Long-Term Neurodevelopmental Outcome of Children after in Utero Exposure to Chemotherapy

 , , , and
, , , and
Abstract
:Simple Summary
Abstract
1. Introduction
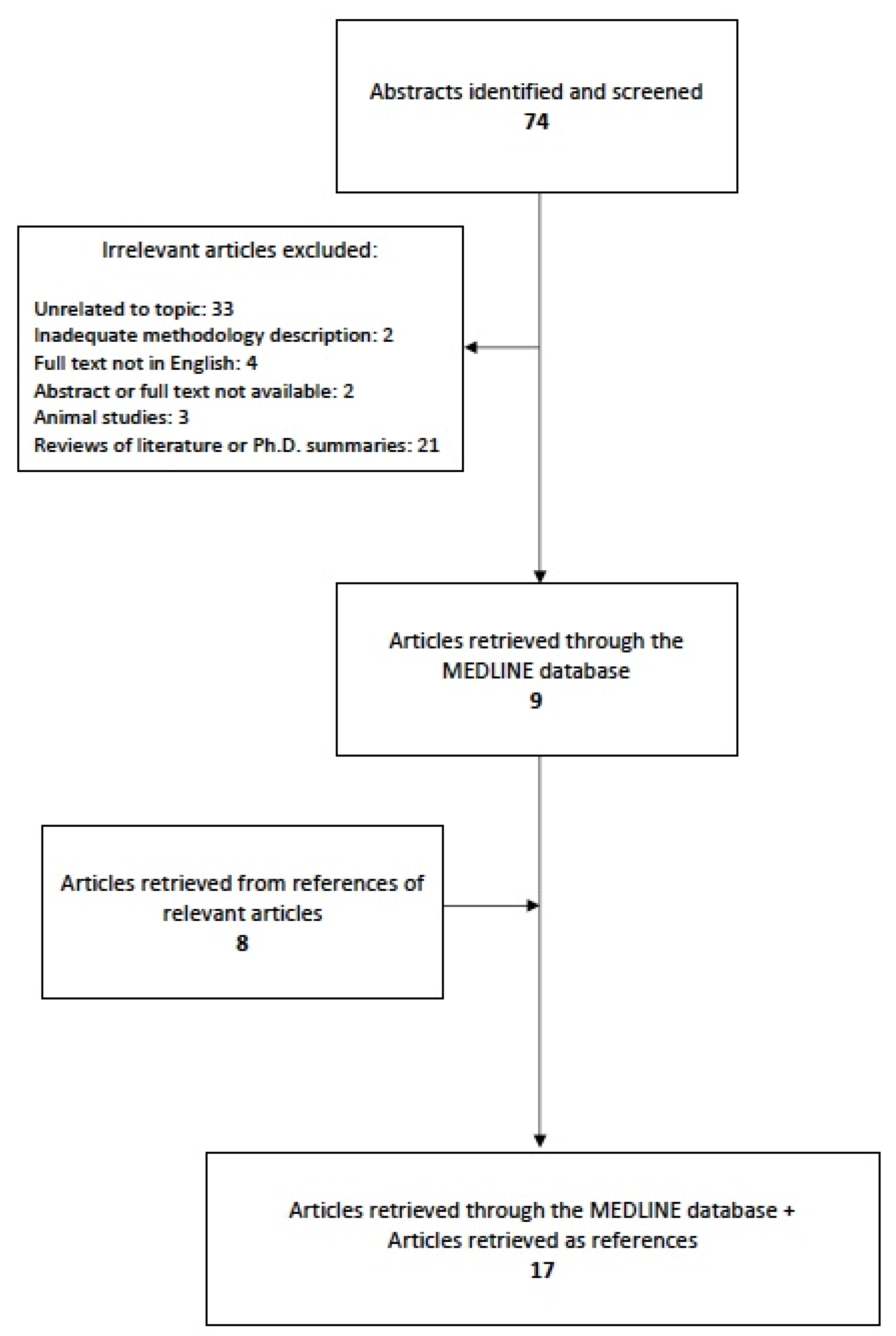
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Abbreviations
References
- De Haan, J.; Verheecke, M.; Van Calsteren, K.; Van Calster, B.; Shmakov, R.G.; Gziri, M.M.; Halaska, M.J.; Fruscio, R.; Lok, C.A.R.; A Boere, I.; et al. Oncological management and obstetric and neonatal outcomes for women diagnosed with cancer during pregnancy: A 20-year international cohort study of 1170 patients. Lancet Oncol. 2018, 19, 337–346. [Google Scholar] [CrossRef]
- Silverstein, J.S.; Post, A.L.; Chien, A.J.; Olin, R.; Tsai, K.K.; Ngo, Z.; Van Loon, K. Multidisciplinary management of cancer during pregnancy. JCO Oncol. Pract. 2020, 16, 545–557. [Google Scholar] [CrossRef] [PubMed]
- Korakiti, A.M.; Moutafi, M.; Zografos, E.; Dimopoulos, M.A.; Zagouri, F. The genomic profile of pregnancy-associated breast cancer: A systematic review. Front. Oncol. 2020, 10, 1773. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.E.; Mayer, E.L.; Partridge, A. Prognosis of pregnancy-associated breast cancer. Breast Cancer Res. Treat. 2017, 163, 417–421. [Google Scholar] [CrossRef]
- Korakiti, A.M.; Kalapanida, D.; Dimopoulos, M.A.; Zagouri, F. The prognostic role of protein expression in pregnancy-associated breast cancer: A literature review. J. Cancer Sci. Clin. Ther. 2020, 4, 189–194. [Google Scholar] [CrossRef]
- Amant, F.; Verheecke, M.; Wlodarska, I.; Dehaspe, L.; Brady, P.; Brison, N.; Bogaert, K.V.D.; Dierickx, D.; Vandecaveye, V.; Tousseyn, T.; et al. Presymptomatic identification of cancers in pregnant women during noninvasive prenatal testing. JAMA Oncol. 2015, 1, 814–819. [Google Scholar] [CrossRef] [Green Version]
- Lenaerts, L.; Jatsenko, T.; Amant, F.; Vermeesch, J.R. Noninvasive prenatal testing and detection of occult maternal malignancies. Clin. Chem. 2019, 65, 1484–1486. [Google Scholar] [CrossRef]
- Maggen, C.; Wolters, V.; Cardonick, E.; Fumagalli, M.; Halaska, M.J.; Lok, C.; De Haan, J.; Van Tornout, K.; Van Calsteren, K.; Amant, F. Pregnancy and Cancer: The INCIP Project. Curr. Oncol. Rep. 2020, 22, 17. [Google Scholar] [CrossRef] [Green Version]
- Zagouri, F.; Dimitrakakis, C.; Marinopoulos, S.; Tsigginou, A.; Dimopoulos, M.A. Cancer in pregnancy: Disentangling treatment modalities. ESMO Open 2016, 1, e000016. [Google Scholar] [CrossRef] [Green Version]
- Zagouri, F.; Psaltopoulou, T.; Dimitrakakis, C.; Bartsch, R.; Dimopoulos, M.A. Challenges in managing breast cancer during pregnancy. J. Thorac. Dis. 2013, 5, S62–S67. [Google Scholar] [CrossRef]
- Loibl, S.; Han, S.N.; Von Minckwitz, G.; Bontenbal, M.; Ring, A.; Giermek, J.; Fehm, T.; Van Calsteren, K.; Linn, S.C.; Schlehe, B.; et al. Treatment of breast cancer during pregnancy: An observational study. Lancet Oncol. 2012, 13, 887–896. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amant, F.; Van Calsteren, K.; Halaska, M.J.; Gziri, M.M.; Hui, W.; Lagae, L.; A Willemsen, M.; Kapusta, L.; Van Calster, B.; Wouters, H.; et al. Long-term cognitive and cardiac outcomes after prenatal exposure to chemotherapy in children aged 18 months or older: An observational study. Lancet Oncol. 2012, 13, 256–264. [Google Scholar] [CrossRef]
