
Assessing Hemorrhagic Shock Severity Using the Second Heart Sound Determined from Phonocardiogram: A Novel Approach

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Anesthesia and Surgical Procedures
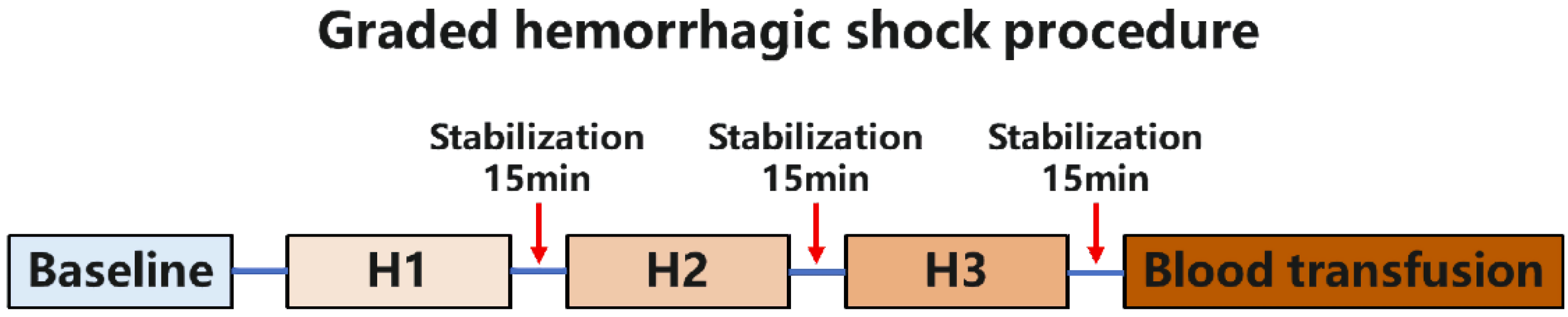
2.3. Experimental Design
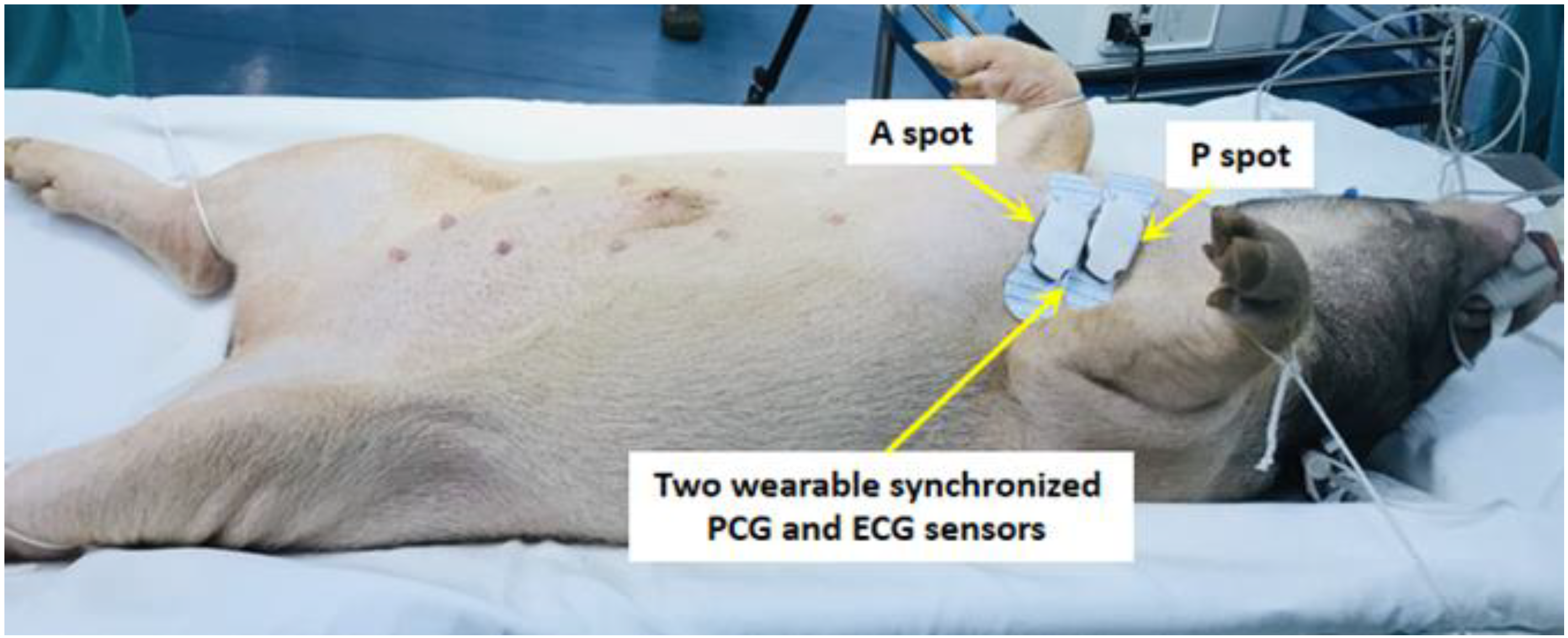
2.4. Heart Sound Signal Collection
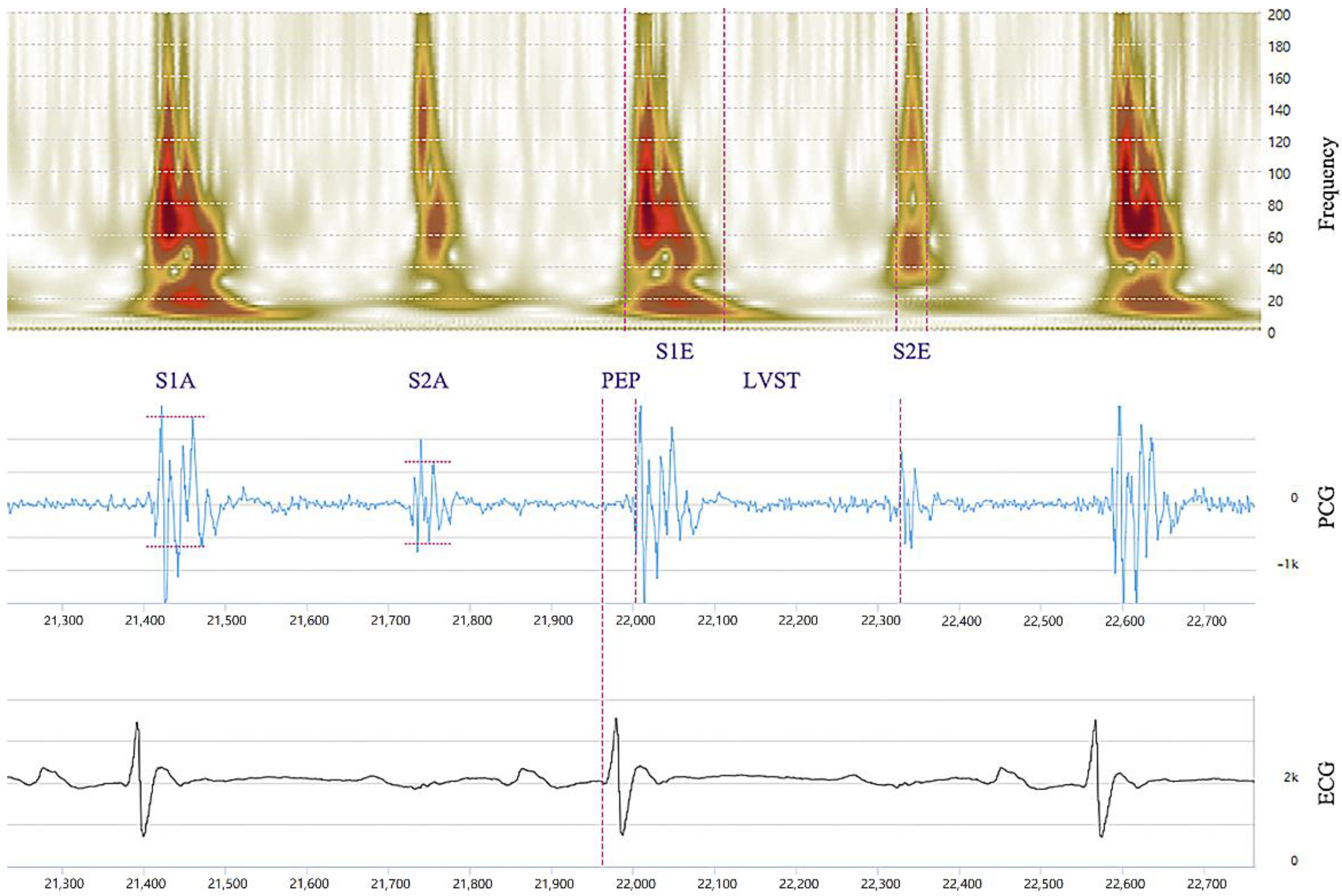
2.5. PCG Data Analysis
2.6. Statistical Analysis
3. Results
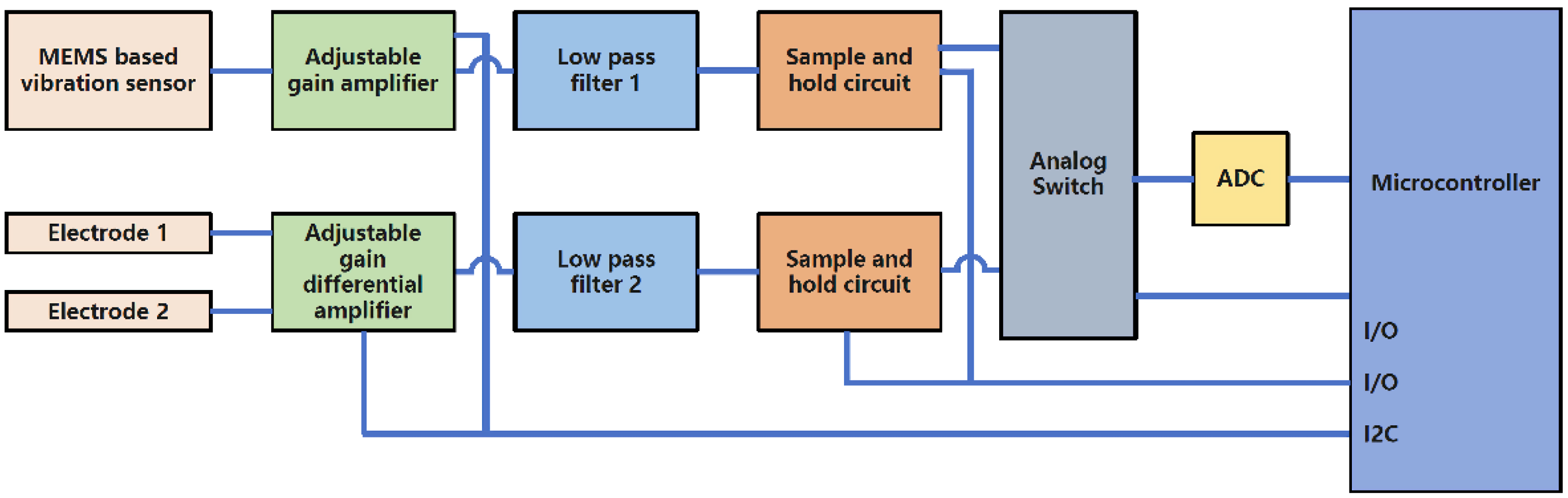
3.1. PCG Sensor Working Process
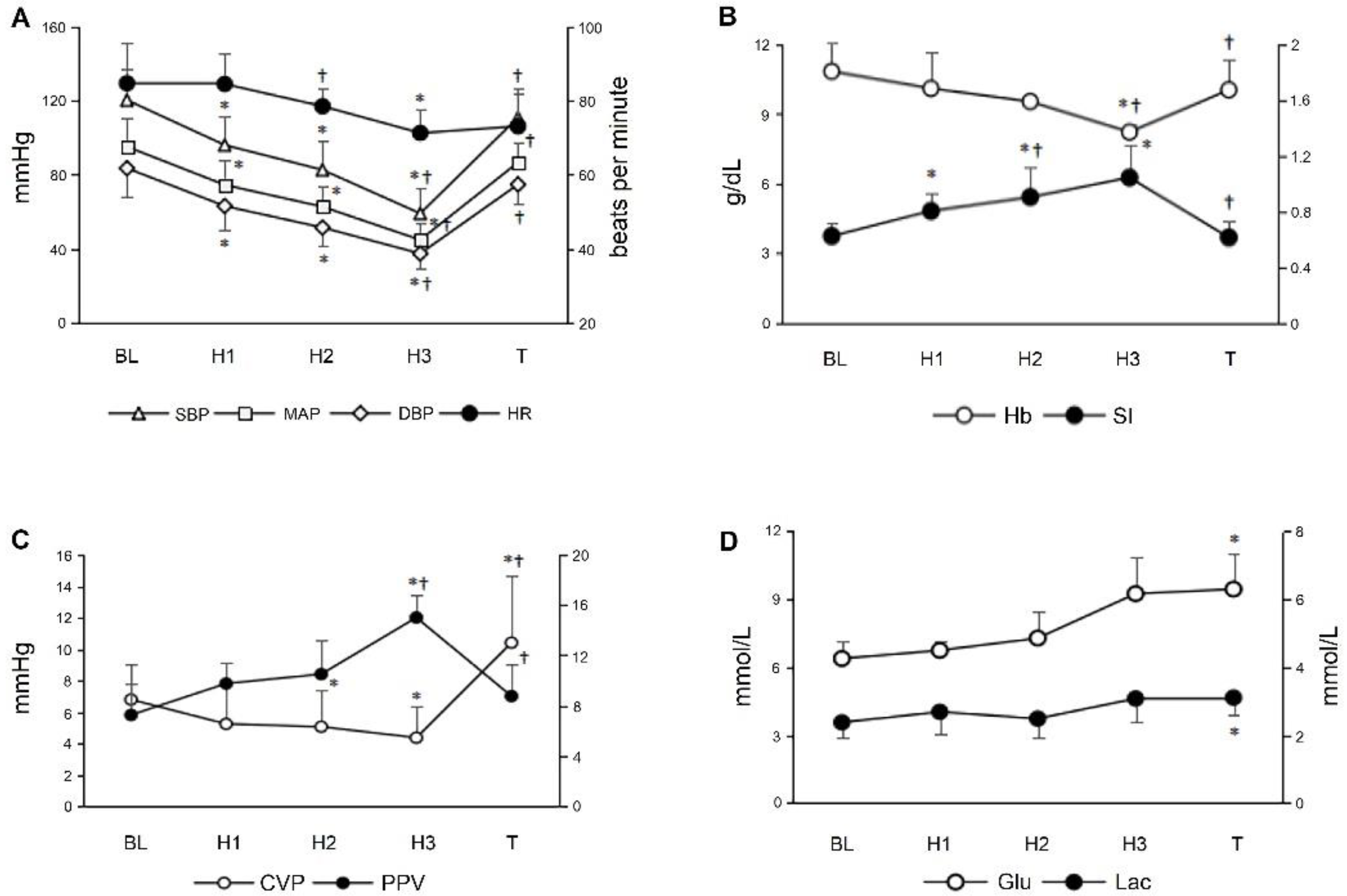
3.2. Routine Monitoring Indicators during Graded Hemorrhagic Shock
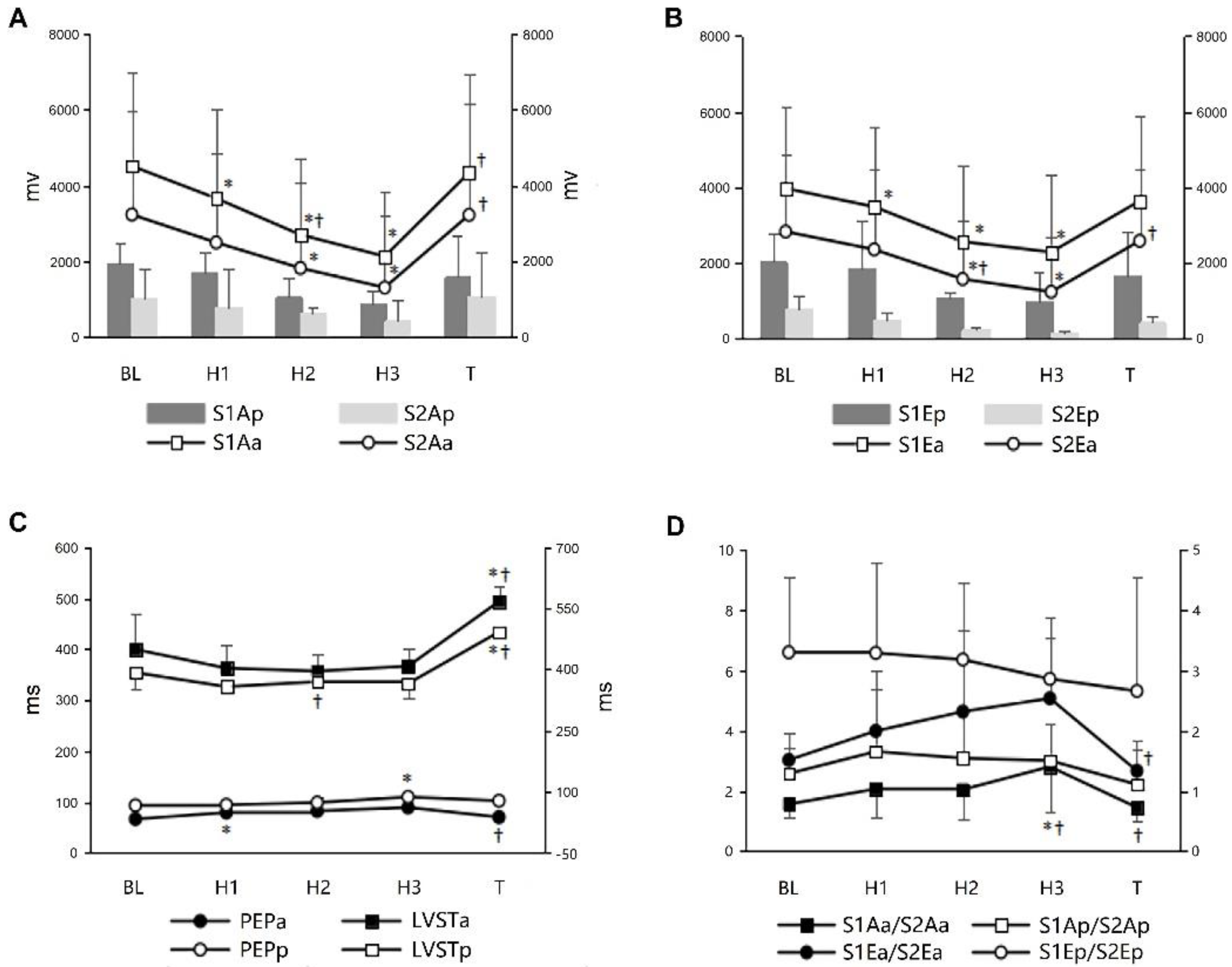
3.3. PCG and Associated Indicators during Graded Hemorrhagic Shock
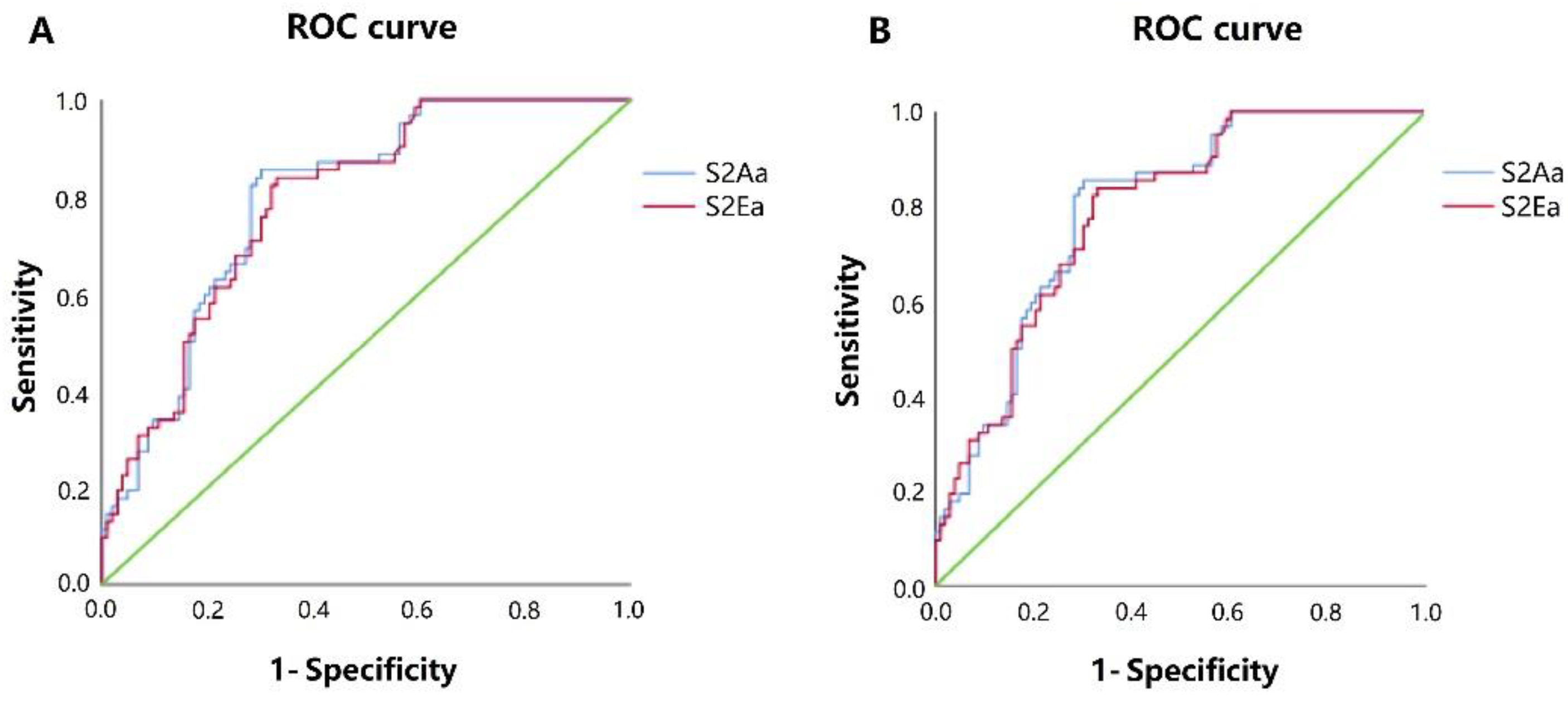
3.4. Correlations between PCG Associated Indicators and Routine Monitoring Indicators
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Cannon, J.W. Hemorrhagic Shock. N. Engl. J. Med. 2018, 378, 370–379. [Google Scholar] [CrossRef] [PubMed]
- Pusateri, A.E.; Moore, E.E.; Moore, H.B.; Le, T.D.; Guyette, F.X.; Chapman, M.P.; Sauaia, A.; Ghasabyan, A.; Chandler, J.; McVaney, K.; et al. Association of Prehospital Plasma Transfusion With Survival in Trauma Patients With Hemorrhagic Shock When Transport Times Are Longer Than 20 Minutes: A Post Hoc Analysis of the PAMPer and COMBAT Clinical Trials. JAMA Surg. 2020, 155, e195085. [Google Scholar] [CrossRef] [PubMed]
