
Microfluidic Paper-Based Blood Plasma Separation Device as a Potential Tool for Timely Detection of Protein Biomarkers

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents and Manufacturing Materials
2.2. Blood Sample Preparation
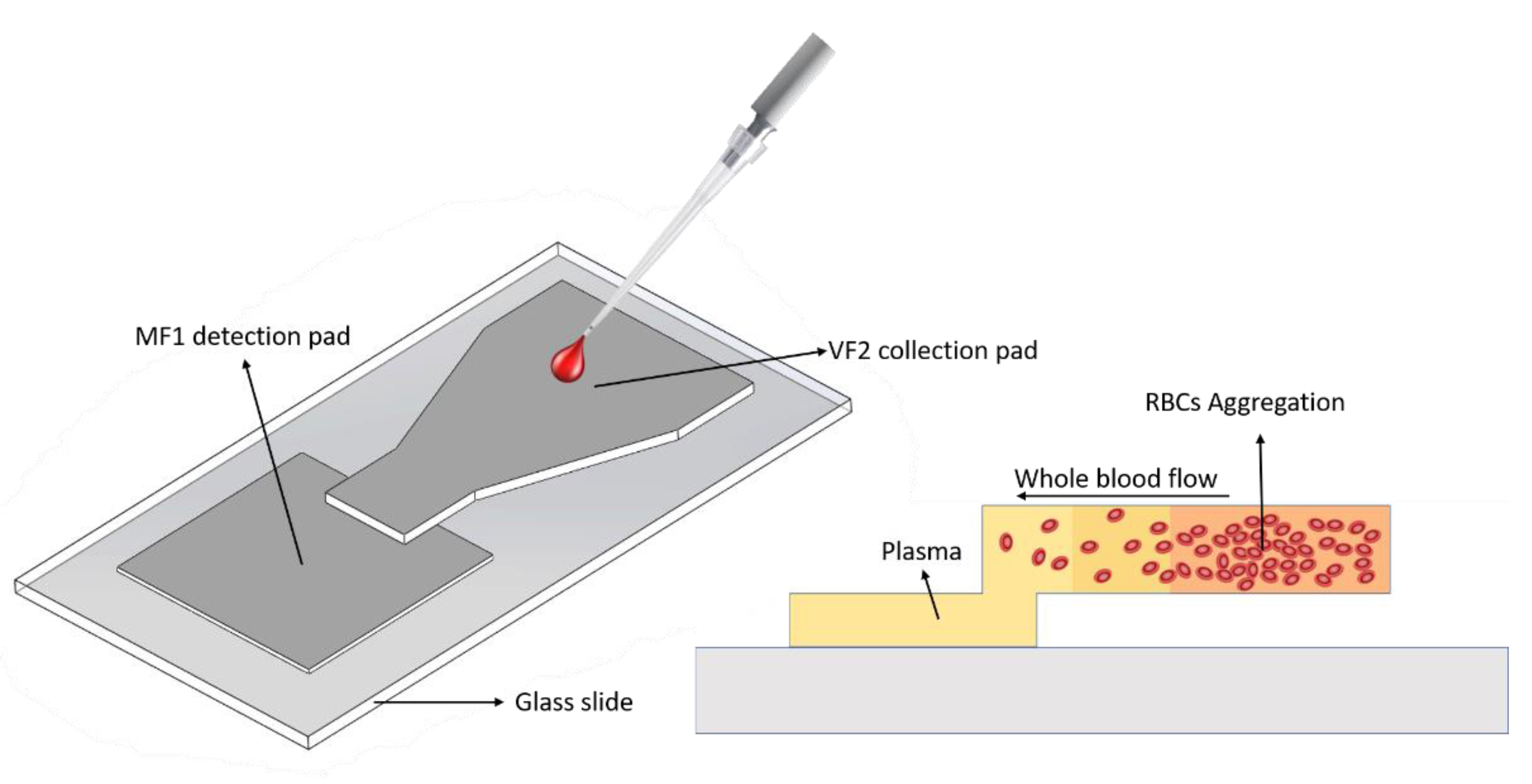
2.3. Device Design and Fabrication
2.4. Separation Efficiency Analysis
2.5. Plasma Flow over Time
2.6. Blood Sample Volume Optimization
2.7. S100B Detection Mechanism
2.8. Design of Experiments
2.9. Robustness Evaluation against Disturbance Factors
2.10. Statistical Analysis
3. Results and Discussion
3.1. Device Fabrication
3.2. Separation Efficiency Analysis
3.3. Plasma Flow over Time
3.4. Blood Sample Volume Optimization
3.5. S100B Detection
3.6. Limitations
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hardman, J.M.; Manoukian, A. Pathology of head trauma. Neuroimaging Clin. N. Am. 2002, 12, 175–187. [Google Scholar] [CrossRef]
- Dong, P.V.; Cremer, O.L. Limitations of the use of the Glasgow Coma Scale in intensive care patients with non-neurological primary disease: A search for alternatives. Crit. Care 2011, 15, P506. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Salgueró, P.; Echevarría, C.; Barrera, J. Traumatismos craneoencefálicos. Escalas de valoración para la medida de resultados en rehabilitación. Rehabilitación 2002, 36, 408–417. [Google Scholar] [CrossRef]
- Zhang, J.; Puvenna, V.; Janigro, D. Biomarkers of Traumatic Brain Injury and Their Relationship to Pathology. Transl. Res. Trauma. Brain Inj. 2016. [Google Scholar]
- Mutch, C.A.; Talbott, J.F.; Gean, A. Imaging Evaluation of Acute Traumatic Brain Injury. Neurosurg. Clin. N. Am. 2016, 27, 409–439. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez Sanjuan, A.; Cervera Silvera, E.; Valencia Villa, G.; Villalba, P. Revisión de tema: Biomarcadores neuro-nales y gliales como estrategia de clasificación cuantitativa de la severidad del trauma craneoencefálico. Rev. Salud Uninorte 2016, 32, 302–318. [Google Scholar] [CrossRef]
- Rodríguez, A.; Burgos-Flórez, F.; Posada, J.; Cervera, E.; Zucolotto, V.; Sanjuán, H.; Sanjuán, M.; Villalba, P. Electrochemical Immunosensor for the Quantification of S100B at Clinically Relevant Levels Using a Cysteamine Modified Surface. Sensors 2021, 21, 1929. [Google Scholar] [CrossRef]
- Burgos-Flórez, F.; Rodríguez, A.; Cervera, E.; Zucolotto, V.; Sanjuán, M.; Villalba, P.J. TBISTAT: An open-source, wireless portable, electrochemical impedance spectroscopy capable potentiostat for the point-of-care detection of S100B in plasma samples. PLoS ONE 2022, 17, e0263738. [Google Scholar] [CrossRef]
