Oxaliplatin-Based Intra-arterial Chemotherapy in Colo-Rectal Cancer Liver Metastases: A Review from Pharmacology to Clinical Application

Abstract
:1. Introduction
2. Chemotherapy in Hepatic Arterial Infusion (HAI)
3. Chemotherapic Drugs in HAI
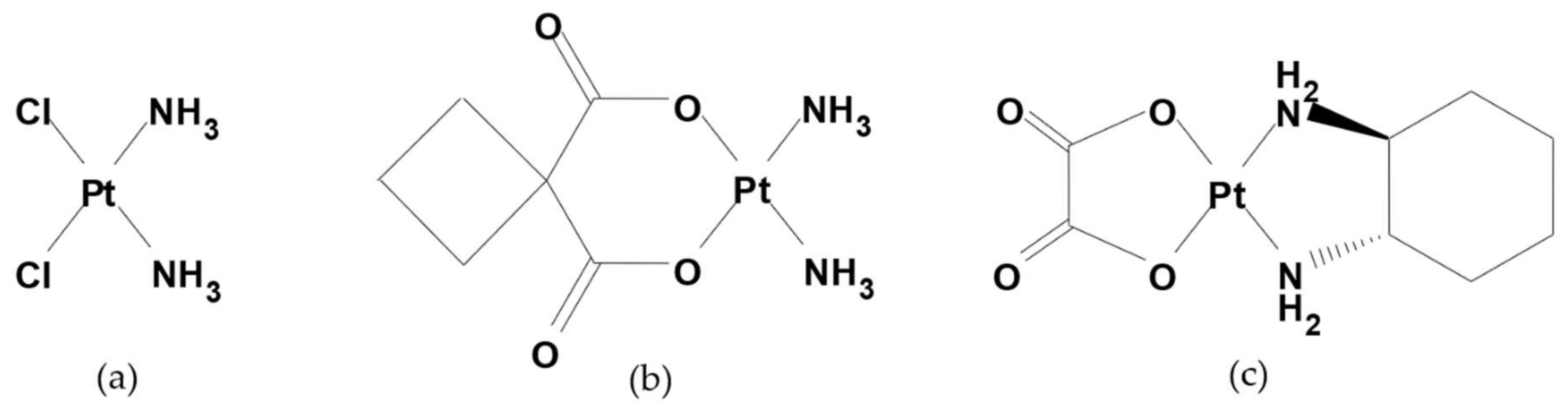
4. Oxaliplatin Chemistry and Pharmaceutical Properties
5. Oxaliplatin Pharmacology and Pharmacokinetics
6. Toxicity in HAI Chemotherapy
7. Clinical Trials with HAI Oxaliplatin
8. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Muggia, F.M.; Bonetti, A.; Hoeschele, J.D.; Rozencweig, M.; Howell, S.B. Platinum Antitumor Complexes: 50 Years Since Barnett Rosenberg’s Discovery. J. Clin. Oncol. 2015, 33, 4219–4226. [Google Scholar] [CrossRef] [PubMed]
- Rose, W.C.; Schurig, J.E. Preclinical antitumor and toxicologic profile of carboplatin. Cancer Treat. Rev. 1985, 12 (Suppl. A), 1–19. [Google Scholar] [CrossRef]
- Sasanelli, R.; Boccarelli, A.; Giordano, D.; Laforgia, M.; Arnesano, F.; Natile, G.; Cardellicchio, C.; Capozzi, M.A.; Coluccia, M. Platinum complexes can inhibit matrix metalloproteinase activity: Platinum diethyl[(methylsulfinyl)methyl]phosphonate complexes as inhibitors of matrix metalloproteinases 2, 3, 9, and 12. J. Med. Chem. 2007, 50, 3434–3441. [Google Scholar] [CrossRef] [PubMed]
- Extra, J.M.; Marty, M.; Brienza, S.; Misset, J.L. Pharmacokinetics and safety profile of oxaliplatin. Semin. Oncol. 1998, 25 (Suppl. 5), 13–22. [Google Scholar]
- Choi, E.; Lee, S.; Nhung, B.C.; Suh, M.; Park, B.; Jun, J.K.; Choi, K.S. Cancer mortality-to-incidence ratio as an indicator of cancer management outcomes in Organization for Economic Cooperation and Development countries. Epidemiol. Health 2017, 39, e2017006. [Google Scholar] [CrossRef] [PubMed]
- Misiakos, E.P.; Karidis, N.P.; Kouraklis, G. Current treatment for colorectal liver metastases. World J. Gastroenterol. 2011, 17, 4067–4075. [Google Scholar] [CrossRef] [PubMed]
- Tsalis, K.; Ioannidis, O.; Cheva, A.; Antigoni, N.S.; Antoniou, N.; Parpoudi, S.; Kyziridis, D.; Tatsis, D.; Konstantaras, D.; Kitsikosta, L.; et al. A 20-year single center experience in the surgical treatment of colorectal liver metastasis. J. BUON 2018, 23, 1640–1647. [Google Scholar]
- Adam, R.; DeGramont, A.; Figueras, J.; Guthrie, A.; Kokudo, N.; Kunstlinger, F.; Loyer, E.; Poston, G.; Rougier, P.; Rubbia-Brandt, L.; et al. The oncosurgery approach to managing liver metastases from colorectal cancer: A multidisciplinary international consensus. Oncologist 2012, 17. [Google Scholar] [CrossRef]
- Dhir, M.; Sasson, A.R. Surgical Management of Liver Metastases from Colorectal Cancer. J. Oncol. Pract. 2016, 12, 1–39. [Google Scholar] [CrossRef]
- Gallinger, S.; Biagi, J.J.; Fletcher, G.G.; Nhan, C.; Ruo, L.; McLeod, R.S. Liver resection for colorectal cancer metastases. Curr. Oncol. 2013, 20, 255–265. [Google Scholar] [CrossRef]
