
Continuous Glucose Monitoring System Based on Percutaneous Microneedle Array


Abstract
:1. Introduction
2. Materials and Methods
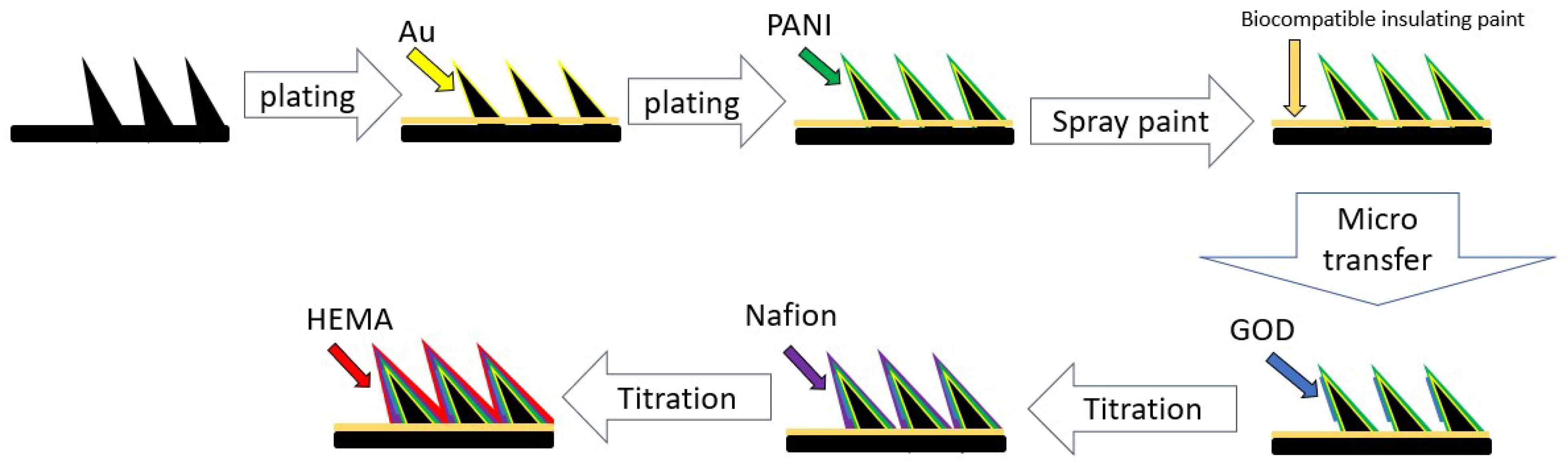
2.1. Micro-Transfer Method
2.2. Reagents and Immobilization
2.3. Blood Glucose Sensing Circuit
3. Experimental Design
3.1. Micro-Transfer Enzyme Measurement on Microneedle Electrodes
3.1.1. The Amount of GOD Used per Transfer
3.1.2. Micro-Transfer Variations
3.2. Combed Test of Glucose Solution with Microneedle Array Sensor and Conditioning Circuit
3.3. Blood Glucose Monitor Circuit Tested in an Agar-Based Skin Model
3.4. Long-Term Stability Test of Blood Glucose Circuit
3.5. Human Experiment Test
4. Conclusions and Prospects
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Guariguata, L.; Whiting, D.; Weil, C.; Unwin, N. The International Diabetes Federation diabetes atlas methodology for estimating global and national prevalence of diabetes in adults. Diabetes Res. Clin. Pract. 2011, 94, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Chou, P.; Tung, T.H.; Li, C.L.; Chuang, S.Y.; Lin, C.H.; Yang, N.P. Epidemiology of Diabetes Mellitus in Taiwan. Taiwan J. Public Health 2002, 21, 83–96. [Google Scholar]
- Wang, J. Glucose Biosensor: 40 Years of Advance and Challenges. Electroanalysis 2001, 13, 983–988. [Google Scholar] [CrossRef]
- Hsieh, M.-L. Exploring the Risk Factors for Diabetic Retinopathy in Diabetes. Master’s Thesis, China Medical University, Taichung, Taiwan, 2013. [Google Scholar]
- Li, S.; Dai, J.; Zhu, M.; Arroyo-Currás, N.; Li, H.; Wang, Y.; Wang, Q.; Lou, X.; Kippin, T.E.; Wang, S.; et al. Hydrogel-coating improves 1 the in-vivo stability of 2 electrochemical aptamer-based biosensors. bioRxiv 2020. [Google Scholar] [CrossRef]
- Caduff, A.; Hirt, E.; Feldman, Y.; Ali, Z.; Heinemann, L. First human experiment with a novel non-invasive, non-optical continuous glucose monitoring system. Biosens. Bioelectron. 2003, 19, 209–217. [Google Scholar] [CrossRef]
- Lahdesmaki, I.; Shum, A.J.; Parviz, B.A. Possibilities for continuous glucose monitoring by a function contact lens. IEEE Instrum. Meas. Mag. 2010, 13, 14–17. [Google Scholar] [CrossRef]
- Liao, C.-Y. The Study of a Non-Invasive Technology for Glucose Measurements. Master’s Thesis, National Taiwan University, Taipei, Taiwan, 1997. [Google Scholar]
- Hsu, W.-L. Development of Optical and Electrical Biotech Methodology: An Optically Multi-Functional Biochip System and Innovative Electro-Chemistry Methodology. Master’s Thesis, National Taiwan University, Taipei, Taiwan, 2004. [Google Scholar]