- Egan, E.D.; Johnson, K.B. The Influence of Hemorrhagic Shock on the Disposition and Effects of Intravenous Anesthetics: A Narrative Review. Anesth. Analg. 2020, 130, 1320–1330. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.S.; Gustafsson, F. Pulmonary artery pulsatility index: Physiological basis and clinical application. Eur. J. Heart Fail. 2020, 22, 32–38. [Google Scholar] [CrossRef]
- Zhu, C.S.; Cobb, D.; Jonas, R.B.; Pokorny, D.; Rani, M.; Cotner-Pouncy, T.; Oliver, J.; Cap, A.; Cestero, R.; Nicholson, S.E.; et al. Shock index and pulse pressure as triggers for massive transfusion. J. Trauma Acute Care Surg. 2019, 87, S159–S164. [Google Scholar] [CrossRef]
- Najarian, K.; Hakimzadeh, R.; Ward, K.; Daneshvar, K.; Ji, S.Y. Combining predictive capabilities of transcranial doppler with electrocardiogram to predict hemorrhagic shock. Annu. Int. Conf. IEEE Eng. Med. Biol Soc. 2009, 2009, 2621–2624. [Google Scholar] [CrossRef]
- Corradi, F.; Brusasco, C.; Garlaschi, A.; Santori, G.; Vezzani, A.; Moscatelli, P.; Pelosi, P. Splenic Doppler resistive index for early detection of occult hemorrhagic shock after polytrauma in adult patients. Shock 2012, 38, 466–473. [Google Scholar] [CrossRef]
