
Wearable Contact Lens Sensor for Non-Invasive Continuous Monitoring of Intraocular Pressure

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
3. Fabrication
4. Testing
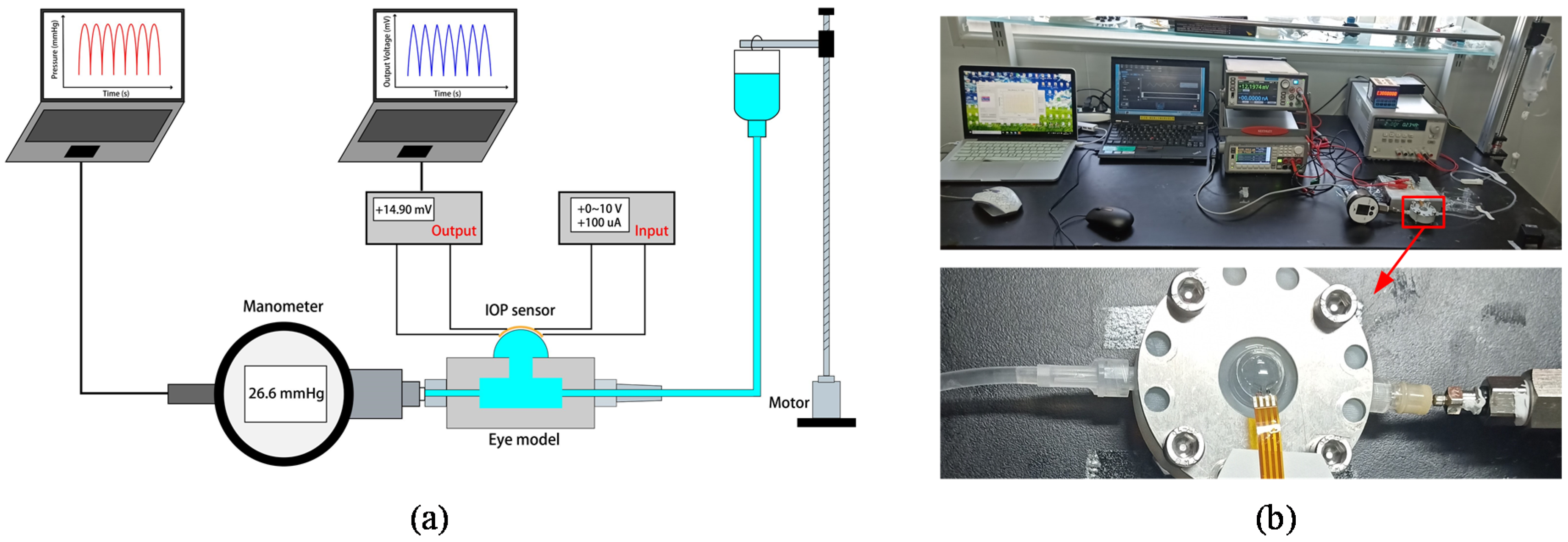
4.1. Setup of the Testing Systems
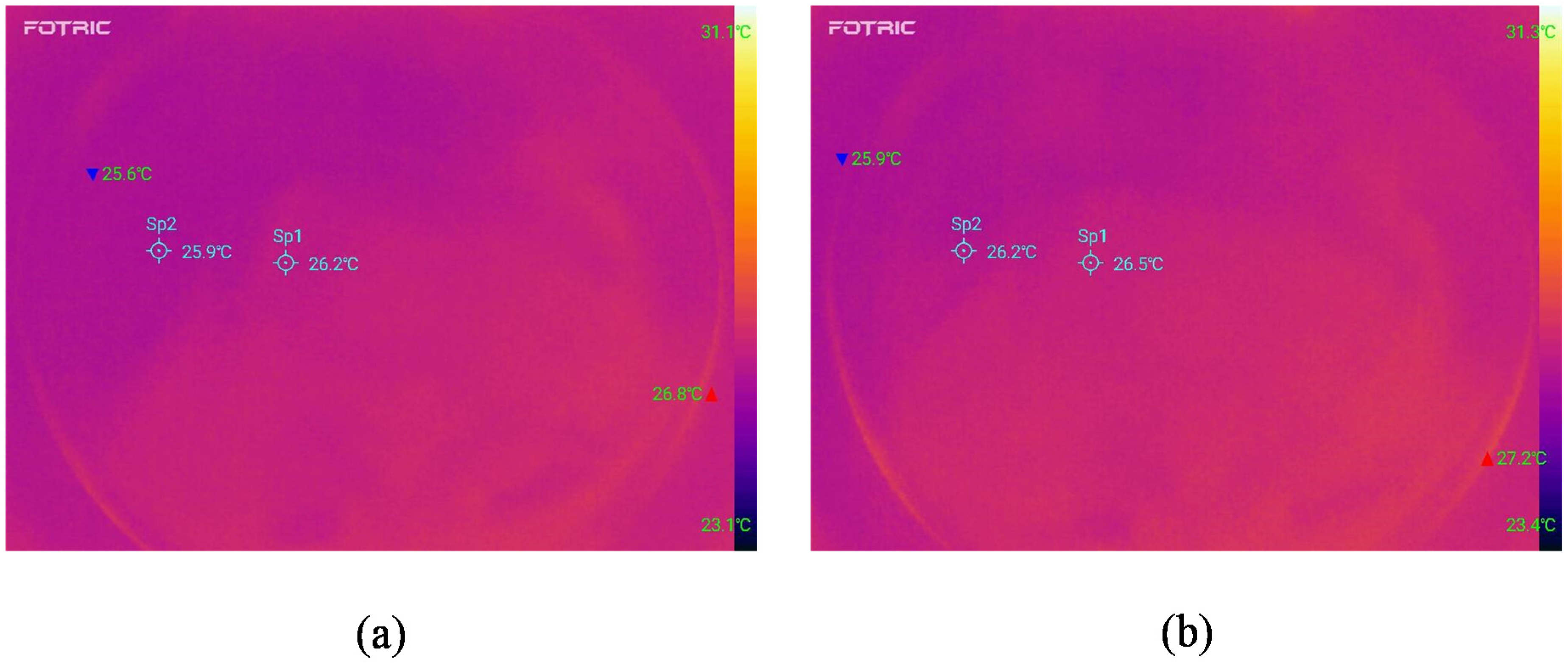
4.2. Temperature Characteristics
5. Results and Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tham, Y.-C.; Li, X.; Wong, T.Y.; Quigley, H.A.; Aung, T.; Cheng, C.-Y. Global prevalence of glaucoma and projections of glaucoma burden through 2040: A systematic review and meta-analysis. Ophthalmology 2014, 121, 2081–2090. [Google Scholar] [CrossRef] [PubMed]
- Weinreb, R.N.; Khaw, P.T. Primary open-angle glaucoma. Lancet 2004, 363, 1711–1720. [Google Scholar] [CrossRef]
- Barkana, Y.; Anis, S.; Liebmann, J.; Tello, C.; Ritch, R.J. Clinical utility of intraocular pressure monitoring outside of normal office hours in patients with glaucoma. Arch. Ophthalmol. 2006, 124, 793–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hughes, E.; Spry, P.; Diamond, J. 24-hour monitoring of intraocular pressure in glaucoma management: A retrospective review. J. Glaucoma 2003, 12, 232–236. [Google Scholar] [CrossRef] [PubMed]
- Yung, E.; Trubnik, V.; Katz, L.J. An overview of home tonometry and telemetry for intraocular pressure monitoring in humans. Graefe’s Arch. Clin. Exp. Ophthalmol. 2014, 252, 1179–1188. [Google Scholar] [CrossRef]
- Moses, R.A. The Goldmann applanation tonometer. Am. J. Ophthalmol. 1958, 46, 865–869. [Google Scholar] [CrossRef]
- Ge, G.; Huang, W.; Shao, J.J.; Dong, X.C. Recent progress of flexible and wearable strain sensors for human-motion monitoring. J. Semicond. 2018, 39, 011012. [Google Scholar] [CrossRef]
- Yang, X.; Cheng, H. Recent Developments of Flexible and Stretchable Electrochemical Biosensors. Micromachines 2020, 11, 243. [Google Scholar] [CrossRef] [Green Version]
