1. Introduction
Pancreatic cancer has extremely poor prognosis and represents the fourth leading cause of cancer-related mortality in the world. Among the various malignancies ten-year (4.6% for males and 4.8% for females) and five-year (7.0% for males and 5.9% for females) survival rates in Japan are the worst for pancreatic cancer [
1,
2]. There are few effective therapies for pancreatic cancer, indicating the urgent need for development of more effective chemotherapies to improve the poor outcomes of this malignancy.
FOLFIRINOX, a combination chemotherapy of oxaliplatin, irinotecan, 5-fluorouracil (5-FU), and L-leucovorin, has been shown to significantly prolong survival and is currently a standard chemotherapy for advanced pancreatic cancer. Conroy et al. showed that FOLFIRINOX therapy exhibited clinical superiority over gemcitabine monotherapy with respect to overall survival (OS), progression-free survival (PFS), and tumor response rate (RR) in patients with metastatic pancreatic cancer [
3]. However, grade 3–4 neutropenia occurs more frequently in patients treated with FOLFIRINOX than gemcitabine (45.7% versus 21.0%,
p < 0.001). A high incidence of grade 3–4 neutropenia (77.8%) has also been observed in Japanese patients receiving FOLFIRINOX for metastatic pancreatic cancer [
4].
To reduce the incidence of toxicities associated with FOLFIRINOX, the chemotherapy regimen has been modified by omission the bolus injection of 5-FU and/or reducing the dose of irinotecan without reducing the clinical response [
5,
6,
7,
8,
9]. Modification of the FOLFIRINOX regimen (oxaliplatin 85 mg/m
2, irinotecan 150 mg/m
2, 5-FU infusion 2400 mg/m
2 over 46 h, no bolus 5-FU) reduces the incidence of grade 3–4 neutropenia to 47.8% [
7]. More importantly, a meta-analysis showed that the modified FOLFIRINOX regimen is as effective as the original, with a similar tumor response rate (32% versus 33%,
p = 0.879), rate of 12-month survival (47% versus 50%,
p = 0.38), rate of 6-month PFS rate (47% versus 53%,
p = 0.38) and reduced frequency of grade 3–4 adverse events [
10].
The occurrence of severe adverse events, including neutropenia [
11,
12], mucositis [
13], neurotoxicity [
14] and diarrhea [
15], during cancer chemotherapy results in impaired patient quality of life and leads to the therapy interruption or dose reduction. The latter may lead to a reduction in the therapeutic effect due to the decrease in the relative dose intensity (RDI). For example, the incidence of grade 4 neutropenia is significantly higher, while median PFS and OS are significantly shorter in non-small cell lung cancer patients receiving irinotecan with
UGT1A1*6 homozygous mutation compared to the heterozygous mutation or wild-type allele [
16]. The incidence rates of diarrhea and neutropenia are significantly higher, while median OS tends to be shorter in metastatic colorectal cancer patients receiving irinotecan with
UGT1A1*28 heterozygous or homozygous mutations compared to the wild-type allele [
17].
In contrary, several investigators have shown that the occurrence myelosuppression such as neutropenia is a surrogate for better survival in patients receiving cancer chemotherapy. In patients with metastatic colorectal cancer who receive FOLFOX therapy, the incidences of mild (grade 1–2) and severe (grade 3–4) neutropenia are associated with improved survival [
18]. In patients with advanced pancreatic cancer who received gemcitabine alone or in combination with other anticancer drugs, the median OS is significantly longer in patients with early onset of neutropenia than in those without neutropenia [
19]. Comparison of the effect of gemcitabine monotherapy on survival among metastatic pancreatic patients with grade 3 neutropenia, those with grade 1–2 neutropenia and those without neutropenia also shows that the median survival time is prolonged with increasing grade of neutropenia [
20]. Therefore, the incidence neutropenia may have different effects on the survival period, depending on the cancer type and chemotherapy regimen.
