Association between Abdominal Obesity and Incident Colorectal Cancer: A Nationwide Cohort Study in Korea

 , , and
, , and
Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics
2.2. Incidence and Risk of Colorectal, Colon, and Rectal Cancers by WC Categories
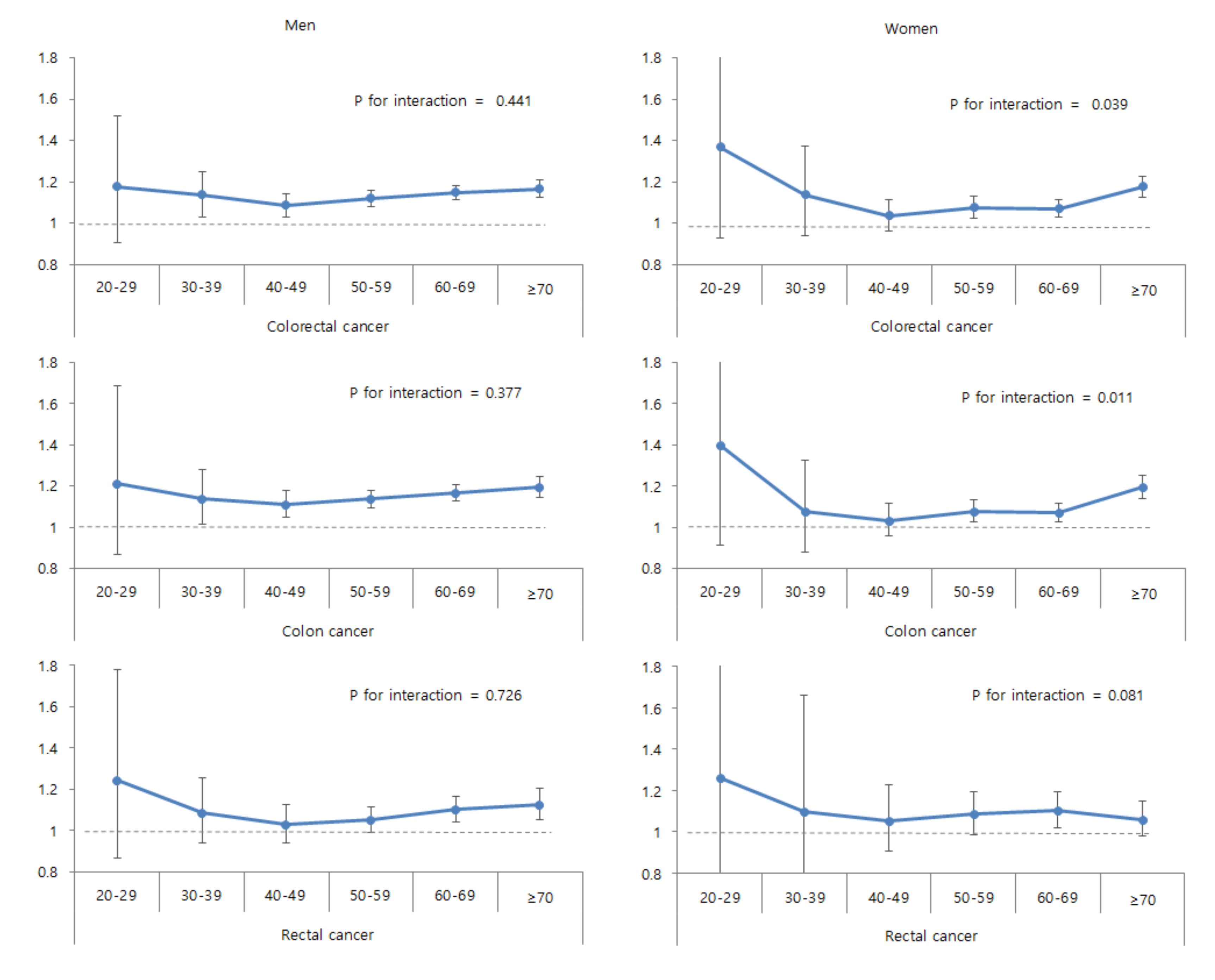
2.3. Subgroup Analysis
2.4. Study Outcomes by the Combination of Obesity Status
3. Discussion
4. Materials and Methods
4.1. Study Setting and Population
4.2. Study Outcomes
4.3. Categories of WC
4.4. Covariates
4.5. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization (WHO). Obesity and Overweight [Updated 16 February 2018; Cited 2019 November]. Available online: https://www.who.int/en/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 10 November 2019).
