Association of Planning Target Volume with Patient Outcome in Inoperable Stage III NSCLC Treated with Chemoradiotherapy: A Comprehensive Single-Center Analysis

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Patients and Methods
2.1. Patient Characterstics
2.2. Chemoradiotherapy
2.3. Patient Follow-Up
2.4. Statistical Analysis
3. Results
3.1. Patient and Tumor Characteristics
3.2. Univariate and Multivariate Analysis
3.3. PSM Analysis with Parameters Showing a Trend in Univariate Analysis
3.4. Additional PSM Analysis with Exact T- and N-Stage Matching
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Mathers, C.; Parkin, D.M.; Pineros, M.; Znaor, A.; Bray, F. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. Int. J. Cancer 2019, 144, 1941–1953. [Google Scholar] [CrossRef] [Green Version]
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina, J.R.; Yang, P.; Cassivi, S.D.; Schild, S.E.; Adjei, A.A. Non-small cell lung cancer: Epidemiology, risk factors, treatment, and survivorship. Mayo Clin. Proc. 2008, 83, 584–594. [Google Scholar] [CrossRef]
- Lemjabbar-Alaoui, H.; Hassan, O.U.; Yang, Y.W.; Buchanan, P. Lung cancer: Biology and treatment options. Biochim. Biophys. Acta 2015, 1856, 189–210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taugner, J.; Kasmann, L.; Eze, C.; Dantes, M.; Roengvoraphoj, O.; Gennen, K.; Karin, M.; Petruknov, O.; Tufman, A.; Belka, C.; et al. Survival score to characterize prognosis in inoperable stage III NSCLC after chemoradiotherapy. Transl. Lung Cancer Res. 2019, 8, 593–604. [Google Scholar] [CrossRef] [PubMed]
- Huber, R.M.; Theis, A. Multimodale therapie des lokal fortgeschrittenen NSCLC. Pneumologe 2005, 2, 254–259. [Google Scholar] [CrossRef]
- Walraven, I.; Damhuis, R.A.; Ten Berge, M.G.; Rosskamp, M.; van Eycken, L.; de Ruysscher, D.; Belderbos, J.S.A. Treatment variation of sequential versus concurrent chemoradiotherapy in stage III non-small cell lung cancer patients in The Netherlands and Belgium. Clin. Oncol. R Coll. Radiol. 2017, 29, e177–e185. [Google Scholar] [CrossRef] [PubMed]
- Du, L.; Waqar, S.N.; Morgensztern, D. Multimodality therapy for NSCLC. Cancer Treat. Res. 2016, 170, 151–163. [Google Scholar]
- Furuse, K.; Fukuoka, M.; Kawahara, M.; Nishikawa, H.; Takada, Y.; Kudoh, S.; Katagami, N.; Ariyoshi, Y. Phase III study of concurrent versus sequential thoracic radiotherapy in combination with mitomycin, vindesine, and cisplatin in unresectable stage III non-small-cell lung cancer. J. Clin. Oncol. 1999, 17, 2692–2699. [Google Scholar] [CrossRef]
- Postmus, P.E.; Kerr, K.M.; Oudkerk, M.; Senan, S.; Waller, D.A.; Vansteenkiste, J.; Escriu, C.; Peters, S.; Committee, E.G. Early and locally advanced non-small-cell lung cancer (NSCLC): ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28, iv1–iv21. [Google Scholar] [CrossRef]
- Brower, V. Adding radiotherapy to chemotherapy in advanced NSCLC. Lancet Oncol. 2017, 18, e645. [Google Scholar] [CrossRef]