- Lee, S.Y.; Huang, P.W.; Chiou, J.R.; Tsou, C.; Liao, Y.Y.; Chen, J.Y. Electrocardiogram and Phonocardiogram Monitoring System for Cardiac Auscultation. IEEE Trans. Biomed. Circuits Syst. 2019, 13, 1471–1482. [Google Scholar] [CrossRef]
- Fernando, T.; Ghaemmaghami, H.; Denman, S.; Sridharan, S.; Hussain, N.; Fookes, C. Heart Sound Segmentation Using Bidirectional LSTMs With Attention. IEEE J. Biomed. Health Inform. 2020, 24, 1601–1609. [Google Scholar] [CrossRef] [Green Version]
- Li, X.C.; Liu, X.H.; Liu, L.B.; Li, S.M.; Wang, Y.Q.; Mead, R.H. Evaluation of left ventricular systolic function using synchronized analysis of heart sounds and the electrocardiogram. Heart Rhythm 2020, 17, 876–880. [Google Scholar] [CrossRef]
- Moon, Y.J.; Kim, S.H.; Park, Y.S.; Kim, J.M.; Hwang, G.S. Quantitative Analysis of an Intraoperative Digitalized Esophageal Heart Sound Signal to Speculate on Perturbed Cardiovascular Function. J. Clin. Med. 2019, 8, 715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, T.E.; Yang, S.I.; Ho, L.T.; Tsai, K.H.; Chen, Y.H.; Chang, Y.F.; Lai, Y.H.; Wang, S.S.; Tsao, Y.; Wu, C.C. S1 and S2 Heart Sound Recognition Using Deep Neural Networks. IEEE Trans. Biomed. Eng. 2017, 64, 372–380. [Google Scholar] [CrossRef] [PubMed]
