Outcome After 68Ga-PSMA-11 versus Choline PET-Based Salvage Radiotherapy in Patients with Biochemical Recurrence of Prostate Cancer: A Matched-Pair Analysis

 , , , , , ,
, , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Population
2.2. PET/CT Imaging
2.3. Treatment Application and Follow Up
2.4. Statistical Analysis
3. Results
3.1. Patient and Treatment Characteristics
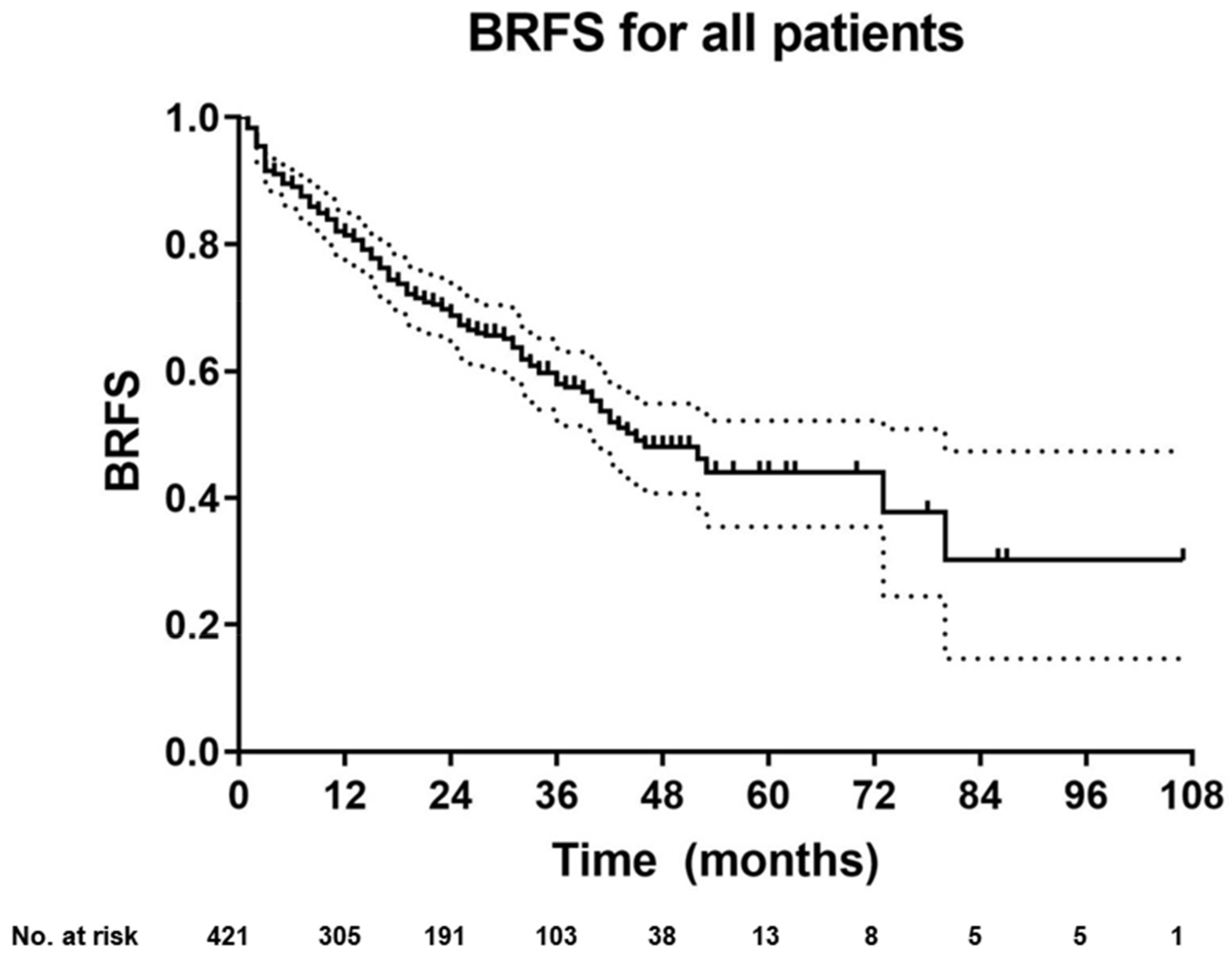
3.2. BRFS for the Entire Cohort
3.3. BRFS for Matched-Pair Analysis: Choline vs. PSMA PET-Based sRT
3.4. BRFS of Patients Without Ongoing ADT at Last Follow-Up
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Han, M.; Partin, A.W.; Zahurak, M.; Piantadosi, S.; Epstein, J.I.; Walsh, P.C. Biochemical (prostate specific antigen) recurrence probability following radical prostatectomy for clinically localized prostate cancer. J. Urol. 2003, 169, 517–523. [Google Scholar] [CrossRef]
- Shipley, W.U.; Seiferheld, W.; Lukka, H.R.; Major, P.P.; Heney, N.M.; Grignon, D.J.; Sartor, O.; Patel, M.P.; Bahary, J.P.; Zietman, A.L.; et al. Radiation with or without Antiandrogen Therapy in Recurrent Prostate Cancer. N. Engl. J. Med. 2017, 376, 417–428. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Picchio, M.; Briganti, A.; Fanti, S.; Heidenreich, A.; Krause, B.J.; Messa, C.; Montorsi, F.; Reske, S.N.; Thalmann, G.N. The role of choline positron emission tomography/computed tomography in the management of patients with prostate-specific antigen progression after radical treatment of prostate cancer. Eur. Urol. 2011, 59, 51–60. [Google Scholar] [CrossRef] [PubMed]
- Casamassima, F.; Masi, L.; Menichelli, C.; Bonucci, I.; Casamassima, E.; Lazzeri, M.; Gulisano, M.; Aterini, S. Efficacy of eradicative radiotherapy for limited nodal metastases detected with choline PET scan in prostate cancer patients. Tumori 2011, 97, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Stefan, A.K.; Katharina, S.; Clemens, K.; Erik, W.; Matthias, F.H.; Sonja, K.; Ingmar, S.; Klaus, H.; Klaus, K.; Ali, A.-O.; et al. Clinical outcome of PSMA-guided radiotherapy for patients with oligorecurrent prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2020. [Google Scholar] [CrossRef] [PubMed]
- Kroeze, S.G.C.; Henkenberens, C.; Schmidt-Hegemann, N.S.; Vogel, M.M.E.; Kirste, S.; Becker, J.; Burger, I.A.; Derlin, T.; Bartenstein, P.; Eiber, M.; et al. Prostate-specific Membrane Antigen Positron Emission Tomography–detected Oligorecurrent Prostate Cancer Treated with Metastases-directed Radiotherapy: Role of Addition and Duration of Androgen Deprivation. Eur. Urol. Focus 2019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, J.; Ferraro, D.A.; Muehlematter, U.J.; Garcia Schüler, H.I.; Kedzia, S.; Eberli, D.; Guckenberger, M.; Kroeze, S.G.C.; Sulser, T.; Schmid, D.M.; et al. Clinical impact of 68Ga-PSMA-11 PET on patient management and outcome, including all patients referred for an increase in PSA level during the first year after its clinical introduction. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 889–900. [Google Scholar] [CrossRef]
