Circulating MicroRNA Biomarkers for Lung Cancer Detection in East Asian Populations


Abstract
:1. Introduction
2. Methods
2.1. Literature Search
2.2. Eligibility Criteria
2.3. Data Extraction and Statistical Analysis
2.4. Quality Assessment
3. Results
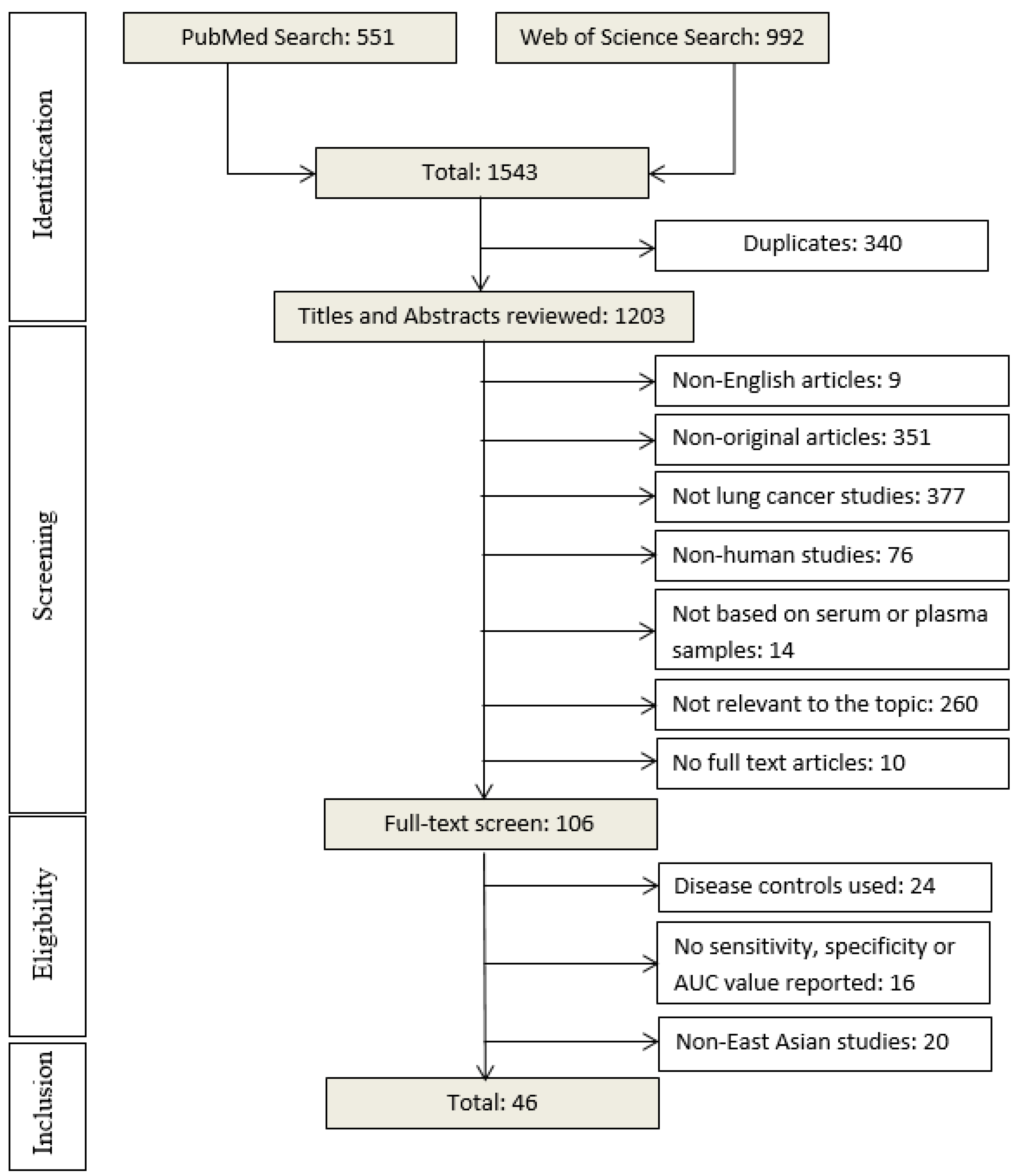
3.1. Literature Search Result
3.2. Study Quality and Characteristics
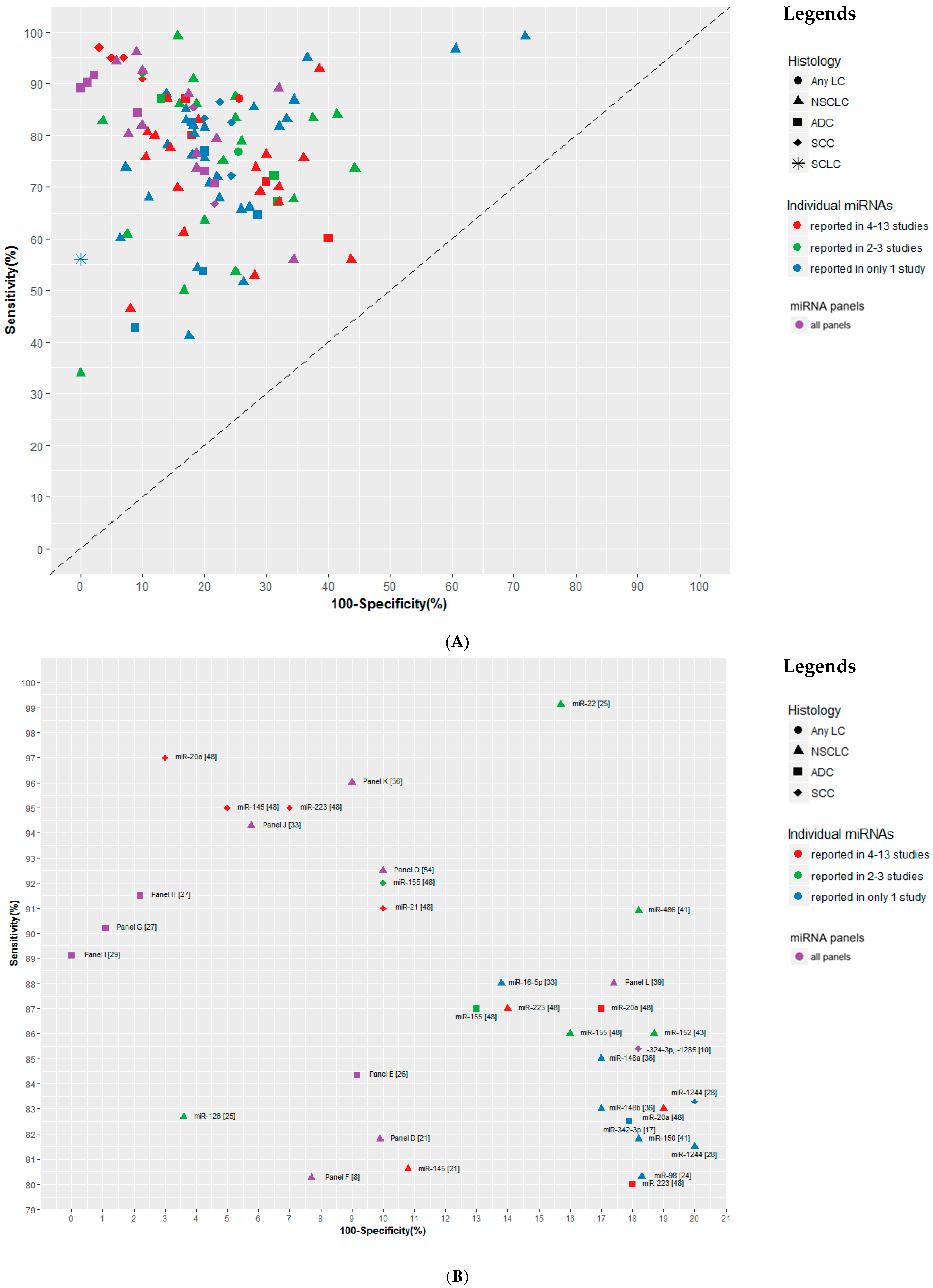
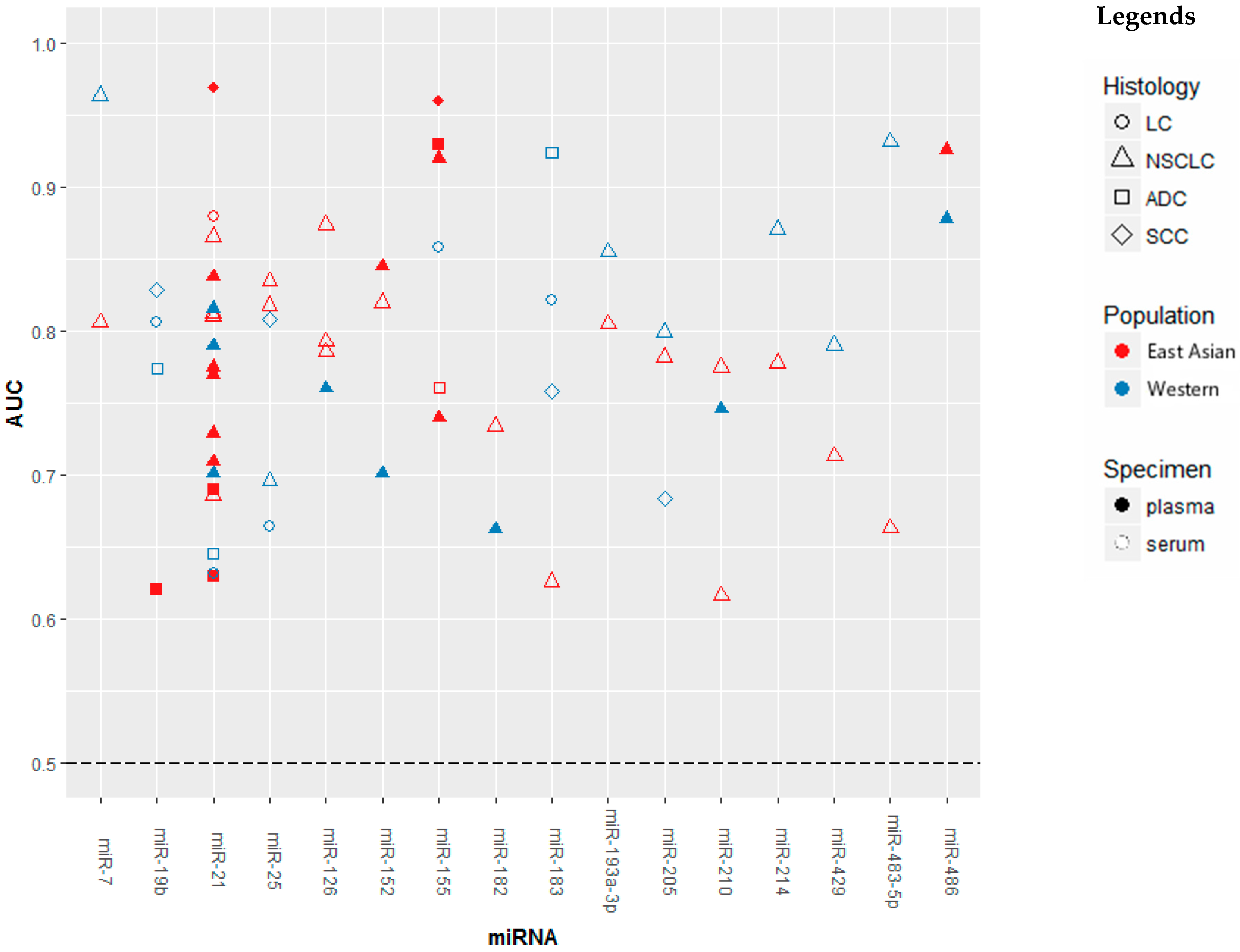
3.3. Diagnostic Performance of miRNA Markers
3.4. Direction of Dysregulation of Circulating miRNAs
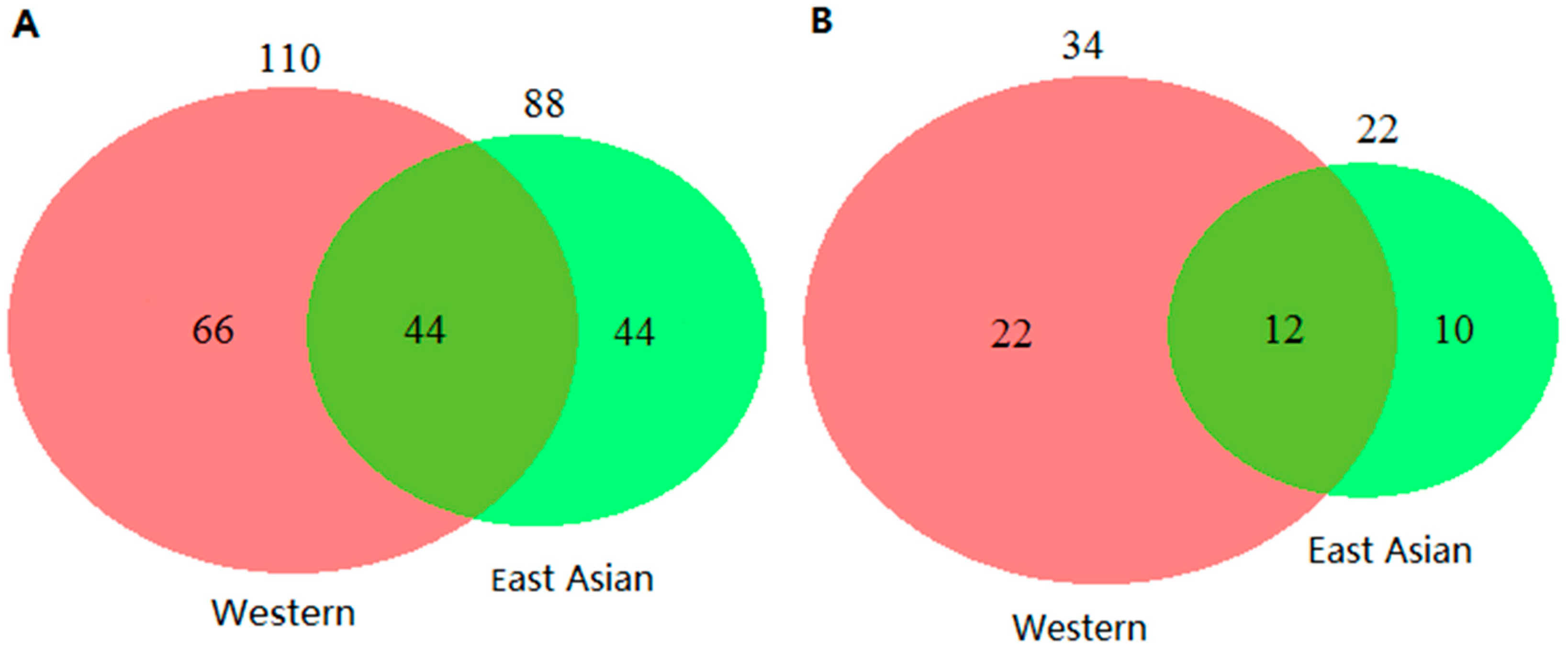
3.5. Comparison of miRNAs Profiles for LC Detection between Eastern Asian and Western Populations
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA-Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, F.R.; Scagliotti, G.V.; Mulshine, J.L.; Kwon, R.; Curran, W.J., Jr.; Wu, Y.L.; Paz-Ares, L. Lung cancer: Current therapies and new targeted treatments. Lancet 2017, 389, 299–311. [Google Scholar] [CrossRef]
- Torre, L.A.; Siegel, R.L.; Jemal, A. Lung cancer statistics. Adv. Exp. Med. Biol. 2016, 893, 1–19. [Google Scholar]
- Manser, R.; Lethaby, A.; Irving, L.B.; Stone, C.; Byrnes, G.; Abramson, M.J.; Campbell, D. Screening for lung cancer. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [Green Version]
- Horeweg, N.; Scholten, E.T.; de Jong, P.A.; van der Aalst, C.M.; Weenink, C.; Lammers, J.W.J.; Nackaerts, K.; Vliegenthart, R.; ten Haaf, K.; Yousaf-Khan, U.A.; et al. Detection of lung cancer through low-dose ct screening (nelson): A prespecifi ed analysis of screening test performance and interval cancers. Lancet Oncol. 2014, 15, 1342–1350. [Google Scholar] [CrossRef]
- Shen, J.; Liao, J.; Guarnera, M.A.; Fang, H.; Cai, L.; Stass, S.A.; Jiang, F. Analysis of micrornas in sputum to improve computed tomography for lung cancer diagnosis. J. Thorac. Oncol. 2014, 9, 33–40. [Google Scholar] [CrossRef] [PubMed]
- Garzon, R.; Calin, G.A.; Croce, C.M. Micrornas in cancer. Annu. Rev. Med. 2009, 60, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Jin, X.; Chen, Y.; Chen, H.; Fei, S.; Chen, D.; Cai, X.; Liu, L.; Lin, B.; Su, H.; Zhao, L.; et al. Evaluation of tumor-derived exosomal mirna as potential diagnostic biomarkers for early-stage non-small cell lung cancer using next-generation sequencing. Clin. Cancer Res. 2017, 23, 5311–5319. [Google Scholar] [CrossRef] [PubMed]
- Zhu, W.Y.; Zhou, K.Y.; Zha, Y.; Chen, D.D.; He, J.Y.; Ma, H.J.; Liu, X.G.; Le, H.B.; Zhang, Y.K. Diagnostic value of serum mir-182, mir-183, mir-210 and mir-126 levels in patients with early-stage non-small cell lung cancer. PLoS ONE 2016, 11, e0153046. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.J.; Wang, Y.; Zhao, H.; Wei, F.; Zhang, X.W.; Su, Y.J.; Wang, C.L.; Li, H.; Ren, X.B. Plasma mir-324-3p and mir-1285 as diagnostic and prognostic biomarkers for early stage lung squamous cell carcinoma. Oncotarget 2016, 7, 59664–59675. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.S.; Gamazon, E.R.; Ziliak, D.; Wen, Y.; Im, H.K.; Zhang, W.; Wing, C.; Duan, S.; Bleibel, W.K.; Cox, N.J.; et al. Population differences in microrna expression and biological implications. RNA Biol. 2011, 8, 692–701. [Google Scholar] [CrossRef]
- Yu, H.; Guan, Z.; Cuk, K.; Brenner, H.; Zhang, Y. Circulating microrna biomarkers for lung cancer detection in western populations. Cancer Med. 2018, 7, 4849–4862. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Grp, P. Preferred reporting items for systematic reviews and meta-analyses: The prisma statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Zhao, Y.Z. The diagnostic and prognostic role of circulating mir-141 expression in non-small-cell lung cancer patients. Int. J. Clin. Exp. Pathol. 2018, 11, 2597–2604. [Google Scholar]
- Sun, B.; Liu, H.F.; Ding, Y.; Li, Z. Evaluating the diagnostic and prognostic value of serum mir-770 in non-small cell lung cancer. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 3061–3066. [Google Scholar] [PubMed]
- Shan, X.; Zhang, H.; Zhang, L.; Zhou, X.; Wang, T.S.; Zhang, J.Y.; Shu, Y.Q.; Zhu, W.; Wen, W.; Liu, P. Identification of four plasma micrornas as potential biomarkers in the diagnosis of male lung squamous cell carcinoma patients in china. Cancer Med. 2018, 7, 2370–2381. [Google Scholar] [CrossRef] [PubMed]
- Qin, Y.Z.; Zhou, X.Y.; Huang, C.; Li, L.; Liu, H.S.; Liang, N.X.; Chen, Y.Y.; Ma, D.J.; Han, Z.J.; Xu, X.H.; et al. Serum mir-342-3p is a novel diagnostic and prognostic biomarker for non-small cell lung cancer. Int. J. Clin. Exp. Pathol. 2018, 11, 2742–2748. [Google Scholar]