- Mehrvarz Sarshekeh, A.; Overman, M.J.; Kopetz, S. Nivolumab in the treatment of microsatellite instability high metastatic colorectal cancer. Future Oncol. 2018, 14, 1869–1874. [Google Scholar] [CrossRef] [PubMed]
- Gadaleta, C.D.; Ranieri, G. Trans-arterial chemoembolization as a therapy for liver tumours: New clinical developments and suggestions for combination with angiogenesis inhibitors. Crit. Rev. Oncol. Hematol. 2011, 80, 40–53. [Google Scholar] [CrossRef] [PubMed]
- Rocha, F.G.; Helton, W.S. Resectability of colorectal liver metastases: An evolving definition. HPB 2012, 14, 283–284. [Google Scholar] [CrossRef] [PubMed]
- Breedis, C.; Young, G. The blood supply of neoplasms in the liver. Am. J. Pathol. 1954, 30, 969–977. [Google Scholar] [PubMed]
- Bierman, H.R.; Byron, R.L.; Kelley, K.H.; Grady, A. Studies on the blood supply of tumors in man. III. Vascular patterns of the liver by hepatic arteriography in vivo. J. Natl. Cancer Inst. 1951, 12, 107–131. [Google Scholar] [PubMed]
- Kemeny, N.; Fata, F. Hepatic-arterial chemotherapy. Lancet Oncol. 2001, 2, 418–428. [Google Scholar] [CrossRef]
- Buchwald, H.; Grage, T.B.; Vassilopoulos, P.P.; Rohde, T.D.; Varco, R.L.; Blackshear, P.J. Intraarterial infusion chemotherapy for hepatic carcinoma using a totally implantable infusion pump. Cancer 1980, 45, 866–869. [Google Scholar] [CrossRef] [Green Version]
- Skitzki, J.J.; Chang, A.E. Hepatic artery chemotherapy for colorectal liver metastases: Technical considerations and review of clinical trials. Surg. Oncol. 2002, 11, 123–135. [Google Scholar] [CrossRef]
- Ranieri, G.; Marech, I.; Porcelli, M.; Giotta, F.; Palmiotti, G.; Laricchia, G.; Fazio, V.; Gadaleta, C.D. Complete response in a patient with liver metastases from breast cancer employing hepatic arterial infusion 5-fluorouracil based chemotherapy plus systemic nab-paclitaxel. Oncotarget 2017, 9, 8197–8203. [Google Scholar] [CrossRef]
- Hildebrandt, B.; Pech, M.; Nicolaou, A.; Langrehr, J.M.; Kurcz, J.; Bartels, B.; Miersch, A.; Felix, R.; Neuhaus, P.; Riess, H.; et al. Interventionally implanted port catheter systems for hepatic arterial infusion of chemotherapy in patients with colorectal liver metastases: A phase II—Study and historical comparison with the surgical approach. BMC Cancer 2007, 7, 69. [Google Scholar] [CrossRef]
- Deschamps, F.; Elias, D.; Goere, D.; Malka, D.; Ducreux, M.; Boige, V.; Auperin, A.; de Baere, T. Intra-arterial hepatic chemotherapy: A comparison of percutaneous versus surgical implantation of port-catheters. Cardiovasc. Intervent. Radiol. 2011, 34, 973–979. [Google Scholar] [CrossRef] [PubMed]
- Doussot, A.; Kemeny, N.E.; D’Angelica, M.I. Hepatic arterial infusional chemotherapy in the management of colorectal cancer liver metastases. Hepatol. Oncol. 2015, 2, 275–290. [Google Scholar] [CrossRef] [PubMed]
