Haute Couture or Ready-To-Wear? Tailored Pelvic Radiotherapy for Prostate Cancer Based on Individualized Sentinel Lymph Node Detection

 ,
, 
Abstract
:1. Introduction
2. Results
2.1. Patient Population
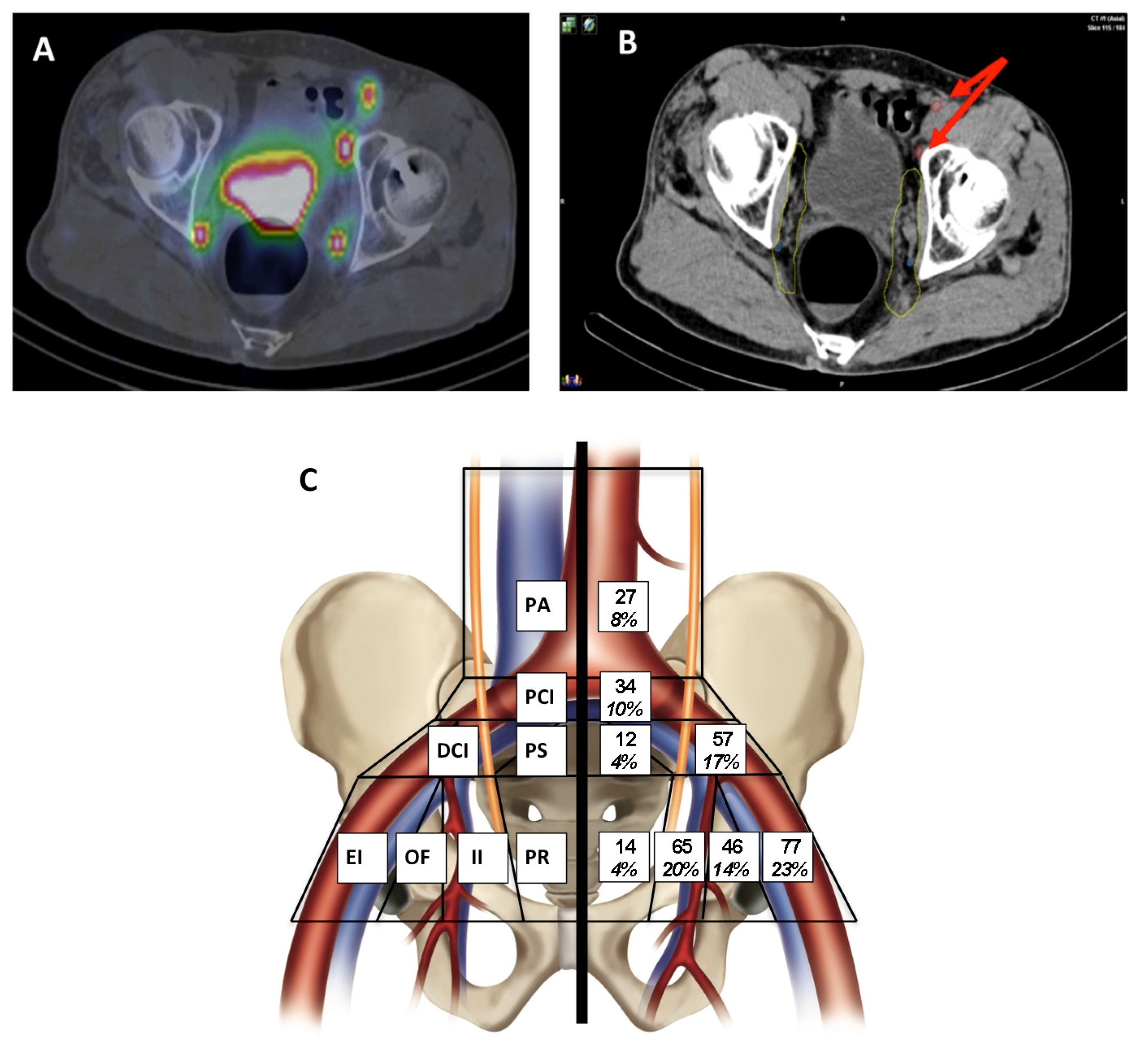
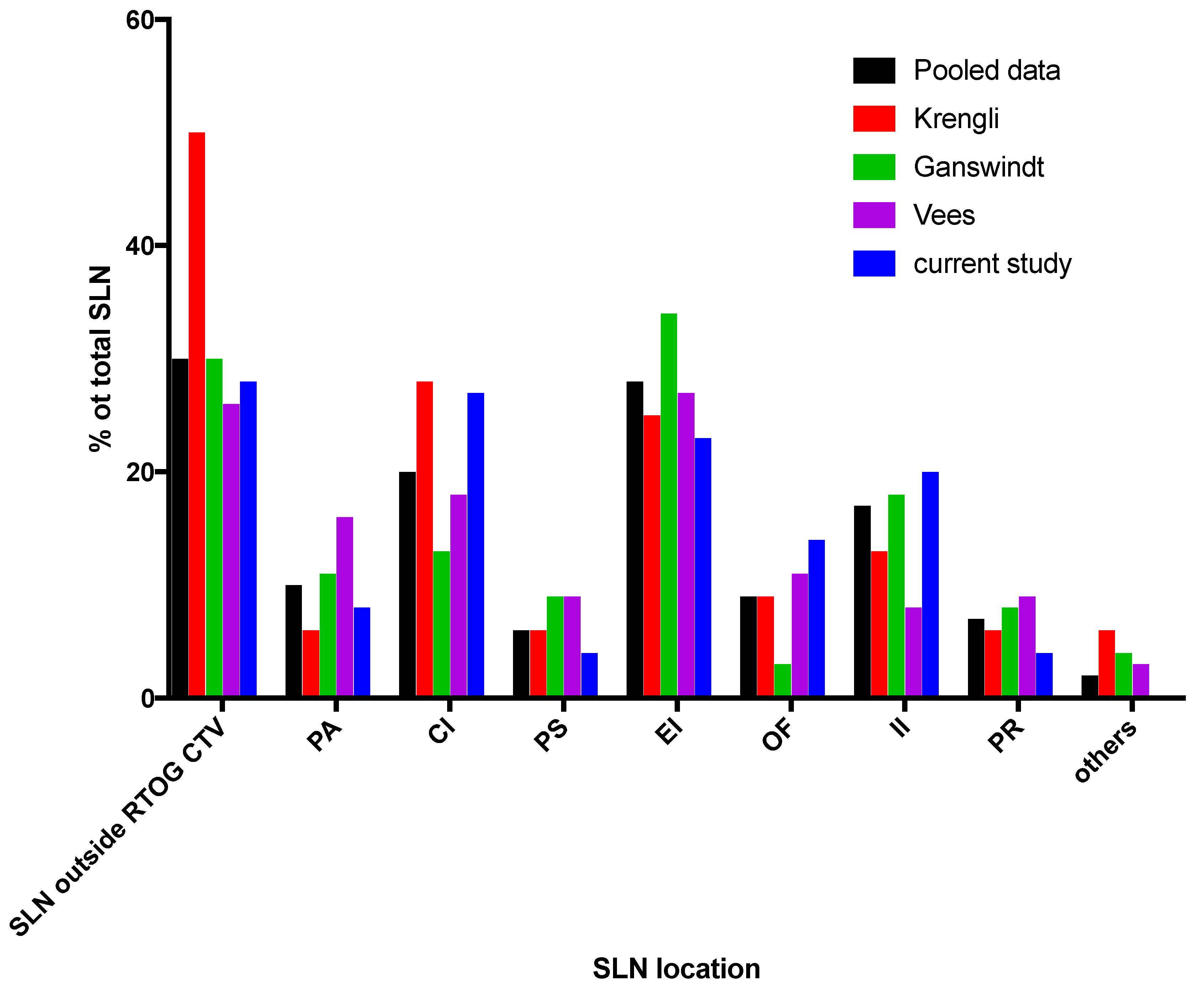
2.2. Anatomical Distribution of SLN on Lymphoscintigraphy
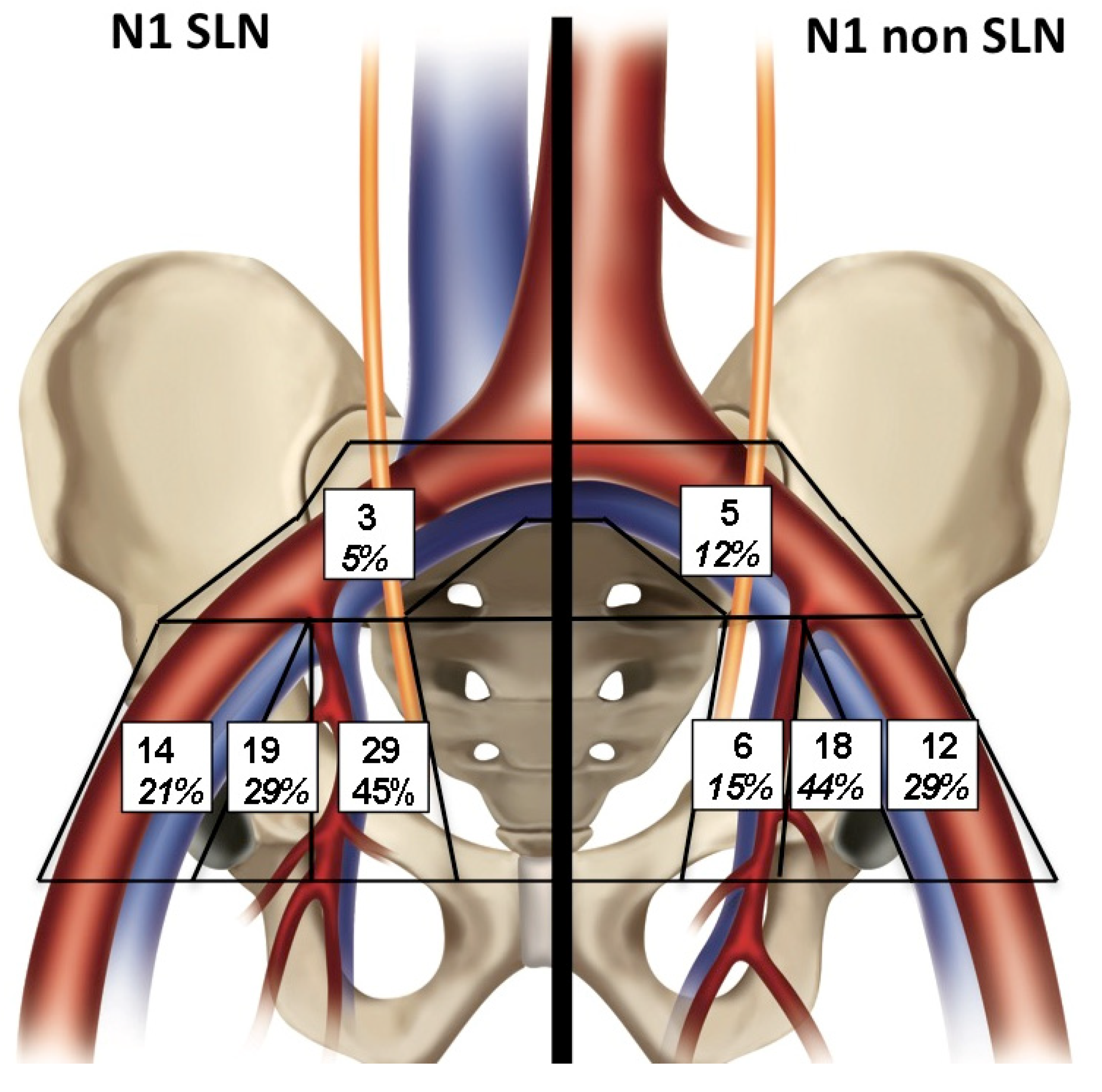
2.3. Histological Distribution of Metastatic and Non Metastatic SLNs
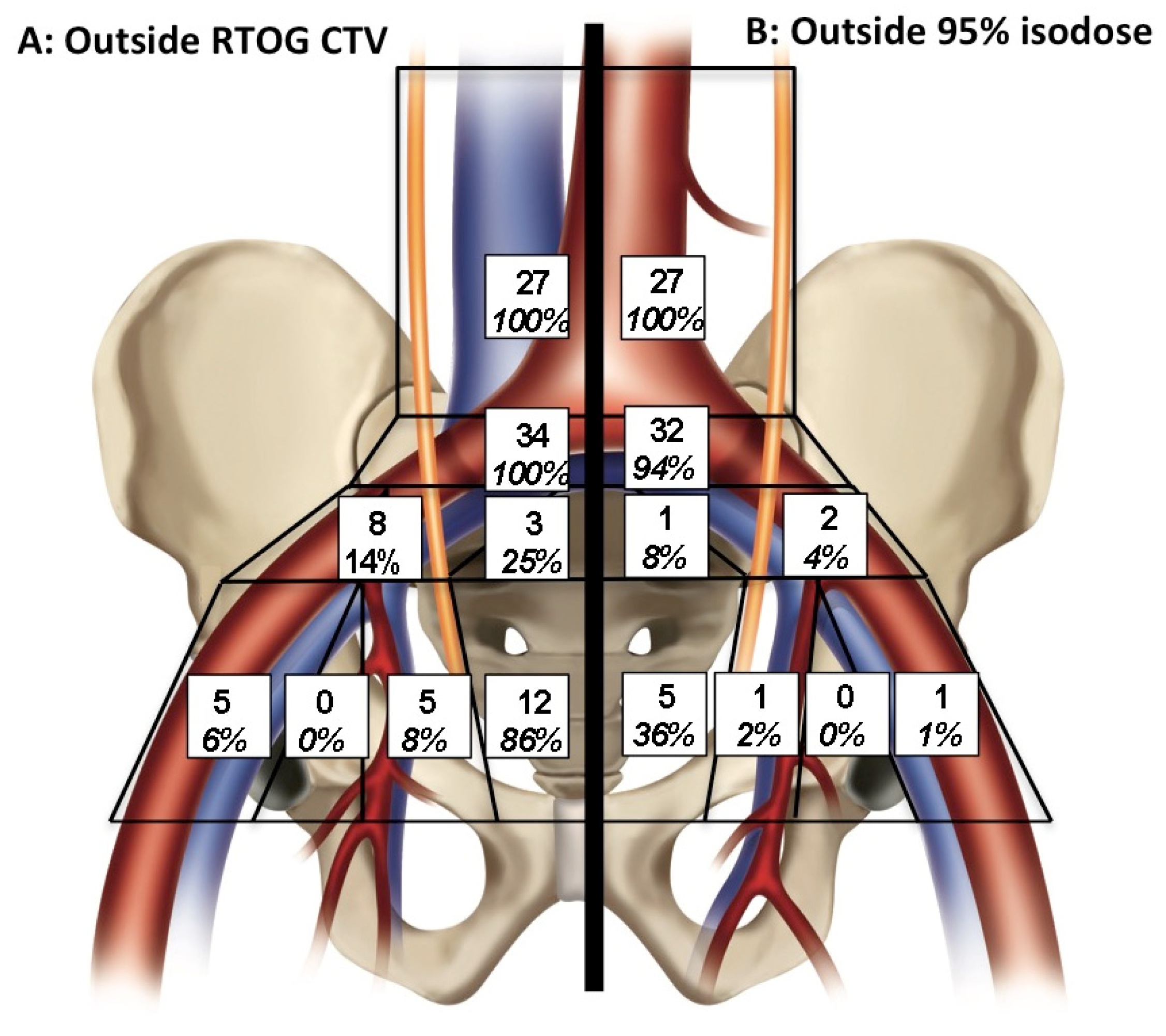
2.4. Pelvic Radiotherapy SLN Dose Distribution
2.5. Distance between SLN and Regional Blood Vessels
3. Discussion
4. Patients and Methods
4.1. Population
4.2. Lymphoscintigraphy
4.3. Target Volumes Definition
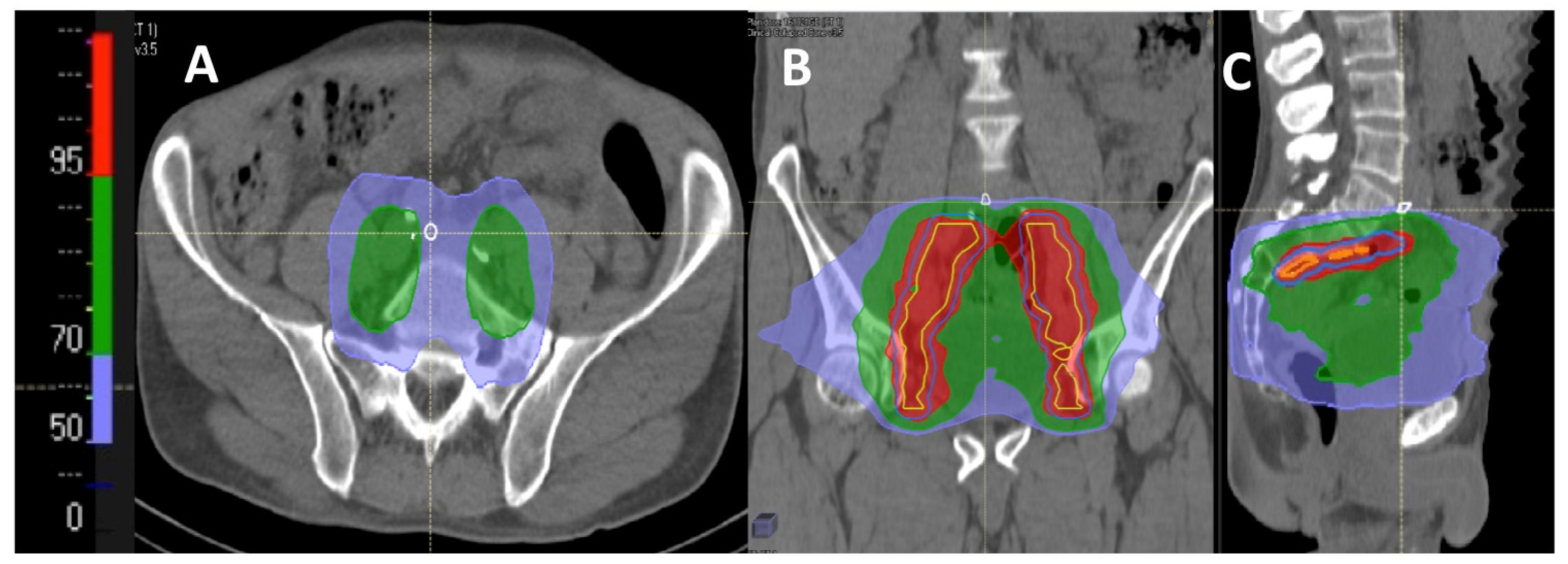
4.4. Dosimetric Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bubendorf, L.; Schopfer, A.; Wagner, U.; Sauter, G.; Moch, H.; Willi, N.; Gasser, T.C.; Mihatsch, M.J. Metastatic patterns of prostate cancer: An autopsy study of 1589 patients. Hum. Pathol. 2000, 31, 578–583. [Google Scholar] [CrossRef]
- Cheng, L.; Zincke, H.; Blute, M.L.; Bergstralh, E.J.; Scherer, B.; Bostwick, D.G. Risk of prostate carcinoma death in patients with lymph node metastasis. Cancer 2001, 91, 66–73. [Google Scholar] [CrossRef]
- Martin, J.M.; Supiot, S.; Berthold, D.R. Pharmacotherapeutic management of locally advanced prostate cancer: Current status. Drugs 2011, 71, 1019–1041. [Google Scholar] [CrossRef]
- Pommier, P.; Chabaud, S.; Lagrange, J.L.; Richaud, P.; Lesaunier, F.; Le Prise, E.; Wagner, J.P.; Hay, M.H.; Beckendorf, V.; Suchaud, J.P.; et al. Is there a role for pelvic irradiation in localized prostate adenocarcinoma? Preliminary results of GETUG-01. J. Clin. Oncol. 2007, 25, 5366–5373. [Google Scholar] [CrossRef]