- Bao, M.; Pan, S.; Yang, W.L.; Chen, S.; Shan, Y.B.; Shi, H.C. Serum mir-10a-5p and mir-196a-5p as non-invasive biomarkers in non-small cell lung cancer. Int. J. Clin. Exp. Pathol. 2018, 11, 773–780. [Google Scholar]
- Zhou, X.; Wen, W.; Shan, X.; Zhu, W.; Xu, J.; Guo, R.H.; Cheng, W.F.; Wang, F.; Qi, L.W.; Chen, Y.; et al. A six-microrna panel in plasma was identified as a potential biomarker for lung adenocarcinoma diagnosis. Oncotarget 2017, 8, 6513–6525. [Google Scholar] [CrossRef]
- Zhang, L.; Shan, X.; Wang, J.; Zhu, J.; Huang, Z.; Zhang, H.; Zhou, X.; Cheng, W.F.; Shu, Y.Q.; Zhu, W.; et al. A three-microrna signature for lung squamous cell carcinoma diagnosis in chinese male patients. Oncotarget 2017, 8, 86897–86907. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Mao, F.; Shen, T.; Luo, Q.; Ding, Z.; Qian, L.; Huang, J. Plasma mir-145, mir-20a, mir-21 and mir-223 as novel biomarkers for screening early-stage non-small cell lung cancer. Oncol. Lett. 2017, 13, 669–676. [Google Scholar] [CrossRef]
- Yu, Y.L.; Zuo, J.C.; Tan, Q.; Thin, K.Z.; Li, P.; Zhu, M.; Yu, M.X.; Fu, Z.M.; Liang, C.Z.; Tu, J.C. Plasma mir-92a-2 as a biomarker for small cell lung cancer. Cancer Biomark. 2017, 18, 319–327. [Google Scholar] [CrossRef]
- Yang, M.; Xiao, L.B.; Zhang, Y.H.; Li, G.J.; Zhou, J.W. Clinical significance of serum mir-31 as a predictive biomarker for lung adenocarcinoma. Int. J. Clin. Exp. Pathol. 2017, 10, 4668–4674. [Google Scholar]
- Wang, K.C.; Dong, L.Y.; Fang, Q.M.; Xia, H.W.; Hou, X.L. Low serum mir-98 as an unfavorable prognostic biomarker in patients with non-small cell lung cancer. Cancer Biomark. 2017, 20, 283–288. [Google Scholar] [CrossRef]
- Shang, A.Q.; Xie, Y.N.; Wang, J.; Sun, L.; Wei, J.; Lu, W.Y.; Lan, J.Y.; Wang, W.W.; Wang, L.; Wang, L.L. Predicative values of serum microrna-22 and microrna-126 levels for non-small cell lung cancer development and metastasis: A case-control study. Neoplasma 2017, 64, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Lv, S.G.; Xue, J.; Wu, C.Y.; Wang, L.; Wu, J.; Xu, S.J.; Liang, X.H.; Lou, J.T. Identification of a panel of serum micrornas as biomarkers for early detection of lung adenocarcinoma. J. Cancer 2017, 8, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhao, H.; Gao, X.J.; Wei, F.; Zhang, X.W.; Su, Y.J.; Wang, C.L.; Li, H.; Ren, X.B. Identification of a three-mirna signature as a blood-borne diagnostic marker for early diagnosis of lung adenocarcinoma. Oncotarget 2016, 7, 26070–26086. [Google Scholar] [CrossRef]
- Wang, W.Z.; Li, W.L.; Ding, M.J.; Yuan, H.N.; Yang, J.; Meng, W.; Jin, E.; Wang, X.J.; Ma, S.L. Identification of mirnas as non-invasive biomarkers for early diagnosis of lung cancers. Tumor Biol. 2016, 37, 16287–16293. [Google Scholar] [CrossRef] [PubMed]
- Tai, M.C.; Yanagisawa, K.; Nakatochi, M.; Hotta, N.; Hosono, Y.; Kawaguchi, K.; Naito, M.; Taniguchi, H.; Wakai, K.; Yokoi, K.; et al. Blood-borne mirna profile-based diagnostic classifier for lung adenocarcinoma. Sci. Rep. 2016, 6, 31389. [Google Scholar] [CrossRef]
- Sun, M.Z.; Song, J.X.; Zhou, Z.W.; Zhu, R.; Jin, H.; Ji, Y.Q.; Lu, Q.; Ju, H.X. Comparison of serum microrna21 and tumor markers in diagnosis of early non-small cell lung cancer. Dis. Markers 2016, 2016, 3823121. [Google Scholar] [CrossRef]
- Su, K.L.; Zhang, T.C.; Wang, Y.R.; Hao, G.J. Diagnostic and prognostic value of plasma microrna-195 in patients with non-small cell lung cancer. World J. Surg. Oncol. 2016, 14, 224. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.; Wang, J.; Li, J.; Zhao, M.; Huang, S.K.; Gu, Y.Y.; Li, Y.; Sun, X.J.; Yang, L.; Luo, Q.; et al. A circulating non-coding rna panel as an early detection predictor of non-small cell lung cancer. Life Sci. 2016, 151, 235–242. [Google Scholar] [CrossRef] [PubMed]
- Fan, L.H.; Qi, H.W.; Teng, J.L.; Su, B.; Chen, H.; Wang, C.H.; Xia, Q. Identification of serum mirnas by nano-quantum dots microarray as diagnostic biomarkers for early detection of non-small cell lung cancer. Tumor Biol. 2016, 37, 7777–7784. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.C.; Chen, Z.L.; Dong, J.S.; Li, J.G.; Shi, X.J.; Sun, N.; Luo, M.; Zhou, F.; Tan, F.W.; He, J. Combination of serum mirnas with cyfra21-1 for the diagnosis of non-small cell lung cancer. Cancer Lett. 2015, 367, 138–146. [Google Scholar] [CrossRef]
