Comparative Analysis of Two Methods for the Detection of EGFR Mutations in Plasma Circulating Tumor DNA from Lung Adenocarcinoma Patients


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
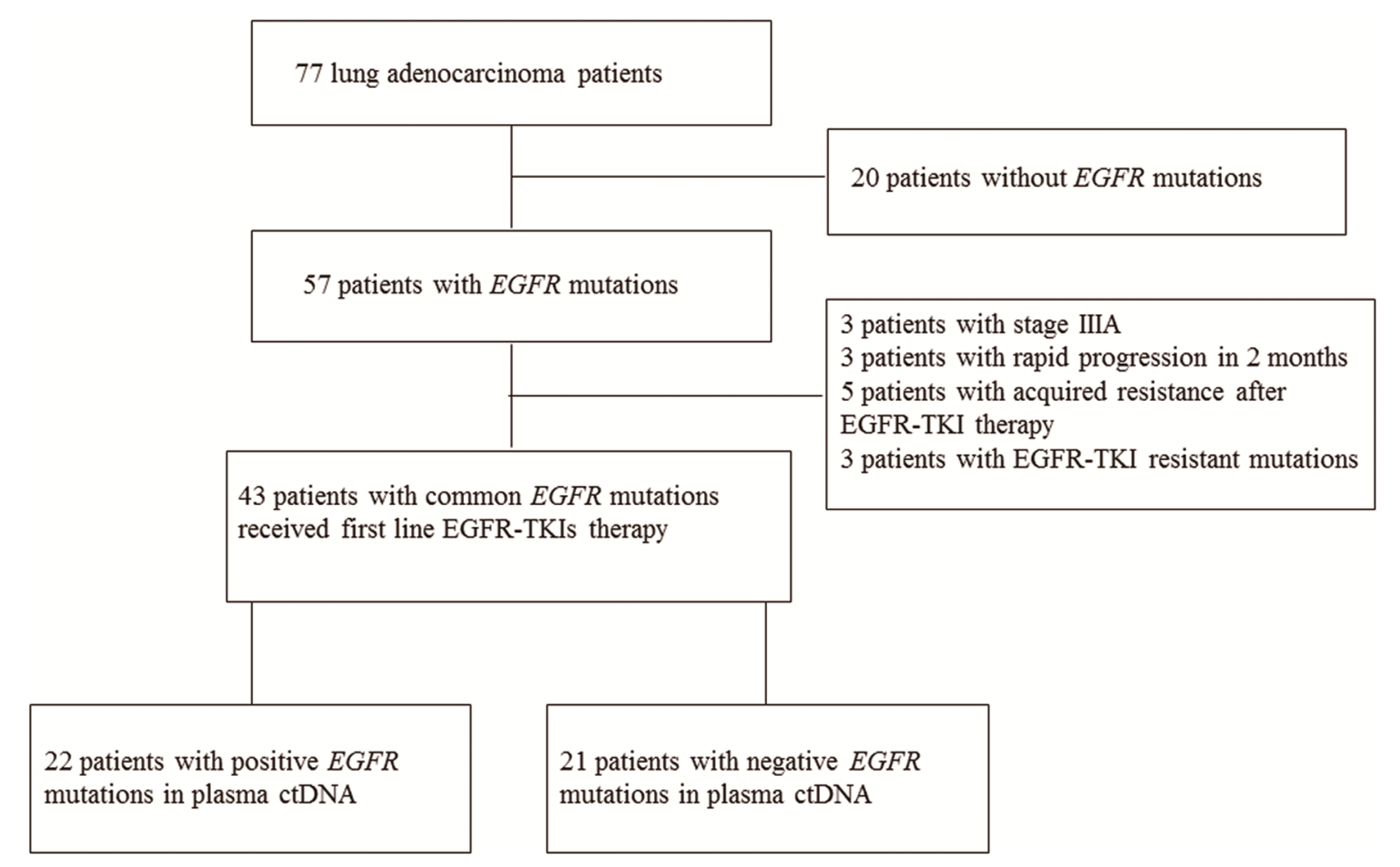
2.1. Patients and Study Design
2.2. DNA Extraction
2.3. Statistical Analysis
3. Results
3.1. Comparison of ARMS and SABER/MassARRAY for the Detection of EGFR Mutations in Plasma ctDNA
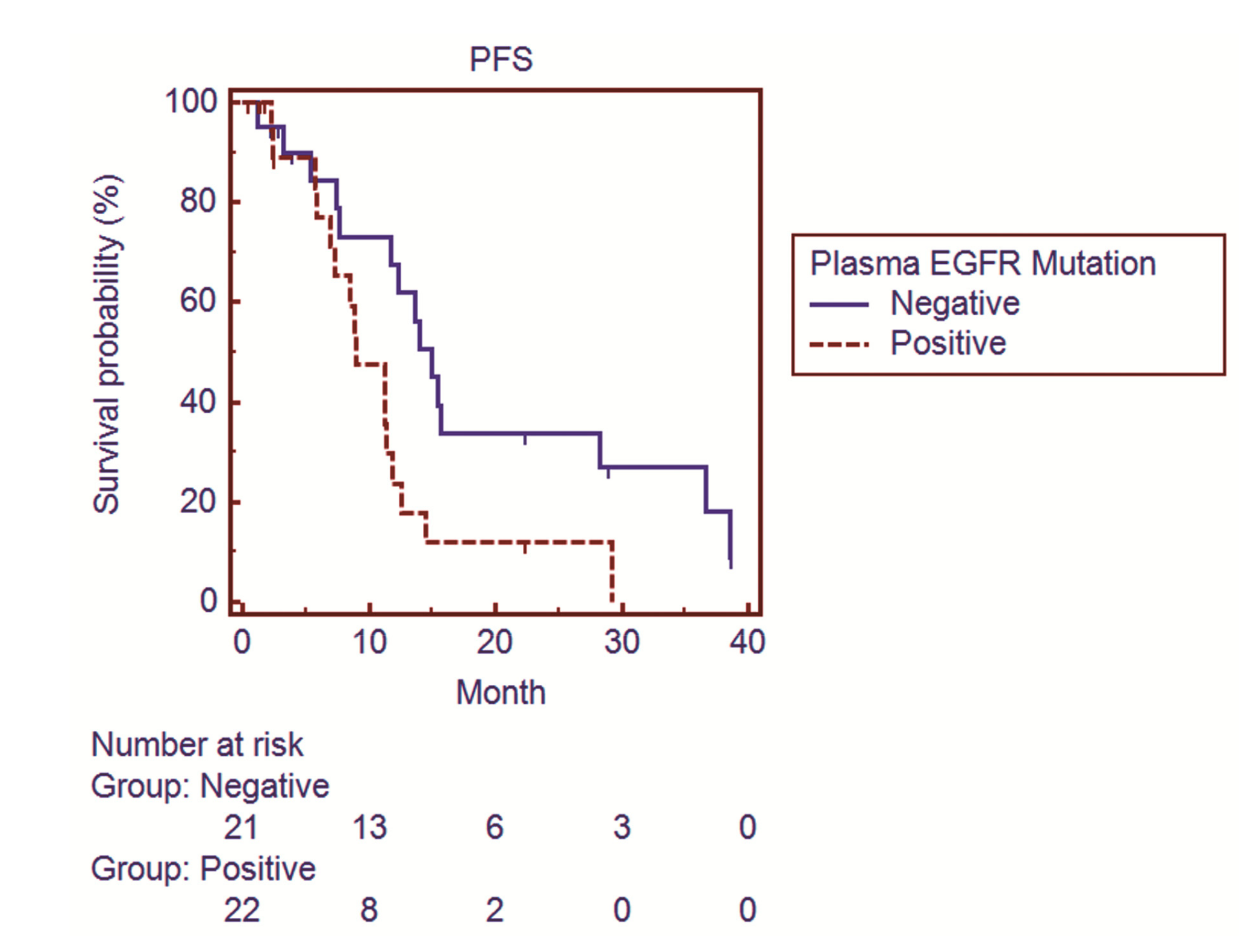
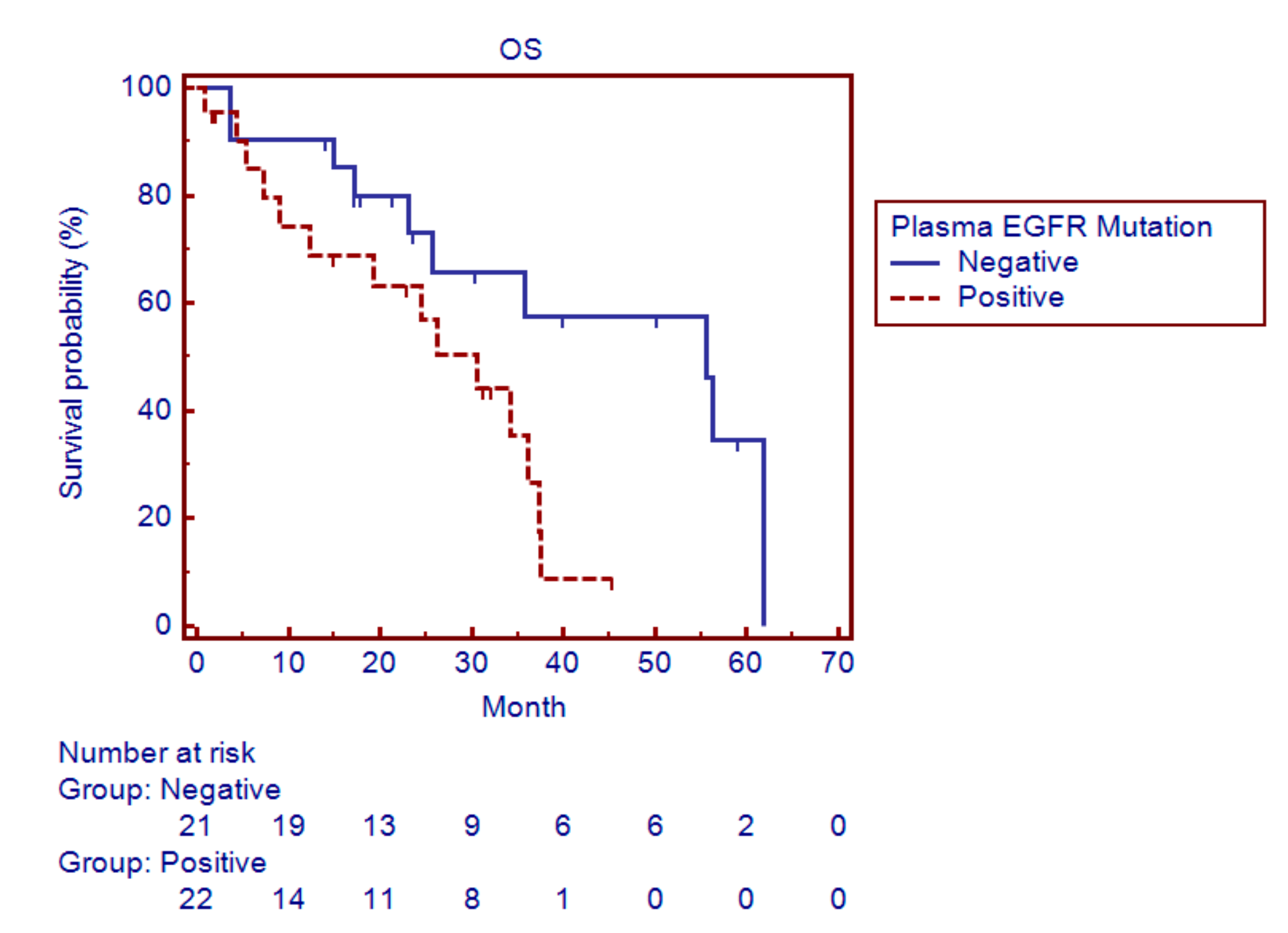
3.2. Relationship between the EGFR Mutation Status after EGFR-TKI Therapy and Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Arteaga, C.L. Epidermal growth factor receptor dependence in human tumors: More than just expression? Oncologist 2002, 7, S31–S39. [Google Scholar] [CrossRef] [PubMed]
- Lynch, T.J.; Bell, D.W.; Sordella, R.; Gurubhagavatula, S.; Okimoto, R.A.; Brannigan, B.W.; Harris, P.L.; Haserlat, S.M.; Supko, J.G.; Haluska, F.G.; et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N. Engl. J. Med. 2004, 350, 2129–2139. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.L.; Zhong, W.Z.; Li, L.Y.; Zhang, X.T.; Zhang, L.; Zhou, C.C.; Liu, W.; Jiang, B.; Mu, X.L.; Lin, J.Y.; et al. Epidermal growth factor receptor mutations and their correlation with gefitinib therapy in patients with non-small cell lung cancer: A meta-analysis based on updated individual patient data from six medical centers in mainland China. J. Thorac. Oncol. 2007, 2, 430–439. [Google Scholar] [CrossRef] [PubMed]
- Paez, J.G.; Janne, P.A.; Lee, J.C.; Tracy, S.; Greulich, H.; Gabriel, S.; Herman, P.; Kaye, F.J.; Lindeman, N.; Boggon, T.J.; et al. EGFR mutations in lung cancer: Correlation with clinical response to gefitinib therapy. Science 2004, 304, 1497–1500. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.F.; Liu, H.P.; Li, L.H.; Ku, Y.C.; Fu, Y.N.; Tsai, H.Y.; Chen, Y.T.; Lin, Y.F.; Chang, W.C.; Kuo, H.P.; et al. High frequency of epidermal growth factor receptor mutations with complex patterns in non-small cell lung cancers related to gefitinib responsiveness in Taiwan. Clin. Cancer Res. 2004, 10, 8195–8203. [Google Scholar] [CrossRef] [PubMed]
- Gazdar, A.F.; Shigematsu, H.; Herz, J.; Minna, J.D. Mutations and addiction to EGFR: The Achilles ’heal’ of lung cancers? Trends Mol. Med. 2004, 10, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.L.; Thongprasert, S.; Yang, C.H.; Chu, D.T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef]
- Zhou, C.; Wu, Y.L.; Chen, G.; Feng, J.; Liu, X.Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): A multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef]
- Wu, Y.L.; Zhou, C.; Hu, C.P.; Feng, J.; Lu, S.; Huang, Y.; Li, W.; Hou, M.; Shi, J.H.; Lee, K.Y.; et al. Afatinib versus cisplatin plus gemcitabine for first-line treatment of Asian patients with advanced non-small-cell lung cancer harbouring EGFR mutations (LUX-Lung 6): An open-label, randomised phase 3 trial. Lancet Oncol. 2014, 15, 213–222. [Google Scholar] [CrossRef]
- Palmirotta, R.; Lovero, D.; Cafforio, P.; Felici, C.; Mannavola, F.; Pelle, E.; Quaresmini, D.; Tucci, M.; Silvestris, F. Liquid biopsy of cancer: A multimodal diagnostic tool in clinical oncology. Ther. Adv. Med. Oncol. 2018, 10. [Google Scholar] [CrossRef]
- Douillard, J.Y.; Ostoros, G.; Cobo, M.; Ciuleanu, T.; Cole, R.; McWalter, G.; Walker, J.; Dearden, S.; Webster, A.; Milenkova, T.; et al. Gefitinib treatment in EGFR mutated caucasian NSCLC: Circulating-free tumor DNA as a surrogate for determination of EGFR status. J. Thorac. Oncol. 2014, 9, 1345–1353. [Google Scholar] [CrossRef] [PubMed]
