Pharmacokinetics of Sublingually Delivered Fentanyl in Head and Neck Cancer Patients Treated with Curatively Aimed Chemo or Bioradiotherapy


Abstract
:1. Introduction
2. Results
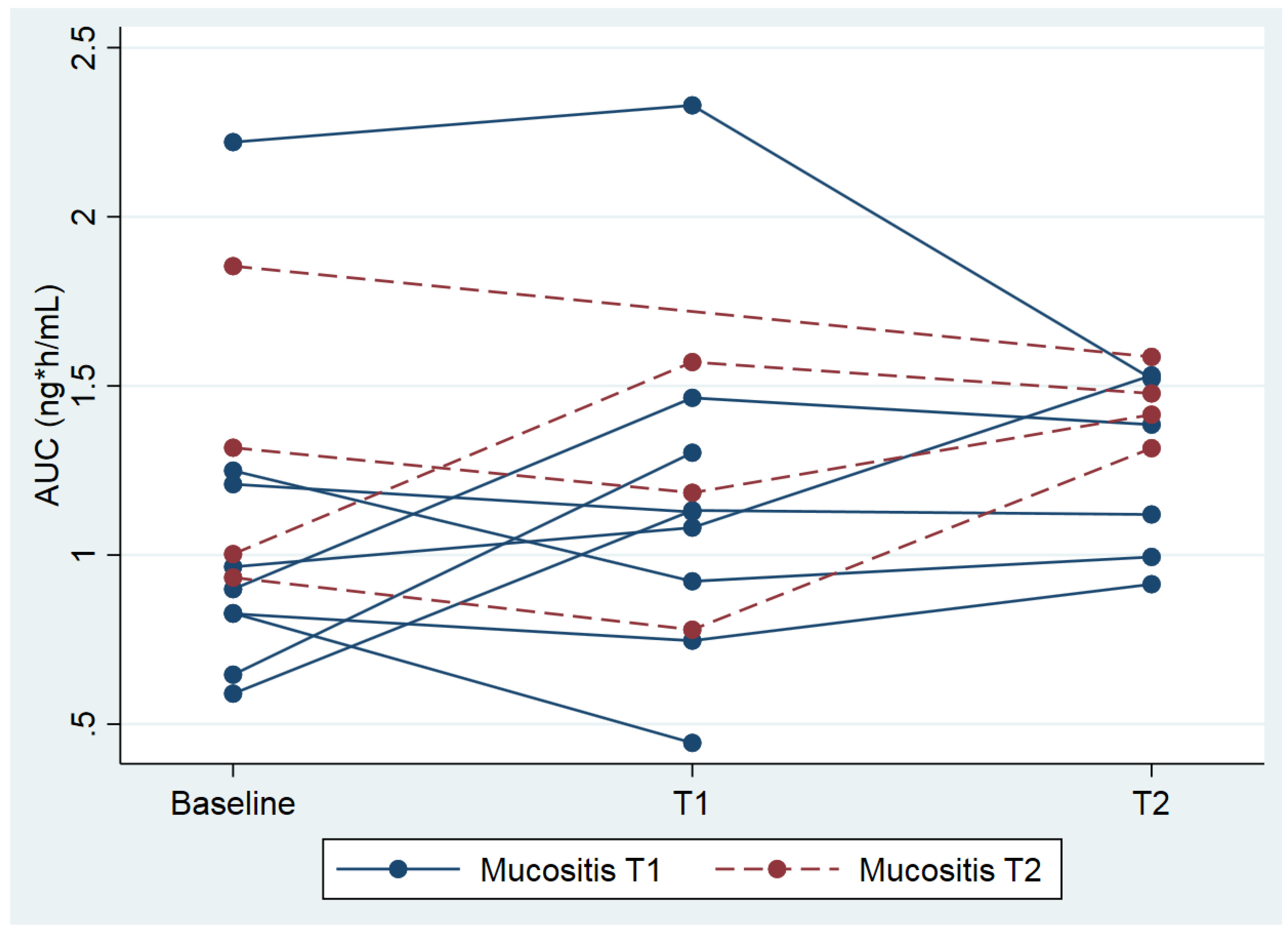
2.1. Analyses for Mucositis
2.2. Analyses for Xerostomia
2.3. Analysis of Pain
2.4. General Toxicity
3. Discussion
4. Methods
4.1. Patients
4.2. Study Design
4.3. Blood Sampling and Measurement of Fentanyl Concentrations
4.4. Clinical Assessments
4.5. Statistical Considerations
4.5.1. Sample Size Calculation
4.5.2. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Forastiere, A.A.; Goepfert, H.; Maor, M.; Pajak, T.F.; Weber, R.; Morrison, W.; Glisson, B.; Trotti, A.; Ridge, J.A.; Chao, C.; et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N. Engl. J. Med. 2003, 349, 2091–2098. [Google Scholar] [CrossRef] [PubMed]
- Forastiere, A.A.; Trotti, A. Radiotherapy and concurrent chemotherapy: A strategy that improves locoregional control and survival in oropharyngeal cancer. J. Natl. Cancer Inst. 1999, 91, 2065–2066. [Google Scholar] [CrossRef] [PubMed]
- Bonner, J.A.; Harari, P.M.; Giralt, J.; Azarnia, N.; Shin, D.M.; Cohen, R.B.; Jones, C.U.; Sur, R.; Raben, D.; Jassem, J.; et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2006, 354, 567–578. [Google Scholar] [CrossRef] [PubMed]
- Wong, P.C.; Dodd, M.J.; Miaskowski, C.; Paul, S.M.; Bank, K.A.; Shiba, G.H.; Facione, N. Mucositis pain induced by radiation therapy: Prevalence, severity, and use of self-care behaviors. J. Pain Symptom Manag. 2006, 32, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Epstein, J.B.; Thariat, J.; Bensadoun, R.J.; Barasch, A.; Murphy, B.A.; Kolnick, L.; Popplewell, L.; Maghami, E. Oral complications of cancer and cancer therapy: From cancer treatment to survivorship. CA Cancer J. Clin. 2012, 62, 400–422. [Google Scholar] [CrossRef] [PubMed]
- Services UDoHaH. Common Terminology Criteria for Adverse Events (CTCAE) Version 4.03; National Institute of Healt (NIH) Publication No. 09-5410; National Cancer Institute: Bethesda, MD, USA, 14 June 2010.
- Trotti, A.; Bellm, L.A.; Epstein, J.B.; Frame, D.; Fuchs, H.J.; Gwede, C.K.; Komaroff, E.; Nalysnyk, L.; Zilberberg, M. Mucositis incidence, severity and associated outcomes in patients with head and neck cancer receiving radiotherapy with or without chemotherapy: A systematic literature review. Radiother. Oncol. 2003, 66, 253–262. [Google Scholar] [CrossRef]
