
Medical Applications of Diode Lasers: Pulsed versus Continuous Wave (cw) Regime


Abstract
:1. Introduction
2. Materials & Methods
3. Results
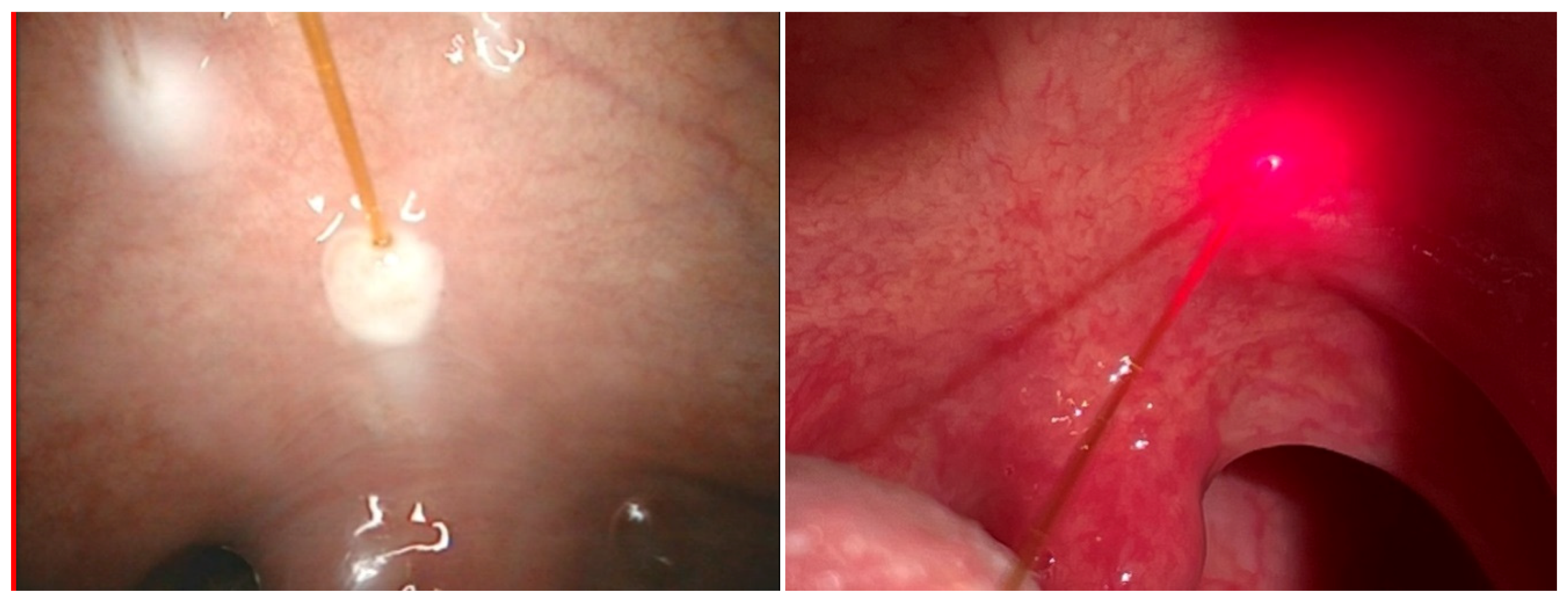
3.1. Pulsed Diode Laser 810 nm (5 W Fluence and Pulse Duration 4 s) in Laryngology Applications in MML Centre
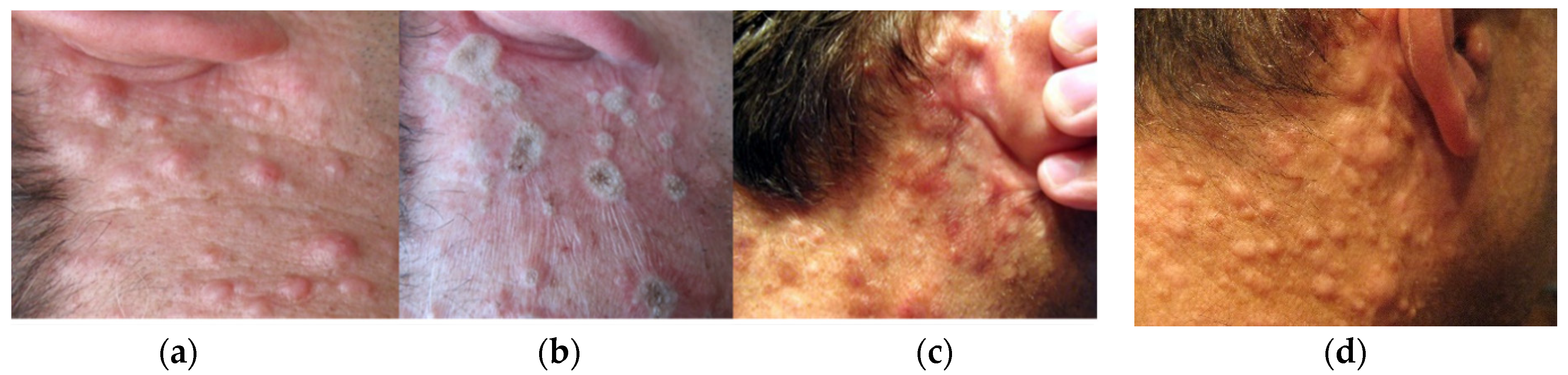
3.2. Pulsed and Continuous (cw) Operation Regime of Diode Laser 975 nm Implemented for Therapy of Dermal Neurofibroma
4. Discussions
5. Conclusions
Author Contributions
Funding
Informed Consent Statement
Conflicts of Interest
Appendix A. Patient Statement of Informed Consent for Surgical Treatment
References
- Goldman, L.; Blaney, D.J.; Kindel, D.J.; Franke, E.K. Effect of the Laser Beam on the Skin**From the Departments of Dermatology and Physics of the University of Cincinnati. The study was done under a grant from the U.S. Public Health Service 0H0018. J. Investig. Dermatol. 1963, 40, 121–122. [Google Scholar] [CrossRef] [Green Version]
- Song, K.U. Footprints in Laser Medicine and Surgery: Beginnings, Present, and Future. Med. Lasers 2017, 6, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Anderson, R.; Parrish, J. Selective photothermolysis: Precise microsurgery by selective absorption of pulsed radiation. Science 1983, 220, 524–527. [Google Scholar] [CrossRef] [Green Version]
- Mester, A. Laser Biostimulation. Photomed. Laser Surg. 2013, 31, 237–239. [Google Scholar] [CrossRef]
- Hamblin, M.R. Photobiomodulation or low-level laser therapy. J. Biophotonics 2016, 9, 1122–1124. [Google Scholar] [CrossRef]
- Mester, E.; Szende, B.; Spiry, T.; Scher, A. Stimulation of wound healing by laser rays. Acta Chir. Acad. Sci. Hung. 1972, 13, 315–324. [Google Scholar]
- Kawalec, J.; Reyes, C.; Penfield, V.; Hetherington, V.; Hays, D.; Feliciano, F.; Gartz, D.; Jones, J.; Esposito, R.; Cernica, M. Evaluation of the Ceralas D15 diode laser as an adjunct tool for wound care: A pilot study. Foot 2001, 11, 68–73. [Google Scholar] [CrossRef]
- Goo, H.; Kim, H.; Ahn, J.-C.; Cho, K.J. Effects of Low-level Light Therapy at 740 nm on Dry Eye Disease In Vivo. Med. Lasers 2019, 8, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Espey, B.T.; Kielwein, K.; van der Ven, H.; Steger, K.; Allam, J.; Paradowska-Dogan, A.; van der Ven, K. Effects of Pulsed-Wave Photobiomodulation Therapy on Human Spermatozoa. Lasers Surg. Med. 2021. [Google Scholar] [CrossRef]