- Farolfi, A.; Gafita, A.; Calais, J.; Eiber, M.; Afshar-Oromieh, A.; Spohn, F.; Barbato, F.; Weber, M.; Ilhan, H.; Cervati, V.; et al. 68Ga-PSMA-11 Positron Emission Tomography Detects Residual Prostate Cancer after Prostatectomy in a Multicenter Retrospective Study. J. Urol. 2019, 202, 1174–1181. [Google Scholar] [CrossRef]
- Michaud, L.; Touijer, K.A.; Mauguen, A.; Zelefsky, M.J.; Morris, M.J.; Lyashschenko, S.K.; Durack, J.C.; Humm, J.L.; Weber, W.A.; Schöder, H. 11C-Choline PET/CT in Recurrent Prostate Cancer: Retrospective Analysis in a Large U.S. Patient Series. J. Nucl. Med. 2020, 61, 827–833. [Google Scholar] [CrossRef]
- McCarthy, M.; Francis, R.; Tang, C.; Watts, J.; Campbell, A. A Multicenter Prospective Clinical Trial of (68)Gallium PSMA HBED-CC PET-CT Restaging in Biochemically Relapsed Prostate Carcinoma: Oligometastatic Rate and Distribution Compared With Standard Imaging. Int J. Radiat. Oncol. Biol. Phys. 2019, 104, 801–808. [Google Scholar] [CrossRef]
- D’Angelillo, R.M.; Sciuto, R.; Ramella, S.; Papalia, R.; Jereczek-Fossa, B.A.; Trodella, L.E.; Fiore, M.; Gallucci, M.; Maini, C.L.; Trodella, L. 18F-Choline Positron Emission Tomography/Computed Tomography–Driven High-Dose Salvage Radiation Therapy in Patients With Biochemical Progression After Radical Prostatectomy: Feasibility Study in 60 Patients. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Hegemann, N.S.; Eze, C.; Li, M.L.; Rogowski, P.; Schaefer, C.; Stief, C.; Buchner, A.; Zamboglou, C.; Fendler, W.P.; Ganswindt, U.; et al. Impact of Ga-68-PSMAPET/CT on the Radiotherapeutic Approach to Prostate Cancer in Comparison to CT: A Retrospective Analysis. J. Nucl. Med. 2019, 60, 963–970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kasivisvanathan, V.; Rannikko, A.S.; Borghi, M.; Panebianco, V.; Mynderse, L.A.; Vaarala, M.H.; Briganti, A.; Budaus, L.; Hellawell, G.; Hindley, R.G.; et al. MRI-Targeted or Standard Biopsy for Prostate-Cancer Diagnosis. N. Engl. J. Med. 2018, 378, 1767–1777. [Google Scholar] [CrossRef]
- Rousseau, E.; Wilson, D.; Lacroix-Poisson, F.; Krauze, A.; Chi, K.; Gleave, M.; McKenzie, M.; Tyldesley, S.; Goldenberg, S.L.; Bénard, F. A Prospective Study on 18F-DCFPyL PSMA PET/CT Imaging in Biochemical Recurrence of Prostate Cancer. J. Nucl. Med. 2019, 60, 1587–1593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fendler, W.P.; Calais, J.; Eiber, M.; Flavell, R.R.; Mishoe, A.; Feng, F.Y.; Nguyen, H.G.; Reiter, R.E.; Rettig, M.B.; Okamoto, S.; et al. Assessment of 68Ga-PSMA-11 PET Accuracy in Localizing Recurrent Prostate Cancer: A Prospective Single-Arm Clinical Trial. JAMA Oncol. 2019, 5, 856–863. [Google Scholar] [CrossRef] [Green Version]