- Zhao, W.; Zhao, J.J.; Zhang, L.; Xu, Q.F.; Zhao, Y.M.; Shi, X.Y.; Xu, A.G. Serum mir-21 level: A potential diagnostic and prognostic biomarker for non-small cell lung cancer. Int. J. Clin. Exp. Med. 2015, 8, 14759–14763. [Google Scholar] [PubMed]
- Yang, J.S.; Li, B.J.; Lu, H.W.; Chen, Y.; Lu, C.; Zhu, R.X.; Liu, S.H.; Yi, Q.T.; Li, J.; Song, C.H. Serum mir-152, mir-148a, mir-148b and mir-21 as novel biomarkers in non-small cell lung cancer screening. Tumor Biol. 2015, 36, 3035–3042. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.J.; Ma, J.Y.; Wang, L.; Gu, W. Expression and significance of circulating microrna-31 in lung cancer patients. Med. Sci. Monit. 2015, 21, 722–726. [Google Scholar] [PubMed]
- Wang, R.J.; Zheng, Y.H.; Wang, P.; Zhang, J.Z. Serum mir-125a-5p, mir-145 and mir-146a as diagnostic biomarkers in non-small cell lung cancer. Int. J. Clin. Exp. Pathol. 2015, 8, 765–771. [Google Scholar] [PubMed]
- Wang, P.; Yang, D.W.; Zhang, H.L.; Wei, X.Y.; Ma, T.L.; Cheng, Z.L.; Hong, Q.Y.; Hu, J.; Zhuo, H.J.; Song, Y.L.; et al. Early detection of lung cancer in serum by a panel of microrna biomarkers. Clin. Lung Cancer 2015, 16, 313–319.e1. [Google Scholar] [CrossRef]
- Wang, C.; Ding, M.; Xia, M.D.; Chen, S.D.; Le, A.V.; Soto-Gil, R.; Shen, Y.; Wang, N.; Wang, J.J.; Gu, W.J.; et al. A five-mirna panel identified from a multicentric case-control study serves as a novel diagnostic tool for ethnically diverse non-small-cell lung cancer patients. Ebiomedicine 2015, 2, 1377–1385. [Google Scholar] [CrossRef]
- Li, W.S.; Wang, Y.; Zhang, Q.; Tang, L.L.; Liu, X.P.; Dai, Y.H.; Xiao, L.; Huang, S.G.; Chen, L.; Guo, Z.M.; et al. Microrna-486 as a biomarker for early diagnosis and recurrence of non-small cell lung cancer. PLoS ONE 2015, 10, e0134220. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.G.; Zhang, Y.X.; Zhang, Y.; Shi, Y.; Xi, J.J.; Fan, H.; Xu, S.T. Decreased expression of mir-204 in plasma is associated with a poor prognosis in patients with non-small cell lung cancer. Int. J. Mol. Med. 2015, 36, 1720–1726. [Google Scholar] [CrossRef] [PubMed]
- Dou, H.L.; Wang, Y.; Su, G.; Zhao, S. Decreased plasma let-7c and mir-152 as noninvasive biomarker for non-small-cell lung cancer. Int. J. Clin. Exp. Med. 2015, 8, 9291–9298. [Google Scholar] [PubMed]
- Zhu, W.Y.; Luo, B.; An, J.Y.; He, J.Y.; Chen, D.D.; Xu, L.Y.; Huang, Y.Y.; Liu, X.G.; Le, H.B.; Zhang, Y.K. Differential expression of mir-125a-5p and let-7e predicts the progression and prognosis of non-small cell lung cancer. Cancer Investig. 2014, 32, 394–401. [Google Scholar] [CrossRef]
- Zhu, W.Y.; He, J.Y.; Chen, D.D.; Zhang, B.J.; Xu, L.Y.; Ma, H.J.; Liu, X.G.; Zhang, Y.K.; Le, H.B. Expression of mir-29c, mir-93 and mir-429 as potential biomarkers for detection of early stage non-small lung cancer. PLoS ONE 2014, 9, e87780. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Zhang, Q.; Wu, L.; Jia, C.Y.; Shi, F.H.; Li, S.C.; Peng, A.M.; Zhang, G.L.; Song, X.L.; Wang, C.H. Serum mir-499 as a novel diagnostic and prognostic biomarker in non-small cell lung cancer. Oncol. Rep. 2014, 31, 1961–1967. [Google Scholar] [CrossRef]
- Huang, J.K.; Wu, J.J.; Li, Y.Q.; Li, X.; Yang, T.; Yang, Q.Y.; Jiang, Y.G. Deregulation of serum microrna expression is associated with cigarette smoking and lung cancer. BioMed Res. Int. 2014, 2014, 364316. [Google Scholar] [CrossRef]
- Geng, Q.; Fan, T.; Zhang, B.Y.; Wang, W.; Xu, Y.; Hu, H. Five micrornas in plasma as novel biomarkers for screening of early-stage non-small cell lung cancer. Respir. Res. 2014, 15, 149. [Google Scholar] [CrossRef]
- Gao, F.; Chang, J.X.; Wang, H.Q.; Zhang, G.J. Potential diagnostic value of mir-155 in serum from lung adenocarcinoma patients. Oncol. Rep. 2014, 31, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Tang, D.F.; Shen, Y.; Wang, M.Z.; Yang, R.H.; Wang, Z.Z.; Sui, A.H.; Jiao, W.J.; Wang, Y.J. Identification of plasma micrornas as novel noninvasive biomarkers for early detection of lung cancer. Eur. J. Cancer Prev. 2013, 22, 540–548. [Google Scholar] [CrossRef]
- Li, Z.H.; Zhang, H.; Yang, Z.G.; Wen, G.Q.; Cui, Y.B.; Shao, G.G. Prognostic significance of serum microrna-210 levels in nonsmall-cell lung cancer. J. Int. Med. Res. 2013, 41, 1437–1444. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Zhang, Q.Y. The expression and clinical significance of circulating microrna-21 in serum of five solid tumors. J. Cancer Res. Clin. Oncol. 2012, 138, 1659–1666. [Google Scholar] [CrossRef] [PubMed]
