

A Microfluidic System for Detecting Tumor Cells Based on Biomarker Hexaminolevulinate (HAL): Applications in Pleural Effusion

Abstract
:1. Introduction
2. Materials and Methods
2.1. Cell Culture
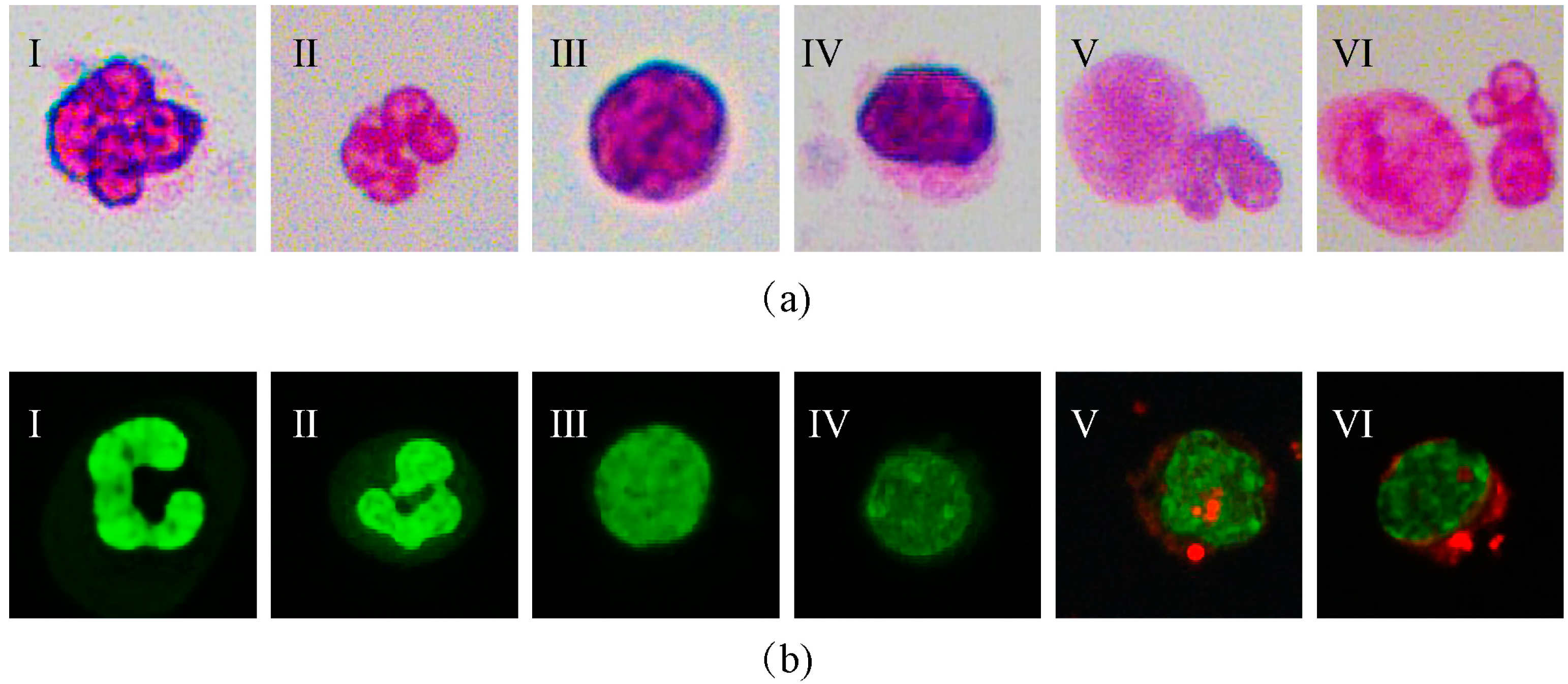
2.2. Wright–Giemsa Staining
2.3. HAL-Induced Fluorescence
2.3.1. HAL-Induced Fluorescence in Cultured Cells
2.3.2. HAL-Induced Fluorescence in Clinical Samples
2.4. Sorting Principle of Microfluidic Chip
2.5. Clinical Samples
3. Results
3.1. Generation of HAL-Induced Fluorescence in Tumor Cells
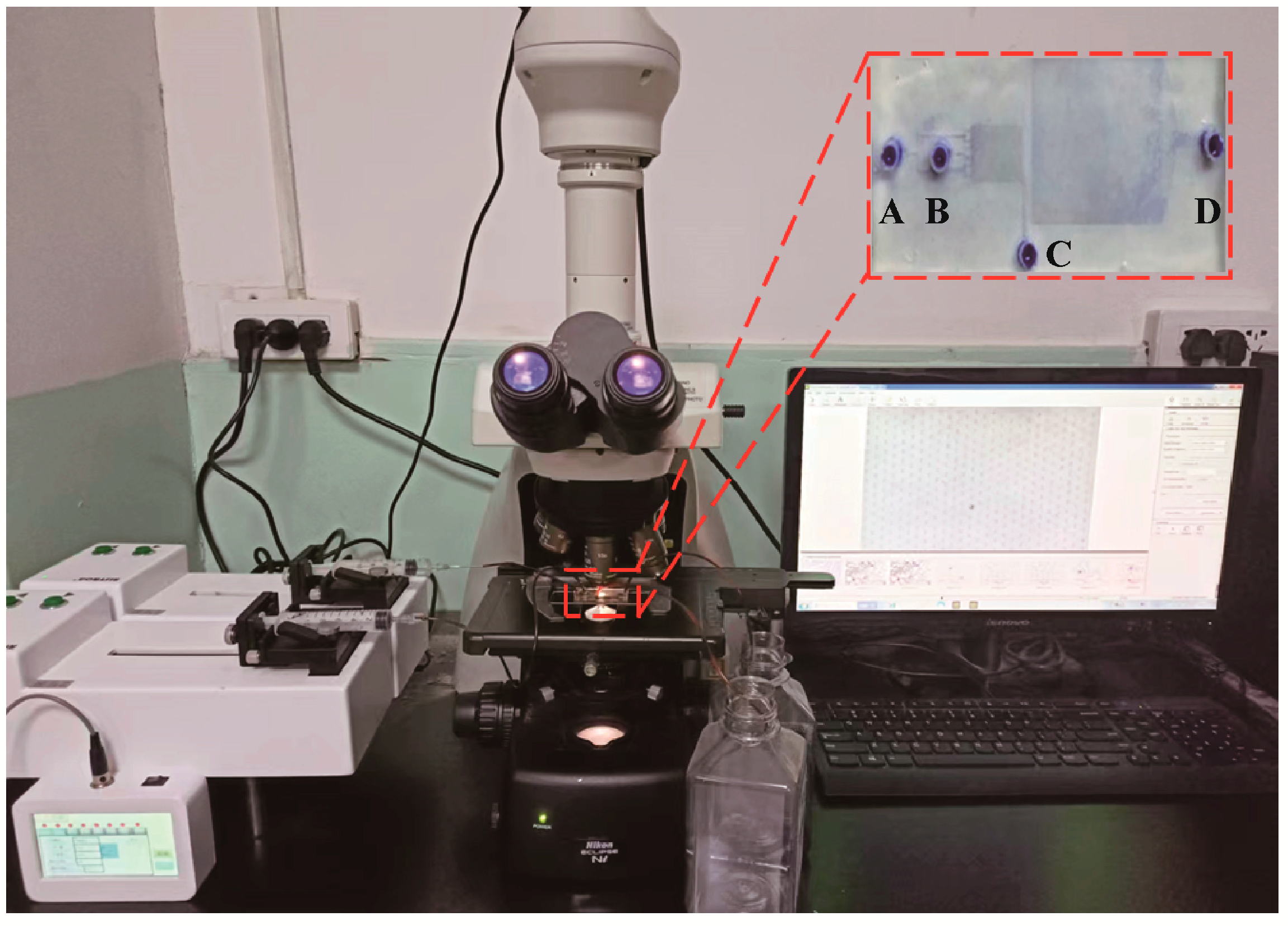
3.2. Construction of the Microfluidic System
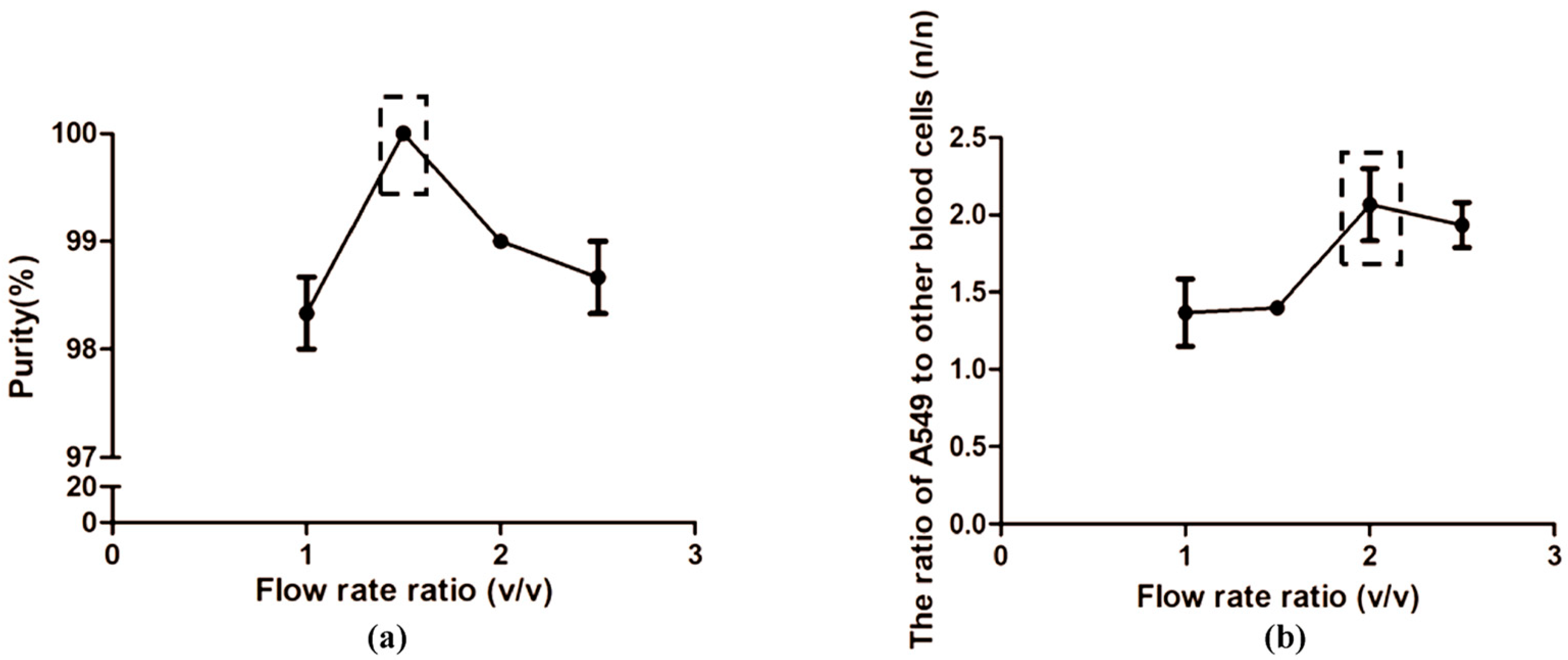
3.3. Optimization of the Flow Rates
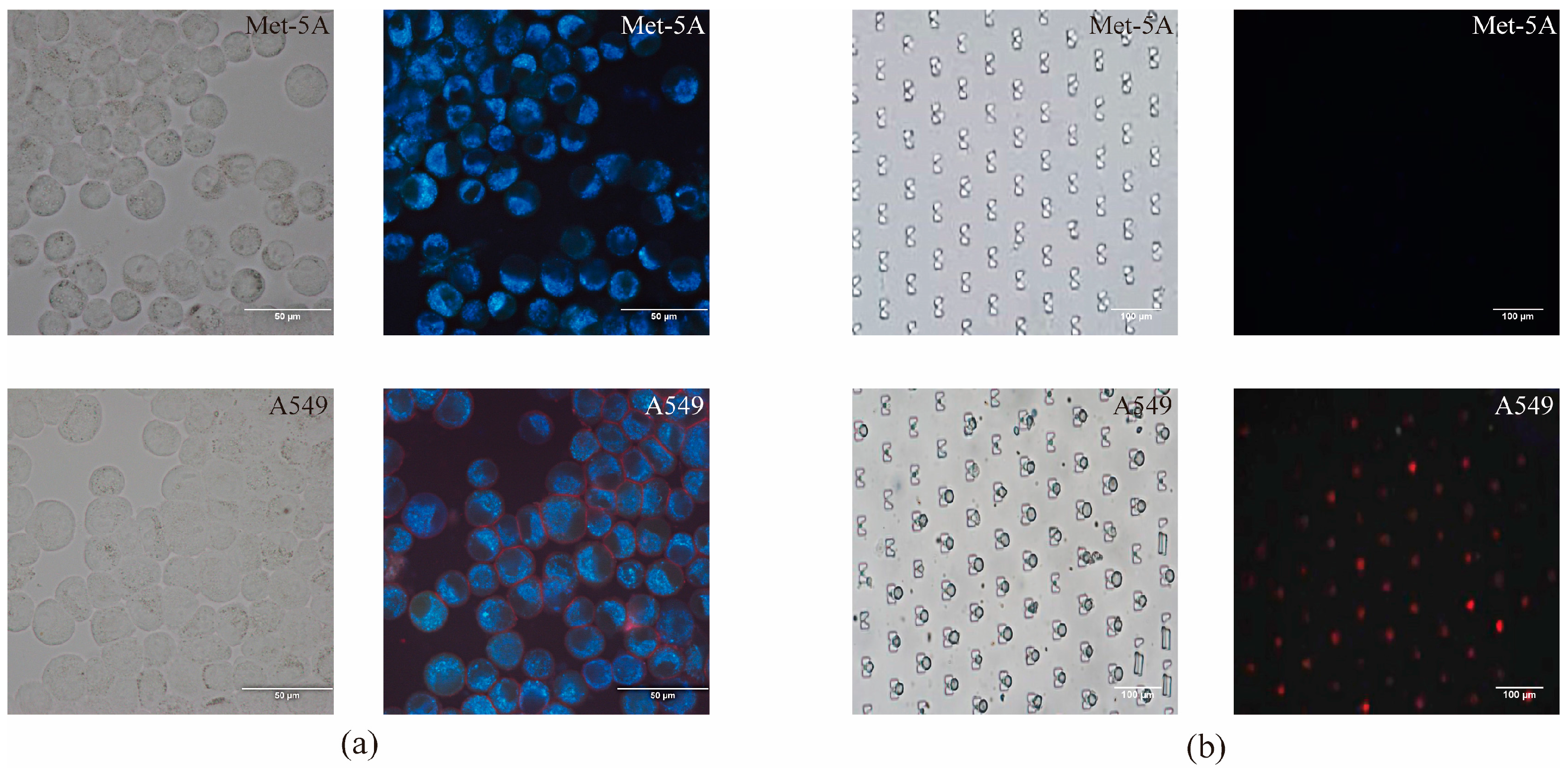
3.4. HAL Fluorescence Detection
3.5. Concentration Performance of the Microfluidic System
3.6. Validation of Clinical Sample
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kastelik, J.A. Management of malignant pleural effusion. Lung 2013, 191, 165–175. [Google Scholar] [CrossRef] [PubMed]
- Penz, E.; Watt, K.N.; Hergott, C.A.; Rahman, N.M.; Psallidas, I. Management of malignant pleural effusion: Challenges and solutions. Cancer Manag. Res. 2017, 9, 229–241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, J.X.; Shi, Y.M.; An, L.Y.; Yang, J.X.; Qi, Y.X.; Yang, T.; Cen, Y.Y.; Lin, Y.Y.; Sun, D.L. Quality assessment of the guidelines for the management of malignant pleural effusions and ascites. World J. Surg. Oncol. 2020, 18, 331. [Google Scholar] [CrossRef]
