Clinicopathologic and Imaging Features of Non-Small-Cell Lung Cancer with MET Exon 14 Skipping Mutations

 ,
,
Abstract
:1. Introduction
2. Results
2.1. Clinicopathologic Characteristics
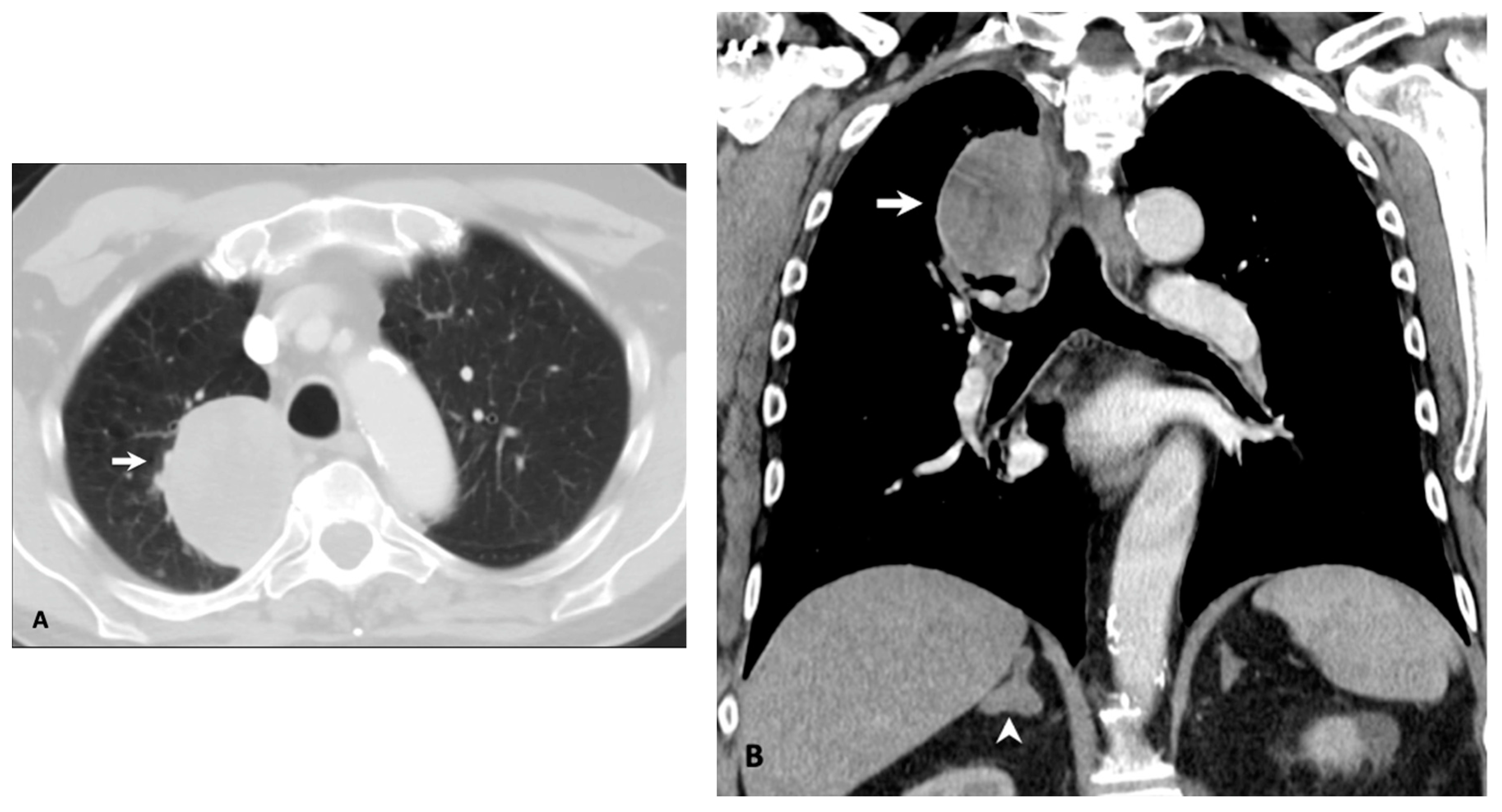
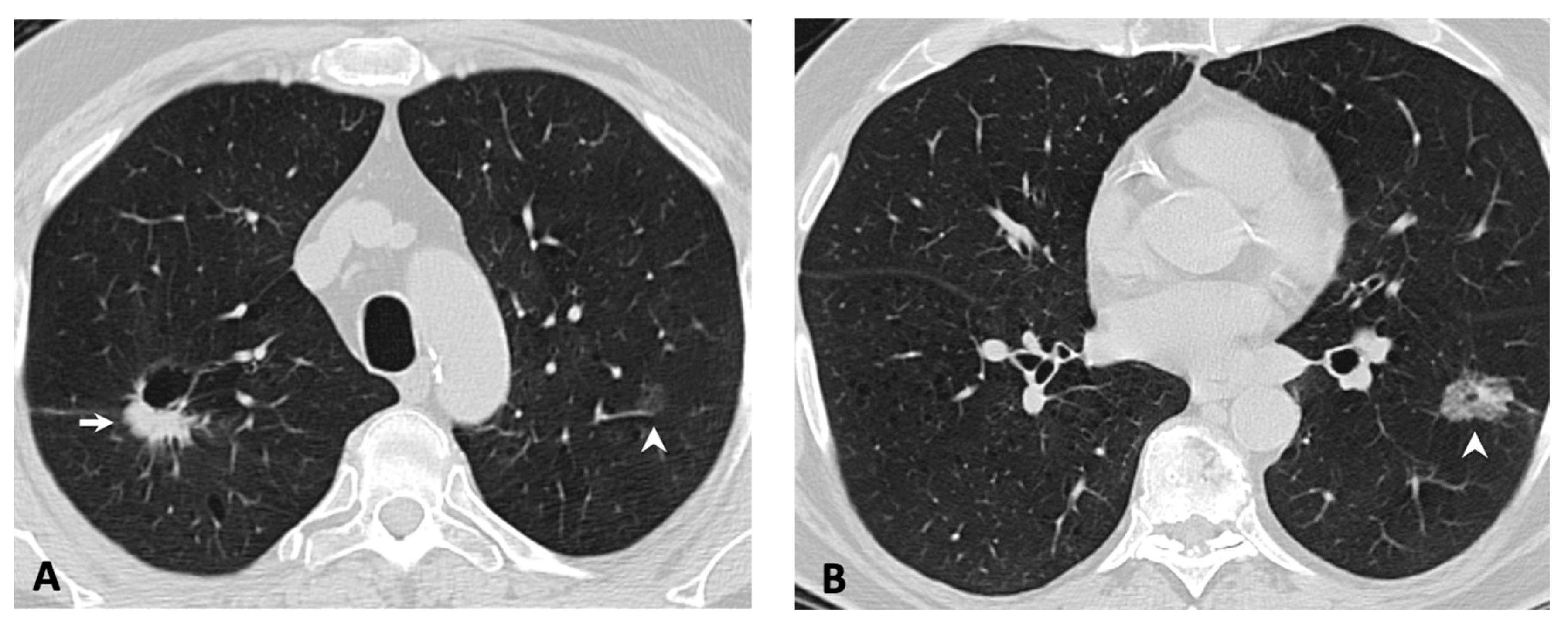
2.2. Imaging Features of the Primary Tumor
2.3. Metastatic Patterns
3. Discussion
4. Materials and Methods
4.1. Patient Identification and Selection
4.2. Molecular Testing
4.3. Imaging Protocol and Image Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Ettinger, D.S.; Aisner, D.L.; Wood, D.E.; Akerley, W.; Bauman, J.; Chang, J.Y.; Chirieac, L.R.; D’Amico, T.A.; Dilling, T.J.; Dobelbower, M.; et al. NCCN Guidelines Insights: Non-Small Cell Lung Cancer, Version 5.2018. J. Natl. Compr. Cancer Netw. 2018, 16, 807–821. [Google Scholar] [CrossRef] [Green Version]
- Planchard, D.; Popat, S.; Kerr, K.; Novello, S.; Smit, E.F.; Faivre-Finn, C.; Mok, T.S.; Reck, M.; Van Schil, P.E.; Hellmann, M.D.; et al. Metastatic non-small cell lung cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2019, 30, 863–870. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.-L.; Thongprasert, S.; Yang, C.-H.; Chu, D.-T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Maemondo, M.; Inoue, A.; Kobayashi, K.; Sugawara, S.; Oizumi, S.; Isobe, H.; Gemma, A.; Harada, M.; Yoshizawa, H.; Kinoshita, I.; et al. Gefitinib or chemotherapy for non-small-cell lung cancer with mutated EGFR. N. Engl. J. Med. 2010, 362, 2380–2388. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, C.; Wu, Y.-L.; Chen, G.; Feng, J.; Liu, X.-Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): A multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef]
- Soria, J.-C.; Ohe, Y.; Vansteenkiste, J.; Reungwetwattana, T.; Chewaskulyong, B.; Lee, K.H.; Dechaphunkul, A.; Imamura, F.; Nogami, N.; Kurata, T.; et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N. Engl. J. Med. 2018, 378, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Shaw, A.T.; Kim, D.-W.; Nakagawa, K.; Seto, T.; Crinó, L.; Ahn, M.-J.; De Pas, T.; Besse, B.; Solomon, B.J.; Blackhall, F.; et al. Crizotinib versus chemotherapy in advanced ALK-positive lung cancer. N. Engl. J. Med. 2013, 368, 2385–2394. [Google Scholar] [CrossRef] [Green Version]