- Ma, Z.; Kong, D.S.; Pan, L.J.; Bao, Z.N. Skin-inspired electronics: Emerging semiconductor devices and systems. J. Semicond. 2020, 41, 041601. [Google Scholar] [CrossRef]
- Park, Y.-G.; Cha, E.; An, H.S.; Lee, K.-P.; Song, M.H.; Kim, H.K.; Park, J.-U. Wireless phototherapeutic contact lenses and glasses with red light-emitting diodes. Nano Res. 2020, 13, 1347–1353. [Google Scholar] [CrossRef]
- Keum, D.H.; Kim, S.-K.; Koo, J.; Lee, G.-H.; Jeon, C.; Mok, J.W.; Mun, B.H.; Lee, K.J.; Kamrani, E.; Joo, C.-K.; et al. Wireless smart contact lens for diabetic diagnosis and therapy. Sci. Adv. 2020, 6, eaba3252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, P.-J.; Saati, S.; Varma, R.; Humayun, M.S.; Tai, Y.-C. Wireless intraocular pressure sensing using microfabricated minimally invasive flexible-coiled LC sensor implant. J. Microelectromech. Syst. 2010, 19, 721–734. [Google Scholar] [CrossRef]
- Todani, A.; Behlau, I.; Fava, M.A.; Cade, F.; Cherfan, D.G.; Zakka, F.R.; Jakobiec, F.A.; Gao, Y.; Dohlman, C.H.; Melki, S.A. Intraocular pressure measurement by radio wave telemetry. Investig. Ophthalmol. Vis. Sci. 2011, 52, 9573–9580. [Google Scholar] [CrossRef] [PubMed]
- Xue, N.; Chang, S.-P.; Lee, J.-B. A SU-8-based microfabricated implantable inductively coupled passive RF wireless intraocular pressure sensor. J. Microelectromech. Syst. 2012, 21, 1338–1346. [Google Scholar] [CrossRef]
- Lin, J.C.-H.; Zhao, Y.; Chen, P.-J.; Humayun, M.; Tai, Y.-C. Feeling the pressure: A parylene-based intraocular pressure sensor. IEEE Nanotechnol. Mag. 2012, 6, 8–16. [Google Scholar] [CrossRef]
- Chitnis, G.; Maleki, T.; Samuels, B.; Cantor, L.B.; Ziaie, B. A minimally invasive implantable wireless pressure sensor for continuous IOP monitoring. IEEE Trans. Biomed. Eng. 2012, 60, 250–256. [Google Scholar] [CrossRef]