- Chapelle, N.; Matysiak-Budnik, T.; Douane, F.; Metairie, S.; Rougier, P.; Touchefeu, Y. Hepatic arterial infusion in the management of colorectal cancer liver metastasis: Current and future perspectives. Dig. Liver Dis. 2018, 50, 220–225. [Google Scholar] [CrossRef] [PubMed]
- Karanicolas, P.J.; Metrakos, P.; Chan, K.; Asmis, T.; Chen, E.; Kingham, T.P.; Kemeny, N.; Porter, G.; Fields, R.C.; Pingpank, J.; et al. Hepatic arterial infusion pump chemotherapy in the management of colorectal liver metastases: Expert consensus statement. Curr. Oncol. 2014, 21, e129. [Google Scholar] [CrossRef] [PubMed]
- Ensminger, W.D.; Gyves, J.W. Clinical pharmacology of hepatic arterial chemotherapy. Semin. Oncol. 1983, 10, 176–182. [Google Scholar] [PubMed]
- Kemeny, N.; Daly, J. Preliminary results of a randomized study of intrahepatic infusion versus systemic infusion of 5-fluoro-2′-deoxyuridine for metastatic colorectal carcinoma. Recent Results Cancer Res. 1986, 100, 171–178. [Google Scholar] [PubMed]
- D’Angelica, M.I.; Correa-Gallego, C.; Paty, P.B.; Cercek, A.; Gewirtz, A.N.; Chou, J.F.; Capanu, M.; Kingham, T.P.; Fong, Y.; De Matteo, R.P.; et al. Phase II trial of hepatic artery infusional and systemic chemotherapy for patients with unresectable hepatic metastases from colorectal cancer: Conversion to resection and long-term outcomes. Ann. Surg. 2015, 261, 353–360. [Google Scholar] [CrossRef]
- Kemeny, N.E.; Melendez, F.D.; Capanu, M.; Paty, P.B.; Fong, Y.; Schwartz, L.H.; Jarnagin, W.R.; Patel, D.; D’Angelica, M. Conversion to resectability using hepatic artery infusion plus systemic chemotherapy for the treatment of unresectable liver metastases from colorectal carcinoma. J. Clin. Oncol. 2009, 27, 3465–3471. [Google Scholar] [CrossRef]
- Mancini, R.; Tedesco, M.; Garufi, C.; Filippini, A.; Arcieri, S.; Caterino, M.; Pizzi, G.; Cortesi, E.; Spila, A.; Sperduti, I.; et al. Hepatic arterial infusion (HAI) of cisplatin and systemic fluorouracil in the treatment of unresectable colorectal liver metastases. Anticancer Res. 2003, 23, 1837–1841. [Google Scholar]
- Ranieri, G.; Niccoli Asabella, A.; Altini, C.; Fazio, V.; Caporusso, L.; Marech, I.; Vinciarelli, G.; Macina, F.; De Ceglia, D.; Fanelli, M.; et al. A pilot study employing hepatic intra-arterial irinotecan injection of drug-eluting beads as salvage therapy in liver metastatic colorectal cancer patients without extrahepatic involvement: The first southern Italy experience. OncoTargets Ther. 2016, 9, 7527–7535. [Google Scholar] [CrossRef]
- Gadaleta, C.D.; Catino, A.; Ranieri, G.; Armenise, F.; Console, G.; Mattioli, V. Hypoxic stop-flow perfusion with mitomycin-C in the treatment of multifocal liver metastases. Usefulness of a vascular arterial stent to prevent iatrogenic lesions of the hepatic arterial wall. J. Exp. Clin. Cancer Res. 2003, 22 (Suppl. 4), 203–206. [Google Scholar]