- Zhang, H.; Li, C.; Hu, F.; Zhang, X.; Shen, Y.; Chen, Y.; Li, F. Auxiliary diagnostic value of tumor biomarkers in pleural fluid for lung cancer-associated malignant pleural effusion. Respir. Res. 2020, 21, 284. [Google Scholar] [CrossRef] [PubMed]
- Ferreiro, L.; Suárez-Antelo, J.; Álvarez-Dobaño, J.M.; Toubes, M.E.; Riveiro, V.; Valdés, L. Malignant Pleural Effusion: Diagnosis and Management. Can. Respir. J. 2020, 2020, 2950751. [Google Scholar] [CrossRef]
- Chen, J.; Yang, Y.; Wang, Z.; Shen, X.; Zhang, Z.; Wang, C.; Xu, H.; Shi, Q. A Multicancer Malignant Pleural Effusion Diagnostic Test Using Hexokinase 2 and Single-Cell Sequencing. Clin. Chem. 2022, 68, 680–690. [Google Scholar] [CrossRef]
- Gayen, S. Malignant Pleural Effusion: Presentation, Diagnosis, and Management. Am. J. Med. 2022, 135, 1188–1192. [Google Scholar] [CrossRef]
- Porcel, J.M. Diagnosis and characterization of malignant effusions through pleural fluid cytological examination. Curr. Opin. Pulm. Med. 2019, 25, 362–368. [Google Scholar] [CrossRef]
- Win, K.Y.; Choomchuay, S.; Hamamoto, K.; Raveesunthornkiat, M.; Rangsirattanakul, L.; Pongsawat, S. Computer Aided Diagnosis System for Detection of Cancer Cells on Cytological Pleural Effusion Images. BioMed Res. Int. 2018, 2018, 6456724. [Google Scholar] [CrossRef]
- Wang, J.; Li, Y.; Wang, R.; Han, C.; Xu, S.; You, T.; Li, Y.; Xia, J.; Xu, X.; Wang, D.; et al. A Fully Automated and Integrated Microfluidic System for Efficient CTC Detection and Its Application in Hepatocellular Carcinoma Screening and Prognosis. ACS Appl. Mater. Interfaces 2021, 13, 30174–30186. [Google Scholar] [CrossRef]