- Narayan, S.; Lehmann, J.; Coleman, M.A.; Vaughan, A.; Yang, C.C.; Enepekides, D.; Farwell, G.; Purdy, J.A.; Laredo, G.; Nolan, K.; et al. Prospective evaluation to establish a dose response for clinical oral mucositis in patients undergoing head-and-neck conformal radiotherapy. Int. J. Radiat. Oncol. 2008, 72, 756–762. [Google Scholar] [CrossRef] [PubMed]
- Napenas, J.J.; Shetty, K.V.; Streckfus, C.F. Oral mucositis: Review of pathogenesis, diagnosis, prevention, and management. Gen. Dent. 2007, 55, 335–344. [Google Scholar] [PubMed]
- Clarkson, J.E.; Worthington, H.V.; Furness, S.; McCabe, M.; Khalid, T.; Meyer, S. Interventions for treating oral mucositis for patients with cancer receiving treatment. Cochrane Database Syst. Rev. 2010, 8, CD001973. [Google Scholar] [CrossRef] [PubMed]
- Ling, I.S.; Larsson, B. Individualized pharmacological treatment of oral mucositis pain in patients with head and neck cancer receiving radiotherapy. Support Care Cancer 2011, 19, 1343–1350. [Google Scholar] [CrossRef] [PubMed]
- Menten, J.; Carpentier, I.; Deschutter, H.; Nuyts, S.; Van Beek, K. The use of transdermal buprenorphine to relieve radiotherapy-related pain in head and neck cancer patients. Cancer Investig. 2013, 31, 412–420. [Google Scholar] [CrossRef] [PubMed]
- Portenoy, R.K.; Lesage, P. Management of cancer pain. Lancet 1999, 353, 1695–1700. [Google Scholar] [CrossRef]
- Simon, S.M.; Schwartzberg, L.S. A review of rapid-onset opioids for breakthrough pain in patients with cancer. J. Opioid. Manag. 2014, 10, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Jandhyala, R.; Fullarton, J.R.; Bennett, M.I. Efficacy of rapid-onset oral fentanyl formulations vs. oral morphine for cancer-related breakthrough pain: A meta-analysis of comparative trials. J. Pain Symptom Manag. 2013, 46, 573–580. [Google Scholar]
- Mercadante, S.; Prestia, G.; Casuccio, A. The use of sublingual fentanyl for breakthrough pain by using doses proportional to opioid basal regimen. Curr. Med. Res. Opin. 2013, 29, 1527–1532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lennernas, B.; Frank-Lissbrant, I.; Lennernas, H.; Kalkner, K.M.; Derrick, R.; Howell, J. Sublingual administration of fentanyl to cancer patients is an effective treatment for breakthrough pain: Results from a randomized phase II