- André, A.; Cisternino, S.; Roy, A.L.; Chiadmi, F.; Schlatter, J.; Agranat, P.; Fain, O.; Fontan, J.E. Stability of oxaliplatin in infusion bags containing 5% dextrose injection. Am. J. Health-Syst. Pharm. 2007, 64, 18–1954. [Google Scholar] [CrossRef] [PubMed]
- Oxaliplatin Technical Data Sheet. Available online: https://www.caymanchem.com/msdss/13106m.pdf (accessed on 10 December 2018).
- Agents Classified by the IARC Monographs, Volumes 1–123—IARC. Available online: https://monographs.iarc.fr/agents-classified-by-the-iarc/ (accessed on 23 January 2019).
- Compendio farmacologico e tecnico-farmaceutico alle linee guida SIFO in Oncologia; Il Pensiero Scientifico Editore: Roma, Italy, 2013.
- Eiden, C.; Philibert, L.; Bekhtari, K.; Poujol, S.; Malosse, F.; Pinguet, F. Physicochemical stability of oxaliplatin in 5% dextrose injection stored in polyvinylchloride, polyethylene, and polypropylene infusion bags. Am. J. Health Syst. Pharm. 2009, 66, 1929–1933. [Google Scholar] [CrossRef] [PubMed]
- Rozencweig, M.; Von Hoff, D.D.; Slavik, M.; Muggia, F.M. Cis-diamminedichloroplatinum(II): A New Anticancer Drug. Ann. Intern. Med. 1977, 86, 803–812. [Google Scholar] [CrossRef] [PubMed]
- Extra, J.M.; Espie, M.; Calvo, F.; Ferme, C.; Mignot, L.; Marty, M. Phase I study of oxaliplatin in patients with advanced cancer. Cancer Chemother. Pharmacol. 1990, 25, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Duffull, S.B.; Robinson, B.A. Clinical pharmacokinetics and dose optimisation of carboplatin. Clin. Pharmacokinet. 1997, 33, 161–183. [Google Scholar] [CrossRef] [PubMed]
- Vander Vijgh, W.J. Clinical pharmacokinetics of carboplatin. Clin. Pharmacokinet. 1991, 21, 242–261. [Google Scholar] [CrossRef]
- Dzodic, R.; Gomez-Abuin, G.; Rougier, P.; Bonnay, M.; Ardouin, P.; Gouyette, A.; Rixe, O.; Ducreux, M.; Munck, J.-N. Pharmacokinetic advantage of hepatic oxaliplatin administration: Comparative results with cisplatin using a rabbit VX2 tumor model. Anticancer Drugs 2004, 15, 647–650. [Google Scholar] [CrossRef]
- Gamelin, E.; Bouil, A.L.; Boisdron-Celle, M.; Turcant, A.; Delva, R.; Cailleux, A.; Krikorian, A.; Brienza, S.; Cvitkovic, E.; Robert, J.; et al. Cumulative pharmacokinetic study of oxaliplatin, administered every three weeks, combined with 5-fluorouracil in colorectal cancer patients. Clin. Cancer Res. 1997, 3, 891–899. [Google Scholar]
- Kern, W.; Beckert, B.; Lang, N.; Stemmler, J.; Beykirch, M.; Stein, J.; Goecke, E.; Waggershauser, T.; Braess, J.; Schalhorn, A.; et al. Phase I and pharmacokinetic study of hepatic arterial infusion with oxaliplatin in combination with folinic acid and 5-fluorouracil in patients with hepatic metastases from colorectal cancer. Ann. Oncol. 2001, 12, 599–603. [Google Scholar] [CrossRef]