- Rodríguez-Pena, A.; Armendariz, E.; Oyarbide, A.; Morales, X.; Ortiz-Espinosa, S.; Ruiz-Fernández de Córdoba, B.; Cochonneau, D.; Cornago, I.; Heymann, D.; Argemi, J.; et al. Design and validation of a tunable inertial microfluidic system for the efficient enrichment of circulating tumor cells in blood. Bioeng. Transl. Med. 2022, 7, e10331. [Google Scholar] [CrossRef]
- Abdulla, A.; Zhang, Z.; Ahmad, K.Z.; Warden, A.R.; Li, H.; Ding, X. Rapid and efficient capturing of circulating tumor cells from breast cancer Patient’s whole blood via the antibody functionalized microfluidic (AFM) chip. Biosens. Bioelectron. 2022, 201, 113965. [Google Scholar] [CrossRef]
- Lv, S.; Yu, J.; Zhao, Y.; Li, H.; Zheng, F.; Liu, N.; Li, D.; Sun, X. A Microfluidic Detection System for Bladder Cancer Tumor Cells. Micromachines 2019, 10, 871. [Google Scholar] [CrossRef] [Green Version]
- Gao, F.; Wang, J.; Yu, Y.; Yan, J.; Ding, G. Comprehensive optimization of urinary exfoliated tumor cells tests in bladder cancer with a promising microfluidic platform. Cancer Med. 2022. [Google Scholar] [CrossRef]
- Carvalho, S.; Abreu, C.M.; Ferreira, D.; Lima, L.; Ferreira, J.A.; Santos, L.L.; Ribeiro, R.; Grenha, V.; Martínez-Fernández, M.; Duenas, M.; et al. Phenotypic Analysis of Urothelial Exfoliated Cells in Bladder Cancer via Microfluidic Immunoassays: Sialyl-Tn as a Novel Biomarker in Liquid Biopsies. Front. Oncol. 2020, 10, 1774. [Google Scholar] [CrossRef] [PubMed]
