1. Introduction
The macroscopic vascular invasion of hepatocellular carcinoma (HCC), including portal vein tumor thrombosis (PVTT) or inferior vena cava tumor thrombosis (IVCTT), corresponds to the Barcelona Clinic Liver Cancer (BCLC) stage C disease and remains a daunting challenge for treatment [
1,
2]. The current standard of care for HCC patients with PVTT/IVCTT is sorafenib, which is recommended as the only treatment option in EASL–EORTC practical guideline [
3]. However, only modest clinical efficiency was observed when adopting sorafenib monotherapy for HCC patients with macrovascular invasion (MVI), with a median overall survival (OS) time of 8.1 months in the SHARP trial [
4].
Transarterial chemoembolization (TACE) is the most popular palliative treatment for patients with unresectable HCC. In the past decade, the strategy of combining conventional TACE and sorafenib to treat HCC patients with macroscopic invasion had been proposed [
5,
6,
7] and reported to prolong the time-to-progression (TTP) by 0.4 months and OS by three months when compared to sorafenib monotherapy [
8]. The underlying rationale for developing this combination is that sorafenib can inhibit the tumor angiogenesis after TACE and lead to a synergistic therapeutic effect, which is supported by a preclinical study [
9]. Although a survival benefit had been witnessed by adopting this combination, the survival of these HCC patients remained poor and a better combination was needed.
In recent years, the advances in radiotherapy techniques, including three-dimensional conformal radiotherapy (3D-CRT), have facilitated the safe and effective delivery of a high dose of radiation to the tumor while preserving the surrounding tissue [
10]. A recent randomized controlled trial conducted in Korea involving HCC patients with macroscopic vascular invasion reported encouraging results where sequentially combined TACE and 3D-CRT was well tolerated, and the combined therapy improved progression-free survival (PFS), objective response rate, TTP, and OS when compared with those of sorafenib monotherapy [
11]. Compared with 3D-CRT, stereotactic body radiotherapy (SBRT) is a more advanced form of radiation modality in which a high-radiation dose can be precisely concentrated on the tumor in a few fractions [
10,
12]. The sequential combination of TACE with SBRT has great potential to challenge the current golden combination of the TACE–sorafenib strategy in the management of HCC patients with PVTT/IVCTT [
13].
Therefore, the goal of this study was to retrospectively compare the OS and PFS in advanced HCC patients with macroscopic vascular invasion who are undergoing combined TACE–SBRT treatment versus combined TACE–sorafenib treatment.
3. Discussion
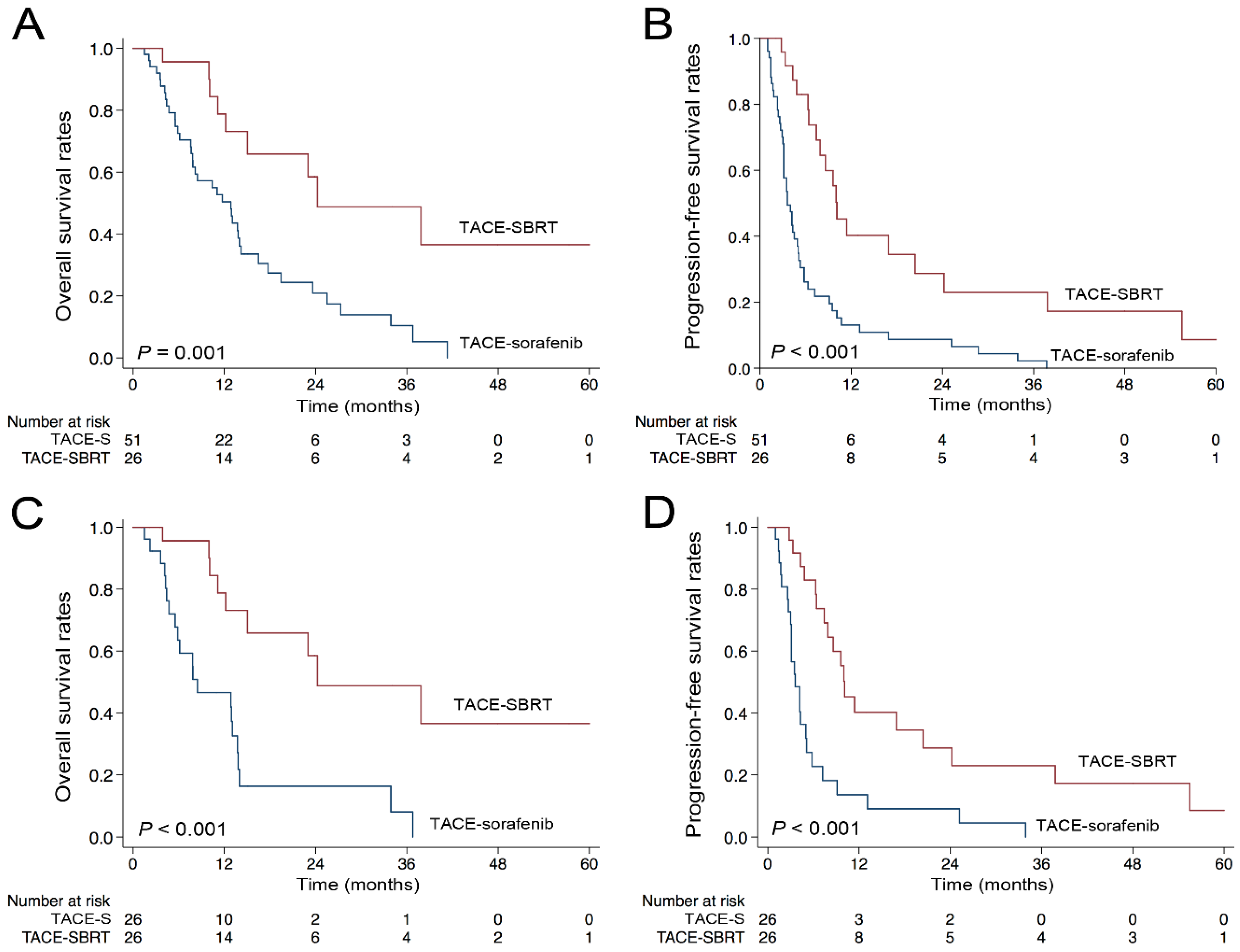