- Lee, J.O.; Park, H.; Du, J.; Balakrishna, A.; Chen, O.; Sretavan, D.; Choo, H. A microscale optical implant for continuous in vivo monitoring of intraocular pressure. Microsyst. Nanoeng. 2017, 3, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Hui, P.C.; Shtyrkova, K.; Zhou, C.; Chen, X.; Chodosh, J.; Dohlman, C.H.; Paschalis, E.I. Implantable self-aligning fiber-optic optomechanical devices for in vivo intraocular pressure-sensing in artificial cornea. J. Biophotonics 2020, 13, e202000031. [Google Scholar]
- Leonardi, M.; Leuenberger, P.; Bertrand, D.; Bertsch, A.; Renaud, P. A soft contact lens with a MEMS strain gage embedded for intraocular pressure monitoring. In Proceedings of the TRANSDUCERS ’03. 12th International Conference on Solid-State Sensors, Actuators and Microsystems, Boston, MA, USA, 8–12 June 2003; pp. 1043–1046. [Google Scholar]
- Agaoglu, S.; Diep, P.; Martini, M.; Samudhyatha, K.; Baday, M.; Araci, I. Ultra-sensitive microfluidic wearable strain sensor for intraocular pressure monitoring. Lab Chip 2018, 18, 3471–3483. [Google Scholar] [CrossRef] [PubMed]
- An, H.; Chen, L.; Liu, X.; Zhao, B.; Zhang, H.; Wu, Z. Microfluidic contact lenses for unpowered, continuous and non-invasive intraocular pressure monitoring. Sens. Actuators A Phys. 2019, 295, 177–187. [Google Scholar] [CrossRef]
- Campigotto, A.; Leahy, S.; Zhao, G.; Campbell, R.J.; Lai, Y. Non-invasive Intraocular pressure monitoring with contact lens. Br. J. Ophthalmol. 2020, 104, 1324–1328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maeng, B.; Chang, H.-K.; Park, J. Photonic crystal-based smart contact lens for continuous intraocular pressure monitoring. Lab Chip 2020, 20, 1740–1750. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.-Z.; Chan, I.-S.; Lam, D.C. Capacitive contact lens sensor for continuous non-invasive intraocular pressure monitoring. Sens. Actuators A Phys. 2013, 203, 112–118. [Google Scholar] [CrossRef]