- Amant, F.; Vandenbroucke, T.; Verheecke, M.; Fumagalli, M.; Halaska, M.J.; Boere, I.; Han, S.; Gziri, M.M.; Peccatori, F.; Rob, L.; et al. Pediatric outcome after maternal cancer diagnosed during pregnancy. N. Engl. J. Med. 2015, 373, 1824–1834. [Google Scholar] [CrossRef]
- Avilés, A.; Niz, J. Long-term follow-up of children born to mothers with acute leukemia during pregnancy. Med. Pediatr. Oncol. 1988, 16, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Avilés, A.; Díaz-Maqueo, J.C.; Talavera, A.; Guzmán, R.; García, E.L. Growth and development of children of mothers treated with chemotherapy during pregnancy: Current status of 43 children. Am. J. Hematol. 1991, 36, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Avilés, A.; Neri, N. Hematological malignancies and pregnancy: A final report of 84 children who received chemotherapy in-utero. Clin. Lymphoma. 2001, 2, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Avilés, A.; Neri, N.; Nambo, M.J. Hematological malignancies and pregnancy: Treat or no treat during the first trimester. Int. J. Cancer 2012, 131, 2678–2683. [Google Scholar] [CrossRef] [PubMed]
- Blatt, J.; Mulvihill, J.J.; Ziegler, J.L.; Young, R.C.; Poplack, D.G. Pregnancy outcome following cancer chemotherapy. Am. J. Med. 1980, 69, 828–832. [Google Scholar] [CrossRef]
- Blommaert, J.; Zink, R.; Deprez, S.; Myatchin, I.; Dupont, P.; Vandenbroucke, T.; Sleurs, C.; Van Calsteren, K.; Amant, F.; Lagae, L. Long-term impact of prenatal exposure to chemotherapy on executive functioning: An ERP study. Clin. Neurophysiol. 2019, 130, 1655–1664. [Google Scholar] [CrossRef]
- Blommaert, J.; Radwan, A.; Sleurs, C.; Maggen, C.; Van Gerwen, M.; Wolters, V.; Christiaens, D.; Peeters, R.; Dupont, P.; Sunaert, S.; et al. The impact of cancer and chemotherapy during pregnancy on child neurodevelopment: A multimodal neuroimaging analysis. EClinicalMedicine 2020, 17, 16. [Google Scholar] [CrossRef]
- Cardonick, E.H.; Gringlas, M.B.; Hunter, K.; Greenspan, J. Development of children born to mothers with cancer during pregnancy: Comparing in utero chemotherapy-exposed children with nonexposed controls. Am. J. Obstet. Gynecol. 2015, 212, 658.e1–658.e8. [Google Scholar] [CrossRef]
- Hahn, K.M.E.; Johnson, P.H.; Gordon, N.; Kuerer, H.; Middleton, L.; Ramirez, M.; Yang, W.; Perkins, G.; Hortobagyi, G.N.; Theriault, R.L. Treatment of pregnant breast cancer patients and outcomes of children exposed to chemotherapy in utero. Cancer 2006, 107, 1219–1226. [Google Scholar] [CrossRef] [PubMed]
- Maggen, C.; Lok, C.A.; Cardonick, E.; Van Gerwen, M.; Ottevanger, P.B.; Boere, I.A.; Koskas, M.; Halaska, M.J.; Fruscio, R.; Gziri, M.M.; et al. Gastric cancer during pregnancy: A report on 13 cases and review of the literature with focus on chemotherapy during pregnancy. Acta Obstet. Gynecol. Scand. 2020, 99, 79–88. [Google Scholar] [CrossRef]
- Murthy, R.K.; Theriault, R.L.; Barnett, C.M.; Hodge, S.; Ramirez, M.M.; Milbourne, A.; A Rimes, S.; Hortobagyi, G.N.; Valero, V.; Litton, J.K. Outcomes of children exposed in utero to chemotherapy for breast cancer. Breast Cancer Res. 2014, 16, 500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Passera, S.; Contarino, V.; Scarfone, G.; Scola, E.; Fontana, C.; Peccatori, F.; Cinnante, C.; Counsell, S.J.; Ossola, M.; Pisoni, S.; et al. Effects of in-utero exposure to chemotherapy on fetal brain growth. Int. J. Gynecol. Cancer 2019, 29, 1195–1202. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, T.; Verheecke, M.; Van Gerwen, M.; Van Calsteren, K.; Halaska, M.J.; Fumagalli, M.; Fruscio, R.; Gandhi, A.; Veening, M.; Lagae, L.; et al. Child development at 6 years after maternal cancer diagnosis and treatment during pregnancy. Eur. J. Cancer 2020, 138, 57–67. [Google Scholar] [CrossRef]