In this study, we found that TACE sequentially combined with SBRT is a safe and effective combination strategy for HCC patients with MVI. The results of PSM suggested that TACE–SBRT combination therapy had superior therapeutic efficacy compared to TACE–sorafenib combination therapy in the treatment of HCC patients with macroscopic vascular invasion.
In Asian regions, TACE is considered the primary treatment for patients with unresectable HCC confined to the liver [
14]. Two randomized trials comparing TACE to conservative treatment in HCC patients with PVTT consistently demonstrated favorable OS in the TACE arm [
15,
16]. Follow-up efforts had been made to improve the embolization efficacy for unresectable HCC through using drug-eluting beads and yttrium-90 radio-embolization; however, the achieved survival benefits were limited, as reported by a recently published network meta-analysis [
17].
Sorafenib has been considered the first-line treatment for HCC patients with MVI in most guidelines [
3,
18,
19]. Past studies suggest that TACE–sorafenib therapy could be a promising treatment combination for advanced stage HCC [
20]. In an Asia-Pacific trial [
21], the median OS time for sorafenib monotherapy was 6.5 months, while the median OS for TACE–sorafenib combination therapy was reported to range from to 8.9 to 11.0 months [
8,
22]. However, until now, neither TACE nor sorafenib had been reported to provide a durable treatment response for tumor thrombus of HCC [
23]. Macrovascular invasion of HCC could not only promote intrahepatic dissemination of tumor cells [
24], but could also contribute to portal hypertension, leading to the deterioration of liver function and subsequent complications including ascites, variceal hemorrhage, and thrombocytopenia induced by splenomegaly [
25]; these complications could impede further treatment. Therefore, a good local control of the tumor thrombus is important in the management of advanced HCC with macrovascular invasion. In our study, a better overall response rate as well as significantly favorable survival were observed in patients in the TACE–SBRT group compared with those in TACE–sorafenib group. The survival benefits of the TACE–SBRT combination therapy could be explained by the fact that SBRT is an advanced radiation modality that can concentrate a high radiation dose precisely on the tumor in a few fractions, provide a high local control rate (>80%) for tumor thrombosis, while TACE provides good control of tumors outside the radiation field as a complement. The combination of TACE and SBRT enabled a balance in the control of HCC and the maintenance of liver function, thereby allowing additional treatments [
11,
26], including subsequent curative surgical resection, as shown in our study.