- Guthoff, I.; Lotspeich, E.; Fester, C.; Wallin, I.; Schatz, M.; Ehrsson, H.; Kornmann, M. Hepatic artery infusion using oxaliplatin in combination with 5-fluorouracil, folinic acid and mitomycin C: Oxaliplatin pharmacokinetics and feasibility. Anticancer Res. 2003, 23, 5203–5208. [Google Scholar] [PubMed]
- Kornmann, M.; Fakler, H.; Butzer, U.; Beger, H.G.; Link, K.H. Oxaliplatin exerts potent in vitro cytotoxicity in colorectal and pancreatic cancer cell lines and liver metastases. Anticancer Res. 2000, 20, 3259–3264. [Google Scholar] [PubMed]
- Kemeny, M.M.; Battifora, H.; Blayney, D.W.; Cecchi, G.; Goldberg, D.A.; Leong, L.A.; Margolin, K.A.; Terz, J.J. Sclerosing cholangitis after continuous hepatic artery infusion of FUDR. Ann. Surg. 1985, 202, 176. [Google Scholar] [CrossRef] [PubMed]
- Sugihara, K.; Ohtsu, A.; Shimada, Y.; Mizunuma, N.; Gomi, K.; Lee, P.H.; Gramont, A.; Rothenberg, M.L.; Andre, T.; Brienza, S.; et al. Analysis of neurosensory adverse events induced by FOLFOX4 treatment in colorectal cancer patients: Acomparison between two Asian studies and four Westernstudies. Cancer Med. 2012, 1, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Bacchetti, S.; Pasqual, E.; Crozzolo, E.; Pellarin, A.; Cagol, P.P. Intra-arterial hepatic chemotherapy for unresectable colorectal liver metastases: A review of medical devices complications in 3172 patients. Med. Devices (Auckl.) 2009, 2, 31–40. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, A.; Giuliani, R.; Accettura, C.; Palma, M.; D’Auria, G.; Cecere, F.; Paoluzzi, L.; Bezzi, M.; Massidda, B.; Cortesi, E. Hepatic arterial continuous infusion (HACI) of oxaliplatin in patients with unresectable liver metastases from colorectal cancer. Anticancer Res. 2003, 23, 1917–1922. [Google Scholar] [PubMed]
- Fiorentini, G.; Rossi, S.; Dentico, P.; Meucci, F.; Bonechi, F.; Bernardeschi, P.; Cantore, M.; Guadagni, S.; DeSimone, M. Oxaliplatin hepatic arterial infusion chemotherapy for hepatic metastases from colorectal cancer: A phase I-II clinical study. Anticancer Res. 2004, 24, 2093–2096. [Google Scholar]
- Ducreux, M.; Ychou, M.; Laplanche, A.; Gamelin, E.; Lasser, P.; Husseini, F.; Quenet, F.; Viret, F.; Jacob, J.H.; Boige, V.; et al. Hepatic arterial oxaliplatin infusion plus intravenous chemotherapy in colorectal cancer with inoperable hepatic metastases: A trial of the gastrointestinal group of the Federation Nationale des Centres de Lutte Contre le Cancer. J. Clin. Oncol. 2005, 23, 4881–4887. [Google Scholar] [CrossRef]
- Boige, V.; Malka, D.; Elias, D.; Castaing, M.; De Baere, T.; Goere, D.; Dromain, C.; Pocard, M.; Ducreux, M. Hepatic arterial infusion of oxaliplatin and intravenous LV 5FU2 in unresectable liver metastases from colorectal cancer after systemic chemotherapy failure. Ann. Surg. Oncol. 2008, 15, 219–226. [Google Scholar] [CrossRef]