- Grooby, E.; He, J.; Kiewsky, J.; Fattahi, D.; Zhou, L.; King, A.; Ramanathan, A.; Malhotra, A.; Dumont, G.A.; Marzbanrad, F. Neonatal Heart and Lung Sound Quality Assessment for Robust Heart and Breathing Rate Estimation for Telehealth Applications. IEEE J. Biomed. Health Inform. 2021, 25, 4255–4266. [Google Scholar] [CrossRef] [PubMed]
- Peng, R.C.; Yan, W.R.; Zhang, N.L.; Lin, W.H.; Zhou, X.L.; Zhang, Y.T. Cuffless and Continuous Blood Pressure Estimation from the Heart Sound Signals. Sensors 2015, 15, 23653–23666. [Google Scholar] [CrossRef] [Green Version]
- Kapur, G.; Chen, L.; Xu, Y.; Cashen, K.; Clark, J.; Feng, X.; Wu, S.F. Noninvasive Determination of Blood Pressure by Heart Sound Analysis Compared With Intra-Arterial Monitoring in Critically Ill Children-A Pilot Study of a Novel Approach. Pediatr. Crit. Care Med. 2019, 20, 809–816. [Google Scholar] [CrossRef]
- Castro, A.; Mattos, S.S.; Coimbra, M.T. Noninvasive blood pressure and the second heart sound analysis. Annu. Int. Conf. IEEE Eng. Med. Biol Soc. 2014, 2014, 5494–5497. [Google Scholar] [CrossRef]