study. Palliat. Med. 2010, 24, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Lennernas, B.; Hedner, T.; Holmberg, M.; Bredenberg, S.; Nystrom, C.; Lennernas, H. Pharmacokinetics and tolerability of different doses of fentanyl following sublingual administration of a rapidly dissolving tablet to cancer patients: A new approach to treatment of incident pain. Br. J. Clin. Pharmacol. 2005, 59, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Lister, N.; Warrington, S.; Boyce, M.; Eriksson, C.; Tamaoka, M.; Kilborn, J. Pharmacokinetics, Safety, and Tolerability of Ascending Doses of Sublingual Fentanyl, With and Without Naltrexone, in Japanese Subjects. J. Clin. Pharmacol. 2011, 51, 1195–1204. [Google Scholar] [CrossRef] [PubMed]
- Kuip, E.J.; Zandvliet, M.L.; Koolen, S.L.; Mathijssen, R.H.; van der Rijt, C.C. A review of factors explaining variability in fentanyl pharmacokinetics; focus on implications for cancer patients. Br. J. Clin. Pharmacol. 2017, 83, 294–313. [Google Scholar] [CrossRef] [PubMed]
- Darwish, M.; Kirby, M.; Robertson, P.; Tracewell, W.; Jiang, J.G. Absorption of fentanyl from fentanyl buccal tablet in cancer patients with or without oral mucositis—A. pilot study. Clin. Drug Investig. 2007, 27, 605–611. [Google Scholar] [CrossRef] [PubMed]
- Finn, A.; Hill, W.I.T.; Gever, L.N. Absorption and tolerability of fentanyl buccal soluble film (FBSF) in patients with cancer in the presence of oral mucositis. J. Pain Res. 2011, 4, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Braam, P.M.; Roesink, J.M.; Raaijmakers, C.P.J.; Busschers, W.B.; Terhaard, C.H.J. Quality of life and salivary output in patients with head-and-neck cancer five years after radiotherapy. Radiat. Oncol. 2007, 2, 3. [Google Scholar] [CrossRef] [PubMed]
- Le, Q.T.; Kim, H.E.; Schneider, C.J.; Murakozy, G.; Skladowski, K.; Reinisch, S.; Chen, Y.; Hickey, M.; Mo, M.; Chen, M.-G.; et al. Palifermin Reduces Severe Mucositis in Definitive Chemoradiotherapy of Locally Advanced Head and Neck Cancer: A Randomized, Placebo-Controlled Study. J. Clin. Oncol. 2011, 29, 2808–2814. [Google Scholar] [CrossRef] [PubMed]
- Cawley, M.M.; Benson, L.M. Current trends in managing oral mucositis. Clin. J. Oncol. Nurs. 2005, 9, 584–592. [Google Scholar] [CrossRef] [PubMed]
