Applications of Artificial Intelligence to Prostate Multiparametric MRI (mpMRI): Current and Emerging Trends

 , , ,
, , ,
Abstract
:1. Introduction
2. Multiparametric Magnetic Resonance Imaging
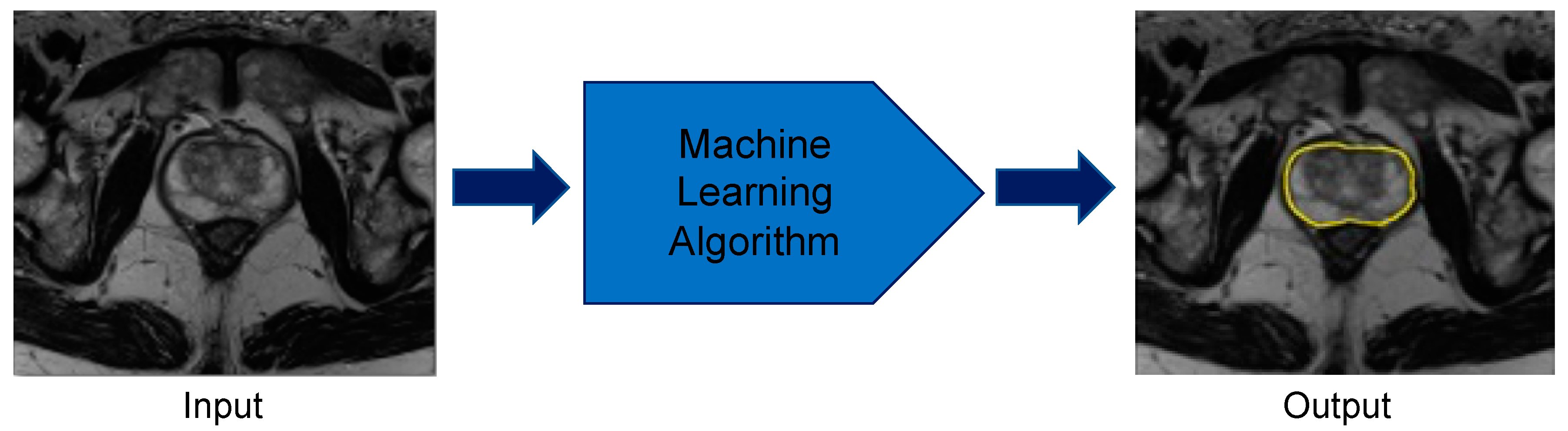
3. Artificial Intelligence Paradigms: Machine Learning and Deep Learning
4. Prostate Organ: Segmentation and Volume Estimation
5. Prostate Lesion: Detection, Segmentation, and Volume Estimation
6. Prostate Lesion: Characterization
7. Future Work
8. Conclusions
Funding
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 7–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hugosson, J.; Carlsson, S. Overdetection in screening for prostate cancer. Curr. Opin. Urol. 2014, 24, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Schröder, F.H.; Hugosson, J.; Roobol, M.J.; Tammela, T.L.; Ciatto, S.; Nelen, V.; Kwiatkowski, M.; Lujan, M.; Lilja, H.; Zappa, M.; et al. Screening and prostate-cancer mortality in a randomized European study. N. Engl. J. Med. 2009, 360, 1320–1328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oberlin, D.T.; Casalino, D.D.; Miller, F.H.; Meeks, J.J. Dramatic increase in the utilization of multiparametric magnetic resonance imaging for detection and management of prostate cancer. Abdom. Radiol. (Ny) 2017, 42, 1255–1258. [Google Scholar] [CrossRef] [PubMed]
- Monni, F.; Fontanella, P.; Grasso, A.; Wiklund, P.; Ou, Y.C.; Randazzo, M.; Rocco, B.; Montanari, E.; Bianchi, G. Magnetic resonance imaging in prostate cancer detection and management: A systematic review. Minerva. Urol. Nefrol. 2017, 69, 567–578. [Google Scholar] [CrossRef] [PubMed]
- Uzzo, R.G.; Wei, J.T.; Waldbaum, R.S.; Perlmutter, A.P.; Byrne, J.C.; Vaughan, D., Jr. The influence of prostate size on cancer detection. Urology 1995, 46, 831–836. [Google Scholar] [CrossRef]
- Boyle, P.; Gould, A.L.; Roehrborn, C.G. Prostate volume predicts outcome of treatment of benign prostatic hyperplasia with finasteride: Meta-analysis of randomized clinical trials. Urology 1996, 48, 398–405. [Google Scholar] [CrossRef]
- Sparks, R.; Bloch, B.N.; Feleppa, E.; Barratt, D.; Madabhushi, A. Fully automated prostate magnetic resonance imaging and transrectal ultrasound fusion via a probabilistic registration metric. Proc. SPIE Int. Soc. Opt. Eng. 2013, 8671. [Google Scholar] [CrossRef] [Green Version]
- Tay, K.J.; Gupta, R.T.; Rastinehad, A.R.; Tsivian, E.; Freedland, S.J.; Moul, J.W.; Polascik, T.J. Navigating MRI-TRUS fusion biopsy: Optimizing the process and avoiding technical pitfalls. Expert Rev. Anticancer Ther. 2016, 16, 303–311. [Google Scholar] [CrossRef]
- Lim, K.B. Epidemiology of clinical benign prostatic hyperplasia. Asian J. Urol. 2017, 4, 148–151. [Google Scholar] [CrossRef]
- Garvey, B.; Türkbey, B.; Truong, H.; Bernardo, M.; Periaswamy, S.; Choyke, P.L. Clinical value of prostate segmentation and volume determination on MRI in benign prostatic hyperplasia. Diagn. Interv. Radiol. 2014, 20, 229. [Google Scholar] [CrossRef] [PubMed]
- Kolman, C.; Girman, C.J.; Jacobsen, S.J.; Lieber, M.M. Distribution of post-void residual urine volume in randomly selected men. J. Urol. 1999, 161, 122–127. [Google Scholar] [CrossRef]
- Girman, C.J.; Jacobsen, S.J.; Guess, H.A.; Oesterling, J.E.; Chute, C.G.; Panser, L.A.; Lieber, M.M. Natural history of prostatism: Relationship among symptoms, prostate volume and peak urinary flow rate. J. Urol. 1995, 153, 1510–1515. [Google Scholar] [CrossRef]
- Oelke, M.; Bachmann, A.; Descazeaud, A.; Emberton, M.; Gravas, S.; Michel, M.C.; N’dow, J.; Nordling, J.; Jean, J. EAU guidelines on the treatment and follow-up of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. Eur. Urol. 2013, 64, 118–140. [Google Scholar] [CrossRef] [PubMed]
- Bretton, P.R.; Evans, W.P.; Borden, J.D.; Castellanos, R.D. The use of prostate specific antigen density to improve the sensitivity of prostate specific antigen in detecting prostate carcinoma. Cancer Interdiscip. Int. J. Am. Cancer Soc. 1994, 74, 2991–2995. [Google Scholar] [CrossRef]