- Seo, M.H.; Kim, Y.H.; Han, K.; Jung, J.H.; Park, Y.G.; Lee, S.S.; Kwon, H.S.; Lee, W.Y.; Yoo, S.J. Prevalence of obesity and incidence of obesity-related comorbidities in Koreans based on national health insurance service health checkup data 2006–2015. J. Obes. Metab. Syndr. 2018, 27, 46–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frezza, E.E.; Wachtel, M.S.; Chiriva-Internati, M. Influence of obesity on the risk of developing colon cancer. Gut 2006, 55, 285–291. [Google Scholar] [CrossRef] [PubMed]
- Djalalinia, S.; Qorbani, M.; Peykari, N.; Kelishadi, R. Health impacts of obesity. Pak. J. Med. Sci. 2015, 31, 239–242. [Google Scholar] [PubMed]
- Lee, K.R.; Hwang, I.C.; Han, K.D.; Jung, J.; Seo, M.H. Waist circumference and risk of breast cancer in Korean women: A nationwide cohort study. Int. J. Cancer 2018, 142, 1554–1559. [Google Scholar] [CrossRef]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef]
- Korean Statistical Information Service. Cancer Registration Statistics, Statistical Information Report. 2018. Available online: http://kostat.go.kr/portal/korea/kor_pi/8/6/2/index.board?bmode=download&bSeq=&aSeq=365723&ord=2 (accessed on 10 November 2019).
- Ko, S.; Yoon, S.J.; Kim, D.; Kim, A.R.; Kim, E.J.; Seo, H.Y. Metabolic risk profile and cancer in Korean men and women. J. Prev. Med. Public Health 2016, 49, 143–152. [Google Scholar] [CrossRef] [Green Version]
- De Pergola, G.; Silvestris, F. Obesity as a major risk factor for cancer. J. Obes. 2013, 2013, 291546. [Google Scholar] [CrossRef] [Green Version]
- Moore, L.L.; Bradlee, M.L.; Singer, M.R.; Splansky, G.L.; Proctor, M.H.; Ellison, R.C.; Kreger, B.E. BMI and waist circumference as predictors of lifetime colon cancer risk in Framingham Study adults. Int. J. Obes. Relat. Metab. Disord. 2004, 28, 559–567. [Google Scholar] [CrossRef] [Green Version]
- Misra, A.; Vikram, N.K. Clinical and pathophysiological consequences of abdominal adiposity and abdominal adipose tissue depots. Nutrition 2003, 19, 457–466. [Google Scholar] [CrossRef]
- Kyrgiou, M.; Kalliala, I.; Markozannes, G.; Gunter, M.J.; Paraskevaidis, E.; Gabra, H.; Martin-Hirsch, P.; Tsilidis, K.K. Adiposity and cancer at major anatomical sites: Umbrella review of the literature. BMJ 2017, 356, j477. [Google Scholar] [CrossRef] [Green Version]