- Le, H.B.; Zhu, W.Y.; Chen, D.D.; He, J.Y.; Huang, Y.Y.; Liu, X.G.; Zhang, Y.K. Evaluation of dynamic change of serum mir-21 and mir-24 in pre- and post-operative lung carcinoma patients. Med. Oncol. 2012, 29, 3190–3197. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Hu, Z.B.; Wang, W.J.; Ba, Y.; Ma, L.J.; Zhang, C.N.; Wang, C.; Ren, Z.J.; Zhao, Y.; Wu, S.J.; et al. Identification of ten serum micrornas from a genome-wide serum microrna expression profile as novel noninvasive biomarkers for nonsmall cell lung cancer diagnosis. Int. J. Cancer 2012, 130, 1620–1628. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Liu, L.K.; Gao, W.; Zhu, C.J.; Liu, Y.Q.; Cheng, T.; Shu, Y.Q. Reduction of plasma microrna-21 is associated with chemotherapeutic response in patients with non-small cell lung cancer. Chin. J. Cancer Res. 2011, 23, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Gao, W.; Zhu, C.J.; Liu, Y.Q.; Mei, Z.; Cheng, T.; Shu, Y.Q. Identification of plasma microrna-21 as a biomarker for early detection and chemosensitivity of non-small cell lung cancer. Chin. J. Cancer 2011, 30, 407–414. [Google Scholar] [CrossRef] [PubMed]
- Yuan, P.; Gao, S.L. Management of breast cancer brain metastases: Focus on human epidermal growth factor receptor 2-positive breast cancer. Chronic Dis. Transl. Med. 2017, 3, 21–32. [Google Scholar] [CrossRef]
- Wang, H.Q.; Wu, S.N.; Zhao, L.; Zhao, J.; Liu, J.J.; Wang, Z.H. Clinical use of micrornas as potential non-invasive biomarkers for detecting non-small cell lung cancer: A meta-analysis. Respirology 2015, 20, 56–65. [Google Scholar] [CrossRef]
- Huang, Y.S.; Hu, Q.Y.; Deng, Z.H.; Hang, Y.L.; Wang, J.; Wang, K.Z. Micrornas in body fluids as biomarkers for non-small cell lung cancer: A systematic review. Technol. Cancer Res. Treat. 2014, 13, 277–287. [Google Scholar] [CrossRef]
- He, W.J.; Li, W.H.; Jiang, B.; Wang, Y.F.; Xia, Y.X.; Wang, L. Micrornas level as an initial screening method for early-stage lung cancer: A bivariate diagnostic random-effects meta-analysis. Int. J. Clin. Exp. Med. 2015, 8, 12317–12326. [Google Scholar]
- Chen, L.; Jin, H. Micrornas as novel biomarkers in the diagnosis of non-small cell lung cancer: A meta-analysis based on 20 studies. Tumor Biol. 2014, 35, 9119–9129. [Google Scholar] [CrossRef]
- Griffith, O.L.; Melck, A.; Jones, S.J.M.; Wiseman, S.M. Meta-analysis and meta-review of thyroid cancer gene expression profiling studies identifies important diagnostic biomarkers. J. Clin. Oncol. 2006, 24, 5043–5051. [Google Scholar] [CrossRef] [PubMed]
- Chan, S.K.; Griffith, O.L.; Tai, I.T.; Jones, S.J.M. Meta-analysis of colorectal cancer gene expression profiling studies identifies consistently reported candidate biomarkers. Cancer Epidemiol. Biomark. Prev. 2008, 17, 543–552. [Google Scholar] [CrossRef]
- Sharma, S.; Eghbali, M. Influence of sex differences on microrna gene regulation in disease. Biol. Sex Differ. 2014, 5, 3. [Google Scholar] [CrossRef] [PubMed]
- Hooten, N.N.; Fitzpatrick, M.; Wood, W.H.; De, S.; Ejiogu, N.; Zhang, Y.Q.; Mattison, J.A.; Becker, K.G.; Zonderman, A.B.; Evans, M.K. Age-related changes in microrna levels in serum. Aging 2013, 5, 725–740. [Google Scholar] [CrossRef] [PubMed]
- Oyetunji, S.O.; Xi, S.C.; Azoury, S.C.; Zhang, M.; Hong, J.; Inchauste, S.M.; Schrump, D. Cigarette smoke induces epigenetic dysregulation of microrna expression during esophageal adenocarcinogenesis. J. Am. Coll. Surg. 2014, 219, e68. [Google Scholar] [CrossRef]
- Takahashi, K.; Yokota, S.; Tatsumi, N.; Fukami, T.; Yokoi, T.; Nakajima, M. Cigarette smoking substantially alters plasma microrna profiles in healthy subjects. Toxicol. Appl. Pharmacol. 2013, 272, 154–160. [Google Scholar] [CrossRef]
- Olson, P.; Lu, J.; Zhang, H.; Shai, A.; Chun, M.G.; Wang, Y.C.; Libutti, S.K.; Nakakura, E.K.; Golub, T.R.; Hanahan, D. Microrna dynamics in the stages of tumorigenesis correlate with hallmark capabilities of cancer. Gene Dev. 2009, 23, 2152–2165. [Google Scholar] [CrossRef] [PubMed]
- Duttagupta, R.; Jiang, R.; Gollub, J.; Getts, R.C.; Jones, K.W. Impact of cellular mirnas on circulating mirna biomarker signatures. PLoS ONE 2011, 6, e20769. [Google Scholar] [CrossRef] [PubMed]
- McDonald, J.S.; Milosevic, D.; Reddi, H.V.; Grebe, S.K.; Algeciras-Schimnich, A. Analysis of circulating microrna: Preanalytical and analytical challenges. Clin. Chem. 2011, 57, 833–840. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, C.C.; Kroh, E.; Wood, B.; Arroyo, J.D.; Dougherty, K.J.; Miyaji, M.M.; Tait, J.F.; Tewari, M. Blood cell origin of circulating micrornas: A cautionary note for cancer biomarker studies. Cancer Prev. Res. 2012, 5, 492–497. [Google Scholar] [CrossRef]
