
Development of an Assessment Model for the Effect of the Replacement of Minimal Artificial Ossicles on Hearing in the Inner Ear
Abstract
:1. Introduction
2. Materials and Methods
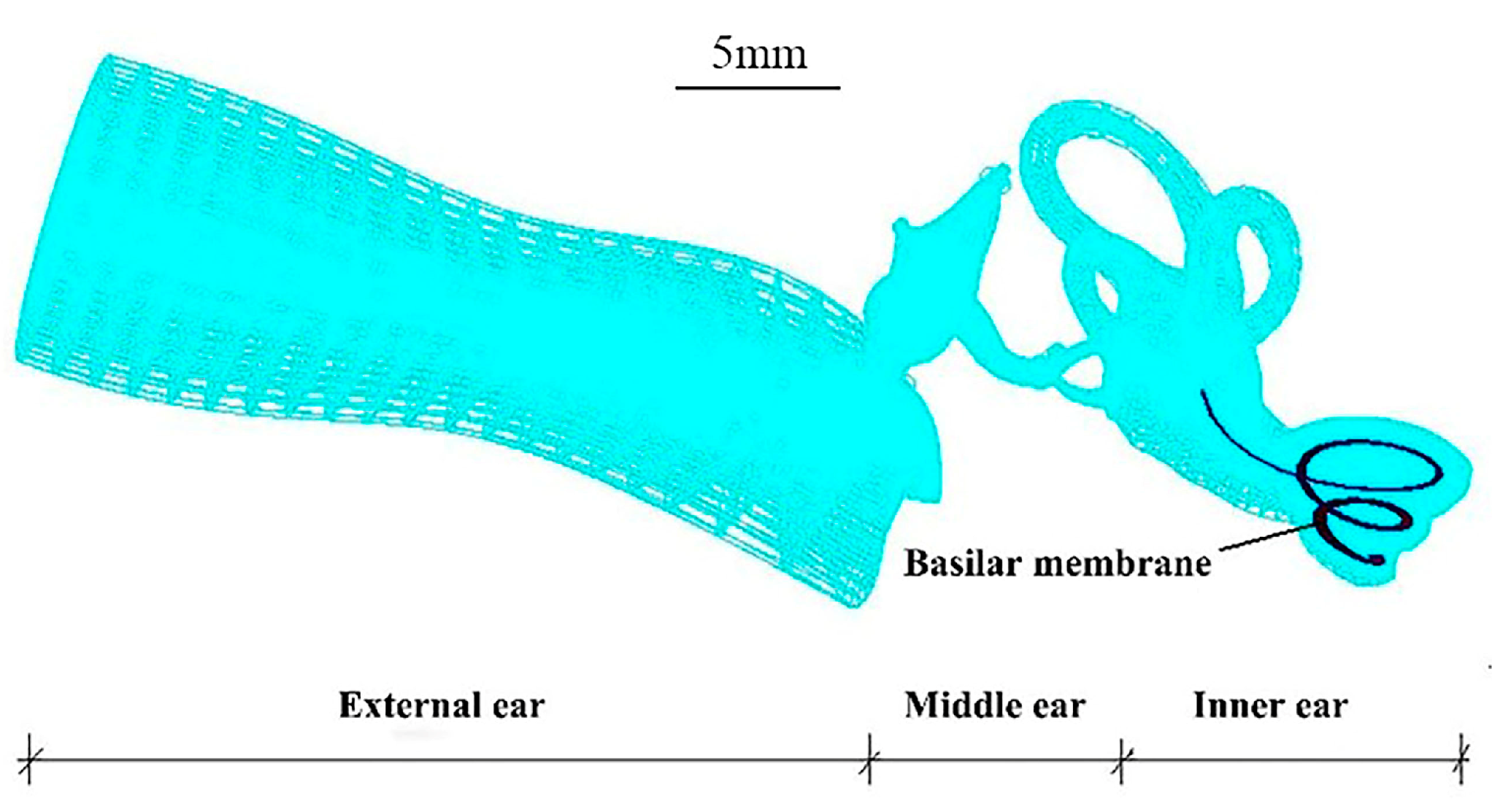
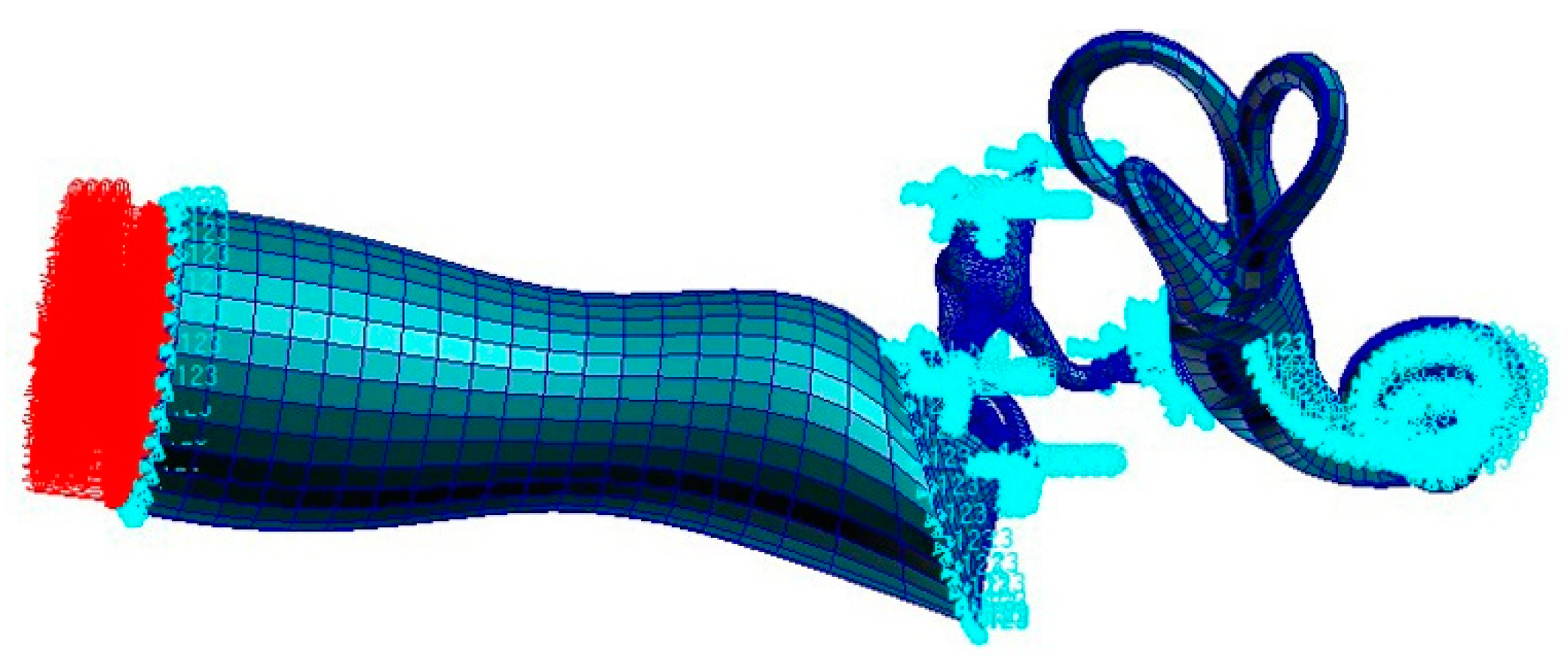
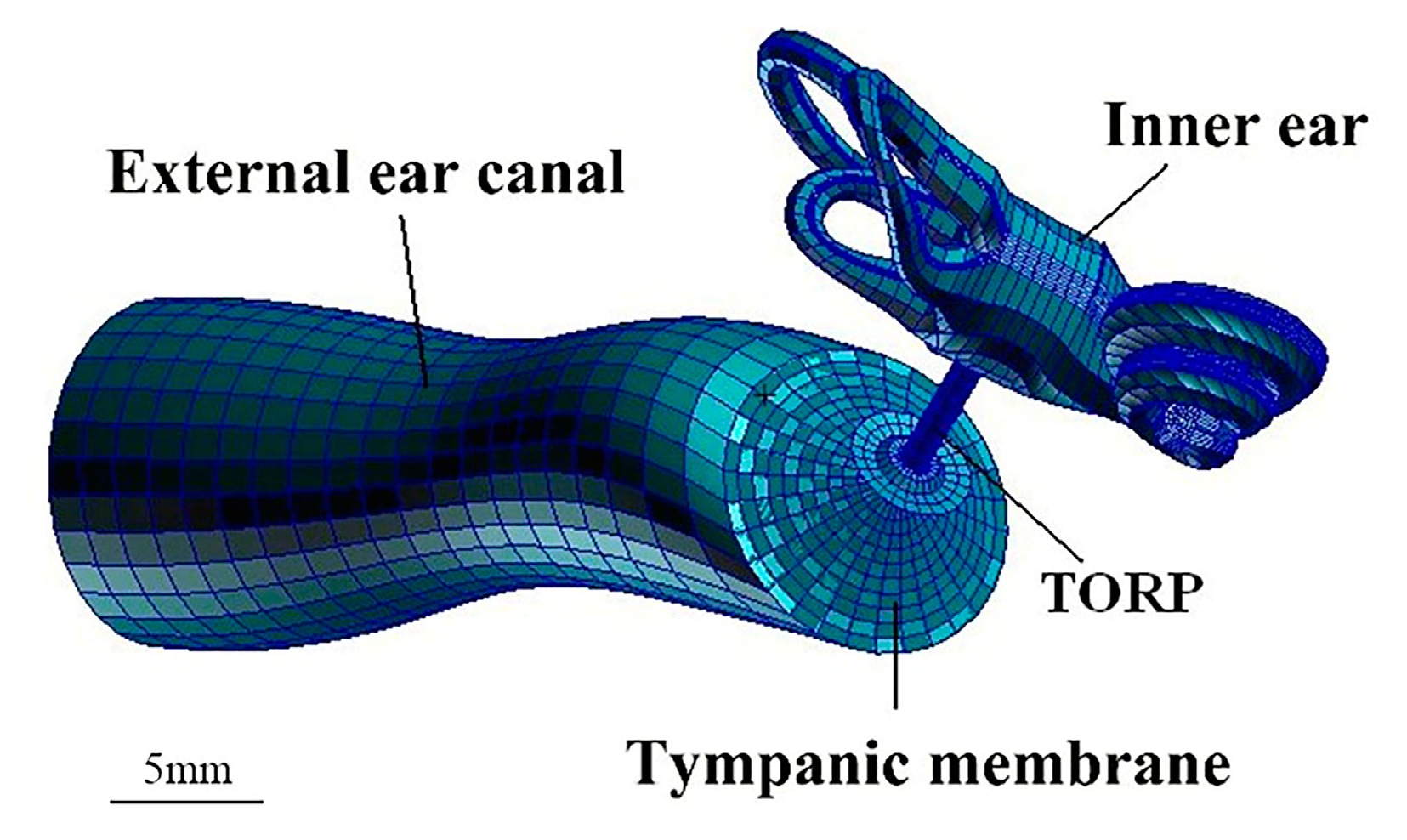
2.1. Establishment of an FE Model of the Human Ear
2.1.1. Establishment of the Model
2.1.2. Material Properties
2.1.3. Boundary Conditions of the Whole Ear FEM
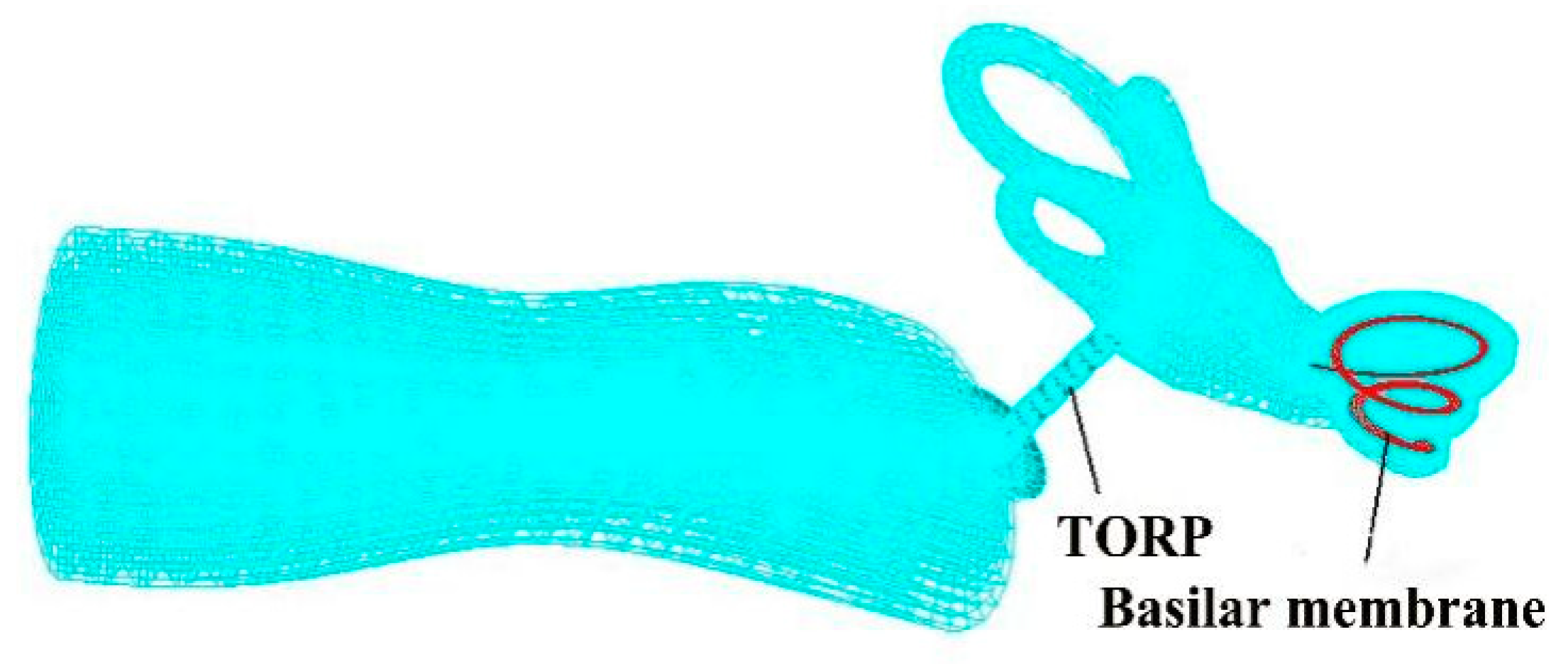
2.2. Establishment of the TORP Model
3. Results and Discussion
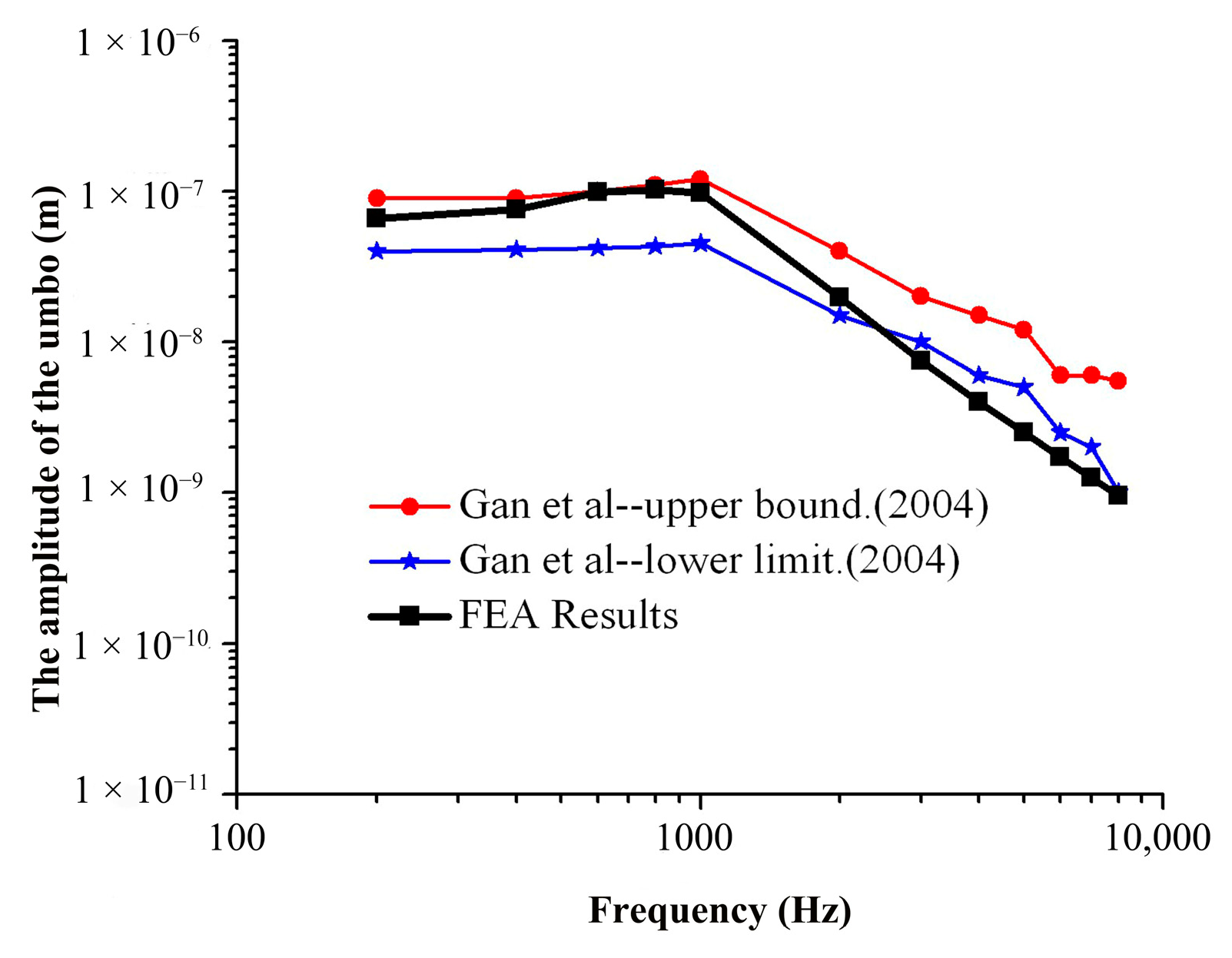
3.1. Verification of the FEM of the Human Ear
3.1.1. Load Acting on the TM
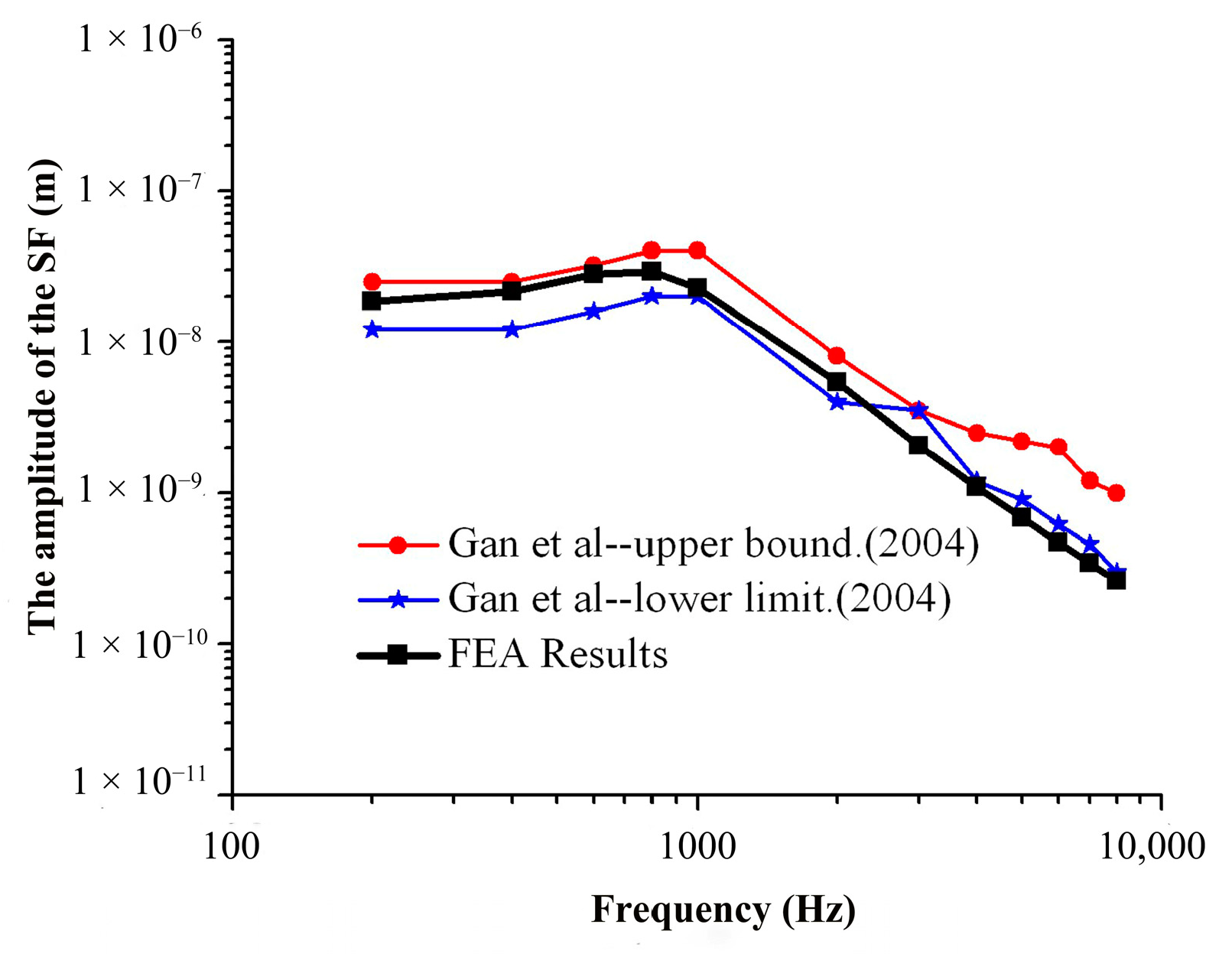
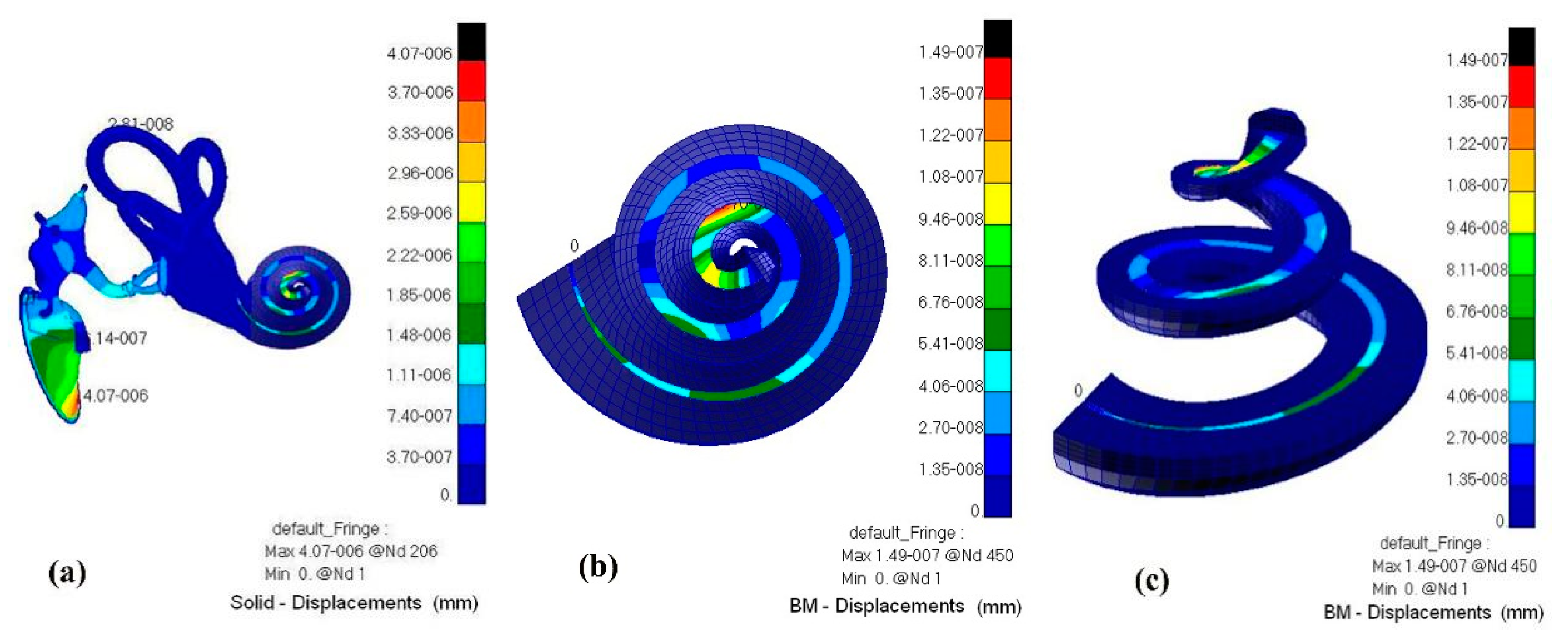
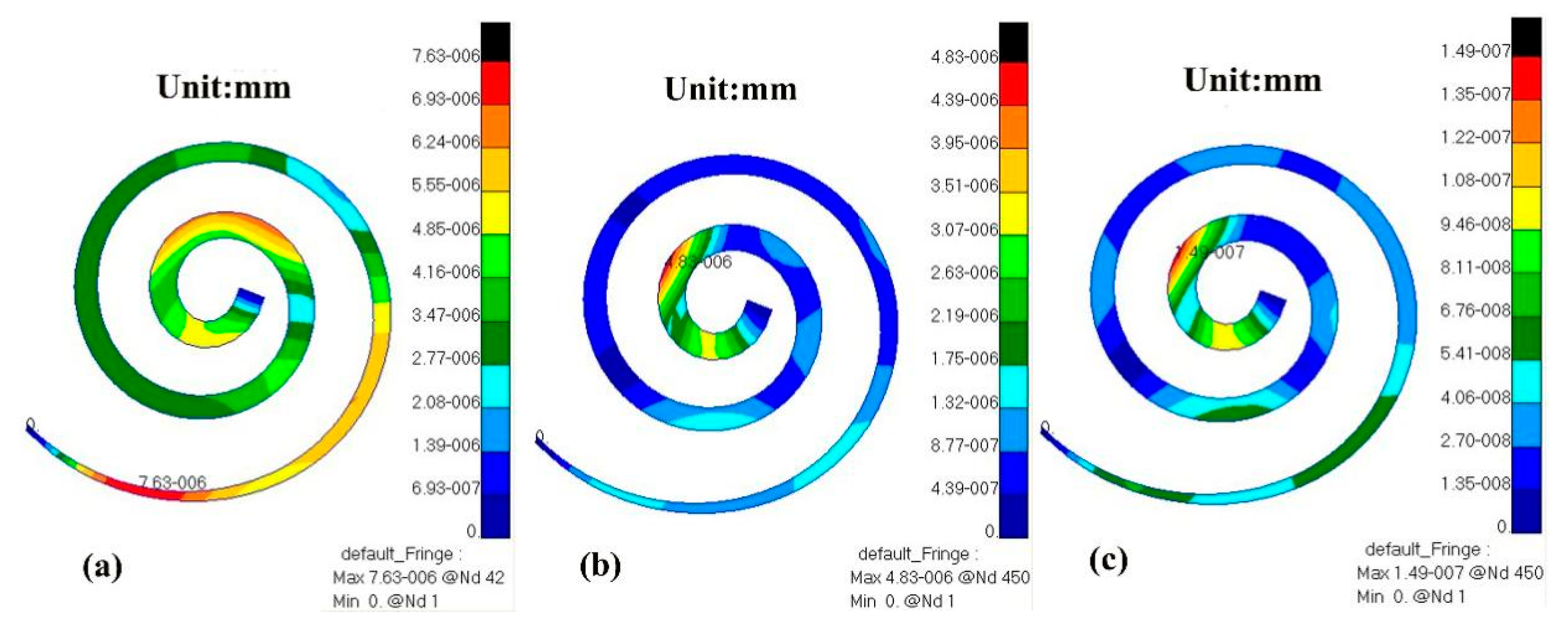
3.1.2. Verification of the FEM of the Spiral BM
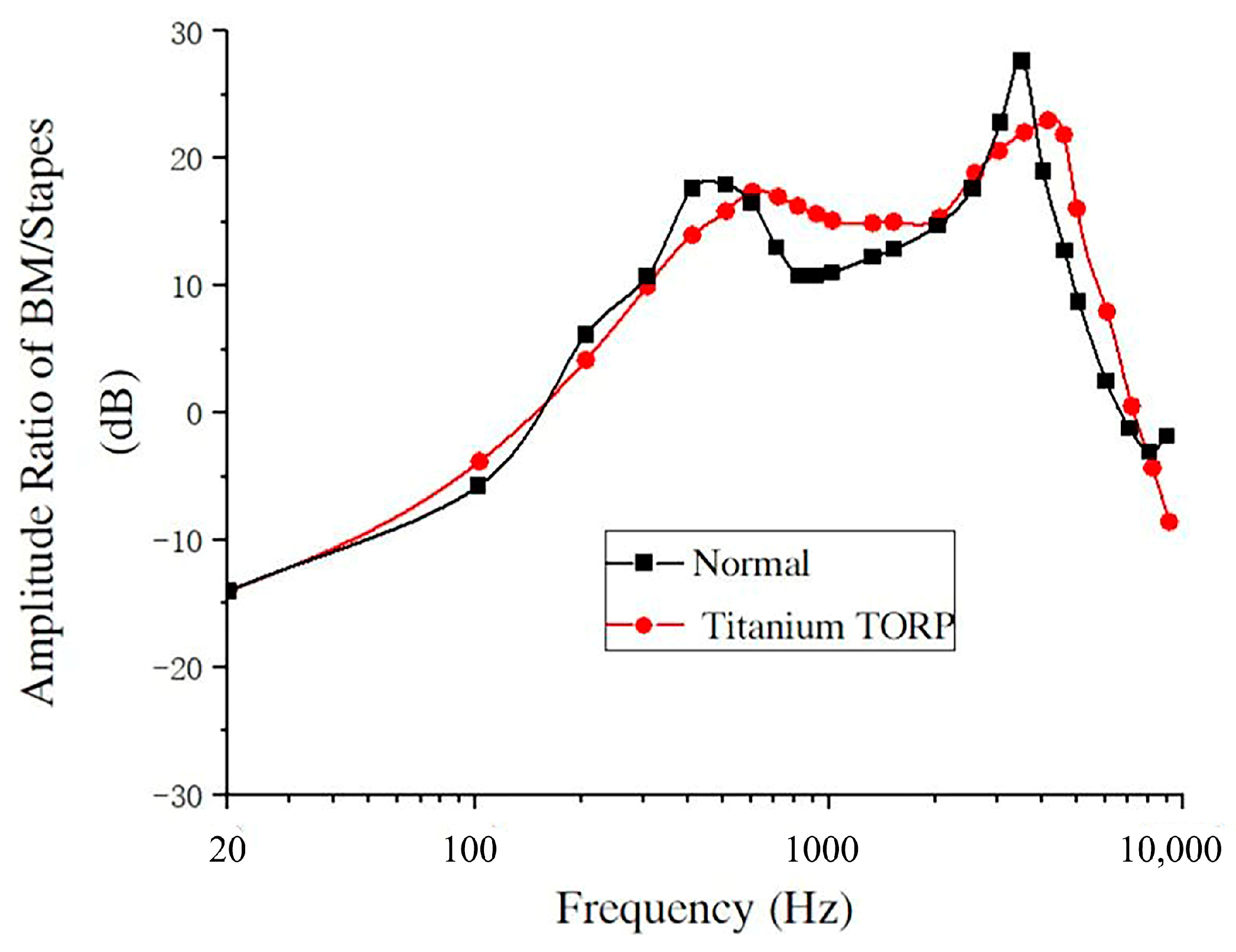
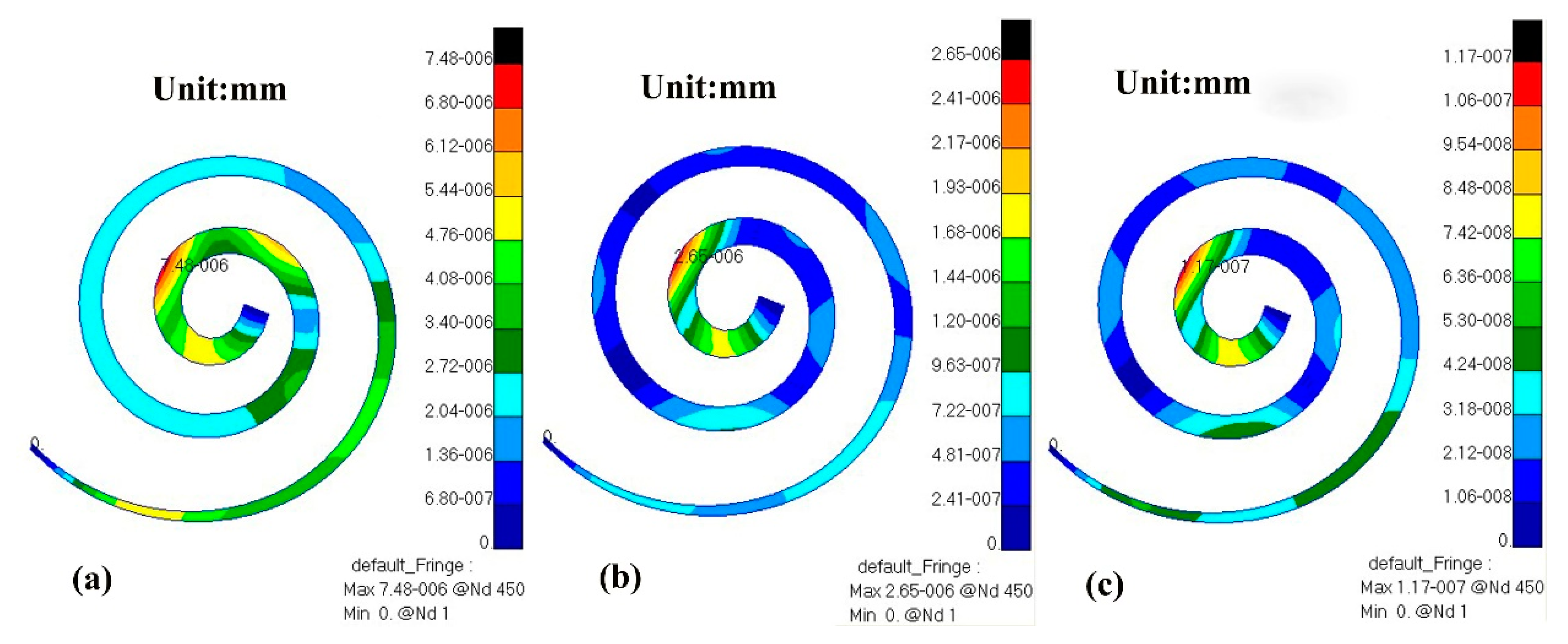
3.2. Numerical Analysis of the Vibration Characteristics of the BM after Replacement with a TORP
4. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Géléoc, G.S.; Holt, J.R. Sound strategies for hearing restoration. Science 2014, 344, 1241062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jia, S.; He, D.Z. Motility-associated hair-bundle motion in mammalian outer hair cells. Nat. Neurosci. 2005, 8, 1028–1034. [Google Scholar] [CrossRef] [PubMed]
- Murphy, T.P. Hearing Results in Pediatric Patients with Chronic Otitis Media After Ossicular Reconstruction with Partial Ossicular Replacement Prostheses and Total Ossicular Replacement Prostheses. Laryngoscope 2000, 110, 536–544. [Google Scholar] [CrossRef] [PubMed]
- Yao, W.; Guo, C.; Luo, X. Study on effects of partial ossicular replacement prostheses with different materials on hearing restoration. J. Mater. Sci. Mater. Med. 2013, 24, 515–522. [Google Scholar] [CrossRef]
- Kelly, D.J.; Prendergast, P.J.; Blayney, A.W. The Effect of Prosthesis Design on Vibration of the Reconstructed Ossicular Chain: A Comparative Finite Element Analysis of Four Prosthese. Otol. Neurotol. 2003, 24, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Marchese, M.R.; Cianfrone, F.; Passali, G.C.; Paludetti, G. Hearing results after stapedotomy: Role of the prosthesis diameter. Audiol. Neurootol. 2007, 12, 221–225. [Google Scholar] [CrossRef]