- Afshar-Oromieh, A.; Zechmann, C.M.; Malcher, A. Comparison of PET imaging with a (68)Ga-labelled PSMA ligand and (18)F-choline-based PET/CT for the diagnosis of recurrent prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2014, 41. [Google Scholar] [CrossRef] [Green Version]
- Schwenck, J.; Rempp, H.; Reischl, G.; Kruck, S.; Stenzl, A.; Nikolaou, K.; Pfannenberg, C.; la Fougere, C. Comparison of (68)Ga-labelled PSMA-11 and (11)C-choline in the detection of prostate cancer metastases by PET/CT. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 92–101. [Google Scholar] [CrossRef]
- Morigi, J.J.; Stricker, P.D.; Leeuwen, P.J. Prospective comparison of 18F-fluoromethylcholine versus 68Ga-PSMA PET/CT in prostate cancer patients who have rising PSA after curative treatment and are being considered for targeted therapy. J. Nucl. Med. 2015, 56. [Google Scholar] [CrossRef] [Green Version]
- Schmidt-Hegemann, N.-S.; Chukwuka, E.; Minglun, L.; Rogowski, P.; Schaefer, C.; Stief, C.; Buchner, A.; Zamboglou, C.; Fendler, W.P.; Ganswindt, U.; et al. Impact of 68Ga-PSMA-PET/CT on the radiotherapeutic approach for prostate cancer in comparison to CT—A retrospective analysis. J. Nucl. Med. 2018. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.K.; Watson, T.; Denham, J.; Shakespeare, T.P.; Rutherford, N.; McLeod, N.; Picton, K.; Ainsworth, P.; Bonaventura, T.; Martin, J.M. Prostate-Specific Membrane Antigen Positron Emission Tomography-Computed Tomography for Prostate Cancer: Distribution of Disease and Implications for Radiation Therapy Planning. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, 701–709. [Google Scholar] [CrossRef]
- Fendler, W.; Ferdinandus, J.; Calais, J.; Eiber, M.; Flavell, R.R.; Mishoe, A.; Feng, F.Y.; Nguyen, H.G.; Reiter, R.E.; Rettig, M.; et al. Impact of 68Ga-PSMA-11 PET on the management of biochemically recurrent prostate cancer in a prospective single-arm clinical trial. J. Clin. Oncol. 2020, 38. [Google Scholar] [CrossRef]
- US Food and Drug Administration. FDA Approves 11C-Choline for PET in Prostate Cancer. J. Nucl. Med. 2012, 53, 11N. [Google Scholar]
- The World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. J. Am. Coll. Dent. 2014, 81, 14–18. [Google Scholar]
- Schmidt-Hegemann, N.-S.; Stief, C.; Kim, T.-H.; Eze, C.; Kirste, S.; Strouthos, I.; Li, M.; Schultze-Seemann, W.; Ilhan, H.; Fendler, W.P.; et al. Outcome After PSMA PET/CT–Based Salvage Radiotherapy in Patients with Biochemical Recurrence After Radical Prostatectomy: A 2-Institution Retrospective Analysis. J. Nucl. Med. 2019, 60, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Jilg, C.A.; Schultze-Seemann, W.; Drendel, V.; Vach, W.; Wieser, G.; Krauss, T.; Jandausch, A.; Holz, S.; Henne, K.; Reske, S.N.; et al. Detection of Lymph Node Metastasis in Patients with Nodal Prostate Cancer Relapse Using F-18/C-11-Choline Positron Emission Tomography/Computerized Tomography. J. Urol. 2014, 192, 103–110. [Google Scholar] [CrossRef]