- Bass, L.S. Photosclerosis of cutaneous vascular malformations with a pulsed 810-nm diode laser. In Lasers in Surgery: Advanced Characterization, Therapeutics, and Systems V, Proceedings of the Photonics West '95, San Jose, CA, USA, 1−28 February 1995; SPIE: Bellingham, WA, USA, 1995; pp. 559–565. [Google Scholar] [CrossRef]
- Romanos, G.; Nentwig, G.-H. Diode Laser (980 nm) in Oral and Maxillofacial Surgical Procedures: Clinical Observations Based on Clinical Applications. J. Clin. Laser Med. Surg. 1999, 17, 193–197. [Google Scholar] [CrossRef] [PubMed]
- Desiate, A.; Cantore, S.; Tullo, D.; Profeta, G.; Grassi, F.R.; Ballini, A. 980 nm diode lasers in oral and facial practice: Current state of the science and art. Int. J. Med. Sci. 2009, 6, 358–364. [Google Scholar] [CrossRef] [Green Version]
- Saetti, R.; Silvestrini, M.; Cutrone, C.; Narne, S. Treatment of Congenital Subglottic Hemangiomas. Arch. Otolaryngol. Head Neck Surg. 2008, 134, 848–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferri, E.; Armato, E. Diode laser microsurgery for treatment of Tis and T1 glottic carcinomas. Am. J. Otolaryngol. 2008, 29, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Mittnacht, D.; Linder, A.; Foth, H.-J. Medical Application of a High Power Diode Laser. In Therapeutic Laser Applications and Laser-Tissue Interactions II, In Proceedings of the SPIE—The International Society for Optical Engineering, Munich, Germany, 12–16 Jun 2005; Optical Society of America: Washington, DC, USA, 2005. [Google Scholar]
- Azma, E.; Safavi, N. Diode Laser Application in Soft Tissue Oral Surgery. J. Lasers Med. Sci. 2013, 4, 206–211. [Google Scholar] [PubMed]
- Lee, D.Y.; Cho, J.-G.; Im, N.-R.; Lee, H.-J.; Kim, B.; Jung, K.-Y.; Kim, T.H.; Baek, A.S.-K. Evaluation of the Efficacy of 1940-nm Diode Laser in Tonsillectomy: Preliminary Report. Med. Lasers 2015, 4, 29–34. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.H.; Lim, S.; Oh, D.; Kang, K.; Jung, K.J.; Kim, H.K.; Lee, S.H.; Baek, S.-K.; Kim, A.T.H. Clinical Feasibility Trial of 1,940-nm Diode Laser in Korean Patients with Inferior Turbinate Hypertrophy. Med. Lasers 2015, 4, 60–64. [Google Scholar] [CrossRef] [Green Version]
- Agrawal, A.A.; Prabhu, R.; Sankhe, R.; Wagle, S.V. Influence of external chromophore on cutting efficacy of 940 nm diode laser: An In vitro animal tissue study. Contemp. Clin. Dent. 2018, 9, 79–S82. [Google Scholar] [CrossRef]
- Im, N.-R.; Kim, B.; Kim, J.; Baek, S.-K. Treating Oral Leukoplakia with a 532-nm Pulsed Diode Laser. Med. Lasers 2019, 8, 39–42. [Google Scholar] [CrossRef] [Green Version]
