am. Med. Dir. Assoc. 2014, 15, 240–250. [Google Scholar] [CrossRef] [Green Version]
- Smith, M.R.; Saad, F.; Egerdie, B.; Sieber, P.R.; Tammela, T.L.; Ke, C.; Leder, B.Z.; Goessl, C.; Smith, M.R.; Saad, F.; et al. Sarcopenia during androgen-deprivation therapy for prostate cancer. J. Clin. Oncol. 2012, 30, 3271–3276. [Google Scholar] [CrossRef] [Green Version]
- Hulsegge, G.; Herber-Gast, G.C.M.; Spijkerman, A.M.W.; Susan, H.; Picavet, J.; van der Schouw, Y.T.; Bakker, S.J.L.; Gansevoort, R.T.; Dollé, M.E.T.; Smit, H.A.; et al. Obesity and age-related changes in Markers of oxidative stress and inflammation across four generations. Obesity 2016, 24, 1389–1396. [Google Scholar] [CrossRef] [Green Version]
- Picca, A.; Ponziani, F.R.; Calvani, R.; Marini, F.; Biancolillo, A.; Coelho-Junior, H.J.; Gervasoni, J.; Primiano, A.; Putignani, L.; Del Chierico, F.; et al. Gut microbial, inflammatory and metabolic signatures in older people with physical frailty and sarcopenia: Results from the BIOSPHERE Study. Nutrients 2020, 12, 65. [Google Scholar] [CrossRef] [Green Version]
- Handforth, C.; Clegg, A.; Young, C.; Simpkins, S.; Seymour, M.T.; Selby, P.J.; Young, J. The prevalence and outcomes of frailty in older cancer patients: A systematic review. Ann. Oncol. 2015, 26, 1091–1101. [Google Scholar] [CrossRef]
- Radloff, L.S. The CES-D scale: A self-report depression scale for research in the general population. Appl. Psychol. Meas. 1977, 1, 385–401. [Google Scholar] [CrossRef]
- Ottenbacher, K.J.; Branch, L.G.; Ray, L.; Gonzales, V.A.; Peek, M.K.; Hinman, M.R. The reliability of upper- and lower-extremity strength testing in a community survey of older adults. Arch. Phis. Med. Rehabil. 2002, 83, 1423–1427. [Google Scholar] [CrossRef] [PubMed]
- Guralnik, J.; Simonsick, E.; Ferrucci, L.; Glynn, R.; Berkman, L.; Blazer, D.; Scherr, P.; Wallace, R. A short physical performance battery assessing lower extremity function: Association with self-reported Disability and prediction of mortality and nursing home admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Category | Variation | n | % |
|---|---|---|---|
| Marital status | Married | 34 | 87.2 |
| Widower | 1 | 2.6 | |
| Divorced | 3 | 7.7 | |
| Others | 1 | 2.6 | |
| Cohabitation status | Single | 4 | 10.3 |
| With partner | 28 | 71.8 | |
| With family | 7 | 17.9 | |
| Educational level | Without studies | 7 | 17.9 |
| Primary | 17 | 43.6 | |
| Secondary | 9 | 23.1 | |
| University | 6 | 15.4 | |
| Previous prostatectomy | Yes | 13 | 33.3 |
| No | 26 | 66.7 | |
| Metastases | Yes | 8 | 23.1 |
| No | 31 | 76.9 | |
| ADT treatment | Leuprorelin | 10 | 25.7 |
| Triptorelin | 29 | 74.3 | |
| NCCN risk score in PCa diagnoses | Low | 11 | 28.2 |
| Intermediate | 8 | 20.5 | |
| High | 12 | 30.8 | |
| Metastatic | 8 | 20.5 | |
| Gleason score | 5 | 2 | 5.1 |
| 6 | 8 | 20.5 | |
| 7 | 17 | 43.6 | |
| 8 | 8 | 20.5 | |
| 9 | 4 | 10.3 | |
| Ability to perform daily activities (Barthel index) | 90 | 6 | 15.4 |
| 95 | 9 | 23.1 | |
| 100 | 24 | 61.5 | |
| Charlson Comorbidity Index | <4 | 22 | 59 |
| ≥4 | 16 | 41 |
| Analytical Parameters at Baseline | Frailty Progression at Follow-Up (N = 23) | No Frailty Progression at Follow-Up (N = 16) | p | ||
|---|---|---|---|---|---|
| Mean Value | ±SD | Mean Value | ±SD | ||
| Lymphocytes count (103/µL) | 1.55 | 0.34 | 1.93 | 0.57 | 0.022 |
| Neutrophils count ((103/µL) | 4.56 | 1.54 | 3.98 | 1.66 | 0.26 |
| Monocytes count (103/µL) | 0.59 | 0.19 | 0.54 | 0.31 | 0.45 |
| Eosinophil count (103/µL) | 0.21 | 0.14 | 0.18 | 0.09 | 0.41 |
| Basophils count (103/µL) | 0.03 | 0.03 | 0.02 | 0.02 | 0.20 |
| IL-6 (pg/mL) | 2.12 | 0.55 | 1.78 | 0.45 | 0.038 |
| IL-8 (pg/mL) | 38.23 | 10.98 | 34.45 | 13.74 | 0.35 |
| IL-beta (pg/mL) | 0.25 | 0.10 | 0.29 | 0.09 | 0.19 |
| TNF-α (pg/mL) | 2.07 | 0.80 | 1.60 | 0.72 | 0.07 |
| CRP (mg/L) | 5.11 | 2.53 | 3.81 | 1.68 | 0.08 |
| Age | 72.70 | 9.31 | 70.88 | 10.78 | 0.58 |
| Gleason score | 7.17 | 1.07 | 7.00 | 0.97 | 0.60 |
| Charlson Comorbidity Index | 3.48 | 0.90 | 3.38 | 1.70 | 0.81 |
| Percentage of patients with bone metastases | 26.1% | - | 18.8% | - | 0.59 |
| Percentage of patients underwent prostatectomy | 60.9% | - | 75.0% | - | 0.36 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buigues, C.; Navarro-Martínez, R.; Sánchez-Martínez, V.; Serrano-Carrascosa, M.; Rubio-Briones, J.; Cauli, O. Interleukin-6 and Lymphocyte Count Associated and Predicted the Progression of Frailty Syndrome in Prostate Cancer Patients Undergoing Antiandrogen Therapy. Cancers 2020, 12, 1716. https://doi.org/10.3390/cancers12071716
Buigues C, Navarro-Martínez R, Sánchez-Martínez V, Serrano-Carrascosa M, Rubio-Briones J, Cauli O. Interleukin-6 and Lymphocyte Count Associated and Predicted the Progression of Frailty Syndrome in Prostate Cancer Patients Undergoing Antiandrogen Therapy. Cancers. 2020; 12(7):1716. https://doi.org/10.3390/cancers12071716
Chicago/Turabian StyleBuigues, Cristina, Rut Navarro-Martínez, Vanessa Sánchez-Martínez, María Serrano-Carrascosa, José Rubio-Briones, and Omar Cauli. 2020. "Interleukin-6 and Lymphocyte Count Associated and Predicted the Progression of Frailty Syndrome in Prostate Cancer Patients Undergoing Antiandrogen Therapy" Cancers 12, no. 7: 1716. https://doi.org/10.3390/cancers12071716