- Perera, M.; Krishnananthan, N.; Lindner, U.; Lawrentschuk, N. An update on focal therapy for prostate cancer. Nat. Rev. Urol. 2016, 13, 641–653. [Google Scholar] [CrossRef]
- Zschaeck, S.; Wust, P.; Beck, M.; Wlodarczyk, W.; Kaul, D.; Rogasch, J.; Budach, V.; Furth, C.; Ghadjar, P. Intermediate-term outcome after PSMA-PET guided high-dose radiotherapy of recurrent high-risk prostate cancer patients. Radiat. Oncol. 2017, 12, 140. [Google Scholar] [CrossRef] [Green Version]
- Stephenson, A.J.; Shariat, S.F.; Zelefsky, M.J.; Kattan, M.W.; Butler, E.B.; Teh, B.S.; Klein, E.A.; Kupelian, P.A.; Roehrborn, C.G.; Pistenmaa, D.A.; et al. Salvage radiotherapy for recurrent prostate cancer after radical prostatectomy. JAMA 2004, 291, 1325–1332. [Google Scholar] [CrossRef]
- Stish, B.J.; Pisansky, T.M.; Harmsen, W.S.; Davis, B.J.; Tzou, K.S.; Choo, R.; Buskirk, S.J. Improved Metastasis-Free and Survival Outcomes With Early Salvage Radiotherapy in Men With Detectable Prostate-Specific Antigen After Prostatectomy for Prostate Cancer. J. Clin. Oncol. 2016, 34, 3864–3871. [Google Scholar] [CrossRef]
- Abugharib, A.; Jackson, W.C.; Tumati, V.; Dess, R.T.; Lee, J.Y.; Zhao, S.G.; Soliman, M.; Zumsteg, Z.S.; Mehra, R.; Feng, F.Y.; et al. Very Early Salvage Radiotherapy Improves Distant Metastasis-Free Survival. J. Urol. 2017, 197, 662–668. [Google Scholar] [CrossRef]
- Tendulkar, R.D.; Agrawal, S.; Gao, T.; Efstathiou, J.A.; Pisansky, T.M.; Michalski, J.M.; Koontz, B.F.; Hamstra, D.A.; Feng, F.Y.; Liauw, S.L.; et al. Contemporary Update of a Multi-Institutional Predictive Nomogram for Salvage Radiotherapy After Radical Prostatectomy. J. Clin. Oncol. 2016, 34, 3648–3654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrie, C.; Magné, N.; Burban-Provost, P.; Sargos, P.; Latorzeff, I.; Lagrange, J.-L.; Supiot, S.; Belkacemi, Y.; Peiffert, D.; Allouache, N.; et al. Short-term androgen deprivation therapy combined with radiotherapy as salvage treatment after radical prostatectomy for prostate cancer (GETUG-AFU 16): A 112-month follow-up of a phase 3, randomised trial. Lancet Oncol. 2019. [Google Scholar] [CrossRef]
- Calais, J.; Czernin, J.; Fendler, W.P.; Elashoff, D.; Nickols, N.G. Randomized prospective phase III trial of (68)Ga-PSMA-11 PET/CT molecular imaging for prostate cancer salvage radiotherapy planning [PSMA-SRT]. BMC Cancer 2019, 19, 18. [Google Scholar] [CrossRef]