In our study, the OS and PFS for the TACE–SBRT group were 24.2 and 10.1 months, respectively, which were higher than 12.7 and 7.2 months for patients treated by TACE-3D-CRT in the recently published study by Yoon et al. [
11]. This difference may be due to the fact that in our study, patients with lymph node metastasis and distant metastasis were excluded; moreover, the median tumor size in the TACE–SBRT group in our study was 7.7 cm, which was lower than the 9.8 cm in their study. The encouraging results in our study imply that HCC patients with a small tumor size and macroscopic vascular invasion and without extrahepatic lesions were the ideal population for receiving TACE–SBRT combination therapy. On the other side, our results might also suggest that TACE–SBRT can provide better local control than TACE-3D-CRT, as the overall response rate of 42.3% in the TACE–SBRT group in our study was higher than the response rate of 33.3% in the TACE-3D-CRT group reported by Yoon et al.
Although TACE–SBRT combination therapy had promising therapeutic efficacy in HCC patients with MVI, the median survival time in this group is still shorter. Further enhancing the treatment efficacy may require additional combinations. TACE-combined ablative therapies like radiofrequency ablation have been widely recognized for their efficacy in controlling intrahepatic lesions of HCC [
2,
27,
28]. The combination of TACE, ablative therapies, and SBRT has the potential to achieve better local control than TACE–SBRT alone in a minimally invasive way. However, the ways to combine these three modalities require further research. In the area of immunotherapy, Kim et al. reported preclinical data on the improved anti-tumor effect of checkpoint inhibitors after radiation in HCC [
29]. Hence, combining PD1/PD-L1 antibodies following TACE–SBRT therapy could also be a direction for research.
For the HCC patients who underwent SBRT, image-guided radiation therapy (IGRT) is mandatory and fundamental to ensure precision. The key to safe SBRT is to match the target in the planning CT to the target itself on the cone-beam CT before each fraction [
30]. Since the liver lesions are usually invisible on the cone-beam CT without contrast injection, the use of implanted fiducials in and/or around the tumor as surrogates is a reliable way to assess respiratory motion during treatment, especially for robotic-based liver SBRT [
31]. However, only a minority of patients choose this manner in clinical practice because internal fiducials are invasive to insert and have a relatively higher cost. Therefore, for patients who received TACE as initial treatment before radiotherapy, we usually used embolization material as a surrogate for tumor position at our institution.
This study had several limitations. First, it is a retrospective study. Second, the sample size of patients enrolled in each group was relatively small, which impeded further stratified analysis. Third, all TACE procedures were performed in our cancer center, which may cause bias as TACE is operator dependent. For these reasons, a multi-institutional clinical trial is needed in the future.