- Kim, C.; Searson, P.C. Magnetic bead-quantum dot assay for detection of a biomarker for traumatic brain injury. Nanoscale 2015, 7, 17820–17826. [Google Scholar] [CrossRef] [Green Version]
- Yamada, K.; Shibata, H.; Suzuki, K.; Citterio, D. Toward practical application of paper-based microfluidics for medical diagnostics: State-of-the-art and challenges. Lab Chip 2017, 17, 1206–1249. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Kumar, S.; Agarwal, A.K. Paper Microfluidics-Theory and Applications, 1st ed.; Springer: Singapore, 2019. [Google Scholar]
- Bhamla, M.S.; Benson, B.; Chai, C.; Katsikis, G.; Johri, A.; Prakash, M. Hand-powered ultralow-cost paper centrifuge. Nat. Biomed. Eng. 2017, 1, 0009. [Google Scholar] [CrossRef]
- Gong, M.M.; Macdonald, B.D.; Nguyen, T.V.; Van Nguyen, K.; Sinton, D. Field tested milliliter-scale blood filtration device for point-of-care applications. Biomicrofluidics 2013, 7, 044111. [Google Scholar] [CrossRef] [Green Version]
- Guo, W.; Hansson, J.; van der Wijngaart, W. Synthetic Paper Separates Plasma from Whole Blood with Low Protein Loss. Anal. Chem. 2020, 92, 6194–6199. [Google Scholar] [CrossRef]
- Kar, S.; Maiti, T.K.; Chakraborty, S. Capillarity-driven blood plasma separation on paper-based devices. Analyst 2015, 140, 6473–6476. [Google Scholar] [CrossRef]
- Kim, J.-H.; Woenker, T.; Adamec, J.; Regnier, F.E. Simple, Miniaturized Blood Plasma Extraction Method. Anal. Chem. 2013, 85, 11501–11508. [Google Scholar] [CrossRef]
- Li, C.G.; Joung, H.-A.; Noh, H.; Song, M.-B.; Kim, M.-G.; Jung, H. One-touch-activated blood multidiagnostic system using a minimally invasive hollow microneedle integrated with a paper-based sensor. Lab Chip 2015, 15, 3286–3292. [Google Scholar] [CrossRef]
- Lu, Z.; Rey, E.; Vemulapati, S.; Srinivasan, B.; Mehta, S.; Erickson, D. High-yield paper-based quantitative blood separation system. Lab Chip 2018, 18, 3865–3871. [Google Scholar] [CrossRef]
- Nilghaz, A.; Shen, W. Low-cost blood plasma separation method using salt functionalized paper. RSC Adv. 2015, 5, 53172–53179. [Google Scholar] [CrossRef]
- Noiphung, J.; Songjaroen, T.; Dungchai, W.; Henry, C.S.; Chailapakul, O.; Laiwattanapaisal, W. Electrochemical detection of glucose from whole blood using paper-based microfluidic devices. Anal. Chim. Acta 2013, 788, 39–45. [Google Scholar] [CrossRef]