We investigated the relationship between the incidence of severe neutropenia and OS in patients with advanced pancreatic cancer who received modified FOLFIRINOX as first-line chemotherapy to determine whether or not the incidence of severe neutropenia causes favorable survival outcomes in these patients
3. Discussion
FOLFIRINOX or modified FOLFIRINOX is the first-line chemotherapy for advanced pancreatic cancer, however, these regimens cause a number of severe adverse events, including neutropenia. The present study showed that a large portion of patients (76.5%, 39/51 patients) experienced grade 3-4 neutropenia during the course of modified FOLFIRINOX therapy. The occurrence of severe adverse events may cause therapy interruption or a reduction in the dose of chemotherapy drugs, thereby affecting the clinical outcomes. In the present study, the incidence of severe neutropenia led to dose reduction. In particular, the RDIs for irinotecan, oxaliplatin and 5-FU were all significantly lower in patients with severe neutropenia than in those with grades 0–2 neutropenia.
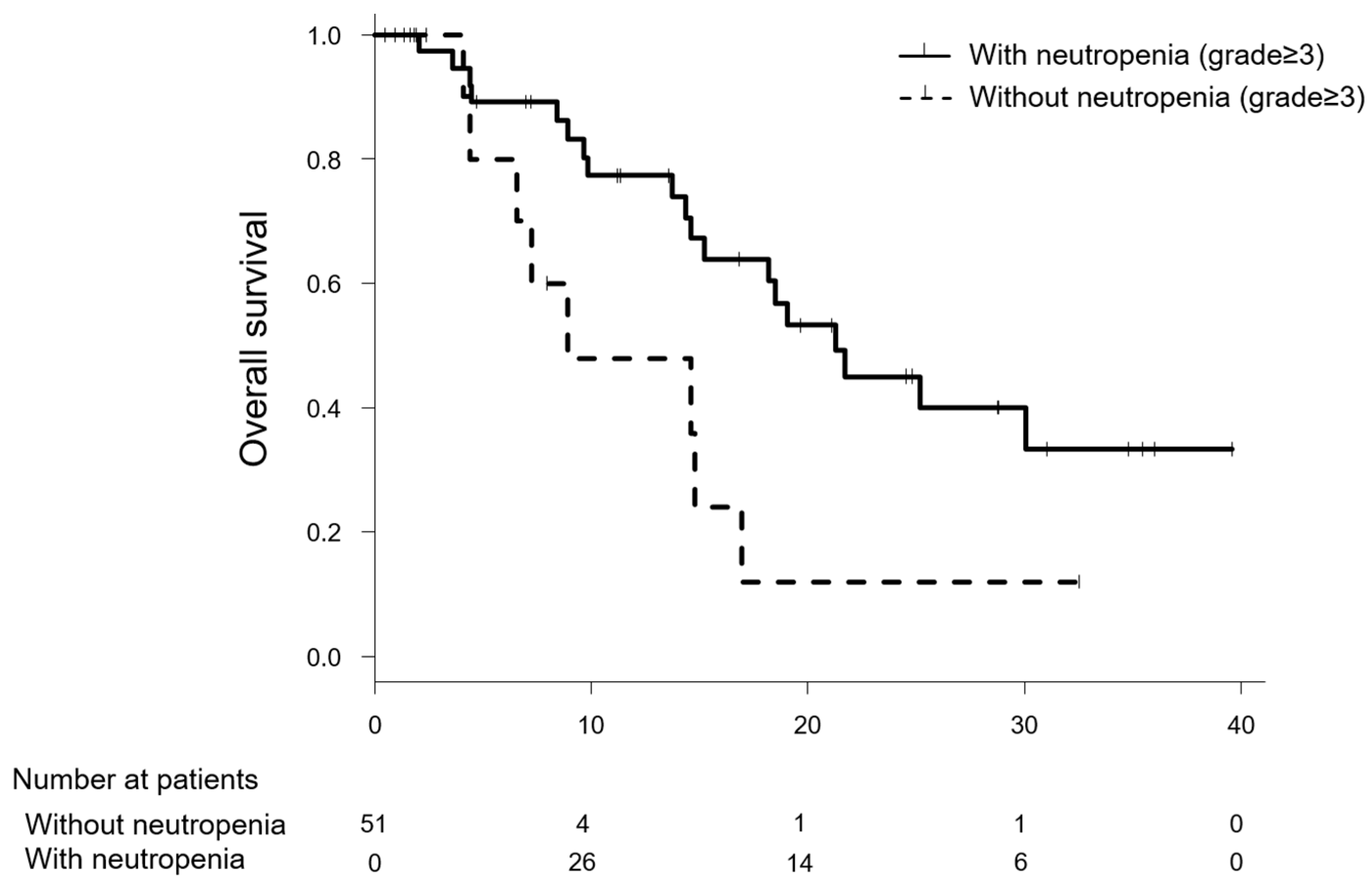
Nevertheless, it was noteworthy that the patients with grade 3–4 neutropenia showed significantly longer survival than those without severe neutropenia in the Simon and Makuch’s modified Kaplan-Meier curves, and the relationship between neutropenia and OS was significant after adjusting for age and NLR with time varying Cox proportional hazards regression.