- Bartkowiak, D.; Siegmann, A.; Bohmer, D.; Budach, V.; Wiegel, T. The impact of prostate-specific antigen persistence after radical prostatectomy on the efficacy of salvage radiotherapy in patients with primary N0 prostate cancer. BJU Int. 2019, 124, 785–791. [Google Scholar] [CrossRef]
- Stephenson, A.J.; Scardino, P.T.; Kattan, M.W.; Pisansky, T.M.; Slawin, K.M.; Klein, E.A.; Anscher, M.S.; Michalski, J.M.; Sandler, H.M.; Lin, D.W.; et al. Predicting the outcome of salvage radiation therapy for recurrent prostate cancer after radical prostatectomy. J. Clin. Oncol. 2007, 25, 2035–2041. [Google Scholar] [CrossRef]
- Bettermann, A.S.; Zamboglou, C.; Kiefer, S.; Jilg, C.A.; Spohn, S.; Kranz-Rudolph, J.; Fassbender, T.F.; Bronsert, P.; Nicolay, N.H.; Gratzke, C.; et al. [Ga-68-]PSMA-11 PET/CT and multiparametric MRI for gross tumor volume delineation in a slice by slice analysis with whole mount histopathology as a reference standard—Implications for focal radiotherapy planning in primary prostate cancer. Radiother. Oncol. 2019, 141, 214–219. [Google Scholar] [CrossRef]
- Scheltema, M.J.; Chang, J.I.; Stricker, P.D.; van Leeuwen, P.J.; Nguyen, Q.A.; Ho, B.; Delprado, W.; Lee, J.; Thompson, J.E.; Cusick, T.; et al. Diagnostic accuracy of Ga-68-prostate-specific membrane antigen (PSMA) positron-emission tomography (PET) and multiparametric (mp)MRI to detect intermediate-grade intra-prostatic prostate cancer using whole-mount pathology: Impact of the addition of Ga-68-PSMA PET to mpMRI. BJU Int. 2019, 124, 42–49. [Google Scholar] [CrossRef] [Green Version]
- Giovacchini, G.; Guglielmo, P.; Mapelli, P.; Incerti, E.; Gajate, A.M.S.; Giovannini, E.; Riondato, M.; Briganti, A.; Gianolli, L.; Ciarmiello, A.; et al. 11C-choline PET/CT predicts survival in prostate cancer patients with PSA < 1 NG/ml. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 921–929. [Google Scholar] [CrossRef]
- Ingrosso, G.; Trippa, F.; Maranzano, E.; Carosi, A.; Ponti, E.; Arcidiacono, F.; Draghini, L.; Di Murro, L.; Lancia, A.; Santoni, R. Stereotactic body radiotherapy in oligometastatic prostate cancer patients with isolated lymph nodes involvement: A two-institution experience. World J. Urol. 2017, 35, 45–49. [Google Scholar] [CrossRef]
- De Bleser, E.; Jereczek-Fossa, B.A.; Pasquier, D.; Zilli, T.; Van As, N.; Siva, S.; Fodor, A.; Dirix, P.; Gomez-Iturriaga, A.; Trippa, F.; et al. Metastasis-directed Therapy in Treating Nodal Oligorecurrent Prostate Cancer: A Multi-institutional Analysis Comparing the Outcome and Toxicity of Stereotactic Body Radiotherapy and Elective Nodal Radiotherapy. Eur. Urol. 2019. [Google Scholar] [CrossRef]