- Robinson, R.; Wong, L.; Monnat, R.J.; Fu, E. Development of a Whole Blood Paper-Based Device for Phenylalanine Detection in the Context of PKU Therapy Monitoring. Micromachines 2016, 7, 28. [Google Scholar] [CrossRef] [Green Version]
- Songjaroen, T.; Dungchai, W.; Chailapakul, O.; Henry, C.S.; Laiwattanapaisal, W. Blood separation on microfluidic paper-based analytical devices. Lab Chip 2012, 12, 3392–3398. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, S.; Garnier, G.; Rao, V.R. One dimensional zinc oxide nanostructures assisted paper-based blood-plasma separation. Vacuum 2017, 146, 586–591. [Google Scholar] [CrossRef]
- Vella, S.J.; Beattie, P.; Cademartiri, R.; Laromaine, A.; Martinez, A.W.; Phillips, S.T.; Mirica, K.A.; Whitesides, G.M. Measuring Markers of Liver Function Using a Micropatterned Paper Device Designed for Blood from a Fingerstick. Anal. Chem. 2012, 84, 2883–2891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, X.; Forouzan, O.; Brown, T.P.; Shevkoplyas, S.S. Integrated separation of blood plasma from whole blood for microfluidic paper-based analytical devices. Lab Chip 2012, 12, 274–280. [Google Scholar] [CrossRef]
- Yamada, K.; Citterio, D. Paper-Based Microfluidics for Point-of-Care Medical Diagnostics. Applications of Micro-fluidic Systems in Biology and Medicine; Springer Nature: Singapore, 2019; pp. 353–382. [Google Scholar]
- Silveira, C.M.; Monteiro, T.; Almeida, M.G. Biosensing with Paper-Based Miniaturized Printed Electrodes—A Modern Trend. Biosensors 2016, 6, 51. [Google Scholar] [CrossRef] [Green Version]
- Nilghaz, A.; Guan, L.; Tan, W.; Shen, W. Advances of Paper-Based Microfluidics for Diagnostics—The Original Motivation and Current Status. ACS Sensors 2016, 1, 1382–1393. [Google Scholar] [CrossRef]
- Tenda, K.; Ota, R.; Yamada, K.; Henares, T.G.; Suzuki, K.; Citterio, D. High-Resolution Microfluidic Paper-Based Analytical Devices for Sub-ΜL Sample Analysis. Micromachines 2016, 7, 80. [Google Scholar] [CrossRef] [Green Version]
- Urdea, M.; Penny, L.A.; Olmsted, S.S.; Giovanni, M.Y.; Kaspar, P.; Shepherd, A.; Wilson, P.; Dahl, C.A.; Buchsbaum, S.; Moeller, G.; et al. Requirements for high impact diagnostics in the developing world. Nature 2006, 444, 73–79. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Capillary Action | Fabrication | Paper Types | Plasma Yield (%) | Separation Time (s) | Hematocrits in the Sample (%) | Blood Volume (μL) |