- Ma, Y.; Yang, Y.; Wang, F.; Zhang, P.; Shi, C.; Zou, Y.; Qin, H. Obesity and risk of colorectal cancer: A systematic review of prospective studies. PLoS ONE 2013, 8, e53916. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, Y.; Zhou, J.; Zhu, Y.; Luo, L.; He, T.; Hu, H.; Liu, H.; Zhang, Y.; Luo, D.; Xu, S.; et al. Abdominal obesity and colorectal cancer risk: Systematic review and meta-analysis of prospective studies. Biosci. Rep. 2017, 37, BSR20170945. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauby-Secretan, B.; Scoccianti, C.; Loomis, D.; Grosse, Y.; Bianchini, F.; Straif, K.; International Agency for Research on Cancer Handbook Working Group. Body fatness and cancer—Viewpoint of the IARC working group. N. Engl. J. Med 2016, 375, 794–798. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morales, Ó.; Regino, W.; Gómez, M.; Castro, D. Abdominal obesity increases the risks of colorectal polyps. Revista Colombiana de Gastroenterologia 2014, 29, 376–382. [Google Scholar]
- Karahalios, A.; Simpson, J.A.; Baglietto, L.; MacInnis, R.J.; Hodge, A.M.; Giles, G.G.; English, D.R. Change in weight and waist circumference and risk of colorectal cancer: Results from the Melbourne Collaborative Cohort Study. BMC Cancer 2016, 16, 157. [Google Scholar] [CrossRef] [Green Version]
- Aran, V.; Victorino, A.P.; Thuler, L.C.; Ferreira, C.G. Colorectal cancer: Epidemiology, disease mechanisms and interventions to reduce onset and mortality. Clin. Colorectal Cancer 2016, 15, 195–203. [Google Scholar] [CrossRef]
- Renehan, A.G.; Roberts, D.L.; Dive, C. Obesity and cancer: Pathophysiological and biological mechanisms. Arch. Physiol. Biochem. 2008, 114, 71–83. [Google Scholar] [CrossRef]
- Vigneri, P.G.; Tirro, E.; Pennisi, M.S.; Massimino, M.; Stella, S.; Romano, C.; Manzella, L. The insulin/IGF system in colorectal cancer development and resistance to therapy. Front. Oncol. 2015, 5, 230. [Google Scholar] [CrossRef] [Green Version]
- Moghaddam, A.A.; Woodward, M.; Huxley, R. Obesity and risk of colorectal cancer: A meta-analysis of 31 studies with 70,000 events. Cancer Epidemiol. Biomark. Prev. 2007, 16, 2533–2547. [Google Scholar] [CrossRef] [Green Version]
- Li, H.; Yang, G.; Xiang, Y.B.; Zhang, X.; Zheng, W.; Gao, Y.T.; Shu, X.O. Body weight, fat distribution and colorectal cancer risk: A report from cohort studies of 134255 Chinese men and women. Int. J. Obes. (Lond.) 2013, 37, 783–789. [Google Scholar] [CrossRef] [Green Version]
- Larsson, S.C.; Wolk, A. Obesity and colon and rectal cancer risk: A meta-analysis of prospective studies. Am. J. Clin. Nutr. 2007, 86, 556–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haftenberger, M.; Lahmann, P.H.; Panico, S.; Gonzalez, C.A.; Seidell, J.C.; Boeing, H.; Giurdanella, M.C.; Krogh, V.; Bueno-de-Mesquita, H.B.; Peeters, P.H.; et al. Overweight, obesity and fat distribution in 50- to 64-year-old participants in the European Prospective Investigation into Cancer and Nutrition (EPIC). Public Health Nutr. 2002, 5, 1147–1162. [Google Scholar] [CrossRef] [PubMed]