- van Houwelingen, M.J.; Merkus, D.; Hofland, J.; Bakker, J.; Tenbrinck, R.; Te Lintel Hekkert, M.; van Dijk, G.; Hoeks, A.P.; Duncker, D.J. A novel approach to assess hemorrhagic shock severity using the arterially determined left ventricular isovolumic contraction period. Am. J. Physiol. Heart Circ. Physiol. 2013, 305, H1790–H1797. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Zhang, R.; Chang, S.; Liu, C.; Sha, X. A Low-Noise-Level Heart Sound System Based on Novel Thorax-Integration Head Design and Wavelet Denoising Algorithm. Micromachines 2019, 10, 885. [Google Scholar] [CrossRef] [Green Version]
- Zhou, C.; Zang, J.; Xue, C.; Ma, Y.; Hua, X.; Gao, R.; Zhang, Z.; Li, B.; Zhang, Z. Design of a Novel Medical Acoustic Sensor Based on MEMS Bionic Fish Ear Structure. Micromachines 2022, 13, 163. [Google Scholar] [CrossRef]
- Becker, M.; Frauenrath, T.; Hezel, F.; Krombach, G.A.; Kremer, U.; Koppers, B.; Butenweg, C.; Goemmel, A.; Utting, J.F.; Schulz-Menger, J.; et al. Comparison of left ventricular function assessment using phonocardiogram- and electrocardiogram-triggered 2D SSFP CINE MR imaging at 1.5 T and 3.0 T. Eur. Radiol. 2010, 20, 1344–1355. [Google Scholar] [CrossRef]