- Van Gerwen, M.; Vandenbroucke, T.; Verheecke, M.; Van Calsteren, K.; Halaska, M.J.; Fumagalli, M.; Fruscio, R.; Gandhi, A.; Veening, M.; Lagae, L.; et al. Data describing child development at 6 years after maternal cancer diagnosis and treatment during pregnancy. Data Brief. 2020, 32, 106209. [Google Scholar] [CrossRef]
- Van Gerwen, M.; Vandenbroucke, T.; Gorissen, A.-S.; Van Grotel, M.; Heuvel-Eibrink, M.V.D.; Verwaaijen, E.; Van Der Perk, M.; Van Calsteren, K.; Van Dijk-Lokkart, E.M.; Amant, F. Executive functioning in 6-year-old children exposed to chemotherapy in utero. Early Hum. Dev. 2020, 151, 105198. [Google Scholar] [CrossRef]
- Vandenbroucke, T.; Verheecke, M.; Fumagalli, M.; Lok, C.; Amant, F. Effects of cancer treatment during pregnancy on fetal and child development. Lancet Child Adolesc. Health 2017, 1, 302–310. [Google Scholar] [CrossRef]
- Peccatori, F.A.; Azim, H.A.; Orecchia, R.; Hoekstra, H.J.; Pavlidis, N.; Kesic, V.; Pentheroudakis, G. Cancer, pregnancy and fertility: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2013, 24 (Suppl. 6), vi160–vi170. [Google Scholar] [CrossRef] [PubMed]
- Syme, M.R.; Paxton, J.W.; Keelan, J.A. Drug transfer and metabolism by the human placenta. Clin. Pharmacokinet. 2004, 43, 487–514. [Google Scholar] [CrossRef] [PubMed]
- Virgintino, D.; Errede, M.; Girolamo, F.; Capobianco, C.; Robertson, D.; Vimercati, A.; Serio, G.; Di Benedetto, A.; Yonekawa, Y.; Frei, K.; et al. Fetal blood-brain barrier P-glycoprotein contributes to brain protection during human development. J. Neuropathol. Exp. Neurol. 2008, 67, 50–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vercruysse, D.; Deprez, S.; Sunaert, S.; Van Calsteren, K.; Amant, F. Effects of prenatal exposure to cancer treatment on neurocognitive development, a review. Neurotoxicology 2016, 54, 11–12. [Google Scholar] [CrossRef]
- Dekrem, J.; Van Calsteren, K.; Amant, F. Effects of prenatal exposure to maternal chemotherapy. Pediatr. Drugs 2013, 15, 329–334. [Google Scholar] [CrossRef]
- Mennes, M.; Stiers, P.; Vandenbussche, E.; Vercruysse, G.; Uyttebroeck, A.; De Meyer, G.; Van Gool, S.W. Attention and information processing in survivors of childhood acute lymphoblastic leukemia treated with chemotherapy only. Paediatr. Blood Cancer 2005, 44, 478–486. [Google Scholar] [CrossRef]
- Betchen, M.; Grunberg, V.A.; Gringlas, M.; Cardonick, E. Being a mother after cancer diagnosis during pregnancy: Maternal psychosocial functioning and child cognitive development and behavior. Psychooncology 2020, 29, 1148–1155. [Google Scholar] [CrossRef]
- Loomans, E.M.; Van der Stelt, O.; Van Eijsden, M.; Gemke, R.J.; Vrijkotte, T.; Van den Bergh, B.R. Antenatal maternal anxiety is associated with problem behaviour at age five. Early Hum. Dev. 2011, 87, 565–570. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, F.; Faccio, F.; Peccatori, F.; Pravetonni, G. Psychological issues and construction of the mother-child relationship in women with cancer during pregnancy: A perspective on current and future directions. BMC Psychol. 2018, 6, 10. [Google Scholar] [CrossRef]