- Stevens, J.; Katz, E.G.; Huxley, R.R. Associations between gender, age and waist circumference. Eur. J. Clin. Nutr. 2010, 64, 6–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karastergiou, K.; Smith, S.R.; Greenberg, A.S.; Fried, S.K. Sex differences in human adipose tissues—The biology of pear shape. Biol. Sex Differ. 2012, 3, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.Y.; Lee, H.S.; Lee, D.C.; Chu, S.H.; Jeon, J.Y.; Kim, N.K.; Lee, J.W. Visceral fat accumulation is associated with colorectal cancer in postmenopausal women. PLoS ONE 2014, 9, e110587. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pischon, T.; Lahmann, P.H.; Boeing, H.; Friedenreich, C.; Norat, T.; Tjønneland, A.; Halkjaer, J.; Overvad, K.; Clavel-Chapelon, F.; Boutron-Ruault, M.C.; et al. Body size and risk of colon and rectal cancer in the European Prospective Investigation Into Cancer and Nutrition (EPIC). J. Natl. Cancer Inst. 2006, 98, 920–931. [Google Scholar] [CrossRef]
- Clark, W.; Siegel, E.M.; Chen, Y.A.; Zhao, X.; Parsons, C.M.; Hernandez, J.M.; Weber, J.; Thareja, S.; Choi, J.; Shibata, D. Quantitative measures of visceral adiposity and body mass index in predicting rectal cancer outcomes after neoadjuvant chemoradiation. J. Am. Coll. Surg. 2013, 216, 1070–1081. [Google Scholar] [CrossRef] [Green Version]
- Li, H.X.; Zhang, F.; Zhao, D.; Xin, D.; Guo, S.Q.; Wang, S.M.; Zhang, J.J.; Wang, J.; Li, Y.; Yang, G.R.; et al. Neck circumference as a measure of neck fat and abdominal visceral fat in Chinese adults. BMC Public Health 2014, 14, 311. [Google Scholar] [CrossRef] [Green Version]
- WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef]
- Lee, S.Y.; Park, H.S.; Kim, D.J.; Han, J.H.; Kim, S.M.; Cho, G.J.; Kim, D.Y.; Kwon, H.S.; Kim, S.R.; Lee, C.B.; et al. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res. Clin. Pract. 2007, 75, 72–80. [Google Scholar] [CrossRef]
- Agarwal, D.P. Cardioprotective effects of light-moderate consumption of alcohol: A review of putative mechanisms. Alcohol Alcohol. 2002, 37, 409–415. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Colorectal Cancer | p1 | |
|---|---|---|---|
| No | Yes | ||
| n | 9,858,408 | 101,197 | |
| Age (years) | 46.8 ± 14.0 | 59.3 ± 11.7 | <0.001 |
| Sex (male) | 5,440,501 (55.2) | 61,271 (60.6) | <0.001 |
| Current smoker | 2,616,381 (26.5) | 24,405 (24.1) | <0.001 |
| Heavy alcohol drinker | 790,083 (8.0) | 9785 (9.7) | <0.001 |
| Regular exerciser | 1,812,993 (18.4) | 21,304 (21.1) | <0.001 |
| Income (lowest quartile) | 2,584,903 (26.2) | 27,341 (27.0) | <0.001 |
| Height (cm) | 164.0 ± 9.2 | 162.1 ± 8.7 | <0.001 |