- Peura, R.A.; Mendelson, Y. Blood Glucose Sensor: An Overview. In Proceedings of the IEEE/NSF Symposium on Biosensor, Los Angeles, CA, USA, 15–17 September 1984; pp. 63–68. [Google Scholar]
- Windmiller, J.R.; Zhou, N.; Chuang, M.C.; Gabriela, V.R.; Santhosh, P.; Miller, P.R.; Roger, N.; Wang, J. Microneedle array-based carbon paste amperometric sensors and biosensors. Analyst 2011, 136, 1846–1851. [Google Scholar] [CrossRef] [PubMed]
- Bollella, P.; Sharma, S.; Cass, A.E.G.; Antiochia, R. Minimally-invasive microneedle-based biosensor array for simulta-neous lactate and glucose monitoring in artificial interstitial fluid. Electroanalysis 2019, 31, 374–382. [Google Scholar] [CrossRef] [Green Version]
- Jia, Z.; Huang, L.; Liu, H.; Huang, Y.; Li, W.; Pi, X.; Zheng, X. Design of a Real-time Self-adjusting Calibration Algorithm to Improve the Accuracy of Continuous Blood Glucose Monitoring. Appl. Biochem. Biotechnol. 2020, 190, 1163–1176. [Google Scholar] [CrossRef] [PubMed]
- Chinnadayyala, S.R.; Satti, A.T.; Kim, D.; Cho, S. Minimally invasive and continuous glucose monitoring sensor based on non-enzymatic porous platinum black-coated gold microneedles. Eletrochim. Acta 2021, 369, 137691. [Google Scholar] [CrossRef]
- Cappon, G.; Vettoretti, M.; Sparacino, G.; Facchinetti, A. Continuous Glucose Monitoring Sensors for Diabetes Management: A Review of Technologies and Applications. Diabetes Metab. J. 2019, 43, 383–397. [Google Scholar] [CrossRef] [PubMed]
- Vashist, S.K. Continuous Glucose Monitoring Systems: A Review. Diagnostics 2013, 3, 385–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klonoff, D.C.; Ahn, D.; Drincic, A. Continuous glucose monitoring: A review of the technology and clinical use. Diabetes Res. Clin. Pract. 2017, 133, 178–192. [Google Scholar] [CrossRef]
- Cai, Y.; Liang, B.; Chen, S.; Zhu, Q.; Tu, T.; Wu, K.; Cao, Q.; Fang, L.; Liang, X.; Ye, X. One-step modification of nano-polyaniline/glucose oxidase on double-side printed flexible electrode for continuous glucose monitoring: Characterization, cytotoxicity evaluation and in vivo experiment. Biosens. Bioelectron. 2020, 165, 112408. [Google Scholar] [CrossRef] [PubMed]
- Hoss, U.; Budiman, E. Factory-Calibrated Continuous Glucose Sensors: The Science behind the Technology. Diabetes Technol. Ther. 2017, 19 (Suppl. S2), S-44–S-50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Diabetes Research in Children Network Study Group. Accuracy of the GlucoWatch G2 Biographer and the continuous glucose monitoring system during hypoglycemia. Diabetes Care 2004, 27, 722–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Santos, A.N.; Soares, D.A.W.; De Queiroz, A.A.A. Low Potential Stable Glucose Detection at Dendrimers Modified Polyaniline Nanotubes. Mater. Res. 2010, 13, 5–10. [Google Scholar] [CrossRef]