- Peters, S.; Camidge, D.R.; Shaw, A.T.; Gadgeel, S.; Ahn, J.S.; Kim, D.-W.; Ou, S.-H.I.; Pérol, M.; Dziadziuszko, R.; Rosell, R.; et al. Alectinib versus Crizotinib in Untreated ALK-Positive Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 829–838. [Google Scholar] [CrossRef]
- Solomon, B.J.; Besse, B.; Bauer, T.M.; Felip, E.; Soo, R.A.; Camidge, D.R.; Chiari, R.; Bearz, A.; Lin, C.-C.; Gadgeel, S.M.; et al. Lorlatinib in patients with ALK-positive non-small-cell lung cancer: Results from a global phase 2 study. Lancet Oncol. 2018, 19, 1654–1667. [Google Scholar] [CrossRef]
- Shaw, A.T.; Ou, S.-H.I.; Bang, Y.-J.; Camidge, D.R.; Solomon, B.J.; Salgia, R.; Riely, G.J.; Varella-Garcia, M.; Shapiro, G.I.; Costa, D.B.; et al. Crizotinib in ROS1-rearranged non-small-cell lung cancer. N. Engl. J. Med. 2014, 371, 1963–1971. [Google Scholar] [CrossRef] [Green Version]
- Siena, S.; Doebele, R.C.; Shaw, A.T.; Karapetis, C.S.; Tan, D.S.-W.; Cho, B.C.; Kim, D.-W.; Ahn, M.-J.; Krebs, M.; Goto, K.; et al. Efficacy of entrectinib in patients (pts) with solid tumors and central nervous system (CNS) metastases: Integrated analysis from three clinical trials. JCO 2019, 37, 3017. [Google Scholar] [CrossRef]
- Planchard, D.; Kim, T.M.; Mazieres, J.; Quoix, E.; Riely, G.; Barlesi, F.; Souquet, P.-J.; Smit, E.F.; Groen, H.J.M.; Kelly, R.J.; et al. Dabrafenib in patients with BRAF(V600E)-positive advanced non-small-cell lung cancer: A single-arm, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 642–650. [Google Scholar] [CrossRef] [Green Version]
- Planchard, D.; Smit, E.F.; Groen, H.J.M.; Mazieres, J.; Besse, B.; Helland, Å.; Giannone, V.; D’Amelio, A.M.; Zhang, P.; Mookerjee, B.; et al. Dabrafenib plus trametinib in patients with previously untreated BRAFV600E-mutant metastatic non-small-cell lung cancer: An open-label, phase 2 trial. Lancet Oncol. 2017, 18, 1307–1316. [Google Scholar] [CrossRef]