- Salama, J.K.; Stinchcombe, T.E.; Gu, L.; Wang, X.; Morano, K.; Bogart, J.A.; Crawford, J.C.; Socinski, M.A.; Blackstock, A.W.; Vokes, E.E.; et al. Pulmonary toxicity in Stage III non-small cell lung cancer patients treated with high-dose (74 Gy) 3-dimensional conformal thoracic radiotherapy and concurrent chemotherapy following induction chemotherapy: A secondary analysis of Cancer and Leukemia Group B (CALGB) trial. Int. J. Radiat. Oncol. Biol. Phys. 2011, 81, e269–e274. [Google Scholar] [PubMed] [Green Version]
- Bradley, J.D.; Paulus, R.; Komaki, R.; Masters, G.; Blumenschein, G.; Schild, S.; Bogart, J.; Hu, C.; Forster, K.; Magliocco, A.; et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): A randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015, 16, 187–199. [Google Scholar] [PubMed] [Green Version]
- Bradley, J.D.; Hu, C.; Komaki, R.R.; Masters, G.A.; Blumenschein, G.R.; Schild, S.E.; Bogart, J.A.; Forster, K.M.; Magliocco, A.M.; Kavadi, V.S.; et al. Long-term results of NRG Oncology RTOG 0617: Standard-Versus high-dose chemoradiotherapy with or without cetuximab for unresectable stage III non-small-cell lung cancer. J. Clin. Oncol. 2020, 38, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Brade, A.M.; Wenz, F.; Koppe, F.; Lievens, Y.; San Antonio, B.; Iscoe, N.A.; Hossain, A.; Chouaki, N.; Senan, S. Radiation Therapy Quality Assurance (RTQA) of concurrent chemoradiation therapy for locally advanced non-small cell lung cancer in the PROCLAIM phase 3 trial. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 927–934. [Google Scholar] [CrossRef]
- Nestle, U.; De Ruysscher, D.; Ricardi, U.; Geets, X.; Belderbos, J.; Pottgen, C.; Dziadiuszko, R.; Peeters, S.; Lievens, Y.; Hurkmans, C.; et al. ESTRO ACROP guidelines for target volume definition in the treatment of locally advanced non-small cell lung cancer. Radiother. Oncol. 2018, 127, 1–5. [Google Scholar] [CrossRef]
- Bertsekas, D.P.; Tseng, P. Relaxation methods for minimum cost ordinary and generalized network flow problems. Oper. Res. 1988, 36, 93–114. [Google Scholar] [CrossRef] [Green Version]
- Hansen, B.B. Full matching in an observational study of coaching for the SAT. J. Am. Stat. Assoc. 2004, 99, 609–618. [Google Scholar] [CrossRef] [Green Version]
- Hansen, B.B.; Klopfer, S.O. Optimal full matching and related designs via network flows. J. Comput. Graph. Stat. 2006, 15, 609–627. [Google Scholar] [CrossRef] [Green Version]
- Hansen, B.B.; Bowers, J. Covariate balance in simple, stratified and clustered comparative studies. Stat. Sci. 2008, 23, 219–236. [Google Scholar] [CrossRef]
- Ho, D.E.; Imai, K.; King, G.; Stuart, E.A. MatchIt: Nonparametric preprocessing for parametric causal inference. J. Stat. Softw. 2011, 42. [Google Scholar] [CrossRef] [Green Version]
- Ho, D.E.; Imai, K.; King, G.; Stuart, E.A. Matching as nonparametric preprocessing for reducing model dependence in parametric causal inference. Political Anal. 2007, 15, 199–236. [Google Scholar] [CrossRef] [Green Version]
- Iacus, S.M.; King, G.; Porro, G. CEM: Software for coarsened exact matching. J. Stat. Softw. 2009, 30, 9. [Google Scholar] [CrossRef] [Green Version]
- Thoemmes, F. Propensity score matching in SPSS. arXiv 2012, arXiv:1201.6385. Available online: https://arxiv.org/abs/1201.6385 (accessed on 14 October 2020).