- Jackson, W.C.; Feng, F.Y.; Daignault, S.; Hussain, M.; Smith, D.; Cooney, K.; Pienta, K.; Jolly, S.; Hollenbeck, B.; Olson, K.B.; et al. A phase 2 trial of salvage radiation and concurrent weekly docetaxel after a rising prostate-specific antigen level after radical prostatectomy. Adv. Radiat. Oncol. 2016, 1, 59–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Supiot, S.; Campion, L.; Pommier, P.; Dore, M.; Palpacuer, C.; Racadot, S.; Rio, E.; Milano, G.A.; Mahier-Ait Oukhatar, C.; Carrie, C. Combined abiraterone acetate plus prednisone, salvage prostate bed radiotherapy and LH-RH agonists (CARLHA-GEP12) in biochemically-relapsing prostate cancer patients following prostatectomy: A phase I study of the GETUG/GEP. Oncotarget 2018, 9, 22147–22157. [Google Scholar] [CrossRef] [PubMed]
- Dess, R.T.; Sun, Y.; Jackson, W.C.; Jairath, N.K.; Kishan, A.U.; Wallington, D.G.; Mahal, B.A.; Stish, B.J.; Zumsteg, Z.S.; Den, R.B.; et al. Association of Presalvage Radiotherapy PSA Levels After Prostatectomy With Outcomes of Long-term Antiandrogen Therapy in Men With Prostate Cancer. JAMA Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Zamboglou, C.; Carles, M.; Fechter, T.; Kiefer, S.; Reichel, K.; Fassbender, T.F.; Bronsert, P.; Koeber, G.; Schilling, O.; Ruf, J.; et al. Radiomic features from PSMA PET for non-invasive intraprostatic tumor discrimination and characterization in patients with intermediate- and high-risk prostate cancer - a comparison study with histology reference. Theranostics 2019, 9, 2595–2605. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Unadjusted | ||||
|---|---|---|---|---|
| Total Cohort | Choline Cohort | PSMA Cohort | p Value | |
| Number (%) | 421 (100) | 166 (39.4) | 255 (60.6) | |
| Age in years (median, range) | 69 (47–83) | 69 (49–82) | 71 (47–83) | n.s. |
| initial PSA in ng/mL (median, range) | 10.3 (1.1–368) | 9.6 (1.1–281) | 11.1 (2.3–368) | ** |
| pT stage (%) | **** | |||
| 2 | 155 (36.8) | 59 (35.4) | 96 (37.6) | |
| 3a | 107 (25.4) | 43 (25.9) | 64 (25.1) | |
| 3b | 117 (27.8) | 31 (18.7) | 86 (33.7) | |
| 4 | 14 (3.3) | 7 (4.2) | 7 (2.7) | |
| unknown | 28 (6.7) | 26 (15.7) | 2 (0.8) | |
| Gleason score (%) | **** | |||
| 6 | 27 (6.4) | 16 (9.6) | 11 (4.3) | |
| 7a | 107 (25.4) | 48 (28.9) | 59 (23.1) | |
| 7b | 117 (27.8) | 50 (30.1) | 67 (26.3) | |
| 8 | 67 (15.9) | 24 (14.5) | 43 (16.9) | |
| ≥9 | 87 (20.7) | 17 (10.2) | 70 (27.5) | |
| unknown | 16 (3.8) | 11 (6.6) | 5 (2) | |
| NCCN risk group (%) | **** | |||
| low risk | 14 (3.3) | 3 (1.8) | 11 (4.3) | |
| intermediate risk | 195 (46.3) | 88 (53.0) | 107 (42) | |
| high risk | 193 (45.8) | 59 (35.5) | 134 (52.5) | |
| unknown | 19 (4.5) | 16 (9.6) | 3 (1.2) | |
| R status (%) | **** | |||
| R0 | 214 (50.8) | 80 (48.2) | 134 (52.5) | |
| R1 or R2 | 161 (38.2) | 51 (30.7) | 110 (43.1) | |
| Rx | 46 (10.9) | 35 (21.1) | 11 (4.3) | |
| pN status (%) | *** | |||
| pN0 | 283 (67.2) | 127 (76.5) | 156 (61.2) | |
| pN1 | 99 (23.5) | 21 (12.7) | 78 (30.6) | |
| pNx | 34 (8.1) | 13 (7.8) | 21 (8.3) | |