|---|---|---|---|---|---|---|---|
| Songjaroen (2012) [22] | Vertical and lateral flow by membrane separation | Wax dipping | MF1 and LF1 and Whatman No. 1 | N.R. | 100–200 | 24–55 | 8–20 |
| Vella (2012) [24] | Vertical flow by membrane separation | Wax printing | VF1, VF2, MF1, Fusion 5, GX, GR, GF, and Whatman No. 1 | N.R. | 300–600 | N.R. | 10–20 |
| Yang (2012) [25] | Vertical and lateral flow by agglutination with anti-A, -B, and -AB antibodies | Wax printing and antibody drop-casting | Whatman No. 1 | N.R. | <300 | N.R. | 7 |
| Noiphung (2013) [20] | Vertical and lateral flow by membrane separation | Wax dipping | VF1, VF2, and Whatman No. 1 | N.R. | 170–270 | 24–60 | 200 |
| Gong (2013) [13] | Vertical and lateral flow by membrane separation | Laser micromachining of PMMA | Polysulfone asymmetric membrane GR VIVID | 6–35 | 300 | N.R. | 800–1000 |
| Kim (2013) [16] | Vertical and lateral flow by membrane separation | N.R. | NOVIPLEX separation membrane | 12–30 | 180 | 20–71 | 25 |
| Nilghaz (2015) [19] | Lateral flow controlled by red blood cells aggregation | Wax patterning | NaCl functionalized Whatman No.4 | N.R. | 180 | 35–55 | 3–10 |
| Kar (2015) [15] | Lateral flow controlled by H channel and changes in blood rheological properties | Inkjet printing followed by Origami protocol | Whatman No. 4 and PBS solution | N.R. | 200 | 37 | 50 |
| G. Li (2015) [17] | Vertical and lateral flow by membrane separation | Paper cutting | Polysulfone asymmetric membrane GR VIVID, Fusion 5 y 10G surfactant treated nitrocellulose membrane | N.R. | 180 | 40 | 15–40 |
| Robinson (2016) [21] | Vertical and lateral flow by membrane separation | Paper cutting | Polysulfone asymmetric membrane GR VIVID, glass fiber membrane filter, and nitrocellulose membrane | N.R. | 360 | N.R. | 40 |
| Tiwari (2017) [23] | Vertical and lateral flow by functionalized membrane separation | Paper cutting | GF/C glass fiber paper disks, Whatman No.1, No.2, No.5, and Zinc nanorods | N.R. | 600 | N.R. | 3 |
| Bhamla (2017) [12] | Paper-based centrifuge | Paper cutting | Paper wood, Nylon threads | N.R. | 90 | N.R. | 20 |
| Lu (2018) [18] | Vertical and lateral flow by membrane separation | Papercutting bound with adhesive tape | Polysulfone asymmetric membrane GR VIVID, FR-1 filter pad, Fusion 5 | 20–30 | 600 | 30–60 | 50–70 |
| Guo (2020) [14] | Vertical and lateral flow by agglutination with anti-A, -B, and -AB antibodies | Paper cutting | N.R. Synthetic paper | 11 | 316 | 45 | 90 |