- Benson, M.C.; Seong Whang, I.; Pantuck, A.; Ring, K.; Kaplan, S.A.; Olsson, C.A.; Cooner, W.H. Prostate specific antigen density: A means of distinguishing benign prostatic hypertrophy and prostate cancer. J. Urol. 1992, 147, 815–816. [Google Scholar] [CrossRef]
- Sfoungaristos, S.; Perimenis, P. PSA density is superior than PSA and Gleason score for adverse pathologic features prediction in patients with clinically localized prostate cancer. Can. Urol. Assoc. J. 2012, 6, 46. [Google Scholar] [CrossRef]
- May, M.; Siegsmund, M.; Hammermann, F.; Loy, V.; Gunia, S. Visual estimation of the tumor volume in prostate cancer: A useful means for predicting biochemical-free survival after radical prostatectomy? Prostate Cancer Prostatic Dis. 2007, 10, 66. [Google Scholar] [CrossRef]
- Steenbergen, P.; Haustermans, K.; Lerut, E.; Oyen, R.; De Wever, L.; Van den Bergh, L.; Kerkmeijer, L.G.; Pameijer, F.A.; Veldhuis, W.B.; Pos, F.J. Prostate tumor delineation using multiparametric magnetic resonance imaging: Inter-observer variability and pathology validation. Radiother. Oncol. 2015, 115, 186–190. [Google Scholar] [CrossRef] [Green Version]
- Njeh, C. Tumor delineation: The weakest link in the search for accuracy in radiotherapy. J. Med. Phys./Assoc. Med. Phys. India 2008, 33, 136. [Google Scholar] [CrossRef]
- Denis, L.J.; Murphy, G.P.; Schroder, F.H. Report of the consensus workshop on screening and global strategy for prostate cancer. Cancer 1995, 75, 1187–1207. [Google Scholar] [CrossRef]
- Edwards, B.K.; Ward, E.; Kohler, B.A.; Eheman, C.; Zauber, A.G.; Anderson, R.N.; Jemal, A.; Schymura, M.J.; Lansdorp-Vogelaar, I.; Seeff, L.C.; et al. Annual report to the nation on the status of cancer, 1975-2006, featuring colorectal cancer trends and impact of interventions (risk factors, screening, and treatment) to reduce future rates. Cancer 2010, 116, 544–573. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etzioni, R.; Tsodikov, A.; Mariotto, A.; Szabo, A.; Falcon, S.; Wegelin, J.; DiTommaso, D.; Karnofski, K.; Gulati, R.; Penson, D.F.; et al. Quantifying the role of PSA screening in the US prostate cancer mortality decline. Cancer Causes Control. 2008, 19, 175–181. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahdensuo, K.; Erickson, A.; Saarinen, I.; Seikkula, H.; Lundin, J.; Lundin, M.; Nordling, S.; Bützow, A.; Vasarainen, H.; Bostrom, P.J.; et al. Loss of PTEN expression in ERG-negative prostate cancer predicts secondary therapies and leads to shorter disease-specific survival time after radical prostatectomy. Mod. Pathol. 2016, 29, 1565–1574. [Google Scholar] [CrossRef] [Green Version]
- Rothwax, J.T.; George, A.K.; Wood, B.J.; Pinto, P.A. Multiparametric MRI in biopsy guidance for prostate cancer: Fusion-guided. Biomed. Res. Int. 2014, 2014, 439171. [Google Scholar] [CrossRef] [Green Version]
- Lips, I.M.; van der Heide, U.A.; Haustermans, K.; van Lin, E.N.; Pos, F.; Franken, S.P.; Kotte, A.N.; van Gils, C.H.; van Vulpen, M. Single blind randomized phase III trial to investigate the benefit of a focal lesion ablative microboost in prostate cancer (FLAME-trial): Study protocol for a randomized controlled trial. Trials 2011, 12, 255. [Google Scholar] [CrossRef] [Green Version]
- Cellini, N.; Morganti, A.G.; Mattiucci, G.C.; Valentini, V.; Leone, M.; Luzi, S.; Manfredi, R.; Dinapoli, N.; Digesu’, C.; Smaniotto, D. Analysis of intraprostatic failures in patients treated with hormonal therapy and radiotherapy: Implications for conformal therapy planning. Int. J. Radiat. Oncol. Biol. Phys. 2002, 53, 595–599. [Google Scholar] [CrossRef]
- Chun, F.K.-H.; Briganti, A.; Jeldres, C.; Gallina, A.; Erbersdobler, A.; Schlomm, T.; Walz, J.; Eichelberg, C.; Salomon, G.; Haese, A. Tumour volume and high grade tumour volume are the best predictors of pathologic stage and biochemical recurrence after radical prostatectomy. Eur. J. Cancer 2007, 43, 536–543. [Google Scholar] [CrossRef]
- Chung, B.I.; Tarin, T.V.; Ferrari, M.; Brooks, J.D. Comparison of prostate cancer tumor volume and percent cancer in prediction of biochemical recurrence and cancer specific survival. Urol. Oncol. 2011, 29, 314–318. [Google Scholar] [CrossRef]