- Kang, H.Y.; Park, E.S.; Nam, S.M. Prospective, Comparative Evaluation of Forearm and Lower Leg Hair Removal with 808-nm Diode Laser at Different Fluences. Med. Lasers 2018, 7, 55–61. [Google Scholar] [CrossRef]
- Im, N.-R.; Moon, J.; Choi, W.; Kim, B.; Lee, J.J.; Kim, H.; Baek, S.-K. Histologic Evaluation of Blood Vessels Sealed with 1,470-nm Diode Laser: Determination of Adequate Condition for Laser Vessel Sealing. Med. Lasers 2018, 7, 6–12. [Google Scholar] [CrossRef]
- Newman, J.; Anand, V. Applications of the diode laser in otolaryngology. Ear Nose Throat J. 2002, 81, 850–851. [Google Scholar] [CrossRef]
- Schmedt, C.-G.; Sroka, R.; Steckmeier, S.; Meissner, O.A.; Babaryka, G.; Hunger, K.; Ruppert, V.; Sadeghi-Azandaryani, M.; Steckmeier, B.M. Investigation on Radiofrequency and Laser (980 nm) Effects after Endoluminal Treatment of Saphenous Vein Insufficiency in an Ex-vivo Model. Eur. J. Vasc. Endovasc. Surg. 2006, 32, 318–325. [Google Scholar] [CrossRef] [Green Version]
- Reynaud, J.P.; Skibinski, M.; Wassmer, B.; Rochon, P.; Mordon, S. Lipolysis using a 980-nm diode laser: A retrospective analysis of 534 procedures. Aesthetic Plast. Surg. 2009, 33, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Weiss, R.A.; Beasley, K. Laser-assisted liposuction using a novel blend of lipid- and water-selective wavelengths. Lasers Surg. Med. 2009, 41, 760–766. [Google Scholar] [CrossRef] [PubMed]
- Tunçel, Ü.; Cömert, E. Preliminary Results of Diode Laser Surgery for Early Glottic Cancer. Otolaryngol. Neck Surg. 2013, 149, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Karasu, M.F.; Gundogdu, R.; Cagli, S.; Aydin, M.; Arli, T.; Aydemir, S.; Yüce, I.; Aydın, M. Comparison of Effects on Voice of Diode Laser and Cold Knife Microlaryngology Techniques for Vocal Fold Polyps. J. Voice 2014, 28, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Hwang, S.M.; Lee, D.Y.; Im, N.-R.; Lee, H.-J.; Kim, B.; Jung, K.-Y.; Kim, T.H.; Baek, A.S.-K. Office-Based Laser Surgery for Benign Laryngeal Lesion. Med. Lasers 2015, 4, 65–69. [Google Scholar] [CrossRef]
- Karkos, P.D.; Stavrakas, M. Minimizing revision rates with the “Π” technique for bilateral vocal fold immobility: A new technique combining carbon dioxide and diode laser. Head Neck 2015, 38, 801–803. [Google Scholar] [CrossRef]