- Roach, M., III; Marquez, C.; Yuo, H.S.; Narayan, P.; Coleman, L.; Nseyo, U.O.; Navvab, Z.; Carroll, P.R. Predicting the risk of lymph node involvement using the pre-treatment prostate specific antigen and Gleason score in men with clinically localized prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 1994, 28, 33–37. [Google Scholar] [CrossRef]
- Roach, M.; Moughan, J.; Lawton, C.A.F.; Dicker, A.P.; Zeitzer, K.L.; Gore, E.M.; Kwok, Y.; Seider, M.J.; Hsu, I.C.; Hartford, A.C.; et al. Sequence of hormonal therapy and radiotherapy field size in unfavourable, localised prostate cancer (NRG/RTOG 9413): Long-term results of a randomised, phase 3 trial. Lancet Oncol. 2018, 19, 1504–1515. [Google Scholar] [CrossRef]
- Heemsbergen, W.D.; Al-Mamgani, A.; Witte, M.G.; van Herk, M.; Lebesque, J.V. Radiotherapy with rectangular fields is associated with fewer clinical failures than conformal fields in the high-risk prostate cancer subgroup: Results from a randomized trial. Radiother. Oncol. 2013, 107, 134–139. [Google Scholar] [CrossRef]
- Sargos, P.; Guerif, S.; Latorzeff, I.; Hennequin, C.; Pommier, P.; Lagrange, J.L.; Crehange, G.; Chapet, O.; de Crevoisier, R.; Azria, D.; et al. Definition of lymph node areas for radiotherapy of prostate cancer: A critical literature review by the French Genito-Urinary Group and the French Association of Urology (GETUG-AFU). Cancer Treat. Rev. 2015, 41, 814–820. [Google Scholar] [CrossRef]
- Lawton, C.A.; Michalski, J.; El-Naqa, I.; Buyyounouski, M.K.; Lee, W.R.; Menard, C.; O’Meara, E.; Rosenthal, S.A.; Ritter, M.; Seider, M. RTOG GU Radiation oncology specialists reach consensus on pelvic lymph node volumes for high-risk prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 383–387. [Google Scholar] [CrossRef] [Green Version]
- Krengli, M.; Ballare, A.; Cannillo, B.; Rudoni, M.; Kocjancic, E.; Loi, G.; Brambilla, M.; Inglese, E.; Frea, B. Potential advantage of studying the lymphatic drainage by sentinel node technique and SPECT-CT image fusion for pelvic irradiation of prostate cancer. Int. J. Radiat. Oncol. Biol. Phys. 2006, 66, 1100–1104. [Google Scholar] [CrossRef]