- Nelson, B.A.; Shappell, S.B.; Chang, S.S.; Wells, N.; Farnham, S.B.; Smith, J.A., Jr.; Cookson, M.S. Tumour volume is an independent predictor of prostate-specific antigen recurrence in patients undergoing radical prostatectomy for clinically localized prostate cancer. BJU Int. 2006, 97, 1169–1172. [Google Scholar] [CrossRef]
- Fukuhara, H.; Kume, H.; Suzuki, M.; Fujimura, T.; Enomoto, Y.; Nishimatsu, H.; Ishikawa, A.; Homma, Y. Maximum tumor diameter: A simple independent predictor for biochemical recurrence after radical prostatectomy. Prostate Cancer Prostatic Dis. 2010, 13, 244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephenson, A.J.; Scardino, P.T.; Kattan, M.W.; Pisansky, T.M.; Slawin, K.M.; Klein, E.A.; Anscher, M.S.; Michalski, J.M.; Sandler, H.M.; Lin, D.W. Predicting the outcome of salvage radiation therapy for recurrent prostate cancer after radical prostatectomy. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2007, 25, 2035. [Google Scholar] [CrossRef] [PubMed]
- Bjurlin, M.A.; Taneja, S.S. Standards for prostate biopsy. Curr. Opin. Urol. 2014, 24, 155–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borghesi, M.; Ahmed, H.; Nam, R.; Schaeffer, E.; Schiavina, R.; Taneja, S.; Weidner, W.; Loeb, S. Complications After Systematic, Random, and Image-guided Prostate Biopsy. Eur. Urol. 2017, 71, 353–365. [Google Scholar] [CrossRef] [PubMed]
- Walsh, P.C.; Marschke, P.; Ricker, D.; Burnett, A.L. Patient-reported urinary continence and sexual function after anatomic radical prostatectomy. Urology 2000, 55, 58–61. [Google Scholar] [CrossRef]
- Hu, K.; Wallner, K. Clinical course of rectal bleeding following I-125 prostate brachytherapy. Int. J. Radiat. Oncol. Biol. Phys. 1998, 41, 263–265. [Google Scholar] [CrossRef]
- Theodorescu, D.; Gillenwater, J.Y.; Koutrouvelis, P.G. Prostatourethral-rectal fistula after prostate brachytherapy: Incidence and risk factors. Cancer Interdiscip. Int. J. Am. Cancer Soc. 2000, 89, 2085–2091. [Google Scholar] [CrossRef]
- Shaver, M.M.; Kohanteb, P.A.; Chiou, C.; Bardis, M.D.; Chantaduly, C.; Bota, D.; Filippi, C.G.; Weinberg, B.; Grinband, J.; Chow, D.S. Optimizing neuro-oncology imaging: A review of deep learning approaches for glioma imaging. Cancers 2019, 11, 829. [Google Scholar] [CrossRef] [Green Version]
- Jordan, M.I.; Mitchell, T.M. Machine learning: Trends, perspectives, and prospects. Science 2015, 349, 255–260. [Google Scholar] [CrossRef]
- Johnson, L.M.; Turkbey, B.; Figg, W.D.; Choyke, P.L. Multiparametric MRI in prostate cancer management. Nat. Rev. Clin. Oncol. 2014, 11, 346–353. [Google Scholar] [CrossRef]
- Stabile, A.; Giganti, F.; Rosenkrantz, A.B.; Taneja, S.S.; Villeirs, G.; Gill, I.S.; Allen, C.; Emberton, M.; Moore, C.M.; Kasivisvanathan, V. Multiparametric MRI for prostate cancer diagnosis: Current status and future directions. Nat. Rev. Urol. 2020, 17, 41–61. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, L.; Ahmed, H.U.; Allen, C.; Barentsz, J.O.; Carey, B.; Futterer, J.J.; Heijmink, S.W.; Hoskin, P.J.; Kirkham, A.; Padhani, A.R.; et al. Magnetic resonance imaging for the detection, localisation, and characterisation of prostate cancer: Recommendations from a European consensus meeting. Eur. Urol. 2011, 59, 477–494. [Google Scholar] [CrossRef] [PubMed]
- De Rooij, M.; Hamoen, E.H.; Futterer, J.J.; Barentsz, J.O.; Rovers, M.M. Accuracy of multiparametric MRI for prostate cancer detection: A meta-analysis. AJR Am. J. Roentgenol. 2014, 202, 343–351. [Google Scholar] [CrossRef] [PubMed]
- Fütterer, J.J.; Briganti, A.; De Visschere, P.; Emberton, M.; Giannarini, G.; Kirkham, A.; Taneja, S.S.; Thoeny, H.; Villeirs, G.; Villers, A. Can clinically significant prostate cancer be detected with multiparametric magnetic resonance imaging? A systematic review of the literature. Eur. Urol. 2015, 68, 1045–1053. [Google Scholar] [CrossRef] [PubMed]
- Daun, M.; Fardin, S.; Ushinsky, A.; Batra, S.; Nguyentat, M.; Lee, T.; Uchio, E.; Lall, C.; Houshyar, R. PI-RADS version 2 is an excellent screening tool for clinically significant prostate cancer as designated by the validated international society of urological pathology criteria: A retrospective analysis. Curr. Probl. Diagn. Radiol. 2019. [Google Scholar] [CrossRef]