- Liu, L.J.; Wang, J.B.; Chen, D.Y.; Chen, J. Non-Invasive Wireless and Passive MEMS Intraocular Pressure Sensor Based on Flexible Substrate. Appl. Mech. Mater. 2015, 748, 115–127. [Google Scholar] [CrossRef]
- Chiou, J.-C.; Huang, Y.-C.; Yeh, G.-T. A capacitor-based sensor and a contact lens sensing system for intraocular pressure monitoring. J. Micromech. Microeng. 2015, 26, 015001. [Google Scholar] [CrossRef]
- Chen, G.-Z.; Chan, I.-S.; Leung, L.K.; Lam, D.C. Soft wearable contact lens sensor for continuous intraocular pressure monitoring. Med. Eng. Phys. 2014, 36, 1134–1139. [Google Scholar] [CrossRef]
- Kouhani, M.H.M.; Wu, J.; Tavakoli, A.; Weber, A.J.; Li, W. Wireless, passive strain sensor in a doughnut-shaped contact lens for continuous non-invasive self-monitoring of intraocular pressure. Lab Chip 2020, 20, 332–342. [Google Scholar] [CrossRef]
- Leonardi, M.; Leuenberger, P.; Bertrand, D.; Bertsch, A.; Renaud, P. First steps toward noninvasive intraocular pressure monitoring with a sensing contact lens. Investig. Ophthalmol. Vis. Sci. 2004, 45, 3113–3117. [Google Scholar] [CrossRef]
- Leonardi, M.; Pitchon, E.M.; Bertsch, A.; Renaud, P. Wireless contact lens sensor for intraocular pressure monitoring: Assessment on enucleated pig eyes. Acta Ophthalmol. 2009, 87, 433–437. [Google Scholar] [CrossRef]
- Laukhin, V.; Sánchez, I.; Moya, A.; Laukhina, E.; Martin, R.; Ussa, F.; Rovira, C.; Guimera, A.; Villa, R.; Aguiló, J.; et al. Non-invasive intraocular pressure monitoring with a contact lens engineered with a nanostructured polymeric sensing film. Sens. Actuators A Phys. 2011, 170, 36–43. [Google Scholar] [CrossRef]