4. Materials and Methods
4.1. Study Design
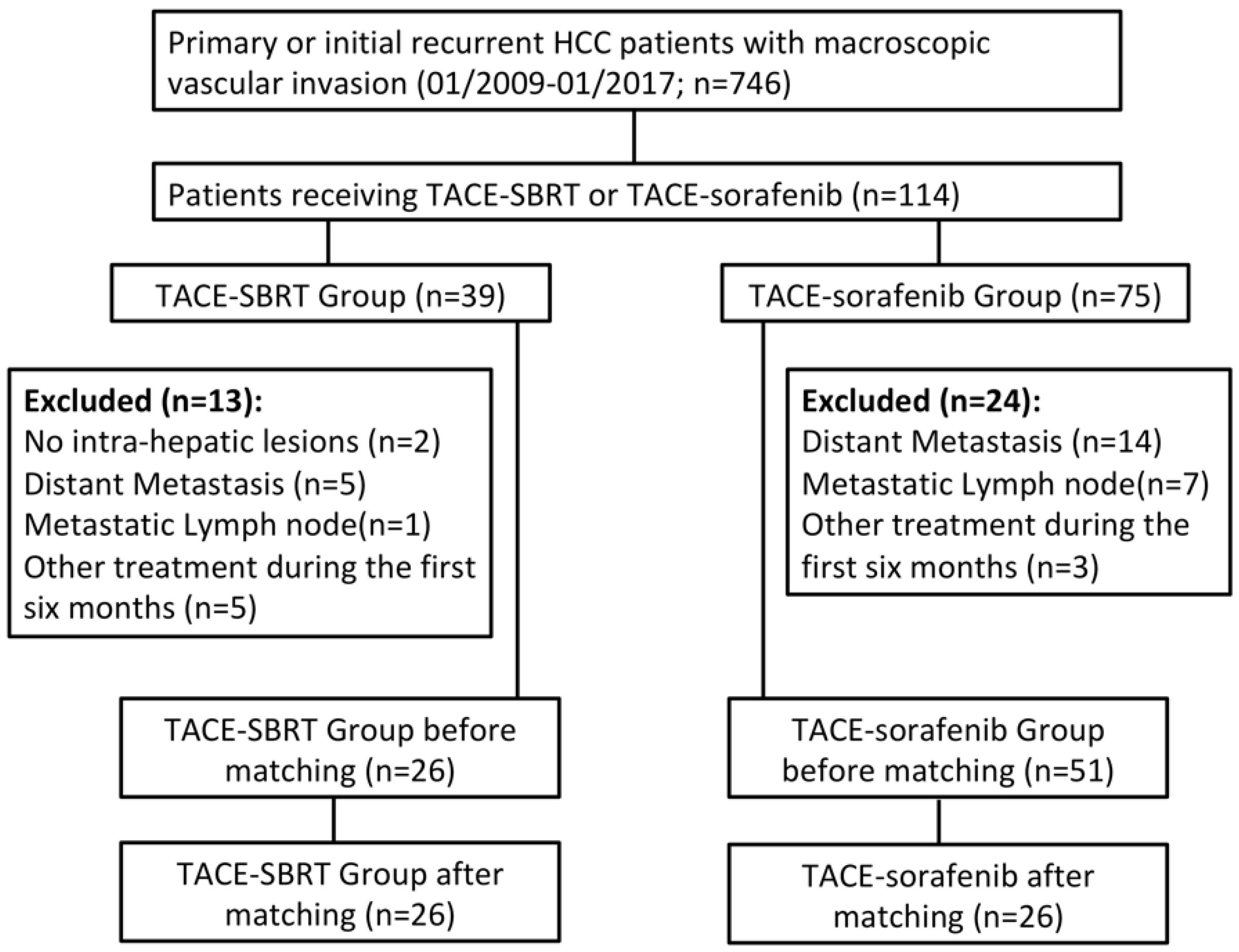
From January 2009 to January 2017, a consecutive series of 746 HCC patients with macroscopic vascular invasion were retrospectively reviewed. This study was approved by the SYSUCC Hospital Ethics Committee (No. B2018-156-01), which waived the need for written informed consent because of the retrospective nature of the study. The inclusion criteria were: (a) initially diagnosed HCC with macroscopic vascular invasion or recurrent HCC after surgical resection with macroscopic vascular invasion; (b) received TACE as initial treatment and achieved technical success; (c) potential candidates for SBRT of vascular tumor thrombi evaluated by two radiation oncologists with more than 10 years’ experience; (d) received SBRT of vascular invasion within 3 months after first TACE or started sorafenib treatment within 1 week after first TACE as combination treatment; and (e) Child–Pugh A or B. The exclusion criteria were: (a) presence of extrahepatic metastasis detected on abdominal CT/MRI scan or chest CT scan/digital chest radiograph; (b) recurrent tumors with no intrahepatic lesions; (c) received other treatment including ablative therapies, surgical resection, transplantation within the first 6 months after initial TACE; and (d) other malignancies. A total of 77 patients were enrolled in this study with 26 in the TACE–SBRT group and 51 in the TACE–sorafenib group (
Figure 2).
In this study, each case was fully evaluated by a multidisciplinary team before the initiating treatment, including interventional radiologists, oncologists, pathologists, radiologists, and radiation oncologists. Each patient was informed of the advantages and disadvantages of the two treatment plans before initial TACE, including costs, treatment-related morbidities, and treatment outcomes. The decision regarding the treatment plan was made jointly by the patient and doctors.
4.2. Transarterial Chemoembolization
For the TACE procedure, based on the tumor size, location, number, and vascular supply, a super-selective microcatheter was inserted into the supplying artery of the tumor. Then a combination of lipiodol (5–15 mL), lobaplatin (30–50 mg) and pirarubicin (30–50 mg) was introduced into the tumor. Technical success was defined as full embolization of the tumor feeding artery and with no tumor staining observed by angiogram at the end of procedure. Transarterial chemoembolization was repeated every 4–5 weeks thereafter, and was discontinued if the patients could not tolerate additional procedures due to adverse effects or when they refused further treatment. For the initial 6 months, the mean repeats of TACE for patients in the TACE–SBRT group was 1.50 (range, 1–2) before SBRT and 0.3 (range, 0–3) after SBRT (
Table S1); the mean repeats of TACE for patients in the TACE–sorafenib group was 2.1 (range, 1–6).