- Zheng, X.H.; Cui, C.; Zhou, X.X.; Zeng, Y.X.; Jia, W.H. Centrifugation: An important pre-analytic procedure that influences plasma microrna quantification during blood processing. Chin. J. Cancer 2013, 32, 667–672. [Google Scholar] [CrossRef] [PubMed]
- Becker, N.; Lockwood, C.M. Pre-analytical variables in mirna analysis. Clin. Biochem. 2013, 46, 861–868. [Google Scholar] [CrossRef]
- Kirschner, M.B.; Kao, S.C.; Edelman, J.J.; Armstrong, N.J.; Vallely, M.P.; van Zandwijk, N.; Reid, G. Haemolysis during sample preparation alters microrna content of plasma. PLoS ONE 2011, 6, e24145. [Google Scholar] [CrossRef] [PubMed]
- Mensah, M.; Borzi, C.; Verri, C.; Suatoni, P.; Conte, D.; Pastorino, U.; Orazio, F.; Sozzi, G.; Boeri, M. Microrna based liquid biopsy: The experience of the plasma mirna signature classifier (msc) for lung cancer screening. J. Vis. Exp. 2017. [Google Scholar] [CrossRef] [PubMed]
- El-Khoury, V.; Pierson, S.; Kaoma, T.; Bernardin, F.; Berchem, G. Assessing cellular and circulating mirna recovery: The impact of the rna isolation method and the quantity of input material. Sci. Rep. 2016, 6, 19529. [Google Scholar] [CrossRef]
- Rice, J.; Roberts, H.; Burton, J.; Pan, J.; States, V.; Rai, S.N.; Galandiuk, S. Assay reproducibility in clinical studies of plasma mirna. PLoS ONE 2015, 10, e0121948. [Google Scholar] [CrossRef]
- Appaiah, H.N.; Goswami, C.P.; Mina, L.A.; Badve, S.; Sledge, G.W.; Liu, Y.L.; Nakshatri, H. Persistent upregulation of u6:Snord44 small rna ratio in the serum of breast cancer patients. Breast Cancer Res. 2011, 13, R86. [Google Scholar] [CrossRef]
- Chen, X.; Ba, Y.; Ma, L.J.; Cai, X.; Yin, Y.; Wang, K.H.; Guo, J.G.; Zhang, Y.J.; Chen, J.N.; Guo, X.; et al. Characterization of micrornas in serum: A novel class of biomarkers for diagnosis of cancer and other diseases. Cell Res. 2008, 18, 997–1006. [Google Scholar] [CrossRef]
- Boeri, M.; Verri, C.; Conte, D.; Roz, L.; Modena, P.; Facchinetti, F.; Calabro, E.; Croce, C.M.; Pastorino, U.; Sozzi, G. Microrna signatures in tissues and plasma predict development and prognosis of computed tomography detected lung cancer. Proc. Natl. Acad. Sci. USA 2011, 108, 3713–3718. [Google Scholar] [CrossRef]
- Hennessey, P.T.; Sanford, T.; Choudhary, A.; Mydlarz, W.W.; Brown, D.; Adai, A.T.; Ochs, M.F.; Ahrendt, S.A.; Mambo, E.; Califano, J.A. Serum microrna biomarkers for detection of non-small cell lung cancer. PLoS ONE 2012, 7, e32307. [Google Scholar] [CrossRef]
- Sozzi, G.; Boeri, M.; Rossi, M.; Verri, C.; Suatoni, P.; Bravi, F.; Roz, L.; Conte, D.; Grassi, M.; Sverzellati, N.; et al. Clinical utility of a plasma-based mirna signature classifier within computed tomography lung cancer screening: A correlative mild trial study. J. Clin. Oncol. 2014, 32, 768–773. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, P.S.; Parkin, R.K.; Kroh, E.M.; Fritz, B.R.; Wyman, S.K.; Pogosova-Agadjanyan, E.L.; Peterson, A.; Noteboom, J.; O’Briant, K.C.; Allen, A.; et al. Circulating micrornas as stable blood-based markers for cancer detection. Proc. Natl. Acad. Sci. USA 2008, 105, 10513–10518. [Google Scholar] [CrossRef]
- Balzano, F.; Deiana, M.; Dei Giudici, S.; Oggiano, A.; Baralla, A.; Pasella, S.; Mannu, A.; Pescatori, M.; Porcu, B.; Fanciulli, G.; et al. Mirna stability in frozen plasma samples. Molecules 2015, 20, 19030–19040. [Google Scholar] [CrossRef] [PubMed]
- Kroh, E.M.; Parkin, R.K.; Mitchell, P.S.; Tewari, M. Analysis of circulating microrna biomarkers in plasma and serum using quantitative reverse transcription-pcr (qrt-pcr). Methods 2010, 50, 298–301. [Google Scholar] [CrossRef]
- Keller, A.; Leidinger, P.; Gislefoss, R.; Haugen, A.; Langseth, H.; Staehler, P.; Lenhof, H.P.; Meese, E. Stable serum mirna profiles as potential tool for non-invasive lung cancer diagnosis. RNA Biol. 2011, 8, 506–516. [Google Scholar] [CrossRef] [PubMed]
- Hoseok, I.; Cho, J.Y. Lung cancer biomarkers. Adv. Clin. Chem. 2015, 72, 107–170. [Google Scholar]
- Sanfiorenzo, C.; Ilie, M.I.; Belaid, A.; Barlesi, F.; Mouroux, J.; Marquette, C.H.; Brest, P.; Hofman, P. Two panels of plasma micrornas as non-invasive biomarkers for prediction of recurrence in resectable nsclc. PLoS ONE 2013, 8, e54596. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Schottker, B.; Ordonez-Mena, J.; Holleczek, B.; Yang, R.X.; Burwinkel, B.; Butterbach, K.; Brenner, H. F2rl3 methylation, lung cancer incidence and mortality. Int. J. Cancer 2015, 137, 1739–1748. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study a | Cases vs. Controls | Specimen | Histology | Stage | miRNA | SEN | SPE | AUC | p-Value | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Number | Age (y) | Male (%) | |||||||||