- Bodo, M.; Pearce, F.J.; Tsai, M.C.; Garcia, A.; Vanalbert, S.; Armonda, R. Cessation of vital signs monitored during lethal hemorrhage: A Swine study. J. Spec. Oper. Med. 2013, 13, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Dhar, R.; Zazulia, A.R.; Videen, T.O.; Zipfel, G.J.; Derdeyn, C.P.; Diringer, M.N. Red blood cell transfusion increases cerebral oxygen delivery in anemic patients with subarachnoid hemorrhage. Stroke 2009, 40, 3039–3044. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cantle, P.M.; Cotton, B.A. Prediction of Massive Transfusion in Trauma. Crit. Care Clin. 2017, 33, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Kreutziger, J.; Rafetseder, A.; Mathis, S.; Wenzel, V.; El Attal, R.; Schmid, S. Admission blood glucose predicted haemorrhagic shock in multiple trauma patients. Injury 2015, 46, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.Y.; Lee, W.H.; Yoo, T.K.; Park, I.; Kim, D.W. A new severity predicting index for hemorrhagic shock using lactate concentration and peripheral perfusion in a rat model. Shock 2012, 38, 635–641. [Google Scholar] [CrossRef] [PubMed]
- Bendjelid, K.; Suter, P.M.; Romand, J.A. The respiratory change in preejection period: A new method to predict fluid responsiveness. J. Appl. Physiol. 2004, 96, 337–342. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.L. Triboelectric nanogenerators as new energy technology and self-powered sensors—Principles, problems and perspectives. Faraday Discuss. 2014, 176, 447–458. [Google Scholar] [CrossRef]