- Shih, H.A.; Harisinghani, M.; Zietman, A.L.; Wolfgang, J.A.; Saksena, M.; Weissleder, R. Mapping of nodal disease in locally advanced prostate cancer: Rethinking the clinical target volume for pelvic nodal irradiation based on vascular rather than bony anatomy. Int. J. Radiat. Oncol. Biol. Phys. 2005, 63, 1262–1269. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, R.; Wilson, T.G. Sentinel node evaluation in prostate cancer. Clin. Exp. Metastasis 2018, 35, 471–485. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, C.; Rousseau, T.; Campion, L.; Lacoste, J.; Aillet, G.; Potiron, E.; Lacombe, M.; Le Coguic, G.; Mathieu, C.; Kraeber-Bodere, F. Laparoscopic sentinel lymph node versus hyperextensive pelvic dissection for staging clinically localized prostate carcinoma: A prospective study of 200 patients. J. Nucl. Med. 2014, 55, 753–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wit, E.M.K.; Acar, C.; Grivas, N.; Yuan, C.; Horenblas, S.; Liedberg, F.; Valdes Olmos, R.A.; van Leeuwen, F.W.B.; van den Berg, N.S.; Winter, A.; et al. Sentinel Node Procedure in Prostate Cancer: A Systematic Review to Assess Diagnostic Accuracy. Eur. Urol. 2017, 71, 596–605. [Google Scholar] [CrossRef]
- Acar, C.; Kleinjan, G.H.; van den Berg, N.S.; Wit, E.M.; van Leeuwen, F.W.; van der Poel, H.G. Advances in sentinel node dissection in prostate cancer from a technical perspective. Int. J. Urol. 2015, 22, 898–909. [Google Scholar] [CrossRef] [Green Version]
- Grivas, N.; Wit, E.M.K.; Kuusk, T.; KleinJan, G.H.; Donswijk, M.L.; van Leeuwen, F.W.B.; van der Poel, H.G. The Impact of Adding Sentinel Node Biopsy to Extended Pelvic Lymph Node Dissection on Biochemical Recurrence in Prostate Cancer Patients Treated with Robot-Assisted Radical Prostatectomy. J. Nucl. Med. 2018, 59, 204–209. [Google Scholar] [CrossRef] [Green Version]