- Fisch, U.; May, J.; Linder, T.; Naumann, L.C. A New L-Shaped Titanium Prosthesis for Total Reconstruction of the Ossicular Chain. Otol. Neurotol. 2004, 25, 891–902. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, D.P.; Bance, M.; Vanwijhe, R.G.; Kiefte, M.; Smith, R. Optimum Tension for Partial Ossicular Replacement Prosthesis Reconstruction in the Human Middle Ear. Laryngoscope 2004, 114, 305–308. [Google Scholar] [CrossRef] [PubMed]
- Vincent, R.; Sperling, N.M.; Oates, J.; Osborne, J. Ossiculoplasty with Intact Stapes and Absent Malleus: The Silastic Banding Technique. Otol. Neurotol. 2005, 26, 846–852. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.; Xue, L.; Yang, J. Modeling the effect of cochlear windows activity on reverse stimulation under the role of physiological third windows. Appl. Acoust. 2020, 169, 107473. [Google Scholar] [CrossRef]
- Huttenbrink, K.B.; Beutner, D.; Zahnert, T. Clinical Results with an Active Middle Ear Implant in the Oval Window. Adv. Otorhinolaryngol. 2010, 69, 27–31. [Google Scholar] [PubMed] [Green Version]
- Gundersen, T.; Skarstein, O.; Sikkeland, T. A study of the vibration of the basilar membrane in human temporal bone preparations by the use of the mossbauer effect. Acta Otolaryngol. 1978, 86, 225–232. [Google Scholar] [CrossRef] [PubMed]