| Zhao, 2018 [14] b | 108/54 | / | 61/NA | serum | NSCLC | I–IV | miR-141 | / | / | 0.86 | <0.001 c |
| Sun, 2018 [15] b | 196/77 | / | 58/NA | serum | NSCLC | I–IV | miR-770 | 68 | 89 | 0.84 | <0.01 c |
| Shan, 2018 [16] b | 102/101 | / | 100/100 | plasma | SCC | I–III | miR-181a-5p | / | / | 0.73 | <0.001 c |
| miR-21-5p | / | / | 0.74 | <0.001 c | |||||||
| miR-106a-5p | / | / | 0.74 | <0.001 c | |||||||
| miR-93-5p | / | / | 0.69 | <0.001 c | |||||||
| Qin, 2018 [17] | 146/40 | 63/NA | 73/NA | serum | NSCLC | I–IV | miR-342-3p | 60 | 94 | 0.89 | <0.01 c |
| 78/40 | / | / | SCC | miR-342-3p | 83 | 76 | 0.87 | <0.01 c | |||
| 68/40 | / | / | ADC | miR-342-3p | 83 | 82 | 0.90 | <0.01 c | |||
| Bao, 2018 [18] b | 80/75 | / | 61/60 | serum | NSCLC | I–IV | miR-10a-5p | 66 | 73 | 0.71 | <0.0001 c |
| miR-196a-5p | 68 | 78 | 0.79 | 0.0018 c | |||||||
| Zhang, 2017 [20] b | 102/108 | / | 100/100 | Serum | SCC | I–III | miR-106a-5p | / | / | 0.83 | <0.001 c |
| miR-20a-5p | / | / | 0.80 | <0.001 c | |||||||
| miR-93-5p | / | / | 0.82 | <0.001 c | |||||||
| Wang, 2017 [24] | 127/60 | 58/59 | 62/58 | serum | NSCLC | I–IV | miR-98 | 80 | 82 | 0.86 | <0.01 c |
| Zhou, 2017 [19] b | 108/94 | / | 43/46 | plasma | ADC | I–IV | miR-19b-3p | / | / | 0.62 | <0.001 c |
| miR-21-5p | / | / | 0.69 | <0.001 c | |||||||
| miR-221-3p | / | / | 0.68 | <0.001 c | |||||||
| miR-409-3p | / | / | 0.61 | <0.001 c | |||||||
| miR-425-5p | / | / | 0.66 | <0.001 c | |||||||
| miR-584-5p | / | / | 0.69 | <0.001 c | |||||||
| Zhang, 2017 [21] | 129/83 | 60/60 | 63/58 | plasma | NSCLC | I–II | miR-145 | 81 | 89 | 0.89 | <0.0001 c |
| miR-20a | 80 | 88 | 0.89 | <0.0001 c | |||||||
| miR-21 | 78 | 86 | 0.84 | <0.001 c | |||||||
| miR-223 | 70 | 84 | 0.81 | <0.001 c | |||||||
| Yu, 2017 [22] b | 50/30 | / | 82/83 | plasma | SCLC | I–IV | miR-92a-2-5p | 56 | 100 | 0.76 | <0.001 c |
| Yang, 2017 [23] b | 113/30 | / | 52/NA | serum | ADC | I–IV | miR-31 | / | / | 0.84 | <0.01 c |
| Shang, 2017 [25] | 127/112 | 55/44 | 65/56 | serum | NSCLC | I–IV | miR-22 | 99 | 84 | 0.92 | <0.001 |
| miR-126 | 83 | 96 | 0.87 | <0.001 | |||||||
| Lv, 2017 [26] | 120/120 | 60/59 | 52/51 | serum | ADC | I–IV | miR-103 | / | / | 0.80 | <0.0001 c |
| miR-146a | / | / | 0.90 | <0.0001 c | |||||||
| miR-151 | / | / | 0.85 | <0.0001 c | |||||||
| miR-221 | / | / | 0.79 | <0.0001 c | |||||||
| miR-222 | / | / | 0.86 | <0.0001 c | |||||||
| miR-223 | / | / | 0.91 | <0.0001 c | |||||||
| Zhu, 2016 [9] | 112/40 | 59/58 | 54/55 | serum | NSCLC | 0–IIIB | miR-182 | 63 | 80 | 0.73 | <0.0001 |
| miR-183 | 41 | 83 | 0.63 | 0.0091 | |||||||
| miR-210 | 34 | 100 | 0.62 | 0.0121 | |||||||
| miR-126 | 61 | 93 | 0.79 | <0.0001 | |||||||
| Wang, 2016 [27] | 82/91 | / | / | plasma | ADC | I–II | miR-628-3p | 43 | 91 | 0.73 | <0.001 c |
| miR-339-3p | 65 | 71 | 0.72 | <0.001 c | |||||||
| miR-425-3p | 67 | 68 | 0.73 | <0.001 c | |||||||
| miR-532 | 54 | 80 | 0.66 | <0.001 c | |||||||
| Wang, 2016 [28] | 54/15 | 60/51 | / | serum | NSCLC | I–IV | miR-1244 | 82 | 80 | 0.83 | / |
| 26/15 | NA/51 | / | ADC | miR-1244 | 77 | 80 | 0.79 | <0.05 c | |||
| 18/15 | NA/51 | / | SCC | miR-1244 | 83 | 80 | 0.85 | <0.05 c | |||
| Sun, 2016 [30] | 50/60 | 67/62 | 76/78 | serum | NSCLC | I–IV | miR-21 | / | / | 0.87 | 0.000 |
| Su, 2016 [32] b | 100/100 | / | 65/70 | plasma | NSCLC | I–III | miR-195 | 78 | 86 | 0.89 | <0.01 c |
| Peng, 2016 [32] | 120/71 | 60/58 | 72/62 | serum | NSCLC | I–IV | miR-1254 | 97 | 39 | 0.68 | 0.000 |
| miR-485-5p | 95 | 63 | 0.79 | 0.000 | |||||||
| miR-574-5p | 99 | 28 | 0.64 | 0.002 | |||||||
| Gao, 2016 [10] | 90/90 | 62/62 | 80/78 | plasma | SCC | I | miR-324-3p | 72 | 76 | 0.79 | / |
| miR-1285 | 87 | 78 | 0.85 | / | |||||||
| Fan, 2016 [33] d | 94/58 | 60/58 | 54/53 | serum | NSCLC | I–IIIB | miR-15b-5p | 52 | 74 | / | 0.006 c |
| miR-16-5p | 88 | 86 | / | 0.0001 c | |||||||
| miR-17-5p | 82 | 68 | / | 0.0001 c | |||||||
| miR-19-3p | 83 | 67 | / | 0.0001 c | |||||||
| miR-20a-5p | 76 | 90 | / | 0.0001 c | |||||||
| miR-28-3p | 71 | 79 | / | 0.0001 c | |||||||
| miR-92a-3p | 87 | 66 | / | 0.0001 c | |||||||
| Zhou, 2015 [34] | 87/61 | 59/56 | 63/52 | serum | NSCLC | I–IV | miR-194 | / | / | 0.66 | / |
| miR-652 | / | / | 0.82 | / | |||||||