- Cancer Genome Atlas Research Network Comprehensive molecular profiling of lung adenocarcinoma. Nature 2014, 511, 543–550. [CrossRef]
- Charest, A.; Wilker, E.W.; McLaughlin, M.E.; Lane, K.; Gowda, R.; Coven, S.; McMahon, K.; Kovach, S.; Feng, Y.; Yaffe, M.B.; et al. ROS fusion tyrosine kinase activates a SH2 domain-containing phosphatase-2/phosphatidylinositol 3-kinase/mammalian target of rapamycin signaling axis to form glioblastoma in mice. Cancer Res. 2006, 66, 7473–7481. [Google Scholar] [CrossRef] [Green Version]
- Yeung, S.F.; Tong, J.H.M.; Law, P.P.W.; Chung, L.Y.; Lung, R.W.M.; Tong, C.Y.K.; Chow, C.; Chan, A.W.H.; Wan, I.Y.P.; Mok, T.S.K.; et al. Profiling of Oncogenic Driver Events in Lung Adenocarcinoma Revealed MET Mutation as Independent Prognostic Factor. J. Thorac. Oncol. 2015, 10, 1292–1300. [Google Scholar] [CrossRef] [Green Version]
- Aisner, D.L.; Sholl, L.M.; Berry, L.D.; Rossi, M.R.; Chen, H.; Fujimoto, J.; Moreira, A.L.; Ramalingam, S.S.; Villaruz, L.C.; Otterson, G.A.; et al. The Impact of Smoking and TP53 Mutations in Lung Adenocarcinoma Patients with Targetable Mutations-The Lung Cancer Mutation Consortium (LCMC2). Clin. Cancer Res. 2018, 24, 1038–1047. [Google Scholar] [CrossRef] [Green Version]
- Organ, S.L.; Tsao, M.-S. An overview of the c-MET signaling pathway. Ther. Adv. Med. Oncol. 2011, 3, S7–S19. [Google Scholar] [CrossRef] [Green Version]
- Peruzzi, B.; Bottaro, D.P. Targeting the c-Met signaling pathway in cancer. Clin. Cancer Res. 2006, 12, 3657–3660. [Google Scholar] [CrossRef] [Green Version]
- Sierra, J.R.; Tsao, M.-S. c-MET as a potential therapeutic target and biomarker in cancer. Ther. Adv. Med. Oncol. 2011, 3, S21–S35. [Google Scholar] [CrossRef] [Green Version]