- Si, H.; Du, D.; Li, W.; Li, Q.; Li, J.; Zhao, D.; Li, L.; Tang, B. Sputum-Based Tumor Fluid Biopsy: Isolation and High-Throughput Single-Cell Analysis of Exfoliated Tumor Cells for Lung Cancer Diagnosis. Anal. Chem. 2021, 93, 10477–10486. [Google Scholar] [CrossRef] [PubMed]
- Peterson, V.M.; Castro, C.M.; Chung, J.; Miller, N.C.; Ullal, A.V.; Castano, M.D.; Penson, R.T.; Lee, H.; Birrer, M.J.; Weissleder, R. Ascites analysis by a microfluidic chip allows tumor-cell profiling. Proc. Natl. Acad. Sci. USA 2013, 110, E4978–E4986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Zhao, J.; Yu, H.; Li, P.; Liang, W.; Liu, Z.; Lee, G.B.; Liu, L.; Li, W.J.; Wang, Z. Detection and isolation of free cancer cells from ascites and peritoneal lavages using optically induced electrokinetics (OEK). Sci. Adv. 2020, 6, eaba9628. [Google Scholar] [CrossRef]
- Che, J.; Mach, A.J.; Go, D.E.; Talati, I.; Ying, Y.; Rao, J.; Kulkarni, R.P.; Di Carlo, D. Microfluidic purification and concentration of malignant pleural effusions for improved molecular and cytomorphological diagnostics. PloS ONE 2013, 8, e78194. [Google Scholar] [CrossRef]
- Zhao, L.; Zhao, M.; Yang, Y.; Gu, Y.; Zheng, F.; Wang, X.; Zheng, Z.; Sun, X. Label-free microfluidic chip for the identification of mesothelial cell clusters in pleural effusion. Oncol. Lett. 2019, 17, 4532–4544. [Google Scholar] [CrossRef] [Green Version]
- Shi, X.; Tan, W.; Liu, L.; Cao, W.; Wang, Y.; Zhu, G. Separation of exfoliated tumor cells from viscoelastic pleural effusion using a microfluidic sandwich structure. Anal. Bioanal. Chem. 2020, 412, 5513–5523. [Google Scholar] [CrossRef]