- Lohaugen, G.C.; Gramstad, A.; Evensen, K.A.; Martinussen, M.; Lindqvist, S.; Idredavik, M.; Vik, T.; Brubakk, A.-M.; Skranes, J. Cognitive profile in young adults born preterm at very low birthweight. Dev. Med. Child Neurol. 2010, 52, 1133–1138. [Google Scholar] [CrossRef]
- Van Bar, A.L.; Vermaas, J.; Knots, E.; De Kleine, M.J.; Soons, P. Functioning at school age of moderately preterm children born at 32 to 36 weeks’ gestational age. Pediatrics 2009, 124, 251–257. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Type of Maternal Cancer Diagnosed during Pregnancy | Chemotherapy Scheme(s) Administered during Pregnancy | Median Maternal Age (y) at Diagnosis | Trimester of Prenatal Exposure to Chemotherapy |
|---|---|---|---|---|
| Amant et al., 2012 [13] | Breast cancer (35) Hematological malignancy (18) Ovarian cancer (6) Cervical cancer (4) Basal cell cancer (1) Brain tumor (1) Ewing sarcoma (1) Colorectal cancer (1)Nasopharyngeal cancer (1) | (F)AC or (F)E(C) (34/68), MOPP or ABV (2/68), ABVD (5/68), CHOP-Rituximab (4/68), Cisplatin +/− [5-FU or Cyclophosphamide] (8/68), Paclitaxel + Cis/Carboplatin (3/68), Paclitaxel or Docetaxel (2/68), CMF (2/68), ALL Hovon scheme (5/68), Idarubicin + Ara C (2/68), Daunorubicin + Ara C (1/68), Temozolomide (1/68), 5-FU (1/68), Vincristine + Doxorubicin + Methotrexate (1/68), Amsacrine + Tenoposide (1/68), VIM (without methotrexate) (1/68) | 32.9 | 2nd and 3rd trimester |
| Amant et al., 2015 [14] | Breast cancer (69)Hematological malignancy (20) Cervical cancer (10) Ovarian cancer (9) Brain cancer (3) Colon cancer (3) Gastric cancer (2) Renal cancer (1) Tongue cancer (2) Lung cancer (1) Thyroid cancer (2) Melanoma (1) Ewing sarcoma (1) Soft tissue sarcoma (1) | (F)AC or (F)E(C) (58/93), ABVD (7/93), CHOP-Rituximab (7/93), Cisplatin +/− Epirubicin (6/93), Carboplatin +/− 5-FU (1/93), Paclitaxel + Cis/Carboplatin (9/93), Paclitaxel or Docetaxel (14/93), Hovon 37 (1/93), Temozolomide (1/93), Idarubicin + Ara C (1/93), Daunorubicin + Ara C (1/93), 5-FU (1/93), VIM (without methotrexate) (1/93) | 33.4 | 2nd and 3rd trimester |
| Avilés et al., 1988 [15] | Acute leukemia (23) | Combination of: Triamcinolone, 6-Mercaptopurine, Cyclophosphamide, Methotrexate, Vincristine, Prednisone, Ara C, Etoposide, Doxorubicin | N/A | 1st, 2nd and 3rd trimester |
| Avilés et al., 1991 [16] | Acute leukemia (7) Non-Hodgkin’s lymphoma (18) Hodgkin’s lymphoma (14) Chronic granulocytic leukemia (4) | Combination of: Vincristine, Prednisone, Doxorubicin, 6-Mercaptopurine, Methotrexate, Cyclophosphamide, Ara C CHO-Bleomycin (2/18), CHOP +/− [Bleomycin +/− Ara C +/− Methotrexate] (12/18), CEOP-Bleomycin +/− [Ara C +/− Methotrexate] (4/18) MOPP (4/14), ABVD (5/14), ABVD + MOPP (3/14), ABVD + PDN (2/14) Combination of: Busulfan, Prednisone, 6-Mercaptopurine | 24.0 29.0 28.0 30.0 | 1st, 2nd and 3rd trimester |
| Avilés et al., 2001 [17] | Acute leukemia (29) Malignant lymphoma (29) Hodgkin’s lymphoma (26) | COPA (10/29), Combination of: Ara C + [Daunorubicin (4/29) or Mitoxantrone (3/29) or Doxorubicin (8/29) or Idarubicin (4/29)] CHOP-Bleomycin (29/29) MOPP (10/26), ABVD (10/26), EBVD (4/26), MOPP + [ABVD or ABD] (2/26) | 29.6 N/A N/A | 1st, 2nd and 3rd trimester |