- Pang, Y.; Li, Y.; Wang, X.; Qi, C.; Yang, Y.; Ren, T.-L. A contact lens promising for non-invasive continuous intraocular pressure monitoring. RSC Adv. 2019, 9, 5076–5082. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Kim, J.; Ku, M.; Cha, E.; Ju, S.; Park, W.Y.; Kim, K.H.; Kim, D.W.; Berggren, P.-O.; Park, J.-U. Intraocular pressure monitoring following islet transplantation to the anterior chamber of the eye. Nano Lett. 2019, 20, 1517–1525. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Zhu, Y.; Nomani, M.W.; Wen, X.; Hsia, T.-Y.; Koley, G. A highly sensitive pressure sensor using a Au-patterned polydimethylsiloxane membrane for biosensing applications. J. Micromech. Microeng. 2013, 23, 025022. [Google Scholar] [CrossRef]
- Chen, J.; Zheng, J.; Gao, Q.; Zhang, J.; Zhang, J.; Omisore, O.M.; Wang, L.; Li, H. Polydimethylsiloxane (PDMS)-Based Flexible Resistive Strain Sensors for Wearable Applications. Appl. Sci. 2018, 8, 345. [Google Scholar] [CrossRef] [Green Version]
- Cho, D.; Park, J.; Kim, T.; Jeon, S. Recent advances in lithographic fabrication of micro-/nanostructured polydimethylsiloxanes and their soft electronic applications. J. Semicond. 2019, 40, 57–74. [Google Scholar] [CrossRef]
- Zhang, J.; Nagao, Y.; Kuwano, S.; Ito, Y. Microstructure and temperature coefficient of resistance of platinum films. Jpn. J. Appl. Phys. 1997, 36, 834. [Google Scholar] [CrossRef]
- Purslow, C.; Wolffsohn, J.S. Ocular surface temperature: A review. Eye Contact Lens Sci. Clin. Pract. 2005, 31, 117–123. [Google Scholar] [CrossRef]
- Chen, W.; Zhou, X.F.; Kang, Y.H. Research on advances of intraocular pressure measuring technology. Int. Eye Sci. 2012, 12, 882–887. [Google Scholar]
- Ye, J.; Lin, Z.; You, J.; Huang, S.; Wu, H. Inconsistency Calibrating Algorithms for Large Scale Piezoresistive Electronic Skin. Micromachines 2020, 11, 162. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
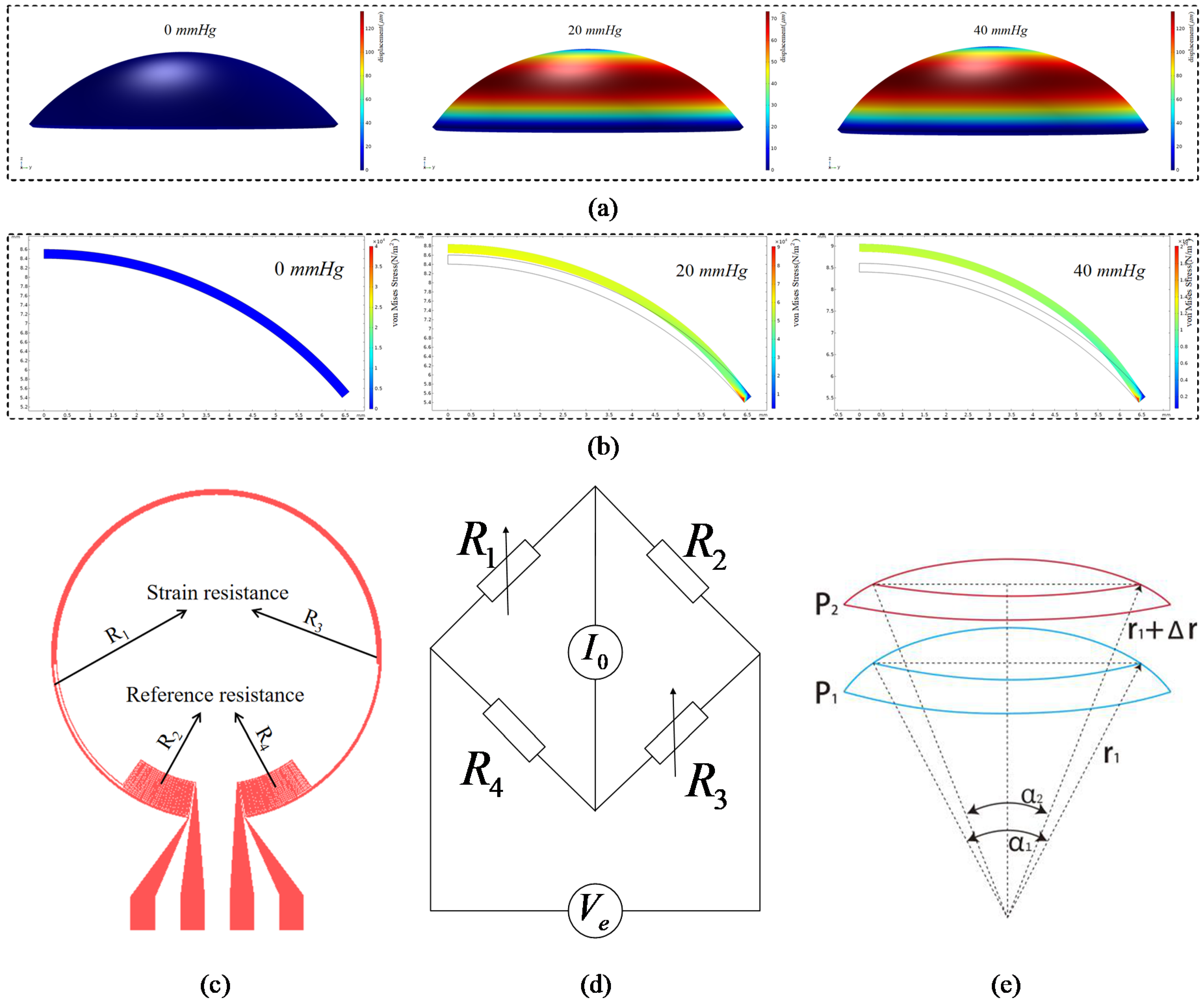