- Holl, G.; Dorn, R.; Wengenmair, H.; Weckermann, D.; Sciuk, J. Validation of sentinel lymph node dissection in prostate cancer: Experience in more than 2000 patients. Eur. J. Nucl. Med. Mol. Imaging 2009, 36, 1377–1382. [Google Scholar] [CrossRef]
- Ganswindt, U.; Paulsen, F.; Corvin, S.; Hundt, I.; Alber, M.; Frey, B.; Stenzl, A.; Bares, R.; Bamberg, M.; Belka, C. Optimized coverage of high-risk adjuvant lymph node areas in prostate cancer using a sentinel node-based, intensity-modulated radiation therapy technique. Int. J. Radiat. Oncol. Biol. Phys. 2007, 67, 347–355. [Google Scholar] [CrossRef]
- Ganswindt, U.; Schilling, D.; Muller, A.C.; Bares, R.; Bartenstein, P.; Belka, C. Distribution of prostate sentinel nodes: A SPECT-derived anatomic atlas. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 1364–1372. [Google Scholar] [CrossRef]
- Vees, H.; Steiner, C.; Dipasquale, G.; Chouiter, A.; Zilli, T.; Velazquez, M.; Namy, S.; Ratib, O.; Buchegger, F.; Miralbell, R. Target volume definition in high-risk prostate cancer patients using sentinel node SPECT/CT and 18 F-choline PET/CT. Radiat. Oncol. 2012, 7, 134. [Google Scholar] [CrossRef] [Green Version]
- Spratt, D.E.; Vargas, H.A.; Zumsteg, Z.S.; Golia Pernicka, J.S.; Osborne, J.R.; Pei, X.; Zelefsky, M.J. Patterns of Lymph Node Failure after Dose-escalated Radiotherapy: Implications for Extended Pelvic Lymph Node Coverage. Eur. Urol. 2017, 71, 37–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lepinoy, A.; Cochet, A.; Cueff, A.; Cormier, L.; Martin, E.; Maingon, P.; Bosset, J.F.; Brunotte, F.; Crehange, G. Pattern of occult nodal relapse diagnosed with (18)F-fluoro-choline PET/CT in prostate cancer patients with biochemical failure after prostate-only radiotherapy. Radiother. Oncol. 2014, 111, 120–125. [Google Scholar] [CrossRef] [PubMed]
- Murray, J.R.; Roach Iii, M. Role of Para-aortic Radiotherapy in the Management of Prostate Cancer. Clin. Oncol. (R. Coll. Radiol.) 2020, 32, 189–198. [Google Scholar] [CrossRef]