- Cooper, C.S.; Park, M.; Blair, D.G.; Tainsky, M.A.; Huebner, K.; Croce, C.M.; Vande Woude, G.F. Molecular cloning of a new transforming gene from a chemically transformed human cell line. Nature 1984, 311, 29–33. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Dean, M.; Cooper, C.S.; Schmidt, M.; O’Brien, S.J.; Blair, D.G.; Vande Woude, G.F. Mechanism of met oncogene activation. Cell 1986, 45, 895–904. [Google Scholar] [CrossRef]
- Birchmeier, C.; Birchmeier, W.; Gherardi, E.; Vande Woude, G.F. Met, metastasis, motility and more. Nat. Rev. Mol. Cell Biol. 2003, 4, 915–925. [Google Scholar] [CrossRef]
- Christensen, J.G.; Burrows, J.; Salgia, R. c-Met as a target for human cancer and characterization of inhibitors for therapeutic intervention. Cancer Lett. 2005, 225, 1–26. [Google Scholar] [CrossRef] [PubMed]
- Engelman, J.A.; Zejnullahu, K.; Mitsudomi, T.; Song, Y.; Hyland, C.; Park, J.O.; Lindeman, N.; Gale, C.-M.; Zhao, X.; Christensen, J.; et al. MET amplification leads to gefitinib resistance in lung cancer by activating ERBB3 signaling. Science 2007, 316, 1039–1043. [Google Scholar] [CrossRef] [PubMed]
- Awad, M.M.; Oxnard, G.R.; Jackman, D.M.; Savukoski, D.O.; Hall, D.; Shivdasani, P.; Heng, J.C.; Dahlberg, S.E.; Jänne, P.A.; Verma, S.; et al. MET Exon 14 Mutations in Non-Small-Cell Lung Cancer Are Associated With Advanced Age and Stage-Dependent MET Genomic Amplification and c-Met Overexpression. J. Clin. Oncol. 2016, 34, 721–730. [Google Scholar] [CrossRef] [Green Version]
- Kong-Beltran, M.; Seshagiri, S.; Zha, J.; Zhu, W.; Bhawe, K.; Mendoza, N.; Holcomb, T.; Pujara, K.; Stinson, J.; Fu, L.; et al. Somatic mutations lead to an oncogenic deletion of met in lung cancer. Cancer Res. 2006, 66, 283–289. [Google Scholar] [CrossRef] [Green Version]
- Heist, R.S.; Shim, H.S.; Gingipally, S.; Mino-Kenudson, M.; Le, L.; Gainor, J.F.; Zheng, Z.; Aryee, M.; Xia, J.; Jia, P.; et al. MET Exon 14 Skipping in Non-Small Cell Lung Cancer. Oncologist 2016, 21, 481–486. [Google Scholar] [CrossRef] [Green Version]