| PSA persistence after surgery (%) | **** | |||
| yes | 171 (40.6) | 46 (27.7) | 125 (49) | |
| no | 250 (59.4) | 120 (72.3) | 130 (51) | |
| PSA before imaging in ng/mL (range, median) | 0.69 (0.07–40.1) | 0.69 (0.07–39.0) | 0.7 (0.13–40.1) | n.s. |
| PET findings (%) | **** | |||
| Positive PET findings | 257 (61) | 92 (55.4) | 165 (64.7) | |
| No PET findings | 164 (39) | 74 (44.6) | 90 (35.3) | |
| Locally recurrent disease | 162 (38.5) | 77 (46.3) | 85 (33.3) | |
| Pelvic lymph nodes | 133 (31.6) | 30 (18.1) | 103 (40.4) | |
| Metastatic disease | 44 (10.5) | 10 (6.0) | 34 (13.3) | |
| PSA before sRT in ng/mL (range, median) | 0.69 (0–40.1) | 0.7 (0–29.0) | 0.66 (0–40.1) | n.s. |
| Unadjusted | ||||
|---|---|---|---|---|
| Total Cohort | Choline Cohort | PSMA Cohort | p Value | |
| Number (%) | 421 (100) | 166 (39.4) | 255 (60.6) | |
| ADT | **** | |||
| yes | 158 (37.5) | 33 (19.9) | 125 (49) | |
| no | 263 (62.5) | 133 (80.1) | 130 (51) | |
| Duration ADT in months | **** | |||
| ≤6 months | 87 (20.7) | 26 (15.7) | 61 (23.9) | |
| >6 months | 54 (14.9) | 2 (1.2) | 52 (20.4) | |
| Unknown duration (n, %) | 17 (3.9) | 5 (3.0) | 12 (4.7) | |
| RT dose prostatic fossa in Gy (median, range) | 66.6 (54.5–75.6) | 70.2 (56–72) | 66.6 (54.5–75.6) | **** |
| RT to elective pelvic lymphatics | **** | |||
| yes | 160 (38) | 33 (19.9) | 127 (49.8) | |
| no | 261 (62) | 133 (80.1) | 128 (51.2) | |
| RT dose to elective pelvic lymphatics in Gy (median, range) | 50.4 (36–54) | 50.4 (36–54) | 50.4 (45–52.8) | n.s. |
| RT boost to pelvic lymph nodes | **** | |||
| yes | 120 (28.5) | 19 (11.4) | 101 (39.6) | |
| no | 301 (71.5) | 147 (88.6) | 154 (60.4) | |
| RT dose to pelvic lymph nodes in Gy (median, range) | 57.6 (45–70) | 56 (50.4–66) | 58.2 (45–70) | n.s. |
| RT to distant metastases | n.s. | |||
| yes | 31 (8.3) | 10 (6.0) | 21 (8.2) | |
| no | 390 (92.6) | 156 (94.0) | 234 (91.8) | |
| RT dose to distant metastases in Gy (median, range) | 42.5 (30–64.7) | 35 (30–56) | 45 (34–64.7) | n.s. |
| Follow-up time in months (median, range) | 30 (1–107) | 36 (1–108) | 27 (1–56) | **** |
| Biochemical recurrent disease | n.s. | |||
| yes | 154 (36.6) | 56 (33.7) | 98 (38.4) | |
| no | 267 (63.4) | 119 (66.3) | 157 (61.6) | |
| Univariate Cox Regression Analysis | ||||
|---|---|---|---|---|
| Cox ratio (95% CI) | p value | |||
| Indication RT (PSA persistence vs. salvage) | 1.7(1.2–2.3) | 0.001 | ||
| Risk group NCCN (low- vs. intermediate vs. high) | 1.4(1.1–1.9) | 0.019 | ||
| R status (R0 vs. R1) | 0.75 (0.5–1) | 0.092 | ||
| Gleason score (6 vs. 7 vs. 8) | 1.4(1–1.8) | 0.023 | ||
| pT (2 vs. 3 +4) | 1.6(1.2–2.3) | 0.006 | ||
| pN (0 vs. 1) | 1.6(1.2–2,1) | 0.002 | ||
| Time between surgery and PET imaging (days, continuous variable) | 1.0 (1.000-1.000) | 0.252 | ||
| Tracer (PSMA vs. cholin) | 1.5(1.1–2.1) | 0.014 | ||