- Lee, I.; Probst, D.; Klonoff, D.; Sode, K. Continuous glucose monitoring systems—Current status and future perspectives of the flagship technologies in biosensor research. Biosens. Bioelectron. 2021, 181, 113054. [Google Scholar] [CrossRef] [PubMed]
- Dąbrowska, A.K.; Rotaru, G.-M.; Derler, S.; Spano, F.; Camenzind, M.; Annaheim, S.; Stämpfli, R.; Schmid, M.; Rossi, R.M. Materials used to simulate physical properties of human skin. Ski. Res. Technol. 2016, 22, 3–14. [Google Scholar] [CrossRef] [PubMed]

















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Dexcom G5 Mobile CGM System | FreeStyle Navigator | Medtronic iPro 2 | Abbott FreeStyle Pro | |
|---|---|---|---|---|
| Target site | Skin | Skin | skin | skin |
| Sensor lifespan | 7 day | 5 day | 6 day | 14 day |
| Length of microneedle probe | 13 mm | 6 mm | 8.5 mm | 5 mm |
| Sensor warm-up | 2 h | 10 h | 2 h | 1 h |
| Calibration | Every 12 h | Every 12 h | 3 on Day 1, 4 per day after | Factory Calibrated |
| Microtransfer | Dispensing (0.25 µL) | Signal Error | |
|---|---|---|---|
| 50 mg/dL | 3.75 × 106 | 3.55 × 106 | 5.75% |
| 400 mg/dL | 8.94 × 106 | 8.46 × 106 | 5.382% |
| Concentration | Microneedle-Random Sampling | ||||||
|---|---|---|---|---|---|---|---|
| Transfer-1 | Transfer-2 | Transfer-3 | Transfer-4 | Average | Standard Deviation | Variability Test Error | |
| 50 mg/dL | 3.68 × 106 | 3.80 × 106 | 3.99 × 106 | 3.54 × 106 | 3.75 × 106 | 1.6 × 107 | 4.266% |
| 400 mg/dL | 8.86 × 106 | 8.48 × 106 | 8.77 × 106 | 7.88 × 106 | 8.50 × 106 | 4.43 × 107 | 5.220% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chien, M.-N.; Chen, Y.-J.; Bai, C.-H.; Huang, J.-T. Continuous Glucose Monitoring System Based on Percutaneous Microneedle Array. Micromachines 2022, 13, 478. https://doi.org/10.3390/mi13030478
Chien M-N, Chen Y-J, Bai C-H, Huang J-T. Continuous Glucose Monitoring System Based on Percutaneous Microneedle Array. Micromachines. 2022; 13(3):478. https://doi.org/10.3390/mi13030478
Chicago/Turabian StyleChien, Ming-Nan, Yu-Jen Chen, Chin-Han Bai, and Jung-Tung Huang. 2022. "Continuous Glucose Monitoring System Based on Percutaneous Microneedle Array" Micromachines 13, no. 3: 478. https://doi.org/10.3390/mi13030478