- Dinniwell, R.; Chan, P.; Czarnota, G.; Haider, M.A.; Jhaveri, K.; Jewett, M.; Fyles, A.; Jaffray, D.; Milosevic, M. Pelvic lymph node topography for radiotherapy treatment planning from ferumoxtran-10 contrast-enhanced magnetic resonance imaging. Int. J. Radiat. Oncol. Biol. Phys. 2009, 74, 844–851. [Google Scholar] [CrossRef]
- Hegemann, N.S.; Wenter, V.; Spath, S.; Kusumo, N.; Li, M.; Bartenstein, P.; Fendler, W.P.; Stief, C.; Belka, C.; Ganswindt, U. Distribution of prostate nodes: A PET/CT-derived anatomic atlas of prostate cancer patients before and after surgical treatment. Radiat. Oncol. 2016, 11, 37. [Google Scholar] [CrossRef] [Green Version]
- Doughton, J.A.; Hofman, M.S.; Eu, P.; Hicks, R.J.; Williams, S. A First-in-Human Study of (68)Ga-Nanocolloid PET/CT Sentinel Lymph Node Imaging in Prostate Cancer Demonstrates Aberrant Lymphatic Drainage Pathways. J. Nucl. Med. 2018, 59, 1837–1842. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.K.; Watson, T.; Denham, J.; Shakespeare, T.P.; Rutherford, N.; McLeod, N.; Picton, K.; Ainsworth, P.; Bonaventura, T.; Martin, J.M. Prostate-Specific Membrane Antigen Positron Emission Tomography-Computed Tomography for Prostate Cancer: Distribution of Disease and Implications for Radiation Therapy Planning. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 701–709. [Google Scholar] [CrossRef]
- Keenan, L.G.; Rock, K.; Azmi, A.; Salib, O.; Gillham, C.; McArdle, O. An atlas to aid delineation of para-aortic lymph node region in cervical cancer: Design and validation of contouring guidelines. Radiother. Oncol. 2018, 127, 417–422. [Google Scholar] [CrossRef]
- Takiar, V.; Fontanilla, H.P.; Eifel, P.J.; Jhingran, A.; Kelly, P.; Iyer, R.B.; Levenback, C.F.; Zhang, Y.; Dong, L.; Klopp, A. Anatomic distribution of fluorodeoxyglucose-avid para-aortic lymph nodes in patients with cervical cancer. Int. J. Radiat. Oncol. Biol. Phys. 2013, 85, 1045–1050. [Google Scholar] [CrossRef] [Green Version]