- Turkbey, B.; Mani, H.; Shah, V.; Rastinehad, A.R.; Bernardo, M.; Pohida, T.; Pang, Y.; Daar, D.; Benjamin, C.; McKinney, Y.L.; et al. Multiparametric 3T prostate magnetic resonance imaging to detect cancer: Histopathological correlation using prostatectomy specimens processed in customized magnetic resonance imaging based molds. J. Urol. 2011, 186, 1818–1824. [Google Scholar] [CrossRef] [Green Version]
- Leake, J.L.; Hardman, R.; Ojili, V.; Thompson, I.; Shanbhogue, A.; Hernandez, J.; Barentsz, J. Prostate MRI: Access to and current practice of prostate MRI in the United States. J. Am. Coll. Radiol. 2014, 11, 156–160. [Google Scholar] [CrossRef] [Green Version]
- Latchamsetty, K.C.; Borden, L.S., Jr.; Porter, C.R.; Lacrampe, M.; Vaughan, M.; Lin, E.; Conti, N.; Wright, J.L.; Corman, J.M. Experience improves staging accuracy of endorectal magnetic resonance imaging in prostate cancer: What is the learning curve? Can. J. Urol. 2007, 14, 3429–3434. [Google Scholar]
- Gaziev, G.; Wadhwa, K.; Barrett, T.; Koo, B.C.; Gallagher, F.A.; Serrao, E.; Frey, J.; Seidenader, J.; Carmona, L.; Warren, A.; et al. Defining the learning curve for multiparametric magnetic resonance imaging (MRI) of the prostate using MRI-transrectal ultrasonography (TRUS) fusion-guided transperineal prostate biopsies as a validation tool. BJU Int. 2016, 117, 80–86. [Google Scholar] [CrossRef]
- Rosenkrantz, A.B.; Babb, J.S.; Taneja, S.S.; Ream, J.M. Proposed adjustments to PI-RADS Version 2 decision rules: Impact on prostate cancer detection. Radiology 2017, 283, 119–129. [Google Scholar] [CrossRef]
- De Visschere, P.J.; Vral, A.; Perletti, G.; Pattyn, E.; Praet, M.; Magri, V.; Villeirs, G.M. Multiparametric magnetic resonance imaging characteristics of normal, benign and malignant conditions in the prostate. Eur. Radiol. 2017, 27, 2095–2109. [Google Scholar] [CrossRef] [PubMed]
- Barentsz, J.O.; Richenberg, J.; Clements, R.; Choyke, P.; Verma, S.; Villeirs, G.; Rouviere, O.; Logager, V.; Futterer, J.J.; European Society of Urogenital, R. ESUR prostate MR guidelines 2012. Eur. Radiol. 2012, 22, 746–757. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinreb, J.C.; Barentsz, J.O.; Choyke, P.L.; Cornud, F.; Haider, M.A.; Macura, K.J.; Margolis, D.; Schnall, M.D.; Shtern, F.; Tempany, C.M.; et al. PI-RADS Prostate imaging—Reporting and data system: 2015, version 2. Eur. Urol. 2016, 69, 16–40. [Google Scholar] [CrossRef] [PubMed]
- Turkbey, B.; Rosenkrantz, A.B.; Haider, M.A.; Padhani, A.R.; Villeirs, G.; Macura, K.J.; Tempany, C.M.; Choyke, P.L.; Cornud, F.; Margolis, D.J.; et al. Prostate imaging reporting and data system version 2.1: 2019 update of prostate imaging reporting and data system version 2. Eur. Urol. 2019, 76, 340–351. [Google Scholar] [CrossRef] [PubMed]
- Stonier, T. The evolution of machine intelligence. In Beyond Information: The Natural History of Intelligence; Springer: London, UK, 1992; pp. 107–133. [Google Scholar] [CrossRef]
- Poole, D.; Mackworth, A.; Goebel, R. Computational Intelligence; Oxford University Press: Oxford, UK, 1998; Volume 1. [Google Scholar]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016. [Google Scholar]
- Krizhevsky, A.; Sutskever, I.; Hinton, G.E. Imagenet classification with deep convolutional neural networks. In Proceedings of the Advances in Neural information Processing Systems, Lake Tahoe, NV, USA, 3–6 December 2012; pp. 1097–1105. [Google Scholar]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436. [Google Scholar] [CrossRef] [PubMed]
- Ueda, D.; Shimazaki, A.; Miki, Y. Technical and clinical overview of deep learning in radiology. Jpn. J. Radiol. 2019, 37, 15–33. [Google Scholar] [CrossRef] [PubMed]
- Ghose, S.; Oliver, A.; Martí, R.; Lladó, X.; Vilanova, J.C.; Freixenet, J.; Mitra, J.; Sidibé, D.; Meriaudeau, F. A survey of prostate segmentation methodologies in ultrasound, magnetic resonance and computed tomography images. Comput. Methods Prog. Biomed. 2012, 108, 262–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasch, C.; Barillot, I.; Remeijer, P.; Touw, A.; van Herk, M.; Lebesque, J.V. Definition of the prostate in CT and MRI: A multi-observer study. Int. J. Radiat. Oncol. Biol. Phys. 1999, 43, 57–66. [Google Scholar] [CrossRef]