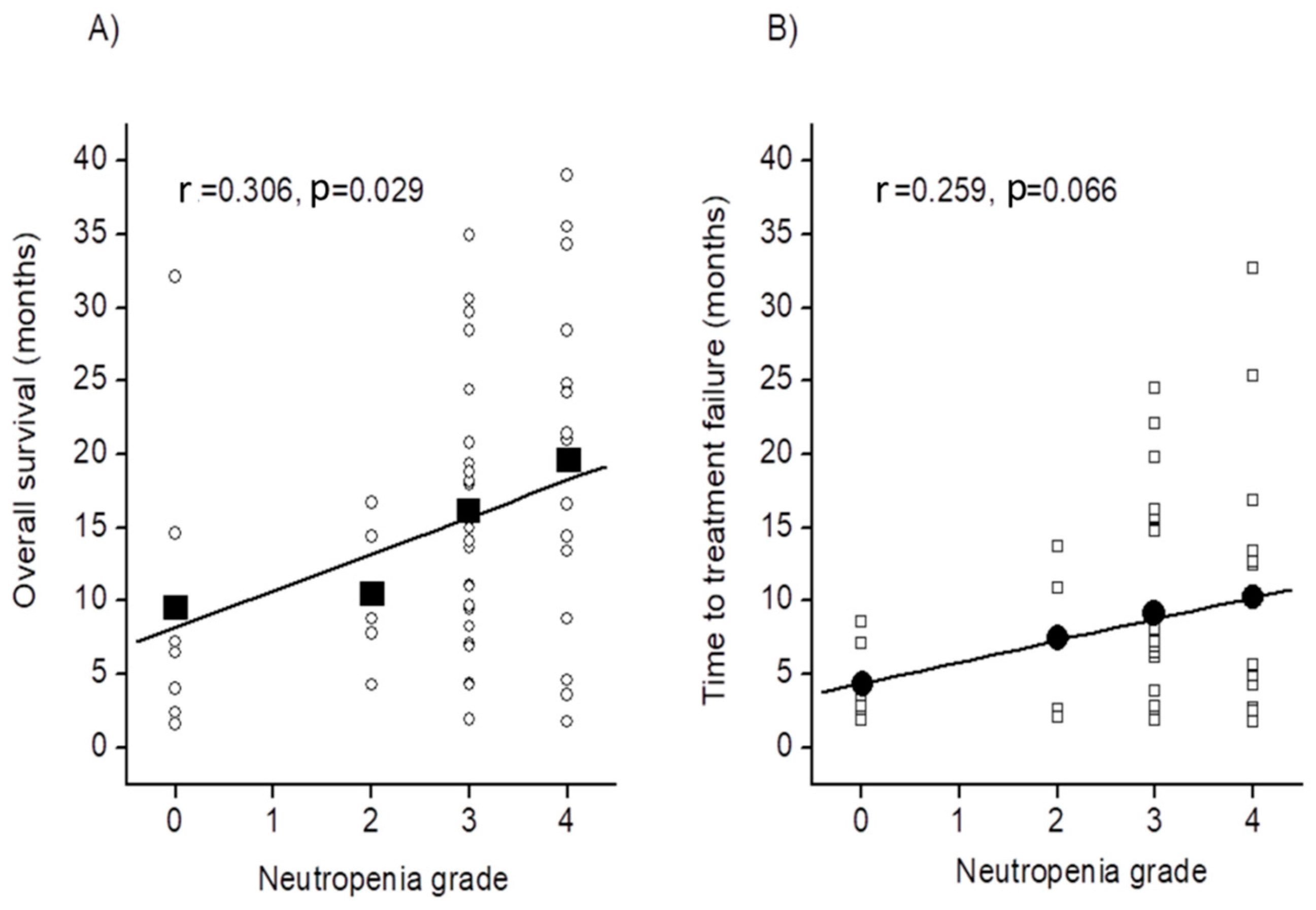
Additionally, severe neutropenia was a significant factor for better survival, and the OS well correlated with the grade of neutropenia. Moreover, there was also a trend towards a correlation between the grade of neutropenia and TTF. Other clinical responses, including OS rate at one-year, ORR, and DCR, also tended to be better in patients with severe neutropenia than in those without it. Therefore, severe neutropenia may be a surrogate marker for better survival outcome due to modified FOLFIRINOX therapy in patients with advanced pancreatic cancer. Our data were generally consistent with a previous report that showed that patients with severe neutropenia after treatment with gemcitabine-containing chemotherapy for advanced pancreatic cancer had significantly longer OS than those without it [
19]. The survival effect of gemcitabine monotherapy for metastatic pancreatic cancer is better for patients with grade 3 neutropenia than those with lower grades of neutropenia [
20].