- Vees, H.; Dipasquale, G.; Nouet, P.; Zilli, T.; Cozzi, L.; Miralbell, R. Pelvic Lymph Node Irradiation Including Pararectal Sentinel Nodes for Prostate Cancer Patients: Treatment Optimization Comparing Intensity Modulated X-rays, Volumetric Modulated Arc Therapy, and Intensity Modulated Proton Therapy. Technol. Cancer Res. Treat. 2015, 14, 181–189. [Google Scholar] [CrossRef]
- Muller, A.C.; Eckert, F.; Paulsen, F.; Zips, D.; Stenzl, A.; Schilling, D.; Alber, M.; Bares, R.; Martus, P.; Weckermann, D.; et al. Nodal Clearance Rate and Long-Term Efficacy of Individualized Sentinel Node-Based Pelvic Intensity Modulated Radiation Therapy for High-Risk Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2016, 94, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Hinsenveld, F.J.; Wit, E.M.K.; van Leeuwen, P.J.; Brouwer, O.R.; Donswijk, M.L.; Tillier, C.N.; Vegt, E.; van Muilekom, H.A.M.; van Oosterom, M.N.; van Leeuwen, F.W.B.; et al. Prostate-specific membrane antigen positron emission tomography/computed tomography combined with sentinel node biopsy for primary lymph node staging in prostate cancer. J. Nucl. Med. 2020, 61, 540–545. [Google Scholar] [CrossRef] [PubMed]
- Rousseau, C.; Rousseau, T.; Mathieu, C.; Lacoste, J.; Potiron, E.; Aillet, G.; Nevoux, P.; Le Coguic, G.; Campion, L.; Kraeber-Bodere, F. Laparoscopic sentinel lymph node dissection in prostate cancer patients: The additional value depends on preoperative data. Eur. J. Nucl. Med. Mol. Imaging 2016, 43, 1849–1856. [Google Scholar] [CrossRef] [PubMed]
- Foster, B.; Bagci, U.; Mansoor, A.; Xu, Z.; Mollura, D.J. A review on segmentation of positron emission tomography images. Comput. Biol. Med. 2014, 50, 76–96. [Google Scholar] [CrossRef] [Green Version]