- Tsimberidou, A.M.; Fu, S.; Ng, C.; Lim, J.A.; Wen, S.; Hong, D.; Wheler, J.; Bedikian, A.Y.; Eng, C.; Wallace, M.; et al. A phase 1 study of hepatic arterial infusion of oxaliplatin in combination with systemic 5-fluorouracil, leucovorin, and bevacizumab in patients with advanced solid tumors metastatic to the liver. Cancer 2010, 116, 4086–4094. [Google Scholar] [CrossRef] [Green Version]
- Tsimberidou, A.M.; Leick, M.B.; Lim, J.; Fu, S.; Wheler, J.; Piha-Paul, S.A.; Hong, D.; Falchook, G.S.; Naing, A.; Subbiah, I.M.; et al. Dose-finding study of hepatic arterial infusion of oxaliplatin-based treatment in patients with advanced solid tumors metastatic to the liver. Cancer Chemother. Pharmacol. 2013, 71, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Allard, M.A.; Sebagh, M.; Baillie, G.; Lemoine, A.; Dartigues, P.; Faitot, F.; Faron, M.; Boige, V.; Vitadello, F.; Vibert, E.; et al. Comparison of complete pathologic response and hepatic injuries between hepatic arterial infusion and systemic administration of oxaliplatin in patients with colorectal liver metastases. Ann. Surg. Oncol. 2015, 22, 1925–1932. [Google Scholar] [CrossRef] [PubMed]
- Volovat, S.R.; Volovat, C.; Negru, S.M.; Danciu, M.; Scripcariu, V. The efficacy and safety of hepatic arterial infusion of oxaliplatin plus intravenous irinotecan, leucovorin and fluorouracil in colorectal cancer with inoperable hepatic metastasis. J. Chemother. 2016, 28, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Lévi, F.A.; Boige, V.; Hebbar, M.; Smith, D.; Lepère, C.; Focan, C.; Karaboué, A.; Guimbaud, R.; Carvalho, C.; Tumolo, S.; et al. Association Internationale pour Recherche sur Temps Biologique et Chronothérapie (ARTBC International). Conversion to resection of liver metastases from colorectal cancer with hepatic artery infusion of combined chemotherapy and systemic cetuximab in multicenter trial OPTILIV. Ann. Oncol. 2016, 27, 267–274. [Google Scholar] [PubMed]
- Lim, A.; LeSourd, S.; Senellart, H.; Luet, D.; Douane, F.; Perret, C.; Bouvier, A.; Métairie, S.; Cauchin, E.; Rougier, P.; et al. Hepatic arterial infusion chemotherapy for unresectable liver metastases of colorectal cancer: A multicenter retrospective study. Clin. Colorectal Cancer 2017, 16, 308–315. [Google Scholar] [CrossRef] [PubMed]
- Sato, Y.; Inaba, Y.; Ura, T.; Nishiofuku, H.; Yamaura, H.; Kato, M.; Takahari, D.; Tanaka, T.; Muro, K. Outcomes of a Phase I/II trial of hepatic arterial infusion of oxaliplatin combined with intravenous 5-fluorouracil and I-leucovorin in patients with unresectable liver metastases from colorectal cancer after systemic chemotherapy failure. J. Gastrointest. Cancer 2018, 49, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Laforgia, M.; Cerasino, L.; Margiotta, N.; Capozzi, M.A.M.; Cardellicchio, C.; Naso, F.; Natile, G. Synthesis and Characterization of Platinum(II) Complexes of Diethyl[(Methylsulfinyl)methyl]phosphonate: Potential Drugs against Bone Tumors. Eur. J. Inorg. Chem. 2004, 17, 3445–3452. [Google Scholar] [CrossRef]