- Flentje, M.; Huber, R.M.; Engel-Riedel, W.; Andreas, S.; Kollmeier, J.; Staar, S.; Dickgreber, N.; Vaissiere, N.; De Almeida, C.; Edlich, B.; et al. GILT—A randomised phase III study of oral vinorelbine and cisplatin with concomitant radiotherapy followed by either consolidation therapy with oral vinorelbine and cisplatin or best supportive care alone in stage III non-small cell lung cancer. Strahlenther. Onkol. 2016, 192, 216–222. [Google Scholar] [CrossRef] [PubMed]
- Werner-Wasik, M.; Swann, R.S.; Bradley, J.; Graham, M.; Emami, B.; Purdy, J.; Sause, W. Increasing tumor volume is predictive of poor overall and progression-free survival: Secondary analysis of the Radiation Therapy Oncology Group 93-11 phase I-II radiation dose-escalation study in patients with inoperable non-small-cell lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 385–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basaki, K.; Abe, Y.; Aoki, M.; Kondo, H.; Hatayama, Y.; Nakaji, S. Prognostic factors for survival in stage III non-small-cell lung cancer treated with definitive radiation therapy: Impact of tumor volume. Int. J. Radiat. Oncol. Biol. Phys. 2006, 64, 449–454. [Google Scholar] [CrossRef]
- Alexander, B.M.; Othus, M.; Caglar, H.B.; Allen, A.M. Tumor volume is a prognostic factor in non-small-cell lung cancer treated with chemoradiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 1381–1387. [Google Scholar] [CrossRef] [PubMed]
- Ball, D.L.; Fisher, R.J.; Burmeister, B.H.; Poulsen, M.G.; Graham, P.H.; Penniment, M.G.; Vinod, S.K.; Krawitz, H.E.; Joseph, D.J.; Wheeler, G.C.; et al. The complex relationship between lung tumor volume and survival in patients with non-small cell lung cancer treated by definitive radiotherapy: A prospective, observational prognostic factor study of the Trans-Tasman Radiation Oncology Group (TROG 99.05). Radiother. Oncol. 2013, 106, 305–311. [Google Scholar] [CrossRef] [PubMed]
- Dehing-Oberije, C.; De Ruysscher, D.; van der Weide, H.; Hochstenbag, M.; Bootsma, G.; Geraedts, W.; Pitz, C.; Simons, J.; Teule, J.; Rahmy, A.; et al. Tumor volume combined with number of positive lymph node stations is a more important prognostic factor than TNM stage for survival of non-small-cell lung cancer patients treated with (chemo)radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 1039–1044. [Google Scholar] [CrossRef]
- Wiersma, T.G.; Dahele, M.; Verbakel, W.F.; van de Ven, P.M.; de Haan, P.F.; Smit, E.F.; van Reij, E.J.; Slotman, B.J.; Senan, S. Concurrent chemoradiotherapy for large-volume locally-advanced non-small cell lung cancer. Lung Cancer 2013, 80, 62–67. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Entire Cohort | Retrospective Subgroup | Prospective Subgroup |