| Avilés et al., 2012 [18] | Acute leukemia (14) Non-Hodgkin’s lymphoma (25) Hodgkin’s lymphoma (19) | COPA (6/14), Ara C + Anthracycline (8/14) CHOP (17/25), CHOP-Rituximab (3/25), Intensive (5/25) ABVD (12/19), MOPP (5/19), MOPP + ABVD (2/19) | 26.8 29.3 22.0 | 1st trimester |
| Blatt et al., 1980 [19] | Acute leukemia (2) Hodgkin’s lymphoma (1) Undifferentiated sarcoma (1) | Ara C (1/2), Prednisone + Vincristine + Methotrexate + 6-Mercaptopurine (1/2) MOPP (1/1) Cyclophosphamide + Adriamycin + Vincristine + AMSA (1/1) | N/A | 1st, 2nd and 3rd trimester |
| Blommaert et al., 2019 [20] | Breast cancer (12) Cervical cancer (2) Hodgkin’s lymphoma (2) Non-Hodgkin’s lymphoma (1) Acute leukemia (2) Colon carcinoma (1) | FEC or FAC (7/20), Cyclophosphamide + Doxorubicin (3/20), ABVD (2/20), Platinum derivative (2/20), 5-FU (1/20), Ara C + Vincristine + Mitoxantrone (1/20), Cyclophosphamide + Methotrexate (1/20), Daunorubicin + Ara C (1/20), CHOP-Rituximab (1/20), Trastuzumab (1/20) | 34.0 (at birth) | 2nd and 3rd trimester |
| Blommaert et al., 2020 [21] | Breast cancer (25) Cervical cancer (3) Ovarian cancer (1) Hodgkin’s lymphoma (3) Tongue cancer (3) Leukemia (2) Brain tumor (2) Melanoma (1) Kidney carcinoma (1) Colon cancer (1) | FEC or FAC (11/30), Cyclophosphamide + [Doxorubicin or Epirubicin] (7/30), ABVD (3/30), Cisplatin (3/30), Carboplatin + 5-FU (2/30), 5-FU (1/30), Daunorubicin + Ara C (1/30), Epirubicin (1/30), Temozolomide (1/30) | 32.0 (at birth) | 2nd and 3rd trimester |
| Cardonick et al., 2015 [22] | Breast cancer (26) Ovarian cancer (4) Hodgkin’s lymphoma (4) Acute leukemia (1) | Doxorubicin + Cyclophosphamide (22/26) +/− [5-FU (3/26) or Paclitaxel (1/26)] Cisplatin + Paclitaxel (2/4), Etoposide + Cisplatin + Bleomycin (1/4), Carboplatin + Paclitaxel (1/4) Doxorubicin + Bleomycin + Vinblastine + Dacarbazine (4/4) Cyclophosphamide + Daunorubicin + Vincristine + L-asparaginase + Cytarabine + 6-Mercaptopurine + Intrathecal Methotrexate (1/1) | N/A | 2nd and 3rd trimester |
| Hahn et al., 2006 [23] | Breast cancer (57) | Combination of: Cyclophosphamide (36/57), Doxorubicin (36/57), 5-FU (35/57) | 33.5 (mean) | 2nd and 3rd trimester |
| Maggen et al., 2020 [24] | Gastric cancer (13) | 5-FU or FOLFOX or [Carboplatin + Paclitaxel] (13/13) | 31.7 | 2nd and 3rd trimester |
| Murthy et al., 2014 [25] | Breast cancer (81) | FAC (81/81) | N/A | 2nd and 3rd trimester |
| Passera et al., 2019 [26] | Breast cancer (24) Ovarian cancer (1) Cervical cancer (1) Lung cancer (1) Nasopharyngeal cancer (1) Hodgkin’s lymphoma (2) Non-Hodgkin’s lymphoma (1) | [Anthracyclines (Epirubicin 26/31) + Cyclophosphamide] (31/31) | 35.0 (mean) | 2nd and 3rd trimester |
| Vandenbroucke et al., 2020 [27] and Van Gerwen et al., 2020 [28] | Breast cancer (69) Hematological malignancy (20) Cervical cancer (10) Ovarian cancer (10) Brain cancer (4) Oral cavity and oropharyngeal cavity cancer (4) Nasopharyngeal cancer (1) Gastric cancer (2) Colon cancer (1) Melanoma (2) Thyroid cancer (1) Soft tissue sarcoma (1) Kidney carcinoma (1) Lung cancer (1) | (F)AC or (F)E(C) (58/93), ABVD (5/93), CHOP-Rituximab (5/93), Cisplatin +/− Epirubicin (9/93), Carboplatin +/− 5-FU or Cisplatin +/− 5-FU (3/93), Paclitaxel + Cis/Carboplatin (7/93), Paclitaxel or Docetaxel (12/93), Hovon 30 or 70 or 42A (2/93), Temozolomide (1/93), Idarubicin + Ara C (2/93), 5-FU (1/93), CMF (1/93) | N/A | 2nd and 3rd trimester |