- Michalski, J.M.; Gay, H.; Jackson, A.; Tucker, S.L.; Deasy, J.O. Radiation dose-volume effects in radiation-induced rectal injury. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76 (Suppl. 3), S123–S129. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | n = 57 (%) |
|---|---|
| Median age, years (range) | 65 (51–78) |
| Tumor Stage | |
| T1 | 12 (21) |
| T2 | 30 (53) |
| T3 | 15 (26) |
| ISUP Grade | |
| Group 1 | 5 (9) |
| Group 2 | 15 (26) |
| Group 3 | 15 (26) |
| Group 4 | 14 (25) |
| Group 5 | 8 (14) |
| Percentage of positive biopsy cores (%) Mean, (median) Range | 50.5 (44) 5.2–100 |
| Initial PSA (ng/mL) Median, (range) | |
| <10 | 30 (53) |
| 10 to 20 | 16 (28) |
| >20 | 11 (19) |
| D’Amico risk grouping | |
| Intermediate risk | 20 (35) |
| High risk | 37 (65) |
| Location | Number of Metastatic Sentinel Lymph Nodes (% of Total) | Number of Metastatic Non-Sentinel Lymph Nodes (% of Total) | Total |
|---|---|---|---|
| CI | 3 (4.6) | 5 (12.2) | 8 (8.3) |
| II | 29 (44.6) | 6 (14.6) | 35 (36.5) |
| EI | 14 (21.5) | 12 (29.3) | 26 (27.1) |
| OF | 19 (29.3) | 18 (43.9) | 37 (28.1) |
| Total | 65 (100) | 41 (100) | 106 (100) |
| Location | Total SLN Number (%) | SLN NUMBER Outside RTOG CTV (%) |
|---|---|---|
| CI (PCI and DCI) | 89 (29.4) | 40 (44.9) |
| II | 65 (21.2) | 5 (7.7) |
| EI | 77 (25.2) | 5 (6.5) |
| OF | 46 (15.1) | 0 (0.0) |
| PS | 22 (7.1) | 13 (59.1) |
| PR | 6 (2.0) | 4 (66.7) |
| Total | 305 | 67 (22.0) |
| Region | Median Minimal Distance (mm) | Number of Lymph Nodes (%) Located within a CTV Based on an Expansion around Pelvic Blood Vessels | |||
|---|---|---|---|---|---|
| ≤10 mm | ≤12 mm | ≤15 mm | ≤20 mm | ||
| PA | 7 | 16 (61) | 19 (72) | 22 (83) | 27 (100) |
| PCI | 6 | 30 (88) | 31 (91) | 33 (97) | 34 (100) |
| DCI | 13.5 | 1 (13) | 4 (50) | 6 (75) | 8 (100) |
| II | 15 | 0 (0) | 2 (40) | 5 (100) | 5(100) |
| EI | 10 | 3 (60) | 4 (80) | 5 (100) | 5 (100) |
| Study | Current Study | Krengli | Ganswindt | Vees | Total | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Number of patients | 57 | 20 | 59 | 20 | 156 | |||||