| Weight (kg) | 64.0 ± 11.6 | 63.5 ± 10.6 | <0.001 |
| Body mass index (kg/m2) | 23.7 ± 3.2 | 24.1 ± 3.1 | <0.001 |
| Waist circumference (cm) | 80.2 ± 9.1 | 83.0 ± 8.6 | <0.001 |
| Systolic blood pressure (mmHg) | 122.4 ± 14.9 | 127.0 ± 15.9 | <0.001 |
| Diastolic blood pressure (mmHg) | 76.3 ± 10.06 | 78.1 ± 10.2 | <0.001 |
| Glucose (mg/dL) | 97.0 ± 22.8 | 103.3 ± 28.1 | <0.001 |
| Total cholesterol (mg/dL) | 195.0 ± 36.6 | 197.7 ± 37.8 | <0.001 |
| Triglycerides 2 | 113.7 (113.7–113.8) | 124.7 (124.3–125.1) | <0.001 |
| HDL-C | 55.7 ± 21.8 | 54.4 ± 24.4 | <0.001 |
| LDL-C | 114.2 ± 47.0 | 115.7 ± 42.4 | <0.001 |
| Hypertension | 2,498,816 (25.4) | 44,630 (44.1) | <0.001 |
| Diabetes mellitus | 842,122 (8.5) | 17,305 (17.1) | <0.001 |
| Dyslipidemia | 1,785,678 (18.1) | 25,471 (25.2) | <0.001 |
| WC Category | n | Events | Person-Years | IR 1 | HR (95% CI) | ||
|---|---|---|---|---|---|---|---|
| Model 1 2 | Model 2 3 | Model 3 4 | |||||
| Colorectal cancer | |||||||
| WC (per 5 cm) | 1.18 (1.18–1.19) | 1.033 (1.029–1.037) | 1.040 (1.033–1.046) | ||||
| WC (cm) | |||||||
| M: <75.0, F: <70.0 | 1,724,651 | 9794 | 14,213,668 | 0.69 | 0.47 (0.46–0.48) | 0.90 (0.88–0.92) | 0.89 (0.86–0.91) |
| M: 75.0–79.9, F: 70.0–74.9 | 1,937,992 | 15,181 | 15,975,402 | 0.95 | 0.64 (0.63–0.66) | 0.94 (0.92–0.96) | 0.93 (0.91–0.95) |
| M: 80.0–84.9, F: 75.0–79.9 | 2,371,404 | 23,630 | 19,513,766 | 1.21 | 0.82 (0.80–0.83) | 0.96 (0.94–0.98) | 0.95 (0.94–0.97) |
| M: 85.0–89.9, F: 80.0–84.9 | 1,974,893 | 24,032 | 16,220,342 | 1.48 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| M: 90.0–94.9, F: 85.0–89.9 | 1,156,111 | 16,485 | 9,470,747 | 1.74 | 1.18 (1.15–1.20) | 1.05 (1.03–1.07) | 1.06 (1.04–1.08) |
| M: 95.0–99.9, F: 90.0–94.9 | 514,810 | 7797 | 4,208,225 | 1.85 | 1.25 (1.22–1.28) | 1.06 (1.03–1.08) | 1.06 (1.04–1.09) |
| M: ≥100.0, F: ≥95.0 | 279,744 | 4278 | 2,278,692 | 1.88 | 1.27 (1.23–1.31) | 1.08 (1.05–1.12) | 1.10 (1.06–1.14) |
| P | <0.001 | <0.001 | <0.001 | ||||
| p for trend | <0.001 | <0.001 | <0.001 | ||||
| M: <90.0, F: <85.0 | 8,008,940 | 72,637 | 65,923,178 | 1.10 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| M: ≥90.0, F: ≥85.0 | 1,950,665 | 28,560 | 15,957,664 | 1.79 | 1.62 (1.60–1.65) | 1.10 (1.08–1.12) | 1.08 (1.06–1.10) |
| Colon cancer | |||||||
| WC (per 5 cm) | 1.181 (1.177–1.186) | 1.035 (1.031–1.040) | 1.039 (1.032–1.046) | ||||
| WC (cm) | |||||||
| M: <75.0, F: <70.0 | 1,724,651 | 8114 | 14,213,668 | 0.57 | 0.46 (0.45–0.48) | 0.90 (0.88–0.92) | 0.90 (0.87–0.93) |
| M: 75.0–79.9, F: 70.0–74.9 | 1,937,992 | 12,621 | 15,975,402 | 0.79 | 0.64 (0.63–0.66) | 0.94 (0.92–0.96) | 0.94 (0.91–0.96) |