- Palazzo, B.; Iafisco, M.; Laforgia, M.; Margiotta, N.; Natile, G.; Bianchi, C.L.; Walsh, D.; Mann, S.; Roveri, N. Biomimetic Hydroxyapatite-Drug Nanocrystals as potential Bone Substitutes with Antitumor Drug Delivery Properties. Adv. Func. Mat. 2007, 17, 2180–2188. [Google Scholar] [CrossRef]
- Groot Koerkamp, B.; Sadot, E.; Kemeny, N.E.; Gönen, M.; Leal, J.N.; Allen, P.J.; Cercek, A.; De Matteo, R.P.; Kingham, T.P.; Jarnagin, W.R.; et al. Perioperative hepatic arterial infusion pump chemotherapy is associated with longer survival after resection of colorectal liver metastases: A propensity score analysis. J. Clin. Oncol. 2017, 35, 1938–1944. [Google Scholar] [CrossRef]
- Kemeny, N.E.; Chou, J.F.; Boucher, T.M.; Capanu, M.; De Matteo, R.P.; Jarnagin, W.R.; Allen, P.J.; Fong, Y.C.; Cercek, A.; D’Angelica, M.I. Updated long-term survival for patients with metastatic colorectal cancer treated with liver resection followed by hepatic arterial infusion and systemic chemotherapy. J. Surg. Oncol. 2016, 113, 477–484. [Google Scholar] [CrossRef] [Green Version]
- Lorenz, M.; Müller, H.H.; Schramm, H.; Gassel, H.J.; Rau, H.G.; Ridwelski, K.; Hauss, J.; Stieger, R.; Jauch, K.W.; Bechstein, W.O.; et al. Randomized trial of surgery versus surgery followed by adjuvant hepatic arterial infusion with 5-fluorouracil and folinic acid for liver metastases of colorectal cancer. German Cooperative on liver metastases (ArbeitsgruppeLebermetastasen). Ann. Surg. 1998, 228, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Tono, T.; Hasuike, Y.; Ohzato, H.; Takatsuka, Y.; Kikkawa, N. Limited but definite efficacy of prophylactic hepatic arterial infusion chemotherapy after curative resection of colorectal liver metastases: A randomized study. Cancer 2000, 88, 1549–1556. [Google Scholar] [CrossRef]
- Berlin, J.; Merrick, H.W.; Smith, T.J.; Lerner, H. Phase II evaluation of treatment of complete resection of hepatic metastases from colorectal cancer and adjuvant hepatic arterial infusion of floxuridine: An Eastern Cooperative Oncology Group Study (PB083). Am. J. Clin. Oncol. 1999, 22, 291–293. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Toxicity | Intravenous Oxaliplatin | Intra-Arterial Oxaliplatin |
|---|---|---|
| Allergic reactions | +++ | not known |
| Anorexia | +++ | not known |
| Neuropathy | +++ | ++ |
| Anaemia | +++ | ++ |
| Thrombocytopenia | +++ | ++ |
| Leukopenia | +++ | ++ |
| Asthenia | +++ | ++ |
| Mucositis | +++ | + |
| Alopecia | +++ | + |
| Nausea/Vomiting | +++ | ++ |