- Stenfelt, S.; Puria, S.; Hato, N.; Goode, R.L. Basilar membrane and osseous spiral lamina motion in human cadavers with air and bone conduction stimuli. Hear. Res. 2003, 181, 131–143. [Google Scholar] [CrossRef]
- Nakajima, H.H.; Merchant, S.N.; Rosowski, J.J. Performance considerations of prosthetic actuators for round-window stimulation. Hear. Res. 2010, 263, 114–119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, K.M.; Steele, C.R. Response suppression and transient behavior in a nonlinear active cochlear model with feed-forward. Int. J. Solids Struct. 2003, 40, 5097–5107. [Google Scholar] [CrossRef]
- Kim, N.; Homma, K.; Puria, S. Inertial Bone Conduction: Symmetric and Anti-Symmetric Components. J. Assoc. Res. Otolaryngol. 2011, 12, 261–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, W.; Liang, J.; Ren, L.; Ma, J.; Zhao, Z.; Wang, J.; Xie, Y.; Dai, P.; Zhang, T. Revealing the actions of the human cochlear basilar membrane at low frequency. Commun. Nonlinear. Sci. Numer. Simul. 2021, 104, 106043. [Google Scholar] [CrossRef]
- Yao, W.; Zhao, Z.; Wang, J.; Duan, M. Time-domain analysis of a three-dimensional numerical model of the human spiral cochlea at medium intensity. Comput. Biol. Med. 2021, 136, 104756. [Google Scholar] [CrossRef]
- Wada, H.; Metoki, T.; Kobayashi, T. Analysis of dynamic behavior of human middle ear using a finite-dement method. J. Acoust. Soc. Am. 1992, 92, 3157–3168. [Google Scholar] [CrossRef]
- Herrmann, G.; Liebowitz, H. Mechanics of bone fractures. In Fracture: An Advanced Treatise; Academic Press: New York, NY, USA, 1972; pp. 772–840. [Google Scholar]
- Kirikae, I. The Structure and Function of the Middle Ear; University of Tokyo Press: Tokyo, Japan, 1960. [Google Scholar]
- Békésy, G.V. Experiments in Hearing; McGraw-Hill: New York, NY, USA, 1960. [Google Scholar]
- Sun, Q.; Gan, R.Z.; Chang, H.K.; Dormer, K.J. Computer integrated finite element modeling of human middle ear. Biomech. Model. Mechanobiol. 2002, 1, 109–122. [Google Scholar] [CrossRef]
- Wada, H.; Koike, T.; Kobayashi, T. Three-dimensional finite element method (FEM) analysis of the human middle ear. In Research and Otosurgery: Proceedings of the International Workshop on Middle Ear Mechanics in Research and Otosurgery; Dresden University Press: Dresden, Germany, 1997; pp. 76–80. [Google Scholar]