- Kachouie, N.N.; Fieguth, P.; Rahnamayan, S. An elliptical level set method for automatic TRUS prostate image segmentation. In Proceedings of the 2006 IEEE International Symposium on Signal Processing and Information Technology, Vancouver, BC, Canada, 27–30 August 2006; pp. 191–196. [Google Scholar]
- Ko, J.S.; Landis, P.; Carter, H.B.; Partin, A.W. Effect of intra-observer variation in prostate volume measurement on prostate-specific antigen density calculations among prostate cancer active surveillance participants. BJU Int. 2011, 108, 1739–1742. [Google Scholar] [CrossRef]
- Dianat, S.S.; Ruiz, R.M.R.; Bonekamp, D.; Carter, H.B.; Macura, K.J. Prostate volumetric assessment by magnetic resonance imaging and transrectal ultrasound: Impact of variation in calculated prostate-specific antigen density on patient eligibility for active surveillance program. J. Comput. Assist. Tomogr. 2013, 37, 589–595. [Google Scholar] [CrossRef]
- Bezinque, A.; Moriarity, A.; Farrell, C.; Peabody, H.; Noyes, S.L.; Lane, B.R. Determination of prostate volume: A comparison of contemporary methods. Acad. Radiol. 2018, 25, 1582–1587. [Google Scholar] [CrossRef] [PubMed]
- Rundo, L.; Militello, C.; Russo, G.; Garufi, A.; Vitabile, S.; Gilardi, M.C.; Mauri, G. Automated prostate gland segmentation based on an unsupervised fuzzy C-means clustering technique using multispectral T1w and T2w MR imaging. Information 2017, 8, 49. [Google Scholar] [CrossRef] [Green Version]
- Zou, K.H.; Warfield, S.K.; Bharatha, A.; Tempany, C.M.; Kaus, M.R.; Haker, S.J.; Wells III, W.M.; Jolesz, F.A.; Kikinis, R. Statistical validation of image segmentation quality based on a spatial overlap index1: Scientific reports. Acad. Radiol. 2004, 11, 178–189. [Google Scholar] [CrossRef] [Green Version]
- Litjens, G.; Toth, R.; van de Ven, W.; Hoeks, C.; Kerkstra, S.; van Ginneken, B.; Vincent, G.; Guillard, G.; Birbeck, N.; Zhang, J.; et al. Evaluation of prostate segmentation algorithms for MRI: The PROMISE12 challenge. Med. Image Anal. 2014, 18, 359–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karimi, D.; Samei, G.; Kesch, C.; Nir, G.; Salcudean, S.E. Prostate segmentation in MRI using a convolutional neural network architecture and training strategy based on statistical shape models. Int. J. Comput. Assist. Radiol. Surg. 2018. [Google Scholar] [CrossRef] [PubMed]
- Tian, Z.; Liu, L.; Zhang, Z.; Fei, B. PSNet: Prostate segmentation on MRI based on a convolutional neural network. J. Med. Imaging 2018, 5, 021208. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-net: Convolutional networks for biomedical image segmentation. In Proceedings of the 2015 International Conference on Medical Image Computing and Computer-Assisted Intervention, Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar]
- Clark, T.; Wong, A.; Haider, M.A.; Khalvati, F. Fully Deep Convolutional Neural Networks for Segmentation of the Prostate Gland in Diffusion-Weighted MR Images; Springer: Cham, Switzerland, 2017; pp. 97–104. [Google Scholar]
- Zhu, Y.; Wei, R.; Gao, G.; Ding, L.; Zhang, X.; Wang, X.; Zhang, J. Fully automatic segmentation on prostate MR images based on cascaded fully convolution network. J. Magn. Reson. Imaging 2018, 49, 1149–1156. [Google Scholar] [CrossRef]
- Zhu, Q.; Du, B.; Turkbey, B.; Choyke, P.L.; Yan, P. Deeply-supervised CNN for prostate segmentation. In Proceedings of the 2017 International Joint Conference on Neural Networks (IJCNN), Anchorage, AK, USA, 14–19 May 2017; pp. 178–184. [Google Scholar]
- Milletari, F.; Navab, N.; Ahmadi, S.-A. V-net: Fully convolutional neural networks for volumetric medical image segmentation. In Proceedings of the 2016 Fourth International Conference on 3D Vision (3DV), Stanford, CA, USA, 25–28 October 2016; pp. 565–571. [Google Scholar]