- Demir, S.M.; Al-Turjman, F.; Muhtaroğlu, A. Energy scavenging methods for WBAN applications: A review. IEEE Sens. J. 2018, 18, 6477–6488. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ΔHR | ΔSBP | ΔMAP | ΔDBP | ΔSI | ΔPPV | ΔCVP | |
|---|---|---|---|---|---|---|---|
| ΔS1Aa | |||||||
| r | 0.045 | 0.241 | 0.210 | 0.189 | −0.271 | −0.349 | 0.279 |
| p | 0.574 | 0.002 | 0.008 | 0.018 | 0.001 | <0.001 | 0.001 |
| ΔS2Aa | |||||||
| r | −0.036 | 0.519 | 0.511 | 0.478 | −0.179 | −0.442 | 0.227 |
| p | 0.652 | <0.001 | <0.001 | <0.001 | 0.025 | <0.001 | 0.007 |
| ΔS1Ea | |||||||
| r | −0.006 | 0.254 | 0.225 | 0.210 | −0.369 | −0.154 | 0.105 |
| p | 0.941 | 0.001 | 0.005 | 0.008 | <0.001 | 0.100 | 0.220 |
| ΔS2Ea | |||||||
| r | −0.160 | 0.559 | 0.532 | 0.489 | −0.363 | −0.380 | 0.161 |
| p | 0.045 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.060 |
| ΔS1Aa/S2Aa | |||||||
| r | 0.252 | −0.550 | −0.523 | −0.503 | 0.455 | 0.117 | −0.092 |
| p | 0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.211 | 0.283 |
| ΔS1Ea/S2Ea | |||||||
| r | 0.237 | −0.526 | −0.509 | −0.489 | 0.448 | 0.098 | −0.200 |