| Diarrhea/Constipation | +++ | ++ |
| Abdominal pain | +++ | ++ |
| Hypertransaminasemia | +++ | ++ |
| Bleeding | +++ | + |
| Thrombosis | ++ | ++ |
| Dyspnea | +++ | not known |
| Reference | Phase of Study | No.of Patients | Previous Treatments | Dose | Systemic Chemotherapy Associated | ORR | mPFS | mOS |
|---|---|---|---|---|---|---|---|---|
| Kern et al. 2001 [43] | I | 21 | Yes or No | 25 mg/m2 with increments of 25 mg/m2 | FUFA | 59% | n.e. | n.e. |
| Mancuso et al. 2003 [49] | I | 17 | Yes | 20 mg/m2/day x 5 days every 3 weeks | None | 67% | n.e. | 19 |
| Fiorentini et al. 2004 [50] | I-II | 12 | Yes | 150 mg/m2 every 3 weeks | None or FUFA ±Irinotecan | 50% | 4 m | 13 m |
| Ducreux et al. 2005 [51] | II | 26 | None or first line of IV CT without oxal | 100 mg/m2 every 2 weeks | FUFA | 64% | 27 m | 27 m |
| Boige et al. 2007 [52] | II | 44 | Yes (> two lines) | 100 mg/m2 every 2 weeks | FUFA | 55% | 7 m | 16 m |
| Tsimberidou et al. 2010 [53] | I | 29 | Yes (> two lines) | 60-175 mg/m2 every 2 weeks | FUFA plus bevacizumab | 43% | n.e. | n.e. |
| Tsimberidou et al.2013 [54] | I | 58 | Yes | 140 mg/m2 every 3 weeks | FUFA+bevacizumab/cetuximab | 12% (KRAS negative) 6% (KRAS positive) | n.e. | 12 m (KRAS negative)7 m (KRAS positive) |
| Allard et al. 2015 [55] | II | 68 | No | 100 mg/m2 every 2 weeks | FUFA+cetuximab | n.e. | n.e. | 114 m |
| Volovat et al. 2016 [56] | II | 24 | Yes or no | 85 mg/m2 every 2 weeks | FOLFIRI | 78% | 20 m | 29 m |
| Lévi et al. 2016 [57] | II | 64 | Yes | 85 mg/m2 every 2 weeks | HAI irinotecan 180 mg/m2+5-FU 2800 mg/m2 plus IV cetuximab | 41% | 9 m | 26 m |
| Lim et al. 2017 [58] | MCS | 61 | Yes or no | every 2 weeks | FUFA+bevacizumab/cetuximab | 11–27% | 9–6 m | 14–8 m |
| Sato et al. 2018 [59] | I-II | 13 | Yes | 50-100 mg/m2 every 2 weeks | FUFA | 70% | n.e. | 7 m |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ranieri, G.; Laforgia, M.; Nardulli, P.; Ferraiuolo, S.; Molinari, P.; Marech, I.; Gadaleta, C.D. Oxaliplatin-Based Intra-arterial Chemotherapy in Colo-Rectal Cancer Liver Metastases: A Review from Pharmacology to Clinical Application. Cancers 2019, 11, 141. https://doi.org/10.3390/cancers11020141
Ranieri G, Laforgia M, Nardulli P, Ferraiuolo S, Molinari P, Marech I, Gadaleta CD. Oxaliplatin-Based Intra-arterial Chemotherapy in Colo-Rectal Cancer Liver Metastases: A Review from Pharmacology to Clinical Application. Cancers. 2019; 11(2):141. https://doi.org/10.3390/cancers11020141
Chicago/Turabian StyleRanieri, Girolamo, Mariarita Laforgia, Patrizia Nardulli, Simona Ferraiuolo, Pasquale Molinari, Ilaria Marech, and Cosmo Damiano Gadaleta. 2019. "Oxaliplatin-Based Intra-arterial Chemotherapy in Colo-Rectal Cancer Liver Metastases: A Review from Pharmacology to Clinical Application" Cancers 11, no. 2: 141. https://doi.org/10.3390/cancers11020141