| miR-660 | / | / | 0.71 | / | |||||||
| 52/61 | NA/56 | NA/52 | ADC | miR-194 | / | / | 0.63 | 0.0192 c | |||
| miR-652 | / | / | 0.82 | <0.0001 c | |||||||
| miR-660 | / | / | 0.72 | <0.0001 c | |||||||
| 35/61 | NA/56 | NA/52 | SCC | miR-194 | / | / | 0.70 | 0.0007 c | |||
| miR-652 | / | / | 0.81 | <0.0001 c | |||||||
| miR-660 | / | / | 0.70 | 0.0003 c | |||||||
| Zhao, 2015 [35] | 80/60 | 58/55 | 61/52 | serum | NSCLC | / | miR-21 | 74 | 72 | 0.81 | 0.001 c |
| Yang, 2015 [36] b | 152/300 | / | 65/69 | serum | NSCLC | I–IV | miR-148a | 85 | 83 | 0.90 | <0.001 c |
| miR-148b | 83 | 83 | 0.90 | <0.001 c | |||||||
| miR-152 | 75 | 77 | 0.82 | <0.001 c | |||||||
| miR-21 | 69 | 71 | 0.81 | <0.001 c | |||||||
| Yan, 2015 [37] b | 300/300 | / | / | plasma | Any LC | I–IV | miR-31 | 77 | 75 | 0.79 | <0.001 c |
| Wang, 2015 [38] | 70/70 | 64/64 | 61/61 | serum | NSCLC | / | miR-125a-5p | 74 | 56 | 0.71 | <0.0001 c |
| miR-145 | 93 | 61 | 0.84 | <0.0001 c | |||||||
| miR-146a | 84 | 59 | 0.78 | <0.0001 c | |||||||
| Wang, 2015 [39] | 94/111 | NA/60 | NA/52 | serum | NSCLC | IA–IIB | miR-125a-5p | 88 | 75 | 0.83 | / |
| miR-25 | 83 | 75 | 0.82 | / | |||||||
| miR-126 | 83 | 63 | 0.79 | / | |||||||
| Wang, 2015 [40] e | 63/63 | 62/60 | 78/59 | serum | NSCLC | I–IV | miR-483-5p | / | / | 0.66 | 0.002 |
| miR-193a-3p | / | / | 0.81 | <0.0001 | |||||||
| miR-214 | / | / | 0.78 | <0.0001 | |||||||
| miR-25 | / | / | 0.84 | <0.0001 | |||||||
| miR-7 | / | / | 0.81 | <0.0001 | |||||||
| Li, 2015 [41] | 11/11 | 59/55 | 64/55 | plasma | NSCLC | I–IIIA | miR-486 | 91 | 82 | 0.93 | 0.0008 c |
| miR-150 | 82 | 82 | 0.75 | 0.0488 c | |||||||
| Guo, 2015 [42] b | 126/50 | / | 64/NA | plasma | NSCLC | I–IV | miR-204 | 76 | 82 | 0.81 | <0.001 c |
| Dou, 2015 [43] | 120/360 | 63/NA | 60/NA | plasma | NSCLC | I–IV | let-7c | 72 | 78 | 0.71 | 0.006 |
| miR-152 | 86 | 81 | 0.85 | 0.0002 | |||||||
| Zhu, 2014 [44] | 36/44 | / | / | serum | NSCLC | I | miR-125a-5p | 54 | 75 | 0.65 | 0.021 |
| let-7e | 50 | 83 | 0.64 | 0.0317 | |||||||
| Zhu, 2014 [45] | 70/48 | 59/NA | 80/NA | serum | NSCLC | I–IV | miR-29c | 66 | 74 | 0.68 | 0.0004 |
| miR-429 | 54 | 81 | 0.71 | <0.0001 | |||||||
| Li, 2014 [46] b | 514/54 | / | 53/NA | serum | NSCLC | I–IV | miR-499 | 74 | 93 | 0.91 | <0.001 c |
| Huang, 2014 [47] | 53/65 | 57/55 | / | serum | NSCLC | / | let-7i-3p | / | / | 0.89 | <0.001 c |
| miR-154-5p | / | / | 0.96 | <0.001 c | |||||||
| Geng, 2014 [48] b | 126/60 | / | 69/60 | plasma | NSCLC | I–II | miR-20a | 83 | 81 | 0.89 | <0.001 c |
| miR-223 | 87 | 86 | 0.94 | <0.001 c | |||||||
| miR-21 | 67 | 68 | 0.77 | <0.001 c | |||||||
| miR-155 | 86 | 84 | 0.92 | <0.001 c | |||||||
| miR-145 | 70 | 68 | 0.77 | <0.001 c | |||||||
| 45/60 | / | / | ADC | I–II | miR-20a | 87 | 83 | 0.90 | / | ||
| miR-223 | 80 | 82 | 0.91 | / | |||||||
| miR-21 | 60 | 60 | 0.63 | / | |||||||
| miR-155 | 87 | 87 | 0.93 | / | |||||||
| miR-145 | 71 | 70 | 0.77 | / | |||||||
| 64/60 | / | / | SCC | I–II | miR-20a | 97 | 97 | 0.98 | / | ||
| miR-223 | 95 | 93 | 0.98 | / | |||||||
| miR-21 | 91 | 90 | 0.97 | / | |||||||
| miR-155 | 92 | 90 | 0.96 | / | |||||||
| miR-145 | 95 | 95 | 0.97 | / | |||||||
| Gao, 2014 [49] | 36/32 | 55/53 | 31/31 | serum | ADC | I–IV | miR-155 | 72 | 69 | 0.76 | 0.000 |
| Tang, 2013 [50] | 34/32 | 65/66 | 65/81 | plasma | NSCLC | I–III | miR-21 | 53 | 72 | 0.71 | / |
| miR-145 | 56 | 56 | 0.66 | / | |||||||
| miR-155 | 68 | 66 | 0.74 | / | |||||||
| Li, 2013 [51] | 60/30 | 54/57 | 70/50 | serum | NSCLC | I–IV | miR-210 | 79 | 74 | 0.78 | <0.005 c |
| Wang, 2012 [52] | 31/39 | 61/46 | 71/23 | serum | Any LC | I–IV | miR-21 | 87 | 74 | 0.88 | <0.001 c |
| Le, 2012 [53] | 82/50 | 59/NA | 56/NA | serum | NSCLC | I–IV | miR-21 | 46 | 92 | 0.69 | 0.0058 c |
| miR-205 | 85 | 72 | 0.78 | 0.0298 c | |||||||
| miR-30d | 76 | 80 | 0.74 | 0.0147 c | |||||||
| miR-24 | 76 | 64 | 0.83 | <0.0001 c | |||||||
| Wei, 2011 [55] | 77/36 | 60/56 | 71/75 | plasma | NSCLC | I–IV | miR-21 | 61 | 83 | 0.73 | <0.0001 |
| Wei, 2011 [56] | 63/30 | 61/57 | 71/67 | plasma | NSCLC | I–IV | miR-21 | 76 | 70 | 0.78 | <0.0001 |
| Study a | Cases vs. Controls | Specimen | Histology | Stage | miRNA | SEN | SPE | AUC | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Number | Age (y) | Male (%) | ||||||||
| Shan, 2018 [16] b | 15/15 | / | 100/100 | plasma | SCC | I–III | Panel A | / | / | 0.91 |
| Zhang, 2017 [20] b | 34/36 | / | 100/100 | serum | SCC | I–III | Panel B | / | / | 0.95 |