A question that the present findings raises is: why dose the incidence of severe neutropenia yielded better survival in advanced pancreatic cancer patients receiving modified FOLFIRINOX therapy? One mechanism underlying this finding might be suppression of neutrophils themselves because these cells play a critical role in growth of tumors by promoting the acceleration of angiogenesis and suppressing the antitumor immune response [
21,
22]. An increase in neutrophils, which reflects systemic inflammation, might promote tumor progression by providing an advantageous environment for invasion and promotion of pancreatic cancer cells. Several studies have revealed that low neutrophil-to-lymphocyte ratio is a good predictor of prognosis in patients with pancreatic cancer [
23,
24]. Whether modified FOLFIRINOX therapy can also decrease the infiltration of neutrophils in pancreatic tumor tissue in patients with neutropenia should be examined in future studies.
We also presume that myelosuppression occurring in severe neutropenic patients contributes to improve the prognosis of the patients. Myeloid-derived suppressor cells (MDSCs), which reveal immunosuppressive in tumor microenvironment via inhibition of CD4+ T cell proliferation [
25], accumulate in tumor cells and peripheral blood as the disease is progressed or in advanced stages of pancreatic cancer [
26,
27,
28,
29,
30]. Reducing the number of MDSCs is a key antitumor mechanisms of some chemotherapy agents, including 5-FU [
31], which prevents the accumulation of MDSCs in patients with pancreatic cancer [
32]. Taken together, these evidence suggest that the suppressive effect of 5-FU included in FOLFIRINOX regimen on MDSCs in tumor microenvironment is more potent in patients with severe neutropenia than in those without it, where it may act to recover the cytotoxic action of T lymphocytes and prolong survival. Unfortunately, the precise mechanism underlying the 5-FU-induced reduction in the number of MDSC is unknown. Vincent et al. [
31] showed that 5-FU induces apoptotic death of MDSCs by activating caspase-3 and caspase-7, and this effect of 5-FU is more potent than that of gemcitabine. They also showed that the suppressive action of 5-FU is more potent as the expression of thymidylate synthase decreases. Therefore, 5-FU in FOLFIRINOX may contribute, at least in part, to reducing the number of MDSCs induced by FOLFIRINOX. Moreover, the reduction in MDSCs may be more potent in patients with severe neutropenia than in those without severe neutropenia due to the more severely depressed thymidylate synthase activity in patients with severe neutropenia.
We found that total bilirubin level was a significant risk factor for severe neutropenia. This suggests that the biological activity of cytotoxic drugs, including irinotecan, is increased in patients with severe neutropenia because elevated bilirubin has critical effects on metabolism of such drugs [
33]. Moreover, patients with severe neutropenia may have a genetic predisposition for drug metabolism that is similar to clinical course features [
34]. Although the RDIs for irinotecan, oxaliplatin and 5-FU were lower in patients with severe neutropenia, these doses may still exert antitumor effects. Further biological activity and/or blood concentration of cytotoxic agents may be relatively higher in severe neutropenic patients; however, future studies are needed to evaluate these hypotheses.




{kind=link}
{kind=link}