- Gan, R.Z.; Sun, Q.; Dyer, R.K.; Chang, K.H.; Dormer, K.J. Three dimensional modeling of middle ear biomechanics and its application. Otol. Neurotol. 2002, 23, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Gan, R.Z.; Reeves, B.P.; Wang, X. Modeling of Sound Transmission from Ear Canal to Cochlea. Ann. Biomed. Eng. 2007, 35, 2180–2195. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Gan, R.Z. A Comprehensive Model of Human Ear for Analysis of Implantable Hearing Devices. IEEE Trans. Biomed. Eng. 2011, 58, 3024–3027. [Google Scholar] [CrossRef] [PubMed]
- Naidu, R.C.; Mountain, D.C. Longitudinal coupling within the basilar membrane, recticular liminae. In Recent Developments in Auditory Mechanics; World Scientific: Teaneck, NJ, USA, 2000; pp. 123–129. [Google Scholar]
- Gan, R.Z.; Feng, B.; Sun, Q. Three-Dimensional Finite Element Modeling of Human Ear for Sound Transmission. Ann. Biomed. Eng. 2004, 32, 847–859. [Google Scholar] [CrossRef]
- Gan, R.Z.; Wood, M.W.; Dormer, K.J. Human middle ear transfer function measured by double laser interferometry system. Otol. Neurotol. 2004, 25, 423–435. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Structure | Density (kg·m−3) | Published Data | Young’s Modulus (Pa) | Published Data |