- Karkos, P.D.; Stavrakas, M.; Koskinas, I.; Markou, K.; Triaridis, S.; Constantinidis, J. 5 Years of Diode Laser “Π” Technique for Bilateral Vocal Fold Immobility: A Technique That Improves Airway and Is Friendly to the Voice. Ear Nose Throat J. 2021, 100, 83S–86S. [Google Scholar] [CrossRef]
- Prażmo, E.; Godlewska, A.; Sałkiewicz, M.; Mielczarek, A. Effects of 980 nm diode laser application protocols on the reduction of Enterococcus faecalis intracanal biofilm: An in vitro study. Dent. Med. Probl. 2017, 54, 333–338. [Google Scholar] [CrossRef] [Green Version]
- Wróbel, M.S.; Jędrzejewska-Szczerska, M.; Galla, S.; Piechowski, L.; Sawczak, M.; Popov, A.P.; Bykov, A.V.; Tuchin, V.V.; Cenian, A. Use of optical skin phantoms for preclinical evaluationof laser efficiency for skin lesion therapy. J. Biomed. Opt. 2015, 20, 085003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szymańczyk, J.; Sawczak, M.; Cenian, W.; Karpienko, K.; Jędrzejewska-Szczerska, M.; Cenian, A. Application of the laser diode with central wavelength 975 nm for the therapy of neurofibroma and hemangiomas. J. Biomed. Opt. 2017, 22, 010502. [Google Scholar] [CrossRef] [Green Version]
- Milanic, M.; Cenian, A.; Verdel, N.; Cenian, W.; Stergar, J.; Majaron, B. Temperature Depth Profiles Induced in Human Skin In Vivo Using Pulsed 975 nm Irradiation. Lasers Surg. Med. 2019, 51, 774–784. [Google Scholar] [CrossRef]
- Piechowski, L.; Cenian, W.; Sawczak, M.; Cenian, A. Pulsed dermatologic 20W diode-laser emitting at 975 nm. In Laser Technology 2012: Applications of Lasers, Proceedings of the Tenth Symposium on Laser Technology, Bellingham, WA, USA, 24−28 September 2012; International Society for Optics and Photonics: Bellingham, WA, USA, 2012. [Google Scholar]
- Bodnar, T.; Galdi, G.P.; Necasova, S. Fluid-Structure Interaction and Biomedical Applications; Springer: Basel, Switzerland, 2014. [Google Scholar]
- Badur, J.; Ziółkowski, P.; Zakrzewski, W.; Sławiński, D.; Kornet, S.; Kowalczyk, T.; Hernet, J.; Piotrowski, R.; Felincjancik, J.; Ziółkowski, P.J. An advanced Thermal–FSI approach to flow heating/cooling. J. Phys. Conf. Ser. 2014, 530, 012039. [Google Scholar] [CrossRef] [Green Version]
- Ziółkowski, P.J.; Ochrymiuk, T.; Eremeyev, V.A. Adaptation of the arbitrary Lagrange–Euler approach to fluid–solid interaction on an example of high velocity flow over thin platelet. Contin. Mech. Thermodyn. 2019, 1–14. [Google Scholar] [CrossRef]
- Maitland, D.J.; Eder, D.C.; London, R.A.; Glinsky, M.E.; Soltz, B.A. Dynamic simulations of tissue welding. Proc. Soc. Photo-Opt. Ins. 1996, 2671, 234–242. [Google Scholar]