- Tsou, P.H.; Chiang, P.H.; Lin, Z.T.; Yang, H.C.; Song, H.L.; Li, B.R. Rapid purification of lung cancer cells in pleural effusion through spiral microfluidic channels for diagnosis improvement. Lab Chip 2020, 20, 4007–4015. [Google Scholar] [CrossRef]
- Zhu, Z.; Li, S.; Wu, D.; Ren, H.; Ni, C.; Wang, C.; Xiang, N.; Ni, Z. High-throughput and label-free enrichment of malignant tumor cells and clusters from pleural and peritoneal effusions using inertial microfluidics. Lab Chip 2022, 22, 2097–2106. [Google Scholar] [CrossRef] [PubMed]
- Pikin, O.; Filonenko, E.; Mironenko, D.; Vursol, D.; Amiraliev, A. Fluorescence thoracoscopy in the detection of pleural malignancy. Eur. J. Cardio-Thorac. Surg. 2012, 41, 649–652. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, S.; Fukuhara, H.; Seki, H.; Kawada, C.; Nakayama, T.; Karashima, T.; Ogura, S.I.; Inoue, K. Predictors of therapeutic efficacy of 5-aminolevulinic acid-based photodynamic therapy in human prostate cancer. Photodiagnosis Photodyn. Ther. 2021, 35, 102452. [Google Scholar] [CrossRef]
- Wang, T.; Guo, Y.; He, Y.; Ren, T.; Yin, L.; Fawcett, J.P.; Gu, J.; Sun, H. Impact of molecular weight on the mechanism of cellular uptake of polyethylene glycols (PEGs) with particular reference to P-glycoprotein. Acta Pharm. Sin. B 2020, 10, 2002–2009. [Google Scholar] [CrossRef]
- Li, Z.; Jiang, L.; Chew, S.H.; Hirayama, T.; Sekido, Y.; Toyokuni, S. Carbonic anhydrase 9 confers resistance to ferroptosis/apoptosis in malignant mesothelioma under hypoxia. Redox Biol 2019, 26, 101297. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.M.; Vasilev, K.; Shirazi, H.S.; McNicholas, K.; Li, J.; Gleadle, J.; MacGregor, M. Biosensor device for the photo-specific detection of immuno-captured bladder cancer cells using hexaminolevulinate: An ex-vivo study. Photodiagnosis Photodyn. Ther. 2019, 28, 238–247. [Google Scholar] [CrossRef]
- Noppen, M.; De Waele, M.; Li, R.; Gucht, K.V.; D’Haese, J.; Gerlo, E.; Vincken, W. Volume and cellular content of normal pleural fluid in humans examined by pleural lavage. Am. J. Respir. Crit. Care Med. 2000, 162, 1023–1026. [Google Scholar] [CrossRef]
- Awadallah, S.F.; Bowling, M.R.; Sharma, N.; Mohan, A. Malignant pleural effusion and cancer of unknown primary site: A review of literature. Ann. Transl. Med. 2019, 7, 353. [Google Scholar] [CrossRef]
- Ali, A.H.; Takizawa, H.; Kondo, K.; Matsuoka, H.; Toba, H.; Nakagawa, Y.; Kenzaki, K.; Sakiyama, S.; Kakiuchi, S.; Sekido, Y.; et al. 5-Aminolevulinic acid-induced fluorescence diagnosis of pleural malignant tumor. Lung Cancer 2011, 74, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.W.; Yow, C.M.; Wong, C.K.; Lam, Y.H. Photodynamic therapy (PDT)—Initiation of apoptosis via activation of stress-activated p38 MAPK and JNK signal pathway in H460 cell lines. Photodiagnosis Photodyn. Ther. 2011, 8, 254–263. [Google Scholar] [CrossRef]
- Chung, C.W.; Kim, C.H.; Lee, H.M.; Kim, D.H.; Kwak, T.W.; Chung, K.D.; Jeong, Y.I.; Kang, D.H. Aminolevulinic acid derivatives-based photodynamic therapy in human intra- and extrahepatic cholangiocarcinoma cells. Eur. J. Pharm. Biopharm. 