| Van Gerwen et al., 2020 [29] | Breast cancer (26) Cervical cancer (3) Tongue cancer (2) Gastric cancer (1) Hodgkin’s lymphoma (1) Non-Hodgkin’s lymphoma (1) | N/A | N/A | 2nd and 3rd trimester |
| Author | Children Evaluated | Perinatal Outcome | Median f/u | Testing Age | Neurodevelopmental Testing Method | Neurodevelopmental Outcome |
|---|---|---|---|---|---|---|
| Amant et al., 2012 [13] | 70 | Median GA (w): 35.7 Preterm: 47/70 SGA: 14/70 | 22.3 months | Birth 18 months 5–6, 8–9, 11–12, 14–15, or 18 years | Clinical neurological examination General health and education questionnaire Bayley Scales of Infant Development Wechsler Preschool and Primary Scale of Intelligence Snijders–Oomen Nonverbal Intelligence Test Children’s Memory Scale Child Behavior Checklist Wechsler Intelligence Scale for Children Test of Everyday Attention for Children Auditory Verbal Learning Test Wechsler Adult Intelligence Scale | Neurocognitive outcome within normal range. Negative prognostic effect of prematurity on cognitive development (Bayley or IQ score). Severe neurodevelopmental delay in two children, both members of a twin pregnancy. Although a clinical picture suggested a syndromal entity, an effect of chemotherapy cannot be excluded. Significant difference between verbal and performance IQ score in children older than 6 years of age (Wechsler Intelligence Test). Internalizing, externalizing, and total behavior problems reported in 6/21 children (CBCL). No significant correlation with prematurity. |
| Amant et al., 2015 [14] | 129 (31 of whom included in previously published results [13]) 96 of whom in utero exposed to chemotherapy | Median GA (w): 36 Preterm: 79/129 ** SGA: 28/127 ** SGA: 24/95 | 21 months | 18 months and/or 36 months | Clinical neurological examination General health and education questionnaire Bayley Scales of Infant Development | Negative prognostic effect of prematurity on cognitive development. Cognitive outcomes not significantly different among the prenatal-exposure group and the control group. No differences according to the type of chemotherapy or the number of chemotherapy cycles administered. |
| Avilés et al., 1988 [15] | 17 | Median GA (w): N/A Preterm: N/A SGA: N/A | 6 years | 4–22 years | Clinical neurological examination School performance questionnaire filled by teachers Wechsler Intelligence Scale for Children Bender–Gestalt Test for Young Children | No abnormalities in conduct or school performance. No differences in cognitive testing. |
| Avilés et al., 1991 [16] | 43 | Median GA (w): 38 Preterm: 8/43 SGA: N/A | N/A | 3–19 years | Clinical neurological examination School performance questionnaire filled by teachers Wechsler Intelligence Scale for Children Bender–Gestalt Test for Young Children | No abnormalities in conduct or school performance. Weschler Intelligence Test results within normal ranges. Development showed no difference in children of the same social and economic background. |
| Avilés et al., 2001 [17] | 84 | Median GA (w): N/A Preterm: N/A SGA: 0/84 | 18.7 years | 6–29 years | Clinical neurological examination School performance questionnaire filled by teachers | Neurological examination, psychological evaluation, educational performance and behavior of children exposed to maternal chemotherapy considered normal. |