- Zhou, J.; Liu, J.; Yu, A. Numerical Study on the Thawing Process of Biological Tissue Induced by Laser Irradiation. ASME. J. Biomech. Eng. 2005, 127, 416–431. [Google Scholar]
- Michalik, M.; Podbielska-Kubera, A.; Dmowska-Koroblewska, A. Diode laser-assisted uvulopalatoplasty using palisade technique. New Med. 2018, 22. [Google Scholar] [CrossRef]
- Broda, M.; Michalik, M.; Białas, D.; Różycki, R. Laser dacryocystorhinostomy—The lasers use in treatment of lacrimal duct obstruction. OphthaTherapy Ther. Ophthalmol. 2018, 5, 109–113. [Google Scholar] [CrossRef]
- Michalik, M. The influence of mitomycin C on clinical results of the nasolacrimal duct anastomosis using the diode laser. OphthaTherapy Ther. Ophthalmol. 2019, 6, 274–278. [Google Scholar] [CrossRef]
- Guerra, R.C.; de Luca, D.N.; Pereira, R.S.; Carvalho, P.H.A.; Homsi, N.; Radaic, P.; Pastore, G.P.; Hochuli-Vieira, E. TMJ diode surgical laser approach in a contemporary treatment of tempomandibular joint pathologies. A technical note. Oral Surg. 2021, 14, 206–208. [Google Scholar] [CrossRef]
- Hanke, A.; Fimmers, R.; Frentzen, M.; Meister, J. Quantitative determination of cut efficiency during soft tissue surgery using diode lasers in the wavelength range between 400 and 1500 nm. Lasers Med. Sci. 2021, 1–15. [Google Scholar] [CrossRef]
- Goel, R.; Nagpal, S.; Garg, S.; Malik, K.P.S. Is transcanalicular laser dacryocystorhinostomy using low energy 810 nm diode laser better than 980 nm diode laser? Oman J. Ophthalmol. 2015, 8, 134. [Google Scholar] [CrossRef]
- George, S.; Hamblin, M.R.; Abrahamse, H. Photobiomodulation-Induced Differentiation of Immortalized Adipose Stem Cells to Neuronal Cells. Lasers Surg. Med. 2020, 52, 1032–1040. [Google Scholar] [CrossRef]
- Akduman, L.; Olk, R.J. Diode Laser (810 nm) versus Argon Green (514 nm) Modified Grid Photocoagulati-on for Diffuse Diabetic Macular Edema. Ophthalmology 1997, 104, 1433–1441. [Google Scholar] [CrossRef]
- Wollina, U.; Goldman, A. The dual 980-nm and 1470-nm diode laser for vascular lesions. Dermatol. Ther. 2020, 33, 085003. [Google Scholar] [CrossRef] [PubMed]
- Wendt-Nordahl, G.; Huckele, S.; Honeck, P.; Alken, P.; Knoll, T.; Michel, M.S.; Häcker, A. 980-nm Diode Laser: A Novel Laser Technology for Vaporization of the Prostate. Eur. Urol. 2007, 52, 1723–1728. [Google Scholar] [CrossRef]