- Paik, P.K.; Drilon, A.; Fan, P.-D.; Yu, H.; Rekhtman, N.; Ginsberg, M.S.; Borsu, L.; Schultz, N.; Berger, M.F.; Rudin, C.M.; et al. Response to MET inhibitors in patients with stage IV lung adenocarcinomas harboring MET mutations causing exon 14 skipping. Cancer Discov. 2015, 5, 842–849. [Google Scholar] [CrossRef] [Green Version]
- Frampton, G.M.; Ali, S.M.; Rosenzweig, M.; Chmielecki, J.; Lu, X.; Bauer, T.M.; Akimov, M.; Bufill, J.A.; Lee, C.; Jentz, D.; et al. Activation of MET via diverse exon 14 splicing alterations occurs in multiple tumor types and confers clinical sensitivity to MET inhibitors. Cancer Discov. 2015, 5, 850–859. [Google Scholar] [CrossRef] [Green Version]
- Jenkins, R.W.; Oxnard, G.R.; Elkin, S.; Sullivan, E.K.; Carter, J.L.; Barbie, D.A. Response to Crizotinib in a Patient With Lung Adenocarcinoma Harboring a MET Splice Site Mutation. Clin. Lung Cancer 2015, 16, e101–e104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, J.H.; Kim, H.S.; Kim, B.J. MET inhibitors in advanced non-small-cell lung cancer: A meta-analysis and review. Oncotarget 2017, 8, 75500–75508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- A Study of Capmatinib (INC280) in NSCLC Patients with MET Exon 14 Alterations Who Have Received Prior MET Inhibitor. Available online: https://clinicaltrials.gov/ct2/show/NCT02750215 (accessed on 26 November 2019).
- Felip, E.; Horn, L.; Patel, J.D.; Sakai, H.; Scheele, J.; Bruns, R.; Paik, P.K. Tepotinib in patients with advanced non-small cell lung cancer (NSCLC) harboring MET exon 14-skipping mutations: Phase II trial. JCO 2018, 36, 9016. [Google Scholar] [CrossRef]
- Tepotinib Phase II in Non-small Cell Lung Cancer (NSCLC) Harboring MET Alteration. Available online: https://clinicaltrials.gov/ct2/show/NCT02864992 (accessed on 26 November 2019).
- Capmatinib in Patients with Non-Small Cell Lung Cancer Harboring cMET Exon 14 Skipping Mutation. Available online: https://clinicaltrials.gov/ct2/show/NCT03693339 (accessed on 26 November 2019).
- CABozantinib in Non-Small Cell Lung Cancer (NSCLC) Patients with MET Deregulation. Available online: https://clinicaltrials.gov/ct2/show/NCT03911193 (accessed on 26 November 2019).