| Total number of SLN | 332 | 32 | 324 | 104 | 792 | |||||
| Mean number of SLN/patient | 5.8 | 1.6 | 5.5 | 5.2 | 5.1 | |||||
| SLN outside RTOG CTV | n | (%) | n | (%) | n | (%) | n | (%) | n | (%) |
| 94 | (28) | 16 | (50) | 98 | (30) | 27 | (26) | 235 | (30) | |
| Distribution of SLN | ||||||||||
| PA | 27 | (8) | 2 | (6) | 35 | (11) | 17 | (16) | 81 | (10) |
| CI | 91 | (27) | 9 | (28) | 41 | (13) | 19 | (18) | 160 | (20) |
| PS | 12 | (4) | 2 | (6) | 28 | (9) | 9 | (9) | 51 | (6) |
| EI | 77 | (23) | 8 | (25) | 111 | (34) | 28 | (27) | 224 | (28) |
| OF | 46 | (14) | 3 | (9) | 10 | (3) | 11 | (11) | 70 | (9) |
| II | 65 | (20) | 4 | (13) | 58 | (18) | 8 | (8) | 135 | (17) |
| PR | 14 | (4) | 2 | (6) | 27 | (8) | 9 | (9) | 52 | (7) |
| Others | 0 | (0) | 2 | (6) | 14 | (4) | 3 | (3) | 19 | (2) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michaud, A.-V.; Samain, B.; Ferrer, L.; Fleury, V.; Dore, M.; Colombie, M.; Dupuy, C.; Rio, E.; Guimas, V.; Rousseau, T.; et al. Haute Couture or Ready-To-Wear? Tailored Pelvic Radiotherapy for Prostate Cancer Based on Individualized Sentinel Lymph Node Detection. Cancers 2020, 12, 944. https://doi.org/10.3390/cancers12040944
Michaud A-V, Samain B, Ferrer L, Fleury V, Dore M, Colombie M, Dupuy C, Rio E, Guimas V, Rousseau T, et al. Haute Couture or Ready-To-Wear? Tailored Pelvic Radiotherapy for Prostate Cancer Based on Individualized Sentinel Lymph Node Detection. Cancers. 2020; 12(4):944. https://doi.org/10.3390/cancers12040944
Chicago/Turabian StyleMichaud, Anne-Victoire, Benoit Samain, Ludovic Ferrer, Vincent Fleury, Melanie Dore, Mathilde Colombie, Claire Dupuy, Emmanuel Rio, Valentine Guimas, Thierry Rousseau, and et al. 2020. "Haute Couture or Ready-To-Wear? Tailored Pelvic Radiotherapy for Prostate Cancer Based on Individualized Sentinel Lymph Node Detection" Cancers 12, no. 4: 944. https://doi.org/10.3390/cancers12040944