- Arif, R.H.; Kareem, F.A.; Zardawi, F.M.; Al-Karadaghi, T.S. Efficacy of 980 nm diode laser and 2940 nm Er: YAG laser in gingival depigmentation: A comparative study. J. Cosmet. Dermatol. 2021, 20, 1684–1691. [Google Scholar] [CrossRef]
- Betka, J.; Plzák, J.; Zábrodský, M.; Kastner, J.; Boucek, J. Lasers in otorhinolaryngology (ORL) and head and neck surgery. In Lasers for Medical Applications; Woodhead Publishing: Sawston, UK, 2013; pp. 556–572. [Google Scholar] [CrossRef]
- Abiri, A.; Bs, K.G.; Maducdoc, M.; Sahyouni, R.; Wang, M.B.; Kuan, E.C. Laser-Assisted Control of Epistaxis in Hereditary Hemorrhagic Telangiectasia: A Systematic Review. Lasers Surg. Med. 2020, 52, 293–300. [Google Scholar] [CrossRef] [PubMed]
- Ferlito, S.; Nane, S.; Grillo, C.; Maugeri, M.; Cocuzza, S.; Grillo, C. Diodes laser in ENT surgery. Acta Med. Mediterr. 2011, 27, 79. [Google Scholar]
- Massaro, B.M.; Gonnering, R.S.; Harris, G.J. Endonasal laser dacryocystorhinostomy. A new approach to nasolacrimal duct obstruction. Arch. Ophthalmol. 1990, 108, 1172–1186. [Google Scholar] [CrossRef] [PubMed]
- Silkiss, R.Z.; Axelrod, R.N.; Iwach, A.G.; Vassiliadis, A.; Hennings, D.R. Transcanalicular THC: YAG dacryocystorhinostomy. Ophthalmic Surg. 1992, 23, 351–353. [Google Scholar] [PubMed]
- Nowak, R.; Rekas, M.; Gospodarowicz, I.N.; Ali, M.J. Long-term outcomes of primary transcanalicular laser dacryocystorhinostomy. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 54, 1–6. [Google Scholar] [CrossRef]
- Yaroslavsky, I.; Boutoussov, D.; Vybornov, A.; Perchuk, I.; Meleshkevich, V.; Altshuler, G.B. Ex vivo evaluation of super pulse diode laser system with smart temperature feedback for contact soft-tissue surgery. In Lasers in Dentistry XXIV, Proceedings of the SPIE BiOS, Bellingham, WA, USA, 27 January−1 February 2018; International Society for Optics and Photonics: Bellingham, WA, USA, 2018; p. 104730. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| λ (nm) | Operation Mode | Applications Field | Ref. |
|---|---|---|---|
| 810 ± 10 | cw and pulsed | photobiomodulation (PBM)—also known as biostimulation or low level laser therapy—LLLT, dental biostimulation, neuronal differentiation | [4,48] |
| τ ~ 5–15 ms ok. 30 Hz | lesion tissue: telangiectasias, spider veins, capillary dermal malformation and a cutaneous venous malformation | [10] | |
| NA | vascular ophtalmology, | [49] | |
| cw and pulsed | congenital subglottic hemangiomas | [13] | |
| cw | Tis and T1 glottic carcinomas | [14] | |
| cw, 3.5 W | Pyogenic granuloma | [16] | |