| M: 80.0–84.9, F: 75.0–79.9 | 2,371,404 | 19,543 | 19,513,766 | 1.00 | 0.81 (0.80–0.83) | 0.96 (0.94–0.97) | 0.96 (0.94–0.97) |
| M: 85.0–89.9, F: 80.0–84.9 | 1,974,893 | 20,011 | 16,220,342 | 1.23 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| M: 90.0–94.9, F: 85.0–89.9 | 1,156,111 | 13,890 | 9,470,747 | 1.47 | 1.19 (1.16–1.22) | 1.06 (1.04–1.09) | 1.06 (1.04–1.09) |
| M: 95.0–99.9, F: 90.0–94.9 | 514,810 | 6600 | 4,208,225 | 1.57 | 1.27 (1.24–1.31) | 1.07 (1.04–1.10) | 1.07 (1.04–1.10) |
| M: ≥100.0, F: ≥95.0 | 279,744 | 3624 | 2,278,692 | 1.59 | 1.29 (1.25–1.34) | 1.09 (1.05–1.13) | 1.09 (1.05–1.14) |
| P | <0.001 | <0.001 | <0.001 | ||||
| p for trend | <0.001 | <0.001 | <0.001 | ||||
| M: <90.0, F: <85.0 | 8,008,940 | 60,289 | 65,923,178 | 0.91 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| M: ≥90.0, F: ≥85.0 | 1,950,665 | 24,114 | 15,957,664 | 1.51 | 1.65 (1.63–1.68) | 1.11 (1.09–1.13) | 1.08 (1.06–1.10) |
| Rectal cancer | |||||||
| WC (per 5 cm) | 1.196 (1.189–1.203) | 1.030 (1.023–1.038) | 1.049 (1.037–1.061) | ||||
| WC (cm) | |||||||
| M: <75.0, F: <70.0 | 1,724,651 | 2945 | 14,213,668 | 0.21 | 0.46 (0.44–0.48) | 0.89 (0.85–0.93) | 0.84 (0.80–0.88) |
| M: 75.0–79.9, F: 70.0–74.9 | 1,937,992 | 4547 | 15,975,402 | 0.28 | 0.62 (0.60–0.65) | 0.92 (0.88–0.95) | 0.89 (0.85–0.92) |
| M: 80.0–84.9, F: 75.0–79.9 | 2,371,404 | 7342 | 19,513,766 | 0.38 | 0.83 (0.80–0.85) | 0.96 (0.93–0.99) | 0.94 (0.91–0.98) |
| M: 85.0–89.9, F: 80.0–84.9 | 1,974,893 | 7397 | 16,220,342 | 0.46 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| M: 90.0–94.9, F: 85.0–89.9 | 1,156,111 | 4914 | 9,470,747 | 0.52 | 1.14 (1.10–1.18) | 1.02 (0.99–1.06) | 1.04 (1.002–1.08) |
| M: 95.0–99.9, F: 90.0–94.9 | 514,810 | 2259 | 4,208,225 | 0.54 | 1.18 (1.12–1.23) | 1.02 (0.97–1.06) | 1.05 (1.00–1.10) |
| M: ≥100.0, F: ≥95.0 | 279,744 | 1266 | 2,278,692 | 0.56 | 1.22 (1.15–1.29) | 1.08 (1.02–1.15) | 1.15 (1.08–1.23) |
| P | <0.001 | <0.001 | <0.001 | ||||
| p for trend | <0.001 | <0.001 | <0.001 | ||||
| M: <90.0, F: <85.0 | 8,008,940 | 22,231 | 65,923,178 | 0.34 | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| M: ≥90.0, F: ≥85.0 | 1,950,665 | 8439 | 15,957,664 | 0.53 | 1.57 (1.53–1.61) | 1.08 (1.05–1.10) | 1.07 (1.04–1.10) |
| Subgroup | Colorectal Cancer | p for Interaction | Colon Cancer | p for Interaction | Rectal Cancer | p for Interaction |
|---|---|---|---|---|---|---|
| Age (years) | 0.102 | 0.024 | 0.959 | |||
| <65 | 1.07 (1.05–1.09) | 1.08 (1.05–1.10) | 1.05 (1.02–1.09) | |||
| ≥65 | 1.15 (1.13–1.18) | 1.18 (1.15–1.20) | 1.11 (1.06–1.15) | |||
| Sex | <0.001 | <0.001 | 0.003 | |||