- Marchetti, A.; Palma, J.F.; Felicioni, L.; de Pas, T.M.; Chiari, R.; del Grammastro, M.; Filice, G.; Ludovini, V.; Brandes, A.A.; Chella, A.; et al. Early Prediction of Response to Tyrosine Kinase Inhibitors by Quantification of EGFR Mutations in Plasma of NSCLC Patients. J. Thorac. Oncol. 2015, 10, 1437–1443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vallee, A.; le Loupp, A.G.; Denis, M.G. Efficiency of the Therascreen(R) RGQ PCR kit for the detection of EGFR mutations in non-small cell lung carcinomas. Clin. Chim. Acta 2014, 429, 8–11. [Google Scholar] [CrossRef]
- Kimura, H.; Suminoe, M.; Kasahara, K.; Sone, T.; Araya, T.; Tamori, S.; Koizumi, F.; Nishio, K.; Miyamoto, K.; Fujimura, M.; et al. Evaluation of epidermal growth factor receptor mutation status in serum DNA as a predictor of response to gefitinib (IRESSA). Br. J. Cancer. 2007, 97, 778–784. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakai, K.; Horiike, A.; Irwin, D.L.; Kudo, K.; Fujita, Y.; Tanimoto, A.; Sakatani, T.; Saito, R.; Kaburaki, K.; Yanagitani, N.; et al. Detection of epidermal growth factor receptor T790M mutation in plasma DNA from patients refractory to epidermal growth factor receptor tyrosine kinase inhibitor. Cancer Sci. 2013, 104, 1198–1204. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Wang, S.; Han, X.; Hu, X.; Wang, X.; Zhao, L.; Tang, L.; Feng, Y.; Wu, D.; Sun, Y.; Shi, Y. Clinical significance of pretreatment plasma biomarkers in advanced non-small cell lung cancer patients. Clin. Chim. Acta 2014, 430, 63–70. [Google Scholar] [CrossRef]
- Liu, X.; Lu, Y.; Zhu, G.; Lei, Y.; Zheng, L.; Qin, H.; Tang, C.; Ellison, G.; McCormack, R.; Ji, Q. The diagnostic accuracy of pleural effusion and plasma samples versus tumour tissue for detection of EGFR mutation in patients with advanced non-small cell lung cancer: Comparison of methodologies. J. Clin. Pathol. 2013, 66, 1065–1069. [Google Scholar] [CrossRef]