|---|---|---|---|---|
| Malleus head | 2.55 × 103 | Kirikae et al. | 1.41 × 1010 | Herrmann et al. |
| Malleus neck | 4.53 × 103 | Kirikae et al. | 1.41 × 1010 | Herrmann et al. |
| Malleus handle | 3.70 × 103 | Kirikae et al. | 1.41 × 1010 | Herrmann et al. |
| Incus body | 2.36 × 103 | Kirikae et al. | 1.41 × 1010 | Herrmann et al. |
| Incus short process | 5.08 × 103 | Kirikae et al. | 1.41 × 1010 | Herrmann et al. |
| Incus long process | 2.26 × 103 | Kirikae et al. | 1.41 × 1010 | Herrmann et al. |
| Stapes | 2.2 × 103 | Kirikae et al. | 1.41 × 1010 | Herrmann et al. |
| Incudomalleolar joint | 3.2 × 103 | Sun et al. | 1.41 × 1010 | Sun et al. |
| Incudostapedial joint | 1.2 × 103 | Sun et al. | 0.6 × 106 | Wada et al. |
| TM (par tensa) | 1.2 × 103 | Wada et al. | 3.5 × 107 | 2.0 × 107 Bekesy et al. |
| TM (par flaccida) | 1.2 × 103 | Wada et al. | 1.0 × 107 | 4.0 × 107 Kirikae et al. |
| Soft Tissue | Young’s Modulus (MPa) | |
|---|---|---|
| FEM | Published Data | |
| Tympanic annulus ligament | 0.6 | 0.6 (Wada et al.) |
| Anterior mallear ligament | 10 | 2.1 (Gan et al.) |