|---|---|---|---|
| N (%) | N (%) | N (%) | |
| Total | 122 | 86 | 36 |
| Age, Years | |||
| ≥65 | 81 (66.4) | 58 (67.4) | 23 (63.9) |
| <65 | 41 (33.6) | 28 (32.6) | 13 (36.1) |
| Gender | |||
| Male | 81 (66.4) | 54 (62.8) | 27 (75.0) |
| Female | 41 (33.6) | 32 (37.2) | 9 (25.0) |
| T-stage | |||
| 1 | 13 (10.7) | 7 (8.1) | 6 (16.7) |
| 2 | 20 (16.4) | 16 (18.6) | 4 (11.1) |
| 3 | 33 (27.0) | 27 (31.4) | 6 (16.7) |
| 4 | 56 (45.9) | 36 (41.9) | 20 (55.6) |
| N-stage | |||
| 0 | 15 (12.3) | 9 (10.5) | 6 (16.7) |
| 1 | 9 (7.4) | 7 (8.1) | 2 (5.6) |
| 2 | 44 (36.1) | 29 (33.7) | 15 (41.7) |
| 3 | 54 (44.3) | 41 (47.7) | 13 (36.1) |
| Histology | |||
| Squamous cell carcinoma (SCC) | 59 (48.4) | 38 (44.2) | 21 (58.3) |
| Adenocarcinoma (AC) | 52 (42.6) | 41 (47.7) | 11 (30.6) |
| Not otherwise specified (NOS) | 11 (9.0) | 7 (8.1) | 4 (11.1) |
| Radiographic imaging | |||
| Positron emission tomography (PET)-CT | 118 (96.7) | 82 (95.3) | 36 (100.0) |
| CT | 4 (3.3) | 4 (4.7) | 0 (0.0) |
| Treatment | |||
| Concurrent chemoradiation (CRT) | 55 (45.1) | 32 (37.2) | 23 (63.9) |
| Induction chemotherapy + CRT | 42 (34.4) | 36 (41.9) | 6 (16.7) |
| Sequential chemo and radiotherapy | 15 (12.3) | 11 (12.8) | 4 (11.1) |
| Radiotherapy only | 10 (8.2) | 7 (8.1) | 3 (8.3) |
| Total RT dose ≥ 60 Gy | 113 (92.6) | 77 (89.5) | 36 (100.0) |
| Total RT dose > 54 Gy and <60 Gy | 9 (7.4) | 9 (10.5) | 0 (0.0) |
| Parameter | PTV < 700 ccm | PTV ≥ 700 ccm |
|---|---|---|
| N (%) | N (%) | |
| Total | 29 | 29 |
| Age, Years | ||
| ≥65 | 21 (72.4) | 24 (82.8) |
| <65 | 8 (27.6) | 5 (17.2) |
| Gender | ||
| Male | 16 (55.2) | 23 (79.3) |
| Female | 13 (44.8) | 6 (20.7) |
| T-stage | ||
| 1 | 5 (17.2) | 5 (17.2) |
| 2 | 6 (20.7) | 6 (20.7) |
| 3 | 9 (31.0) | 9 (31.0) |
| 4 | 9 (31.0) | 9 (31.0) |
| N-stage | ||
| 0 | 5 (17.2) | 5 (17.2) |
| 1 | 3 (10.3) | 3 (10.3) |
| 2 | 11 (37.3) | 11 (37.3) |
| 3 | 10 (34.5) | 10 (34.5) |
| Histology | ||
| Squamous cell carcinoma (SCC) | 14 (48.3) | 12 (41.4) |
| Adenocarcinoma (AC) | 13 (44.8) | 13 (44.8) |
| Not otherwise specified (NOS) | 2 (6.9) | 4 (13.8) |
| Treatment | ||
| Concurrent chemoradiation (CRT) | 13 (44.8) | 13 (44.8) |
| Induction chemotherapy + CRT | 10 (34.5) | 9 (31.0) |
| Sequential chemo and radiotherapy | 3 (10.3) | 4 (13.8) |
| Radiotherapy only | 3 (10.3) | 3 (10.3) |
| Total RT dose ≥ 60 Gy | 28 (96.6) | 28 (96.6) |
| Total RT dose > 54 Gy and <60 Gy | 1 (3.4) | 1 (3.4) |
| Patient Cohort | ||
| Retrospective evaluation | 21 (72.4) | 21 (72.4) |
| Prospective evaluation | 8 (27.6) | 8 (27.6) |
| Authors | Paper Name | Year | Results |
|---|---|---|---|