- Wolf, J.; Seto, T.; Han, J.-Y.; Reguart, N.; Garon, E.B.; Groen, H.J.M.; Tan, D.S.-W.; Hida, T.; De Jonge, M.J.; Orlov, S.V.; et al. Capmatinib (INC280) in METΔex14-mutated advanced non-small cell lung cancer (NSCLC): Efficacy data from the phase II GEOMETRY mono-1 study. JCO 2019, 37, 9004. [Google Scholar]
- Nakada, T.; Okumura, S.; Kuroda, H.; Uehara, H.; Mun, M.; Takeuchi, K.; Nakagawa, K. Imaging Characteristics in ALK Fusion-Positive Lung Adenocarcinomas by Using HRCT. Ann. Thorac. Cardiovasc. Surg. 2015, 21, 102–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Schabath, M.B.; Liu, Y.; Han, Y.; Li, Q.; Gillies, R.J.; Ye, Z. Clinical and CT characteristics of surgically resected lung adenocarcinomas harboring ALK rearrangements or EGFR mutations. Eur. J. Radiol. 2016, 85, 1934–1940. [Google Scholar] [CrossRef] [Green Version]
- Cheng, Z.; Shan, F.; Yang, Y.; Shi, Y.; Zhang, Z. CT characteristics of non-small cell lung cancer with epidermal growth factor receptor mutation: A systematic review and meta-analysis. BMC Med. Imaging 2017, 17, 5. [Google Scholar] [CrossRef] [Green Version]
- Yoon, H.J.; Sohn, I.; Cho, J.H.; Lee, H.Y.; Kim, J.-H.; Choi, Y.-L.; Kim, H.; Lee, G.; Lee, K.S.; Kim, J. Decoding Tumor Phenotypes for ALK, ROS1, and RET Fusions in Lung Adenocarcinoma Using a Radiomics Approach. Medicine 2015, 94, e1753. [Google Scholar] [CrossRef]
- Rizzo, S.; Petrella, F.; Buscarino, V.; Maria, F.D.; Raimondi, S.; Barberis, M.; Fumagalli, C.; Spitaleri, G.; Rampinelli, C.; Marinis, F.D.; et al. CT Radiogenomic Characterization of EGFR, K-RAS, and ALK Mutations in Non-Small Cell Lung Cancer. Eur. Radiol. 2016, 26, 32–42. [Google Scholar] [CrossRef]
- Mendoza, D.P.; Dagogo-Jack, I.; Chen, T.; Padole, A.; Shepard, J.-A.O.; Shaw, A.T.; Digumarthy, S.R. Imaging characteristics of BRAF-mutant non-small cell lung cancer by functional class. Lung Cancer 2019, 129, 80–84. [Google Scholar] [CrossRef]
- Mendoza, D.P.; Lin, J.J.; Rooney, M.M.; Chen, T.; Sequist, A.; Shaw, A.T.; Digumarthy, S.R. Imaging features and metastatic patterns of advanced ALK-positive non-small cell lung cancer. Am. J. Roentgenol. 2019; in press. [Google Scholar]
- Digumarthy, S.R.; Mendoza, D.P.; Padole, A.; Chen, T.; Peterson, P.G.; Piotrowska, Z.; Sequist, L.V. Diffuse Lung Metastases in EGFR-Mutant Non-Small Cell Lung Cancer. Cancers 2019, 11, 1360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Digumarthy, S.R.; Padole, A.M.; Gullo, R.L.; Sequist, L.V.; Kalra, M.K. Can CT radiomic analysis in NSCLC predict histology and EGFR mutation status? Medicine 2019, 98, e13963. [Google Scholar] [CrossRef] [PubMed]
- Digumarthy, S.R.; Mendoza, D.P.; Lin, J.J.; Chen, T.; Rooney, M.M.; Chin, E.; Sequist, L.V.; Lennerz, J.K.; Gainor, J.F.; Shaw, A.T. Computed Tomography Imaging Features and Distribution of Metastases in ROS1-rearranged Non-Small-cell Lung Cancer. Clin. Lung Cancer 2019. [Google Scholar] [CrossRef] [PubMed]
- Mendoza, D.P.; Stowell, J.; Muzikansky, A.; Shepard, J.-A.O.; Shaw, A.T.; Digumarthy, S.R. Computed Tomography Imaging Characteristics of Non-Small-Cell Lung Cancer With Anaplastic Lymphoma Kinase Rearrangements: A Systematic Review and Meta-Analysis. Clin. Lung Cancer 2019. [Google Scholar] [CrossRef]