- Raber-Durlacher, J.E.; Elad, S.; Barasch, A. Oral mucositis. Oral Oncol. 2010, 46, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Scully, C.; Epstein, J.B. Oral health care for the cancer patient. Eur. J. Cancer B Oral Oncol. 1996, 32B, 281–292. [Google Scholar] [CrossRef]
- Beetz, I.; Burlage, F.R.; Bijl, H.P.; Hoegen-Chouvalova, O.; Christianen, M.E.M.C.; Vissink, A.; van der Laan, B.F.A.M.; de Bock, G.H.; Langendijk, J.A. The Groningen Radiotherapy-Induced Xerostomia questionnaire: Development and validation of a new questionnaire. Radiother. Oncol. 2010, 97, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Hu, M.H.; Wang, L.W.; Lu, H.J.; Chu, P.Y.; Tai, S.K.; Lee, T.L.; Chen, M.-H.; Yang, M.-H.; Chang, P.M.-H. Cisplatin-based chemotherapy versus cetuximab in concurrent chemoradiotherapy for locally advanced head and neck cancer treatment. Biomed. Res. Int. 2014, 2014, 904341. [Google Scholar] [CrossRef] [PubMed]
- Davies, A.; Mundin, G.; Vriens, J.; Webber, K.; Buchanan, A.; Waghorn, M. The Influence of Low Salivary Flow Rates on the Absorption of a Sublingual Fentanyl Citrate Formulation for Breakthrough Cancer Pain. J. Pain Symptom Manag. 2016, 51, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Guitart, J.; Vargas, M.I.; De Sanctis, V.; Folch, J.; Salazar, R.; Fuentes, J.; Coma, J.; Ferreras, J.; Moya, J.; Tomas, A.; et al. Efficacy and Safety of Sublingual Fentanyl Tablets in Breakthrough Cancer Pain Management According to Cancer Stage and Background Opioid Medication. Drugs R D 2018, 1–10. [Google Scholar] [CrossRef]
- Mercadante, S.; Adile, C.; Cuomo, A.; Aielli, F.; Marinangeli, F.; Casuccio, A. The use of low doses of a sublingual fentanyl formulation for breakthrough pain in patients receiving low doses of opioids. Support Care Cancer 2017, 25, 645–649. [Google Scholar] [CrossRef] [PubMed]
- De Bruijn, P.; Kuip, E.J.M.; Lam, M.H.; Mathijssen, R.H.J.; Koolen, S.L.W. Bioanalytical methods for the quantification of hydromorphone, fentanyl, norfentanyl, morphine, morphine-3ss-glucuronide and morphine-6ss-glucuronide in human plasma. J. Pharm. Biomed. Anal. 2018, 149, 475–481. [Google Scholar] [CrossRef] [PubMed]
- Farrar, J.T.; Young, J.P., Jr.; LaMoreaux, L.; Werth, J.L.; Poole, R.M. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Schoenfeld, D.A. Statistical Considerations for a Cross-Over Study. Available online: http://hedwig.mgh.harvard.edu/sample_size/quan_measur/cross_quant.html (accessed on 17 October 2012).