- Zhang, C.; Wei, B.; Li, P.; Yang, K.; Wang, Z.; Ma, J.; Guo, Y. Prognostic value of plasma EGFR ctDNA in NSCLC patients treated with EGFR-TKIs. PLoS ONE 2017, 12, e0173524. [Google Scholar] [CrossRef]
- Mehrotra, M.; Singh, R.R.; Loghavi, S.; Duose, D.Y.; Barkoh, B.A.; Behrens, C.; Patel, K.P.; Routbort, M.J.; Kopetz, S.; Broaddus, R.R.; et al. Detection of somatic mutations in cell-free DNA in plasma and correlation with overall survival in patients with solid tumors. Oncotarget 2018, 9, 10259–10271. [Google Scholar] [CrossRef]
- Brevet, M.; Johnson, M.L.; Azzoli, C.G.; Ladanyi, M. Detection of EGFR mutations in plasma DNA from lung cancer patients by mass spectrometry genotyping is predictive of tumor EGFR status and response to EGFR inhibitors. Lung Cancer 2011, 73, 96–102. [Google Scholar] [CrossRef] [Green Version]
- Ellison, G.; Donald, E.; McWalter, G.; Knight, L.; Fletcher, L.; Sherwood, J.; Cantarini, M.; Orr, M.; Speake, G. A comparison of ARMS and DNA sequencing for mutation analysis in clinical biopsy samples. J. Exp. Clin. Cancer Res. 2010, 29, 132. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.; Wu, Y.L.; Lee, J.S.; Yu, C.J.; Sriuranpong, V.; Sandoval-Tan, J.; Ladrera, G.; Thongprasert, S.; Srimuninnimit, V.; Liao, M.; et al. Detection and Dynamic Changes of EGFR Mutations from Circulating Tumor DNA as a Predictor of Survival Outcomes in NSCLC Patients Treated with First-line Intercalated Erlotinib and Chemotherapy. Clin. Cancer Res. 2015, 21, 3196–3203. [Google Scholar] [CrossRef] [PubMed]
- Thress, K.S.; Brant, R.; Carr, T.H.; Dearden, S.; Jenkins, S.; Brown, H.; Hammett, T.; Cantarini, M.; Barrett, J.C. EGFR mutation detection in ctDNA from NSCLC patient plasma: A cross-platform comparison of leading technologies to support the clinical development of AZD9291. Lung Cancer 2015, 90, 509–515. [Google Scholar] [CrossRef] [Green Version]