| 8–10 W τ~ 0.5–1 s | Laser assisted dacryocystorhinostomy | [43] | |
| p. 30 ms, 7 Hz | hair removal | [21] | |
| 5 W, τ = 4 s | Laryngology: laser-assisted somnoplasty, frenuloplasty, closure of tonsillar crypts, haemostasis, removal of cancerous changes, blepharoplasty, surgery of laryngopharynx and larynx, separation of adhesions in nasal septum | here | |
| 980 ± 10 | cw, pulsed | photobiomodulation (PBM)—also known as biostimulation or low level laser therapy—LLLT, wound and ulcers healing applications | [7] |
| pulsed, cw | tissue tumors, frenectomies, excision of gingival hyperplasias, vestibuloplasties, hemangioma removal, and periimplant | [11] | |
| NA | turbinate reduction, nasal polypectomy, ablation of an oral papilloma, photocoagulation of nasal telangiectasias, | [23] | |
| NA | endovenous laser treatment of saphenous veins | [24] | |
| NA | telangiectasias | [12] | |
| cw | early glottic cancer | [27] | |
| cw | vocal fold polyps | [28] | |
| Ceralas D15, 12 W superpulse | laryngeal lesions: vocal polyps, leucoplakia, laryngeal hair, granuloma, subglottic stenosis and tracheal lesions | [29] | |
| cw, | dermatology: neurofibroma, hemangioma | [34] | |
| τ = 50 ms, 10 Hz | |||
| dual 980/1470 nm | vascular lesions of skin and lips: cherry angiomas, venous lakes, lip hemangioma, and spider nevi, couperose, facial telangiectasia | [50] | |
| cw, 30–120 W | prostate treatment | [51] | |
| τ = 0.1 s, 5–9 Hz | |||
| NA | ophthalmology | [47] | |
| 3 W (100 Hz) | removal of intracanal Enterococcus faecalis biofilm | [32] | |
| cw 8 to 9 W | bilateral vocal fold immobility (BVFI) | [30,31] | |
| cw 3–4 W | Maxillofacial surgeries including intrinsic TMJ pathologies | [45] | |
| cw 1.5 W | gingival depigmentation | [52] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Michalik, M.; Szymańczyk, J.; Stajnke, M.; Ochrymiuk, T.; Cenian, A. Medical Applications of Diode Lasers: Pulsed versus Continuous Wave (cw) Regime. Micromachines 2021, 12, 710. https://doi.org/10.3390/mi12060710
Michalik M, Szymańczyk J, Stajnke M, Ochrymiuk T, Cenian A. Medical Applications of Diode Lasers: Pulsed versus Continuous Wave (cw) Regime. Micromachines. 2021; 12(6):710. https://doi.org/10.3390/mi12060710
Chicago/Turabian StyleMichalik, Michał, Jacek Szymańczyk, Michał Stajnke, Tomasz Ochrymiuk, and Adam Cenian. 2021. "Medical Applications of Diode Lasers: Pulsed versus Continuous Wave (cw) Regime" Micromachines 12, no. 6: 710. https://doi.org/10.3390/mi12060710