- Wang, B.; Lei, Y.; Tian, S.; Wang, T.; Liu, Y.; Patel, P.; Jani, A.B.; Mao, H.; Curran, W.J.; Liu, T.; et al. Deeply supervised 3D fully convolutional networks with group dilated convolution for automatic MRI prostate segmentation. Med. Phys. 2019, 46, 1707–1718. [Google Scholar] [CrossRef]
- Cheng, R.; Roth, H.R.; Lu, L.; Wang, S.; Turkbey, B.; Gandler, W.; McCreedy, E.S.; Agarwal, H.K.; Choyke, P.; Summers, R.M. Active appearance model and deep learning for more accurate prostate segmentation on MRI. In Proceedings of the Medical Imaging 2016: Image Processing, San Diego, CA, USA, 27 February–3 March 2016; p. 97842I. [Google Scholar]
- Le Nobin, J.; Orczyk, C.; Deng, F.M.; Melamed, J.; Rusinek, H.; Taneja, S.S.; Rosenkrantz, A.B. Prostate tumour volumes: Evaluation of the agreement between magnetic resonance imaging and histology using novel co-registration software. BJU Int. 2014, 114, E105–E112. [Google Scholar] [CrossRef] [Green Version]
- Van Schie, M.A.; Dinh, C.V.; van Houdt, P.J.; Pos, F.J.; Heijmink, S.W.; Kerkmeijer, L.G.; Kotte, A.N.; Oyen, R.; Haustermans, K.; van der Heide, U.A. Contouring of prostate tumors on multiparametric MRI: Evaluation of clinical delineations in a multicenter radiotherapy trial. Radiother. Oncol. 2018, 128, 321–326. [Google Scholar] [CrossRef]
- Lay, N.; Tsehay, Y.; Greer, M.D.; Turkbey, B.; Kwak, J.T.; Choyke, P.L.; Pinto, P.; Wood, B.J.; Summers, R.M. Detection of prostate cancer in multiparametric MRI using random forest with instance weighting. J. Med. Imaging (Bellingham) 2017, 4, 024506. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.I.; Zelefsky, M.J.; Sjoberg, D.D.; Nelson, J.B.; Egevad, L.; Magi-Galluzzi, C.; Vickers, A.J.; Parwani, A.V.; Reuter, V.E.; Fine, S.W. A contemporary prostate cancer grading system: A validated alternative to the Gleason score. Eur. Urol. 2016, 69, 428–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sumathipala, Y.; Lay, N.; Turkbey, B.; Smith, C.; Choyke, P.L.; Summers, R.M. Prostate cancer detection from multi-institution multiparametric MRIs using deep convolutional neural networks. J. Med. Imaging 2018, 5, 044507. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Baxter, J.S.; Akin, O.; Cantor-Rivera, D. Prostate cancer detection using residual networks. Int. J. Comput. Assist. Radiol. Surg. 2019, 14, 1647–1650. [Google Scholar] [CrossRef]
- Tsehay, Y.K.; Lay, N.S.; Roth, H.R.; Wang, X.; Kwak, J.T.; Turkbey, B.I.; Pinto, P.A.; Wood, B.J.; Summers, R.M. Convolutional neural network based deep-learning architecture for prostate cancer detection on multiparametric magnetic resonance images. In Medical Imaging 2017: Computer-Aided Diagnosis; SPIE: Bellingham, WA, USA, 2017; p. 1013405. [Google Scholar] [CrossRef]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Deep residual learning for image recognition. In Proceedings of the 2016 IEEE Conference on Computer Vision and Pattern Recognition, Las vegas, NV, USA, 26 June–1 July 2016; pp. 770–778. [Google Scholar]
- Liu, X.; Langer, D.L.; Haider, M.A.; Yang, Y.; Wernick, M.N.; Yetik, I.S. Prostate cancer segmentation with simultaneous estimation of Markov random field parameters and class. IEEE Trans. Med. Imaging 2009, 28, 906–915. [Google Scholar] [CrossRef]
- Kohl, S.; Bonekamp, D.; Schlemmer, H.-P.; Yaqubi, K.; Hohenfellner, M.; Hadaschik, B.; Radtke, J.-P.; Maier-Hein, K. Adversarial networks for the detection of aggressive prostate cancer. ArXiv 2017, arXiv:1702.08014. [Google Scholar]
- Dai, Z.; Carver, E.; Liu, C.; Lee, J.; Feldman, A.; Zong, W.; Pantelic, M.; Elshaikh, M.; Wen, N. Segmentation of the Prostatic Gland and the Intraprostatic Lesions on Multiparametic MRI Using Mask-RCNN. ArXiv 2019, arXiv:1904.02575. [Google Scholar]
- Dickinson, L.; Ahmed, H.U.; Allen, C.; Barentsz, J.O.; Carey, B.; Futterer, J.J.; Heijmink, S.W.; Hoskin, P.; Kirkham, A.P.; Padhani, A.R. Scoring systems used for the interpretation and reporting of multiparametric MRI for prostate cancer detection, localization, and characterization: Could standardization lead to improved utilization of imaging within the diagnostic pathway? J. Magn. Reson. Imaging 2013, 37, 48–58. [Google Scholar] [CrossRef]