- Uchida, J.; Kato, K.; Kukita, Y.; Kumagai, T.; Nishino, K.; Daga, H.; Nagatomo, I.; Inoue, T.; Kimura, M.; Oba, S.; et al. Diagnostic Accuracy of Noninvasive Genotyping of EGFR in Lung Cancer Patients by Deep Sequencing of Plasma Cell-Free DNA. Clin. Chem. 2015, 61, 1191–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elazezy, M.; Joosse, S.A. Techniques of using circulating tumor DNA as a liquid biopsy component in cancer management. Comput. Struct. Biotechnol. J. 2018, 16, 370–378. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| ARMS vs. Tissue | |||
| ARMS | Tissue | ||
| Negative | Positive | ||
| Negative | 18 | 29 | |
| Positive | 2 | 28 | |
| Sensitivity: 49.1% | Specificity: 90% | PPV: 93.3% | NPV: 48.7% |
| SABER/MassARRAY vs. Tissue | |||
| SABER/MassARRAY | Tissue | ||
| Negative | Positive | ||
| Negative | 19 | 22 | |
| Positive | 1 | 28 | |
| Sensitivity: 56% | Specificity: 95% | PPV: 96.6% | NPV: 46.3% |
| Exon 19 Deletions ARMS vs. Tissue | |||
| ARMS | Tissue | ||
| Negative | Positive | ||
| Negative | 43 | 16 | |
| Positive | 2 | 16 | |
| Sensitivity: 50% | Specificity: 95.6% | PPV: 88.9% | NPV: 72.9% |
| SABER/MassARRAY vs. Tissue | |||
| SABER/MassARRAY | Tissue | ||
| Negative | Positive | ||
| Negative | 43 | 12 | |
| Positive | 1 | 14 | |
| Sensitivity: 53.8% | Specificity: 97.7% | PPV: 93.3% | NPV: 78.2% |
| L858R ARMS vs. Tissue | |||
| ARMS | Tissue | ||
| Negative | Positive | ||
| Negative | 57 | 11 | |
| Positive | 0 | 9 | |
| Sensitivity: 45% | Specificity: 100% | PPV: 100% | NPV: 83.8% |
| SABER/MassARRAY vs. Tissue | |||
| SABER/MassARRAY | Tissue | ||
| Negative | Positive | ||
| Negative | 51 | 10 | |
| Positive | 0 | 9 | |
| Sensitivity: 47.4% | Specificity: 100% | PPV: 100% | NPV: 83.6% |