| Male | 1.15 (1.13–1.17) | 1.17 (1.15–1.20) | 1.09 (1.06–1.13) | |||
| Female | 1.11 (1.08–1.13) | 1.11 (1.08–1.14) | 1.09 (1.04–1.14) | |||
| Diabetes mellitus | 0.003 | 0.003 | 0.041 | |||
| No | 1.11 (1.09–1.12) | 1.12 (1.10–1.14) | 1.09 (1.05–1.12) | |||
| Yes | 1.08 (1.05–1.11) | 1.09 (1.05–1.13) | 1.04 (0.99–1.10) | |||
| Body mass index (kg/m2) | 0.037 | 0.016 | 0.738 | |||
| <25 | 1.07 (1.04–1.10) | 1.07 (1.04–1.10) | 1.07 (1.02–1.12) | |||
| ≥25 | 1.10 (1.07–1.12) | 1.10 (1.08–1.13) | 1.08 (1.03–1.12) | |||
| Smoking | 0.331 | 0.340 | 0.444 | |||
| Non-smoker | 1.12 (1.10–1.14) | 1.13 (1.11–1.15) | 1.09 (1.06–1.12) | |||
| Current smoker | 1.09 (1.05–1.12) | 1.09 (1.06–1.13) | 1.08 (1.03–1.14) |
| Sex | General Obesity | Abdominal Obesity | HR (95% CI) | ||
|---|---|---|---|---|---|
| Colorectal Cancer | Colon Cancer | Rectal Cancer | |||
| Total | No | No | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| No | Yes | 1.06 (1.03–1.09) | 1.06 (1.03–1.10) | 1.08 (1.02–1.13) | |
| Yes | No | 1.01 (0.99–1.03) | 1.01 (0.99–1.03) | 1.02 (0.98–1.05) | |
| Yes | Yes | 1.11 (1.10–1.13) | 1.13 (1.11–1.15) | 1.08 (1.05–1.11) | |
| P | <0.001 | <0.001 | <0.001 | ||
| Men | No | No | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| No | Yes | 1.14 (1.10–1.17) | 1.14 (1.10–1.19) | 1.15 (1.09–1.22) | |
| Yes | No | 1.05 (1.03–1.08) | 1.06 (1.03–1.09) | 1.04 (1.00–1.08) | |
| Yes | Yes | 1.17 (1.15–1.19) | 1.20 (1.18–1.23) | 1.09 (1.05–1.13) | |
| P | <0.001 | <0.001 | <0.001 | ||
| Women | No | No | 1 (ref.) | 1 (ref.) | 1 (ref.) |
| No | Yes | 1.04 (1.00–1.08) | 1.04 (1.00–1.09) | 0.99 (0.91–1.08) | |
| Yes | No | 1.05 (1.02–1.08) | 1.06 (1.03–1.10) | 1.02 (0.96–1.08) | |
| Yes | Yes | 1.14 (1.11–1.17) | 1.15 (1.12–1.18) | 1.13 (1.07–1.18) | |
| P | <0.001 | <0.001 | <0.001 | ||
| p for interaction | <0.001 | <0.001 | <0.001 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nam, G.E.; Baek, S.-J.; Choi, H.B.; Han, K.; Kwak, J.-M.; Kim, J.; Kim, S.-H. Association between Abdominal Obesity and Incident Colorectal Cancer: A Nationwide Cohort Study in Korea. Cancers 2020, 12, 1368. https://doi.org/10.3390/cancers12061368
Nam GE, Baek S-J, Choi HB, Han K, Kwak J-M, Kim J, Kim S-H. Association between Abdominal Obesity and Incident Colorectal Cancer: A Nationwide Cohort Study in Korea. Cancers. 2020; 12(6):1368. https://doi.org/10.3390/cancers12061368
Chicago/Turabian StyleNam, Ga Eun, Se-Jin Baek, Hong Bae Choi, Kyungdo Han, Jung-Myun Kwak, Jin Kim, and Seon-Hahn Kim. 2020. "Association between Abdominal Obesity and Incident Colorectal Cancer: A Nationwide Cohort Study in Korea" Cancers 12, no. 6: 1368. https://doi.org/10.3390/cancers12061368