| p | 0.003 | <0.001 | <0.001 | <0.001 | <0.001 | 0.294 | 0.019 |
| ΔPEPa | |||||||
| r | −0.397 | −0.469 | −0.509 | −0.509 | −0.105 | 0.170 | −0.331 |
| p | <0.001 | <0.001 | <0.001 | <0.001 | 0.192 | 0.068 | <0.001 |
| ΔLVSTa | |||||||
| r | −0.693 | 0.358 | 0.276 | 0.170 | −0.620 | −0.519 | 0.320 |
| p | <0.001 | <0.001 | <0.001 | 0.033 | <0.001 | <0.001 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, Y.; Hou, A.; Wu, X.; Cong, T.; Zhou, Z.; Jiao, Y.; Luo, Y.; Wang, Y.; Mi, W.; Cao, J. Assessing Hemorrhagic Shock Severity Using the Second Heart Sound Determined from Phonocardiogram: A Novel Approach. Micromachines 2022, 13, 1027. https://doi.org/10.3390/mi13071027
Chen Y, Hou A, Wu X, Cong T, Zhou Z, Jiao Y, Luo Y, Wang Y, Mi W, Cao J. Assessing Hemorrhagic Shock Severity Using the Second Heart Sound Determined from Phonocardiogram: A Novel Approach. Micromachines. 2022; 13(7):1027. https://doi.org/10.3390/mi13071027
Chicago/Turabian StyleChen, Yan, Aisheng Hou, Xiaodong Wu, Ting Cong, Zhikang Zhou, Youyou Jiao, Yungen Luo, Yuheng Wang, Weidong Mi, and Jiangbei Cao. 2022. "Assessing Hemorrhagic Shock Severity Using the Second Heart Sound Determined from Phonocardiogram: A Novel Approach" Micromachines 13, no. 7: 1027. https://doi.org/10.3390/mi13071027