| PSA before PET (</>0.5 ng/mL)) | 1.7(1.2–2.4) | 0.002 | ||
| PSA before PET (ng/mL, continuous variable) | 1.06(1.04–1.09) | <0.001 | ||
| PSA before sRT (</>0.5 ng/mL) | 1.7(1.2–2.4) | 0.002 | ||
| PSA before sRT (ng/mL, continuous variable) | 1.07(1.04–1.09) | <0.001 | ||
| Initial PSA (ng/mL, continuous variable) | 1.005(1.001–1.008) | 0.004 | ||
| PET-positive findings (yes vs. no) | 1.7(1.2–2.4) | 0.002 | ||
| Local recurrence in PET (yes vs. no) | 1.1 (0.8–1.5) | 0.661 | ||
| Pelvic lymph nodes in PET (yes vs. no) | 1.8(1.3–2.5) | <0.001 | ||
| Distant metastases in PET (yes vs. no) | 2.4(1.6–3.7) | <0.001 | ||
| RT dose prostatic fossa (</> 66 Gy) | 1.3 (0.7–2.2) | 0.365 | ||
| ADT (yes vs. no) | 1.08 (0.8–1.5) | 0.632 | ||
| Multivariate Cox regression analysis | ||||
| Cox ratio | 95% CI | p value | ||
| lower | upper | |||
| Indication RT (PSA persistence vs. salvage) | 1.154 | 0.774 | 1.719 | 0.482 |
| Risk group NCCN (LR vs. IR vs. HR) | 0.893 | 0.553 | 1.441 | 0.642 |
| Gleason score (6 vs. 7 vs. 8) | 1.072 | 0.686 | 1.676 | 0.760 |
| pT (2 vs. 3 +4) | 1.258 | 0.811 | 1.950 | 0.305 |
| pN (0 vs. 1) | 1.368 | 0.964 | 1.943 | 0.080 |
| Tracer (PSMA vs. cholin) | 1.019 | 0.685 | 1.517 | 0.926 |
| PSA before PET (ng/mL, continuous variable) | 1.036 | 1.005 | 1.069 | 0.024 |
| Initial PSA (ng/mL, continuous variable) | 1.001 | 0.997 | 1.005 | 0.734 |
| PET-positive findings (yes vs. no) | 1.225 | 0.769 | 1.952 | 0.394 |
| Pelvic lymph nodes in PET (yes vs. no) | 1.035 | 0.651 | 1.645 | 0.885 |
| Distant metastases in PET (yes vs. no) | 1.520 | 0.886 | 2.606 | 0.128 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schmidt Hegemann, N.-S.; Rogowski, P.; Eze, C.; Schäfer, C.; Stief, C.; Lang, S.; Spohn, S.; Steffens, R.; Li, M.; Gratzke, C.; et al. Outcome After 68Ga-PSMA-11 versus Choline PET-Based Salvage Radiotherapy in Patients with Biochemical Recurrence of Prostate Cancer: A Matched-Pair Analysis. Cancers 2020, 12, 3395. https://doi.org/10.3390/cancers12113395
Schmidt Hegemann N-S, Rogowski P, Eze C, Schäfer C, Stief C, Lang S, Spohn S, Steffens R, Li M, Gratzke C, et al. Outcome After 68Ga-PSMA-11 versus Choline PET-Based Salvage Radiotherapy in Patients with Biochemical Recurrence of Prostate Cancer: A Matched-Pair Analysis. Cancers. 2020; 12(11):3395. https://doi.org/10.3390/cancers12113395
Chicago/Turabian StyleSchmidt Hegemann, Nina-Sophie, Paul Rogowski, Chukwuka Eze, Christian Schäfer, Christian Stief, Sebastian Lang, Simon Spohn, Rieke Steffens, Minglun Li, Christian Gratzke, and et al. 2020. "Outcome After 68Ga-PSMA-11 versus Choline PET-Based Salvage Radiotherapy in Patients with Biochemical Recurrence of Prostate Cancer: A Matched-Pair Analysis" Cancers 12, no. 11: 3395. https://doi.org/10.3390/cancers12113395