- Zheng, Z.; Liebers, M.; Zhelyazkova, B.; Cao, Y.; Panditi, D.; Lynch, K.D.; Chen, J.; Robinson, H.E.; Shim, H.S.; Chmielecki, J.; et al. Anchored multiplex PCR for targeted next-generation sequencing. Nat. Med. 2014, 20, 1479–1484. [Google Scholar] [CrossRef]
- Midha, A.; Dearden, S.; McCormack, R. EGFR mutation incidence in non-small-cell lung cancer of adenocarcinoma histology: A systematic review and global map by ethnicity (mutMapII). Am. J. Cancer Res. 2015, 5, 2892–2911. [Google Scholar]
- Fan, J.; Dai, X.; Wang, Z.; Huang, B.; Shi, H.; Luo, D.; Zhang, J.; Cai, W.; Nie, X.; Hirsch, F.R. Concomitant EGFR Mutation and EML4-ALK Rearrangement in Lung Adenocarcinoma Is More Frequent in Multifocal Lesions. Clin. Lung Cancer 2019, 20, e517–e530. [Google Scholar] [CrossRef] [Green Version]
- Wang, S.X.Y.; Lei, L.; Guo, H.H.; Shrager, J.; Kunder, C.A.; Neal, J.W. Synchronous primary lung adenocarcinomas harboring distinct MET Exon 14 splice site mutations. Lung Cancer 2018, 122, 187–191. [Google Scholar] [CrossRef]
- Baek, M.Y.; Ahn, H.K.; Park, K.R.; Park, H.-S.; Kang, S.M.; Park, I.; Kim, Y.S.; Hong, J.; Sym, S.J.; Park, J.; et al. Epidermal growth factor receptor mutation and pattern of brain metastasis in patients with non-small cell lung cancer. Korean J. Intern. Med. 2018, 33, 168–175. [Google Scholar] [CrossRef] [Green Version]
- Drilon, A.; Lin, J.J.; Filleron, T.; Ni, A.; Milia, J.; Bergagnini, I.; Hatzoglou, V.; Velcheti, V.; Offin, M.; Li, B.; et al. Frequency of Brain Metastases and Multikinase Inhibitor Outcomes in Patients With RET-Rearranged Lung Cancers. J. Thorac. Oncol. 2018, 13, 1595–1601. [Google Scholar] [CrossRef] [Green Version]
- Patil, T.; Smith, D.E.; Bunn, P.A.; Aisner, D.L.; Le, A.T.; Hancock, M.; Purcell, W.T.; Bowles, D.W.; Camidge, D.R.; Doebele, R.C. The Incidence of Brain Metastases in Stage IV ROS1-Rearranged Non-Small Cell Lung Cancer and Rate of Central Nervous System Progression on Crizotinib. J. Thorac. Oncol. 2018, 13, 1717–1726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadgeel, S.; Gandhi, L.; Riely, G.; Chiappori, A.; West, H.; Azada, M.; Morcos, P.; Lee, R.; Garcia, L.; Yu, L.; et al. Safety and activity of alectinib against systemic disease and brain metastases in patients with crizotinib-resistant ALK-rearranged non-small-cell lung cancer (AF-002JG): Results from the dose-finding portion of a phase 1/2 study. Lancet Oncol. 2014, 15, 1119–1128. [Google Scholar] [CrossRef]
- Song, Z.; Wang, H.; Yu, Z.; Lu, P.; Xu, C.; Chen, G.; Zhang, Y. De Novo MET Amplification in Chinese Patients With Non-Small-Cell Lung Cancer and Treatment Efficacy With Crizotinib: A Multicenter Retrospective Study. Clin. Lung Cancer 2019, 20, e171–e176. [Google Scholar] [CrossRef] [PubMed]
- Luketich, J.D.; Martini, N.; Ginsberg, R.J.; Rigberg, D.; Burt, M.E. Successful treatment of solitary extracranial metastases from non-small cell lung cancer. Ann. Thorac. Surg. 1995, 60, 1609–1611. [Google Scholar] [CrossRef]