| Avilés et al., 2012 [18] | 54 | Median GA (w): N/A Early preterm: 4/54 SGA: 10/54 | 22.4 years | Birth 3, 6, 12, 18, 24 months 3, 5, 7, 10, 15, 20 years | Clinical neurological examination School performance questionnaire filled by teachers | Intelligence test, including verbal and performance IQ score, within normal ranges. Academic development according to age, economic and social status. |
| Blatt et al., 1980 [19] | 3 | Median GA (w): N/A Preterm: 0/3 SGA: 0/3 | 7 years | 2.5–8 years | Clinical neurological examination Denver Developmental Screening Test School performance questionnaire filled by teachers | Growth, development, and school performance were normal. No major abnormalities. |
| Blommaert et al., 2019 [20] | 20 | Median GA (w): 35.6 Preterm: N/A SGA: N/A | 9.18 years | 9 years | Wechsler Intelligence Scale for Children Event-related potentials (ERP) Electroencephalography (EEG) | Prenatal exposure to chemotherapy had a negative impact on response inhibition and spatial attention. Prenatal exposure to chemotherapy and prematurity might both alter the development of conflict monitoring. |
| Blommaert et al., 2020 [21] | 42 30 of whom in utero exposed to chemotherapy | Median GA (w): 36.3 ** Preterm: 26/42 ** SGA: 7/42 ** | 9.19 years ** | 9 years | Wechsler Intelligence Scale for Children Child Behavior Checklist Behavior Rating Inventory of Executive Function Brain MRI | All psycho-behavioral measures within normal ranges, though children born after cancer-complicated pregnancies showed a slightly lower total IQ score. Psycho-behavioral parameters not significantly related to any of the brain differences in MRI neuroimaging. Differences in brain MRI neuroimaging observed within chemotherapy subgroup when exposed to platinum derivatives or anthracyclines. No significant correlation with neurocognitive outcome. |
| Cardonick et al., 2015 [22] | 35 | Mean GA (w): 36.7 Preterm: 51.4% SGA: 1/35 | Mean value: 4.5 years | 18 months-10.4 years | Bayley Scales of Infant Development Wechsler Preschool and Primary Scale of Intelligence Wechsler Intelligence Scale for Children Wechsler Individual Achievement Test Child Behavior Checklist | No significant differences in cognitive skills, academic achievement, or behavioral competence between the chemotherapy-exposed group and the unexposed children. Premature birth more prevalent in the chemotherapy-exposed group. No correlation with developmental outcome. Older children demonstrated significantly higher rates of internalizing behavior problems. |
| Hahn et al., 2006 [23] | 52 | Mean GA (w): 37 Preterm: N/A SGA: N/A | 38.5 months | 2-157 months | General health and education questionnaire | Of the school-age children (n = 18), only two required special attention in school: one child had attention deficit disorder, whereas the other had Down-syndrome. |
| Maggen et al., 2020 [24] | 10 6 of whom in utero exposed to chemotherapy | Median GA (w): 32 ** Preterm: 4/6 SGA: 2/6 | N/A | 4, 6, 15, 18 months, 3, 6 years | Clinical neurological examination Bayley Scales of Infant and Toddler Development Child Behavior Checklist Behavior Rating Inventory of Executive Function Wechsler Preschool and Primary Scale of Intelligence Children’s Memory Scale Amsterdam Neuropsychological Tasks | No neurocognitive abnormalities. |