{kind=link}
{kind=link}
| Variable | Total N = 13 |
|---|---|
| Sex, n (%) | |
| Male | 11 |
| Female | 2 |
| Age, years (median and range) | 62 (48–72) |
| BMI (median and IQR) | 25.4 (22.8–26.9) |
| Tumor type | |
| oropharyngeal carcinoma | 4 |
| hypopharyngeal carcinoma | 4 |
| laryngeal carcinoma | 4 |
| combined oropharyngeal and laryngeal carcinoma | 1 |
| Concurrent to radiotherapy | |
| Cisplatin | 5 |
| Cetuximab | 8 |
| Laboratory results (median (IQR) (normal range) | |
| Creatinine (55–90 µL/min) | 79.0 (78.0–90.0) |
| MDRD (>60 mL/min/1.73 m2) | 82.5 (73.0–87.5) |
| AST (<31 U/L) | 24.5 (22.0–34.0) |
| ALT (<34 U/L) | 40.5 (21.0–48.0) |
| Bilirubin (<17 µmol/L) | 6.0 (5.0–7.0) |
| Albumin (35–50 g/L) | 41.5 (41.0–46.0) |
| ALP (<98 U/L) | 80.5 (62.0–100.0) |
| Radiotherapy Dose and Fentanyl AUC | Tbaseline | T1 | T2 | Tmucositis T1 n = 9 | Tmucositis T2 n = 4 |
|---|---|---|---|---|---|
| Radiotherapy dose sublingual in Gy (mean, SD) | - | 13.2 (6.7) | 28.2 (12.9) | 12.9 (4.4) | 40.1 (SD 13.7) |
| Radiotherapy dose total in Gy (mean SD) | - | 30.8 (6.2) | 55.6 (4.7) | 32.7 (6.7) | 54.3 (1.3) |
| Fentanyl AUC ng/mL*h geometric mean (CV %) | 1.04 (41.7) | 1.09 (40.6) | 1.31 (42.2) | x | x |
| GRIX Score | Baseline (n = 8) 0–100 | Tlast (n = 8) 0–100 |
|---|---|---|
| Day xerostomia Median (IQR) | 11.11 (0.00–22.22) | 38.89 (22.22–77.78) |
| Day sticky saliva Median (IQR) | 0.00 (0.00–11.11) | 27.78 (0.00–61.11) |
| Night xerostomia Median (IQR) | 22.22 (5.56–27.78) | 38.89 (33.33–66.67) |
| Night sticky saliva Median (IQR) | 0.00 (0.00–8.33) | 16.67 (0.00–66.67) |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuip, E.J.M.; Oldenmenger, W.H.; Oomen-de Hoop, E.; Verduijn, G.M.; Thijs-Visser, M.F.; De Bruijn, P.; Van Meerten, E.; Koolen, S.L.W.; Mathijssen, R.H.J.; Van der Rijt, C.C.D. Pharmacokinetics of Sublingually Delivered Fentanyl in Head and Neck Cancer Patients Treated with Curatively Aimed Chemo or Bioradiotherapy. Cancers 2018, 10, 445. https://doi.org/10.3390/cancers10110445
Kuip EJM, Oldenmenger WH, Oomen-de Hoop E, Verduijn GM, Thijs-Visser MF, De Bruijn P, Van Meerten E, Koolen SLW, Mathijssen RHJ, Van der Rijt CCD. Pharmacokinetics of Sublingually Delivered Fentanyl in Head and Neck Cancer Patients Treated with Curatively Aimed Chemo or Bioradiotherapy. Cancers. 2018; 10(11):445. https://doi.org/10.3390/cancers10110445
Chicago/Turabian StyleKuip, Evelien J. M., Wendy H. Oldenmenger, Esther Oomen-de Hoop, Gerda M. Verduijn, Martine F. Thijs-Visser, Peter De Bruijn, Esther Van Meerten, Stijn L. W. Koolen, Ron H. J. Mathijssen, and Carin C. D. Van der Rijt. 2018. "Pharmacokinetics of Sublingually Delivered Fentanyl in Head and Neck Cancer Patients Treated with Curatively Aimed Chemo or Bioradiotherapy" Cancers 10, no. 11: 445. https://doi.org/10.3390/cancers10110445