- Nguyentat, M.; Ushinsky, A.; Miranda-Aguirre, A.; Uchio, E.; Lall, C.; Shirkhoda, L.; Lee, T.; Green, C.; Houshyar, R. Validation of Prostate Imaging-Reporting and Data System Version 2: A Retrospective Analysis. Curr. Probl. Diagn. Radiol. 2018, 47, 404–409. [Google Scholar] [CrossRef]
- Litjens, G.J.; Barentsz, J.O.; Karssemeijer, N.; Huisman, H.J. Clinical evaluation of a computer-aided diagnosis system for determining cancer aggressiveness in prostate MRI. Eur. Radiol. 2015, 25, 3187–3199. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Wu, C.-J.; Bao, M.-L.; Zhang, J.; Wang, X.-N.; Zhang, Y.-D. Machine learning-based analysis of MR radiomics can help to improve the diagnostic performance of PI-RADS v2 in clinically relevant prostate cancer. Eur. Radiol. 2017, 27, 4082–4090. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Zhang, Y.D.; Yan, X.; Liu, H.; Zhou, M.; Hu, B.; Yang, G. Computer-aided diagnosis of prostate cancer using a deep convolutional neural network from multiparametric MRI. J. Magn. Reson. Imaging 2018, 48, 1570–1577. [Google Scholar] [CrossRef] [PubMed]
- Kwak, J.T.; Xu, S.; Wood, B.J.; Turkbey, B.; Choyke, P.L.; Pinto, P.A.; Wang, S.; Summers, R.M. Automated prostate cancer detection using T2-weighted and high-b-value diffusion-weighted magnetic resonance imaging. Med. Phys. 2015, 42, 2368–2378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Z.; Liu, C.; Cheng, D.; Wang, L.; Yang, X.; Cheng, K.-T. Automated detection of clinically significant prostate cancer in mp-MRI images based on an end-to-end deep neural network. IEEE Trans. Med. Imaging 2018, 37, 1127–1139. [Google Scholar] [CrossRef]
- Seah, J.C.; Tang, J.S.; Kitchen, A. Detection of prostate cancer on multiparametric MRI. In Proceedings of the Medical Imaging 2017: Computer-Aided Diagnosis, Orlando, FL, USA, 13–16 February 2017; p. 1013429. [Google Scholar]
- Liu, S.; Zheng, H.; Feng, Y.; Li, W. Prostate cancer diagnosis using deep learning with 3D multiparametric MRI. In Proceedings of the Medical Imaging 2017: Computer-Aided Diagnosis, Orlando, FL, USA, 13–16 February 2017; p. 1013428. [Google Scholar]
- Mehrtash, A.; Sedghi, A.; Ghafoorian, M.; Taghipour, M.; Tempany, C.M.; Wells, W.M., III; Kapur, T.; Mousavi, P.; Abolmaesumi, P.; Fedorov, A. Classification of clinical significance of MRI prostate findings using 3D convolutional neural networks. Proc. Spie Int. Soc. Opt. Eng. 2017, 10134. [Google Scholar] [CrossRef] [Green Version]
- Chen, Q.; Hu, S.; Long, P.; Lu, F.; Shi, Y.; Li, Y. A transfer learning approach for malignant prostate lesion detection on multiparametric MRI. Technol. Cancer Res. Treat. 2019, 18. [Google Scholar] [CrossRef]
- Armato, S.G.; Huisman, H.; Drukker, K.; Hadjiiski, L.; Kirby, J.S.; Petrick, N.; Redmond, G.; Giger, M.L.; Cha, K.; Mamonov, A. PROSTATEx Challenges for computerized classification of prostate lesions from multiparametric magnetic resonance images. J. Med. Imaging 2018, 5, 044501. [Google Scholar] [CrossRef]
- Hu, X.; Cammann, H.; Meyer, H.-A.; Miller, K.; Jung, K.; Stephan, C. Artificial neural networks and prostate cancer—Tools for diagnosis and management. Nat. Rev. Urol. 2013, 10, 174. [Google Scholar] [CrossRef]
- Chen, T.; Li, M.; Gu, Y.; Zhang, Y.; Yang, S.; Wei, C.; Wu, J.; Li, X.; Zhao, W.; Shen, J. Prostate cancer differentiation and aggressiveness: Assessment with a radiomic-based model vs. PI-RADS v2. J. Magn. Reson. Imaging 2019, 49, 875–884. [Google Scholar] [CrossRef] [Green Version]
- European Society of Radiology. What the radiologist should know about artificial intelligence—An ESR white paper. Insights Imaging 2019, 10, 44. [Google Scholar] [CrossRef] [Green Version]
- Nicolae, A.; Morton, G.; Chung, H.; Loblaw, A.; Jain, S.; Mitchell, D.; Lu, L.; Helou, J.; Al-Hanaqta, M.; Heath, E.; et al. Evaluation of a machine-learning algorithm for treatment planning in prostate low-dose-rate brachytherapy. Int. J. Radiat. Oncol. Biol. Phys. 2017, 97, 822–829. [Google Scholar] [CrossRef]