| T790M ARMS vs. Tissue | |||
| ARMS | Tissue | ||
| Negative | Positive | ||
| Negative | 70 | 4 | |
| Positive | 0 | 2 | |
| Sensitivity: 33.3% | Specificity: 100% | PPV: 100% | NPV: 94.6% |
| SABER/MassARRAY vs. Tissue | |||
| SABER/MassARRAY | Tissue | ||
| Negative | Positive | ||
| Negative | 64 | 3 | |
| Positive | 0 | 3 | |
| Sensitivity: 50% | Specificity: 100% | PPV: 100% | NPV: 95.5% |
| Characteristics | No (%) |
|---|---|
| Patient | 43 (100) |
| Sex | |
| Male | 15 (34.9) |
| Female | 28 (65.1) |
| Smoking | |
| Yes | 4 (9.3) |
| No | 39 (90.7) |
| Age (year)(median) | 71 |
| Pathology | |
| Adenocarcinoma | 43 (100) |
| EGFR-TKI | |
| Gefitinib | 20 (46.5) |
| Erlotinib | 13 (30.2) |
| Afatinib | 10 (23.3) |
| Mutations | |
| Exon 19 | 27 (62.8) |
| Exon 21 | 16 (37.2) |
| Stage | |
| IIIB | 3 (7) |
| IV | 40 (93) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hung, M.-S.; Lung, J.-H.; Lin, Y.-C.; Fang, Y.-H.; Huang, S.-Y.; Jiang, Y.-Y.; Hsieh, M.-J.; Tsai, Y.-H. Comparative Analysis of Two Methods for the Detection of EGFR Mutations in Plasma Circulating Tumor DNA from Lung Adenocarcinoma Patients. Cancers 2019, 11, 803. https://doi.org/10.3390/cancers11060803
Hung M-S, Lung J-H, Lin Y-C, Fang Y-H, Huang S-Y, Jiang Y-Y, Hsieh M-J, Tsai Y-H. Comparative Analysis of Two Methods for the Detection of EGFR Mutations in Plasma Circulating Tumor DNA from Lung Adenocarcinoma Patients. Cancers. 2019; 11(6):803. https://doi.org/10.3390/cancers11060803
Chicago/Turabian StyleHung, Ming-Szu, Jr-Hau Lung, Yu-Ching Lin, Yu-Hung Fang, Shu-Yi Huang, Yuan-Yuan Jiang, Meng-Jer Hsieh, and Ying-Huang Tsai. 2019. "Comparative Analysis of Two Methods for the Detection of EGFR Mutations in Plasma Circulating Tumor DNA from Lung Adenocarcinoma Patients" Cancers 11, no. 6: 803. https://doi.org/10.3390/cancers11060803