2013, 85, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Cunderlíková, B.; Wahlqvist, R.; Berner, A.; Vasovic, V.; Warloe, T.; Nesland, J.M.; Peng, Q. Detection of urinary bladder cancer with flow cytometry and hexaminolevulinate in urine samples. Cytopathology 2007, 18, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.M.; Vasilev, K.; MacGregor, M. Effects of Supplemental Drugs on Hexaminolevulinate (HAL)-Induced PpIX Fluorescence in Bladder Cancer Cell Suspensions. Int. J. Mol. Sci. 2022, 23, 7631. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Before Concentration | After Concentration | |||
|---|---|---|---|---|
| A549 (%) | RBC (%) | A549 (%) | RBC (%) | |
| Proportion | 28.04 ± 3.96 | 71.96 ± 3.96 | 70.01 ± 9.36 | 29.99 ± 9.36 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luan, Y.; Li, L.; Xun, X.; Wang, Y.; Wei, X.; Zheng, Y.; Fan, Z.; Sun, X. A Microfluidic System for Detecting Tumor Cells Based on Biomarker Hexaminolevulinate (HAL): Applications in Pleural Effusion. Micromachines 2023, 14, 771. https://doi.org/10.3390/mi14040771
Luan Y, Li L, Xun X, Wang Y, Wei X, Zheng Y, Fan Z, Sun X. A Microfluidic System for Detecting Tumor Cells Based on Biomarker Hexaminolevulinate (HAL): Applications in Pleural Effusion. Micromachines. 2023; 14(4):771. https://doi.org/10.3390/mi14040771
Chicago/Turabian StyleLuan, Yiran, Lei Li, Xiaoyi Xun, Yang Wang, Xinyue Wei, Yuqun Zheng, Zhijuan Fan, and Xuguo Sun. 2023. "A Microfluidic System for Detecting Tumor Cells Based on Biomarker Hexaminolevulinate (HAL): Applications in Pleural Effusion" Micromachines 14, no. 4: 771. https://doi.org/10.3390/mi14040771