- Wong, N.C.; Lam, C.; Patterson, L.; Shayegan, B. Use of machine learning to predict early biochemical recurrence after robot-assisted prostatectomy. BJU Int. 2019, 123, 51–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cordon-Cardo, C.; Kotsianti, A.; Verbel, D.A.; Teverovskiy, M.; Capodieci, P.; Hamann, S.; Jeffers, Y.; Clayton, M.; Elkhettabi, F.; Khan, F.M.; et al. Improved prediction of prostate cancer recurrence through systems pathology. J. Clin. Invest. 2007, 117, 1876–1883. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Year | ML Algorithm | Patients | Dice | Modalities |
|---|---|---|---|---|---|
| Rundo et al. [67] | 2017 | Fuzzy C-means clustering. Features: T1 intensity, T2 intensity | 21 | 0.91 | T1W, T2W |
| Tian et al. [71] | 2018 | CNN: 7 layers | 140 | 0.85 | T2W |
| Karimi et al. [70] | 2018 | CNN: 3 layers | 49 | 0.88 | T2W |
| Clark et al. [73] | 2017 | CNN: U-Net | 134 | 0.89 | DWI |
| Zhu, Y. et al. [74] | 2018 | CNN: U-Net | 163 | 0.93 | DWI, T2W |
| Zhu, Q. et al. [75] | 2017 | CNN: U-Net | 81 | 0.89 | T2W |
| Milletari et al. [76] | 2016 | CNN: V-Net | 80 | 0.87 | T2W |
| Wang, B. et al. [77] | 2019 | CNN: 3D DSD-FCN | 40 | 0.86 | T2W |
| Cheng et al. [78] | 2016 | CNN and Active Appearance Model | 120 | 0.93 | T2W |
| Reference | Year | ML Algorithm | Patients | Lesions | AUC | Modalities |
|---|---|---|---|---|---|---|
| Lay et al. [81] | 2017 | Random Forest. Features: Intensity, Haralick texture | 224 | 410 | 0.93 | T2W, ADC, DWI |
| Sumathipala et al. [83] | 2018 | CNN: Holistically Nested Edge Detection | 186 | N/A | 0.93 | T2W, ADC, DWI |
| Xu et al. [84] | 2019 | CNN: ResNet | 346 | N/A | 0.97 | T2W, ADC, DWI |
| Tsehay et al. [85] | 2017 | CNN, 5 Layers | 52 | 125 | 0.90 | T2W, ADC, DWI |
| Reference | Year | ML Algorithm | Patients | Dice | Modalities |
|---|---|---|---|---|---|
| Dai et al. [89] | 2019 | CNN: Mask R-CNN | 63 | 0.46 | T2W, ADC |
| Kohl et al. [88] | 2017 | Adversarial Network and CNN: U-Net | 152 | 0.41 | T2W, ADC, DWI |
| Liu et al. [87] | 2009 | Fuzzy Markov Random Fields | 11 | 0.62 | T2W, quantitative T2, DWI, DCE |
| Reference | Year | Algorithm | Patients | Lesions | AUC | Modalities |
|---|---|---|---|---|---|---|
| Litjens et al. [92] | 2015 | Random Forest. Features: Intensity, Position, Pharmacokinetic, Texture, Spatial Filter | 107 | 141 | Benign vs. Cancer; AUC increased from 0.81 to 0.88 with their ML tool Indolent vs. Aggressive; AUC increased from 0.78 to 0.88 with their ML tool | T2W, DCE, DWI |
| Wang, J. et al. [93] | 2017 | SVM. Features: Volumetric Radiomics | 54 | 149 | 0.95 | T2W, DWI |
| Song et al. [94] | 2018 | CNN: Deep CNN and Augmentation | 195 | 547 | 0.94 | T2W, ADC, DWI |
| Kwak et al. [95] | 2015 | SVM. Features: Texture | 244 | 479 | 0.89 | T2W, DWI |
| Wang, Z. et al. [96] | 2018 | CNN: Deep CNN | 360 | 600 | 0.96 | T2W, ADC |
| Seah et al. [97] | 2017 | CNN: Deep CNN | 346 | 538 | 0.84 | T2W, ADC, DCE |
| Liu et al. [98] | 2017 | CNN: XmasNet | 341 | 538 | 0.84 | T2W, ADC, DWI, Ktrans |
| Mehrtash et al. [99] | 2017 | CNN: 3D Implementation | 344 | 538 | 0.80 | ADC, DWI, DCE |
| Chen et al. [100] | 2019 | Two CNNs: Inception V3 and VGG-16 | Training Data: 204 Test Data: N/A | 538 | Inception V3, 0.81 VGG-16, 0.83 | T2W, DWI, DCE |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bardis, M.D.; Houshyar, R.; Chang, P.D.; Ushinsky, A.; Glavis-Bloom, J.; Chahine, C.; Bui, T.-L.; Rupasinghe, M.; Filippi, C.G.; Chow, D.S. Applications of Artificial Intelligence to Prostate Multiparametric MRI (mpMRI): Current and Emerging Trends. Cancers 2020, 12, 1204. https://doi.org/10.3390/cancers12051204
Bardis MD, Houshyar R, Chang PD, Ushinsky A, Glavis-Bloom J, Chahine C, Bui T-L, Rupasinghe M, Filippi CG, Chow DS. Applications of Artificial Intelligence to Prostate Multiparametric MRI (mpMRI): Current and Emerging Trends. Cancers. 2020; 12(5):1204. https://doi.org/10.3390/cancers12051204
Chicago/Turabian StyleBardis, Michelle D., Roozbeh Houshyar, Peter D. Chang, Alexander Ushinsky, Justin Glavis-Bloom, Chantal Chahine, Thanh-Lan Bui, Mark Rupasinghe, Christopher G. Filippi, and Daniel S. Chow. 2020. "Applications of Artificial Intelligence to Prostate Multiparametric MRI (mpMRI): Current and Emerging Trends" Cancers 12, no. 5: 1204. https://doi.org/10.3390/cancers12051204