| This work | Vertical and lateral flow by membrane separation and RBC agglutination | Papercutting bound with adhesive tape | MF1, NaCl functionalized VF2 | 30 | 220 | 45 | 300 |
| Experimental Run | Number of RBCs in Whole Blood | Number of RBCs in Separated Plasma | Separation Efficiency |
|---|---|---|---|
| 1 | 1208 | 99 | 0.92 |
| 2 | 983 | 35 | 0.96 |
| 3 | 1147 | 78 | 0.93 |
| 4 | 947 | 24 | 0.97 |
| 5 | 1369 | 18 | 0.98 |
| Mean | 1130.8 | 50.8 | 0.95 |
| Standard deviation | 172.2 | 35.73 | 0.03 |
| S100B Concentration Using ELISA | ||
|---|---|---|
| Experimental Run | Centrifugation | BPS Device |
| 1 | 138.47 | 167.56 |
| 2 | 126.84 | 266.45 |
| 3 | 202.46 | 91.93 |
| Mean | 155.92 | 175.31 |
| Standard deviation | 40.71 | 87.51 |
| Skewness | 1.11 | 0.27 |
| Test | p-Value | |
| F-test | 4.61 | 0.35 |
| T-test | 0.34 | 0.74 |
| S100B Concentration Using ELISA | ||
|---|---|---|
| Experimental Run | Centrifugation | BPS Device |
| 1 | 371.15 | 400.24 |
| 2 | 417.69 | 435.14 |
| 3 | 382.79 | 347.89 |
| Mean | 390.54 | 394.42 |
| Standard deviation | 24.21 | 43.91 |
| Skewness | 0.91 | −0.41 |
| Test | p-Value | |
| F-test | 0.30 | 0.46 |
| T-test | −0.13 | 0.89 |
| S100B Concentration Using ELISA | ||
|---|---|---|
| Experimental Run | Centrifugation | BPS Device |
| 1 | 1237.91 | 1377.52 |
| 2 | 1191.37 | 1080.85 |
| 3 | 1139.02 | 1278.63 |
| Mean | 1189.43 | 1245.67 |
| Standard deviation | 49.47 | 151.05 |
| Skewness | −0.12 | −0.66 |
| Test | p-Value | |
| F-test | 0.10 | 0.19 |
| T-test | −0.61 | 0.57 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Burgos-Flórez, F.; Rodríguez, A.; Cervera, E.; De Ávila, M.; Sanjuán, M.; Villalba, P.J. Microfluidic Paper-Based Blood Plasma Separation Device as a Potential Tool for Timely Detection of Protein Biomarkers. Micromachines 2022, 13, 706. https://doi.org/10.3390/mi13050706
Burgos-Flórez F, Rodríguez A, Cervera E, De Ávila M, Sanjuán M, Villalba PJ. Microfluidic Paper-Based Blood Plasma Separation Device as a Potential Tool for Timely Detection of Protein Biomarkers. Micromachines. 2022; 13(5):706. https://doi.org/10.3390/mi13050706
Chicago/Turabian StyleBurgos-Flórez, Francisco, Alexander Rodríguez, Eliana Cervera, Marcio De Ávila, Marco Sanjuán, and Pedro J. Villalba. 2022. "Microfluidic Paper-Based Blood Plasma Separation Device as a Potential Tool for Timely Detection of Protein Biomarkers" Micromachines 13, no. 5: 706. https://doi.org/10.3390/mi13050706