- Schanne, D.H.; Heitmann, J.; Guckenberger, M.; Andratschke, N.H.J. Evolution of treatment strategies for oligometastatic NSCLC patients - A systematic review of the literature. Cancer Treat. Rev. 2019, 80, 101892. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Clinical Characteristics | ||
|---|---|---|
| Age | ||
| Mean, SD (in years) | 71.4 | 10 |
| Median, range (in years) | 72.5 | 43–89 |
| Sex | n | % |
| F (%) | 52 | 61.9 |
| M (%) | 32 | 38.1 |
| Smoking status | ||
| Never | 37 | 44.0 |
| Current/Previous | 47 | 56.0 |
| Stage | ||
| I | 34 | 40.5 |
| II | 9 | 10.7 |
| IIIA | 5 | 6.0 |
| IIIB | 2 | 2.4 |
| IV | 34 | 40.5 |
| Histology | ||
| Adenocarcinoma | 72 | 85.7 |
| Squamous | 6 | 7.1 |
| Sarcomatoid carcinoma | 3 | 3.6 |
| Others | 3 | 3.6 |
| Tumor Imaging Features | ||
|---|---|---|
| Size | ||
| Mean, SD (in mm) | 40.8 | 21.4 |
| Median, range (in mm) | 34.5 | 10–109 |
| Size | n | % |
| Mass (>3 cm) | 53 | 63.1 |
| Nodule (≤3 cm) | 31 | 36.9 |
| Lobar location | ||
| RUL | 38 | 45.2 |
| RML | 4 | 4.8 |
| RLL | 10 | 11.9 |
| LUL | 17 | 20.2 |
| LLL | 15 | 17.9 |
| Lobar location | ||
| Upper/Middle | 59 | 70.2 |
| Lower | 25 | 29.8 |
| Axial location | ||
| Peripheral | 62 | 73.8 |
| Central | 22 | 26.2 |
| Density | ||
| Solid | 57 | 67.9 |
| Part-solid | 21 | 25.0 |
| Pure ground-glass | 6 | 7.1 |
| Margin | ||
| Smooth | 9 | 10.7 |
| Lobulated | 53 | 63.1 |
| Spiculated | 22 | 26.2 |
| Other Tumor features | ||
| Air bronchograms | 3 | 3.6 |
| Cavitation | 4 | 4.8 |
| Cystic component | 4 | 4.8 |
| Calcification | 0 | 0.0 |
| Multifocal | 19 | 22.6 |
| Metastatic Site | n | % |
|---|---|---|
| Nodal metastasis | ||
| Ipsilateral hilar | 29 | 85.3 |
| Ipsilateral mediastinal | 19 | 55.9 |
| Contralateral hilar/mediastinal | 12 | 35.3 |
| Supraclavicular | 7 | 20.6 |
| Intrathoracic metastasis | 13 | 38.2 |
| Lung | 5 | 14.7 |
| Lymphangitic carcinomatosis | 4 | 11.8 |
| Pleural | 10 | 29.4 |
| Pericardial | 2 | 5.9 |
| Extrathoracic Metastasis | 28 | 82.4 |
| Adrenal | 7 | 20.6 |
| Liver | 3 | 8.8 |
| Gastric | 2 | 5.9 |
| Splenic | 0 | 0.0 |
| Bone (Lytic) | 14 | 41.2 |
| Brain | 7 | 20.6 |
| Soft tissue | 1 | 2.9 |
| Distant lymph node | 4 | 11.8 |
| Metastatic Distribution | ||
| Intrathoracic only | 1 | 2.9 |
| Extrathoracic only | 23 | 67.6 |
| Intra- and extrathoracic | 10 | 29.4 |
| Number of sites | ||
| One | 4 | 11.8 |
| Two or more | 30 | 88.2 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Digumarthy, S.R.; Mendoza, D.P.; Zhang, E.W.; Lennerz, J.K.; Heist, R.S. Clinicopathologic and Imaging Features of Non-Small-Cell Lung Cancer with MET Exon 14 Skipping Mutations. Cancers 2019, 11, 2033. https://doi.org/10.3390/cancers11122033
Digumarthy SR, Mendoza DP, Zhang EW, Lennerz JK, Heist RS. Clinicopathologic and Imaging Features of Non-Small-Cell Lung Cancer with MET Exon 14 Skipping Mutations. Cancers. 2019; 11(12):2033. https://doi.org/10.3390/cancers11122033
Chicago/Turabian StyleDigumarthy, Subba R., Dexter P. Mendoza, Eric W. Zhang, Jochen K. Lennerz, and Rebecca S. Heist. 2019. "Clinicopathologic and Imaging Features of Non-Small-Cell Lung Cancer with MET Exon 14 Skipping Mutations" Cancers 11, no. 12: 2033. https://doi.org/10.3390/cancers11122033