| Lateral mallear ligament | 6.7 | 6.7 (Gan et al.) |
| Superior mallear ligament | 4.9 | 4.9 (Gan et al.) |
| Tensor tympani tendon | 8.7 | 7 (Gan et al.), 2.6 (Wada et al.) |
| Superior incudal ligament | 4.9 | 4.9 (Gan et al.) |
| Posterior incudal ligament | 6.5 | 6.5 (Gan et al.) |
| Stapedial tendon | 5.2 | 5.2 (Wada et al.) |
| Stapedial annulus ligament | 0.2 | 0.2 (Wada et al.) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, J.; Wang, J.; Yao, W.; Wang, M. Development of an Assessment Model for the Effect of the Replacement of Minimal Artificial Ossicles on Hearing in the Inner Ear. Micromachines 2023, 14, 483. https://doi.org/10.3390/mi14020483
Liang J, Wang J, Yao W, Wang M. Development of an Assessment Model for the Effect of the Replacement of Minimal Artificial Ossicles on Hearing in the Inner Ear. Micromachines. 2023; 14(2):483. https://doi.org/10.3390/mi14020483
Chicago/Turabian StyleLiang, Junyi, Jiakun Wang, Wenjuan Yao, and Mianzhi Wang. 2023. "Development of an Assessment Model for the Effect of the Replacement of Minimal Artificial Ossicles on Hearing in the Inner Ear" Micromachines 14, no. 2: 483. https://doi.org/10.3390/mi14020483