| Murthy et al., 2014 [25] | 81 (Update on previously published initial report in 2006 [23]) | Mean GA (w): 37 Preterm: 28/81 SGA: N/A | 7 years | <1–22 years | General health and education questionnaire | 6/50 survey responders: children with developmental milestone delays (3/50 childhood language delays). No significant cognitive abnormalities. 37 children enrolled in pre-school through college: 3/37 reading delays, 4/37 difficulties in school, 1/37 difficulty with attention span. |
| Passera et al., 2019 [26] | 31 (10 of whom included in previously published results [14]) | Mean GA (w): 36.3 Preterm: 15/31 SGA: 5/31 | Mean value: 41.1 weeks (at brain MRI) Mean value: 19.8 months (at Bayley Scales) | Mean post-menstrual age: 41.1 weeks 18 months | Clinical neurological examination Brain MRI Bayley Scales of Infant Development | No statistically significant differences between children exposed to chemotherapy and controls in both the total and the regional brain volumes (brain MRI). Exposed children with normal Bayley scores. No significant correlation between the brain volumes and the neurodevelopmental outcome. No correlation between the neurodevelopmental outcome and the cumulative dosage of epirubicin administered. |
| Vandenbroucke et al., 2020 [27] and Van Gerwen et al., 2020 [28] | 132 (12 of whom included in previously published results [13]) 97 of whom in utero exposed to chemotherapy | Median GA (w): 36.1 ** Preterm: 80/132 ** SGA: 14/97 | 6.1 years | 6 years | Clinical neurological examination General health and education questionnaire Wechsler Preschool and Primary Scale of Intelligence Wechsler Intelligence Scale for Children Snijders–Oomen Nonverbal Intelligence Test Children’s Memory Scale Amsterdam Neuropsychological Tasks Child Behavior Checklist | Although within normal range, statistically significant differences in mean verbal IQ and visuospatial long-term memory; lower scores in children prenatally exposed to maternal chemotherapy. Verbal IQ more affected in children whose mothers died than in children with surviving mothers. No correlation of prematurity with cognitive outcome. Full scale IQ not related to GA in the chemotherapy-exposed group or to the number of chemotherapy cycles administered during pregnancy. |
| Van Gerwen et al., 2020 [29] | 37 | Median GA (w): 35.6 Preterm: N/A SGA: N/A | 6.1 years | 6 years | Behavior Rating Inventory of Executive Function General health and education questionnaire Wechsler Preschool and Primary Scale of Intelligence | All outcome scales within normal ranges (BRIEF). Significant between-group difference in emotional control; weaker emotion regulation skills in children prenatally exposed to chemotherapy. Significantly lower verbal IQ score in children prenatally exposed to chemotherapy. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Korakiti, A.-M.; Zografos, E.; van Gerwen, M.; Amant, F.; Dimopoulos, M.-A.; Zagouri, F. Long-Term Neurodevelopmental Outcome of Children after in Utero Exposure to Chemotherapy. Cancers 2020, 12, 3623. https://doi.org/10.3390/cancers12123623
Korakiti A-M, Zografos E, van Gerwen M, Amant F, Dimopoulos M-A, Zagouri F. Long-Term Neurodevelopmental Outcome of Children after in Utero Exposure to Chemotherapy. Cancers. 2020; 12(12):3623. https://doi.org/10.3390/cancers12123623
Chicago/Turabian StyleKorakiti, Anna-Maria, Eleni Zografos, Mathilde van Gerwen, Frédéric Amant, Meletios-Athanasios Dimopoulos, and Flora Zagouri. 2020. "Long-Term Neurodevelopmental Outcome of Children after in Utero Exposure to Chemotherapy" Cancers 12, no. 12: 3623. https://doi.org/10.3390/cancers12123623