| Wiersma, T.G., et al. | Concurrent chemoradiotherapy for large-volume locally advanced non-small cell lung cancer | 2013 | The single-center, retrospective study included 121 NSCLC stage III patients treated with CRT between 2004 and 2011. Median follow-up for all patients was 37.6 months. Median OS and PFS were 15.7 and 11.6 months, respectively, OS for patients with PTV > 700 ccm was 14.5 vs. 26.5 months for PTV ≤ 700 ccm (p = 0.009). |
| Bradley, J.D., et al. | Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617) | 2015 | The open-label randomized, two-by-two factorial phase 3 study included 166 patients with unresectable NSCLC stage III treated with CRT between 2007 and 2011. On univariate analysis, increasing values of GTV and PTV were associated with an increased risk of death. On multivariate analysis, PTV was among the factors predicting OS. |
| Bradley, J.D., et al. | Long-term results of RTOG 0617 trial: standard- versus high-dose chemoradiotherapy with or without Cetuximab for unresectable stage III non-small-cell lung cancer | 2020 | Long-term results of the RTOG 0617 trial have confirmed a small PTV as a prognostic factor for better OS in inoperable stage III NSCLC treated with concurrent CRT. |
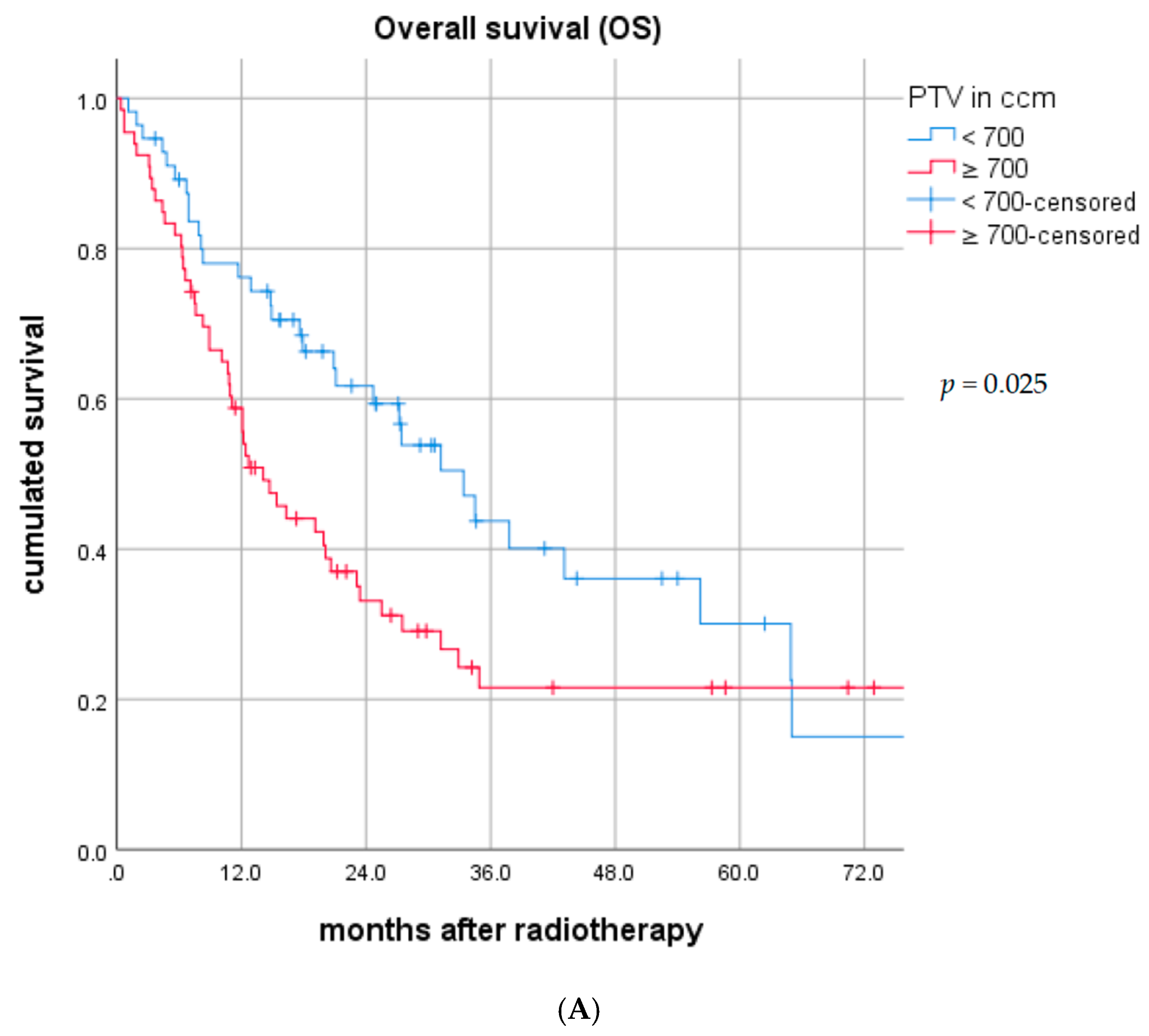
| Present study | Association between planning target volume and patient outcome in inoperable stage III NSCLC treated with chemoradiotherapy | 2020 | The single-center, retrospective and prospective study included 122 NSCLC stage III patients treated with CRT between 2011 and 2018. Median follow-up for all patients was 41.2 months. Median OS and PFS were 20.9 and 7.1 months, respectively, median OS for patients with PTV > 700 ccm was 14.1 vs. 33.4 months for PTV ≤ 700 ccm (p = 0.025). |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karin, M.; Taugner, J.; Käsmann, L.; Eze, C.; Roengvoraphoj, O.; Tufman, A.; Belka, C.; Manapov, F. Association of Planning Target Volume with Patient Outcome in Inoperable Stage III NSCLC Treated with Chemoradiotherapy: A Comprehensive Single-Center Analysis. Cancers 2020, 12, 3035. https://doi.org/10.3390/cancers12103035
Karin M, Taugner J, Käsmann L, Eze C, Roengvoraphoj O, Tufman A, Belka C, Manapov F. Association of Planning Target Volume with Patient Outcome in Inoperable Stage III NSCLC Treated with Chemoradiotherapy: A Comprehensive Single-Center Analysis. Cancers. 2020; 12(10):3035. https://doi.org/10.3390/cancers12103035
Chicago/Turabian StyleKarin, Monika, Julian Taugner, Lukas Käsmann, Chukwuka Eze, Olarn Roengvoraphoj, Amanda Tufman, Claus Belka, and Farkhad Manapov. 2020. "Association of Planning Target Volume with Patient Outcome in Inoperable Stage III NSCLC Treated with Chemoradiotherapy: A Comprehensive Single-Center Analysis" Cancers 12, no. 10: 3035. https://doi.org/10.3390/cancers12103035