| Number of strain resistance turns | 3 |
| Outer diameter of strain resistance | 10 mm |
| Inner diameter of strain resistance | 9.71 mm |
| Outer diameter of reference resistance | 9.68 mm |
| Inner diameter of reference resistance | 7.87 mm |
| Width of strain gauge | 5 μm |
| Thickness of strain gauge | 100 nm |
| The diameter of the contact lens | 14 mm |
| Reference | Invasive or Non-Invasive | Method | Sensitivity |
|---|---|---|---|
| [12] | invasive | capacitance | 160 kHz/mmHg |
| [16] | invasive | capacitance | 15 kHz/mmHg |
| [22] | non-invasive | microfluidic | 28 μm/mmHg |
| [24] | non-invasive | capacitance | 23 kHz/mmHg |
| [27] | non-invasive | inductance | 8 kHz/mmHg |
| [28] | non-invasive | inductance | 35.1 kHz/mmHg |
| [29] | non-invasive | resistance strain | 8.37 μV/mmHg |
| [30] | non-invasive | resistance strain | 113 μV/mmHg |
| [32] | non-invasive | resistance strain | 20 μV/mmHg |
| This work | non-invasive | resistance strain | 289.5 μV/mmHg |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dou, Z.; Tang, J.; Liu, Z.; Sun, Q.; Wang, Y.; Li, Y.; Yuan, M.; Wu, H.; Wang, Y.; Pei, W.; et al. Wearable Contact Lens Sensor for Non-Invasive Continuous Monitoring of Intraocular Pressure. Micromachines 2021, 12, 108. https://doi.org/10.3390/mi12020108
Dou Z, Tang J, Liu Z, Sun Q, Wang Y, Li Y, Yuan M, Wu H, Wang Y, Pei W, et al. Wearable Contact Lens Sensor for Non-Invasive Continuous Monitoring of Intraocular Pressure. Micromachines. 2021; 12(2):108. https://doi.org/10.3390/mi12020108
Chicago/Turabian StyleDou, Zhiqiang, Jun Tang, Zhiduo Liu, Qigong Sun, Yang Wang, Yamin Li, Miao Yuan, Huijuan Wu, Yijun Wang, Weihua Pei, and et al. 2021. "Wearable Contact Lens Sensor for Non-Invasive Continuous Monitoring of Intraocular Pressure" Micromachines 12, no. 2: 108. https://doi.org/10.3390/mi12020108