| Zhou, 2017 [19] b | 33/30 | / | 45/47 | plasma | ADC | I–IV | Panel C | 73 | 80 | 0.84 |
| Zhang, 2017 [21] | 129/83 | 60/60 | 63/58 | plasma | NSCLC | I–II | Panel D | 82 | 90 | 0.90 |
| LV, 2017 [26] | 120/120 | 60/59 | 52/51 | serum | ADC | I–IV | Panel E | 84 | 91 | 0.95 |
| 72/120 | NA/59 | NA/51 | I | / | / | 0.94 | ||||
| 31/120 | NA/59 | NA/51 | II | / | / | 0.97 | ||||
| 10/120 | NA/59 | NA/51 | III | / | / | 0.95 | ||||
| Jin, 2017 [8] | 47/13 | / | / | exosome | NSCLC | I | Panel F | 80 | 92 | 0.90 |
| Wang, 2016 [27] | 82/91 | / | / | plasma | ADC | I–II | Panel G | 90 | 99 | 0.98 |
| Panel H | 92 | 98 | 0.97 | |||||||
| Tai, 2016 [29] | 110/52 | 65/66 | 56/58 | serum | ADC | I–III | Panel I | 89 | 100 | 0.98 |
| Gao, 2016 [10] | 90/90 | 62/62 | 80/78 | plasma | SCC | I | -324-3p, -1285 | 85 | 82 | 0.89 |
| Fan, 2016 [33] c | 70/54 | 60/58 | 60/54 | serum | NSCLC | I–IIIB | Panel J | 94 | 94 | / |
| Zhou, 2015 [34] | 87/61 | 59/56 | 63/52 | serum | NSCLC | I–IV | -652, -660 | / | / | 0.86 |
| 52/61 | NA/56 | NA/52 | ADC | -652, -660 | / | / | 0.85 | |||
| 35/61 | NA/56 | NA/52 | SCC | -652, -660 | / | / | 0.87 | |||
| Yang, 2015 [36] b | 152/300 | / | 65/69 | serum | NSCLC | I–IV | Panel K | 96 | 91 | 0.98 |
| Wang, 2015 [39] | 142/111 | 61/60 | 61/52 | serum | NSCLC | IA–IV | Panel L | 88 | 83 | 0.93 |
| Wang, 2015 [40] d | 63/63 | 62/60 | 78/59 | serum | NSCLC | I–IV | Panel M | 89 | 68 | 0.82 |
| Tang, 2013 [50] | 34/32 | 65/66 | 65/81 | plasma | NSCLC | I–III | -21, -145 | 74 | 81 | 0.85 |
| -21, -145 | 56 | 66 | 0.73 | |||||||
| -145, -155 | 79 | 78 | 0.83 | |||||||
| Panel N | 77 | 81 | 0.87 | |||||||
| 40/60 | NA/66 | NA/77 | ADC | I–III | Panel N | 71 | 78 | / | ||
| 9/60 | NA/66 | NA/77 | SCC | I–III | Panel N | 67 | 78 | / | ||
| Chen, 2012 [54] | 200/110 | 60/59 | 79/72 | serum | NSCLC | I–IV | Panel O | 93 | 90 | 0.97 |
| Study | miR-21 | miR-145 | miR-20a | miR-24 | miR-223 | miR-155 | miR-25 | miR-152 | miR-125a | miR-126 | miR-221 | miR-93 | miR-210 | miR-486 | miR-425 | miR-19b | miR-22 | let-7e | miR-146a | miR-222 | miR-31 | miR-106a |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Shan, 2018 [16] | ○↑ | ○↑ | ○↑ | |||||||||||||||||||
| Zhang, 2017 [20] | ○↑ | ○↑ | ○↑ | |||||||||||||||||||
| Zhou, 2017 [19] | ○↑ | ○↑ | ○↑ | |||||||||||||||||||
| Zhang, 2017 [21] | ○↑ | ○↑ | ○↑ | ○↑ | ||||||||||||||||||
| Yu, 2017 [22] | ||||||||||||||||||||||
| Yang, 2017 [23] | △↑ | |||||||||||||||||||||
| Shang, 2017 [25] | △↓ | △↑ | ||||||||||||||||||||
| Lv, 2017 [26] | ○↑ | △↑ | ○↑ | ○↑ | ||||||||||||||||||
| Jin, 2017 [8] | ○↓ | ○↑ | ○↓ | |||||||||||||||||||
| Zhu, 2016 [9] | △↓ | △↑ | ||||||||||||||||||||
| Wang, 2016 [27] | ○↑ | |||||||||||||||||||||
| Tai, 2016 [29] | ○ | ○ | ○ | ○ | ○ | ○ | ||||||||||||||||
| Sun, 2016 [30] | △↑ | |||||||||||||||||||||
| Fan, 2016 [33] | ○↓ | |||||||||||||||||||||
| Zhao, 2015 [35] | △↑ | |||||||||||||||||||||
| Yang, 2015 [36] | ○↑ | ○↓ | ||||||||||||||||||||
| Yan, 2015 [37] | △↑ | |||||||||||||||||||||
| Wang, 2015 [38] | △↑ | △↑ | △↑ | |||||||||||||||||||
| Wang, 2015 [39] | ○↓ | ○↓ | ○↓ | |||||||||||||||||||
| Wang, 2015 [40] | ○↑ | |||||||||||||||||||||
| Li, 2015 [41] | △↑ | |||||||||||||||||||||
| Dou, 2015 [43] | △↓ | |||||||||||||||||||||
| Zhu, 2014 [44] | △↓ | △↓ | ||||||||||||||||||||
| Geng, 2014 [48] | △↑ | △↑ | △↑ | △↑ | △↑ | |||||||||||||||||
| Gao, 2014 [49] | △↑ | |||||||||||||||||||||
| Tang, 2013 [50] | ○↑ | ○↓ | ○↑ | |||||||||||||||||||
| Li, 2013 [51] | △↑ | |||||||||||||||||||||
| Wang, 2012 [52] | △↑ | |||||||||||||||||||||
| Le, 2012 [53] | △↑ | △↑ | ||||||||||||||||||||
| Chen, 2012 [54] | ○↑ | ○↑ | ○↑ | ○↑ | ○↑ | ○↑ | ○↑ | ○↑ | ||||||||||||||
| Wei, 2011 [55] | △↑ | |||||||||||||||||||||
| Wei, 2011 [56] | △↑ | |||||||||||||||||||||
| Total | 13 | 5 | 5 | 4 | 4 | 3 | 3 | 3 | 3 | 3 | 3 | 3 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yu, H.; Guan, Z.; Cuk, K.; Zhang, Y.; Brenner, H. Circulating MicroRNA Biomarkers for Lung Cancer Detection in East Asian Populations. Cancers 2019, 11, 415. https://doi.org/10.3390/cancers11030415
Yu H, Guan Z, Cuk K, Zhang Y, Brenner H. Circulating MicroRNA Biomarkers for Lung Cancer Detection in East Asian Populations. Cancers. 2019; 11(3):415. https://doi.org/10.3390/cancers11030415
Chicago/Turabian StyleYu, Haixin, Zhong Guan, Katarina Cuk, Yan Zhang, and Hermann Brenner. 2019. "Circulating MicroRNA Biomarkers for Lung Cancer Detection in East Asian Populations" Cancers 11, no. 3: 415. https://doi.org/10.3390/cancers11030415