4.3. Stereotactic Body Radiotherapy
In the TACE–SBRT group, SBRT was scheduled after one to two administrations of TACE and completed within 3 months after the initial TACE. All patients underwent four-dimensional computed tomography (4DCT) scans at 2.5- or 3-mm slice thickness during free breathing. The tumor thrombosis visualized on the CT/MRI images and the contiguous HCC were defined as gross tumor volume (GTV) for all patients; the intrahepatic metastases of HCC were not included in GTV. The internal target volume (ITV) was defined as the combined volume of GTVs in the multiple 4DCT phases. To take interfractional motion variability and daily setup errors into account, the planning target volume (PTV) was acquired by adding a 6-mm margin to the ITV.
Volumetric modulated arc therapy (VMAT) techniques, which typically was planned for a 6 MV photons Elekta accelerator (Versa HD
TM, Stockholm, Sweden), was utilized to perform SBRT. Planning of VMAT was conducted utilizing Monaco TPS (CMS, Elekta, Stockholm, Sweden) and consisted of a single arc [
32].
The median prescription dose was 36 Gy (range, 30–42 Gy) to PTV in six fractions, 3 days per week. The total radiation dose was determined on the basis of tumor size, tumor location, and patients’ Child–Pugh Class. The dose constraints for organs at risk were defined as follows: mean dose of normal liver <18 Gy, mean dose of kidneys <15 Gy, maximum dose to spinal cord <27 Gy, and maximum dose to >0.5 cc of esophagus, stomach, or small intestine <30 Gy. Daily image guidance was performed using cone-beam CT for alignment of liver anatomy prior to each fraction.
4.4. Sorafenib Administration
For patients in the TACE–sorafenib group, sorafenib was continuously administered orally at a dosage of 400 mg twice a day (800 mg/day). Dosage reductions and termination of treatment were permitted if unacceptable treatment-related toxicity occurred or disease progressed.
4.5. Follow-Up and Endpoints
Patients in both groups were followed up and evaluated for response every 4–5 weeks during sessions of treatment and then every 3 months until death through contrast-enhanced CT or MR scans. The primary endpoint was overall survival (OS), which was calculated from the date of the initial treatment to death by any causes. The secondary endpoint was progression-free survival (PFS), which was calculated from the date of the initial treatment to disease progression or death.
Tumor response assessments were made by two independent radiologists using the modified Response Evaluation Criteria in Solid Tumors (mRECIST), who were blinded to each other’s opinion [
33]. According to mRECIST criteria, tumor thrombosis (TT) should be considered a nontarget lesion. Complete response (CR) was defined as the disappearance of TT; incomplete response/stable disease was the persistence of TT; progressive disease was the unequivocal progression of TT. The best treatment response at 24 weeks after initial TACE was assessed for each patient in the two treatment groups. The response rate (RR) was defined as the proportion of patients with complete response (CR) or partial response (PR) in each treatment group.
4.6. Statistical Analysis
Categorical variables between treatment groups were compared using Pearson χ2 test or Fisher’s exact test. Ordinal variables between groups were compared using Wilcoxon rank sum test. OS and PFS were estimated by Kaplan–Meier method and the differences between the groups were compared using the log-rank test. Multivariate Cox regression model in backward conditioned method was utilized to determine the independent prognostic factors for survival.
Propensity score matching analysis was performed to reduce the potential bias in patient selection. The selected variables entered into the propensity model included age, gender, disease onset, Child–Pugh Class, AFP level, liver tumor size, number of tumors, type of PVTT and HV/IVC invasion. One-to-one matching between the groups was accomplished using the nearest-neighbor method, with the caliper of 0.25. Following propensity score matching, the adjusted comparisons were based on data from 26 patients in each treatment arm. Statistical analyses were performed using SPSS 21.0 or R 3.3.2 (The R Foundation for Statistical Computing, 2018). The value p < 0.05 was considered statistically significant.
The authenticity of this article has been validated by uploading the key raw data onto the Research Data Deposit public platform (
www.researchdata.org.cn), with the approval RDD number as RDDA2018000943.

 ,
, 


{kind=link}
{kind=link}