3.1. Correction Factor (CF) and Approximate Factors (F1 and F2) via Numerical Simulation
To find two approximate factors (
F1,
F2) in Equation (11), it was necessary to obtain the
CF by conducting numerical simulation with CFD software (CFD-ACE+, ESI Group, Paris, France). For convenience, the flow rate of the blood sample was assumed to be
QB = 1 mL/h. The viscosities of both fluids (blood sample, reference fluid) were assumed as
μB = 1 cP and
μR = 1 cP, respectively.
Figure 2A showed variations of the interface (
αB) through numerical simulation with respect to the flow-rate ratio (
QR/QB) ((a)
QR/QB = 1, (b)
QR/QB = 0.8, (c)
QR/QB = 0.6, (d)
QR/QB = 0.4, (e)
QR/QB = 0.2, and (f)
QR/QB = 0.1). The interfaces (
αB) for the corresponding flow-rate ratio (
QR/QB) were obtained as (a)
αB = 0.5 for
QR/QB = 1, (b)
αB = 0.553 for
QR/QB = 0.8, (c)
αB = 0.619 for
QR/QB = 0.6, (d)
αB = 0.704 for
QR/QB = 0.4, (e)
αB = 0.818 for
QR/QB = 0.2, and (f)
αB = 0.891 for
QR/QB = 0.1.
According to the coflowing-streams method [
22,
23], the viscosity ratio of the blood sample to the reference fluid (
μB/
μR) was obtained as
by quantifying the interface (
αB) in coflowing streams at the same flow-rate condition (
QB =
QR). The normalized viscosity of the blood sample was obtained by dividing the estimated viscosity (
μest =
μR·
αB/(1 −
αB)) by the given viscosity (
μgiven = 1 cP) (
μn =
μest/
μgiven). As shown in
Figure 2B, variations of
μn were obtained by varying the interface (0.1 <
αB < 0.9). When the interface was located at the center line (
αB = 0.5),
μn was given as
μn = 1. In other words, the blood viscosity could be measured accurately when the interface was located at the center line [
24]. However, when
αB was relocated from the center line to both walls,
μn tended to decrease by approximately 0.8. Because the viscosity of the blood sample was given as
μB = 1 cP, the coflowing-streams method exhibited a large measurement error of approximately 20% when compared with the given viscosity of the blood sample. The reason could be explained by the boundary condition difference between the real physical model and simple mathematical model. Instead of a real and complex model, to construct a simple model of coflowing streams, the coflowing-streams method assumed that the interface of two streams was a virtual wall. In other words, it assumed that the interface was a virtual-wall boundary. Because the
CF varied by channel dimensions (width and depth), the
CF was calculated by referring to the general procedure discussed in previous studies [
17,
19]. The
CF was then estimated by the reciprocating
μn obtained at a specific interface (
CF·(αn) =
μn−1 for
αn). As shown in
Figure 2B, the
CF was obtained as
CF = 1 at the center line (
αB = 0.5). However, the
CF tended to increase gradually when the interface moved to both walls. According to regression analysis, the
CF was obtained as
CF = 4.2162
αB4 – 8.4325
αB3 + 7.0763
αB2 − 2.86
αB + 1.4599 (
R2 = 0.9912). By inserting the correction factor into the coflowing-streams method, the viscosity of the blood sample was estimated with
. The coflowing method with correction factor could be used to measure the viscosity of blood with a specific hematocrit. Based on Equation (12), the approximate factor (
F1) was obtained as
F1 = 1.094. As shown in
Figure 2C, variations of
and
were obtained with respect to α
B. The normalized difference (
ND) between both terms exhibited its maximum value at the center and both walls. The normalized difference was less than 10%. Additionally, according to Equation (13), the approximate factor (
F2) was obtained as
F2 = 1.1087. As shown in
Figure 2D, variations of
and
were obtained with respect to α
B. The maximum value of normalized difference was estimated to be approximately 11%. The simulation study showed that the two approximate factors (
F1 =1.094,
F2 =1.1087) could give consistent results when compared with the original expression. Using
F1 and
F2, the nonlinear Equation (10) was converted into the simple linear Equation (11) for consistency.
3.2. Effect of Period (T) on Viscoelasticity of Blood Sample
To verify the contribution of the period (
T) to the viscoelasticity of the blood sample (Equations [
18] and [
20]), the viscosity and compliance were evaluated by varying the period (
T = 120, 240, 360, and 480 s). The blood sample (
Hct = 50%) was prepared by adding normal RBCs into 1x PBS.
Q0 and
Q1 of the two syringe pumps were controlled at
Q0 = 1 and
Q1 = 0.5 mL/h, respectively. For a rectangular channel with a lower aspect ratio, the shear rate (
) was derived as
[
19]. Based on the shear rate formula, the shear rates of the corresponding flow rate were estimated as
for
QB = 0.5 mL/h and
for
QB = 1.5 mL/h. Because the shear rate (
) was much greater than 1000 s
-1, it was reasonable that the blood sample behaves as a Newtonian fluid. In other words, the blood viscosity (
μB) remained constant within the specific flow rates of the blood sample.
As shown in
Figure 3A, temporal variations of
αB and
βB = (1 −
αB)
−1 were obtained with respect to the period ((a)
T = 120 s, (b)
T = 240 s, (c)
T = 360 s, and (d)
T = 480 s). Based on Equations (21)–(23),
β0 and
β1 were obtained at an interval of the corresponding period.
Figure 3B-a showed variations of
β0 and
β1 with respect to
T, where
β0 and
β1 fluctuated at a shorter period (
T = 120, 360 s). However, they remained stable at a longer period (
T = 360, 480 s).
Figure 3B-b showed variations of
λB with respect to
T. The
λB tended to increase linearly for up to
T = 360 s. However, the slope of
λB tended to decrease between
T= 360 and
T = 480 s. According to Equation (19), the
λB was linearly proportional to the period (i.e.,
λB ~
T). The experimental results showed appropriately consistent variations of
λB with respect to
T. Using Equations (18) and (20), the blood viscosity (
μB) and compliance (
CB) were obtained with respect to
T. As shown in
Figure 3B-c,
μB did not exhibit a linear dependency of
T. It fluctuated at a shorter period. However, it remained constant at a longer period (
T = 360, 480 s). The results agreed with Equation (18), which did not relate to the period. It was necessary, however, to set a longer period for consistently measuring the viscosity of the blood sample. Compliance (
CB) tended to increase linearly for up to
T = 360 s. The slope of
CB tended to decrease between
T = 360 and
T = 480 s. According to the mathematical relation,
CB was linearly proportional to
λB. The experimental results indicated that blood viscosity was independent of period. However, compliance varied linearly depending on the period.
From the results, for consistent measurement of viscoelasticity (blood viscosity and compliance), the period of the syringe pump was set to a longer period of T = 360 s throughout all experiments for convenience.
3.3. Quantification of the Effect of Hematocrit on Blood Viscoelasticity
According to a previous study, hematocrit caused an increase in blood viscosity and elasticity [
16]. In addition, a blood sample with a low hematocrit (
Hct = 30%) exhibited a continuous ESR occurring in a driving syringe [
25]. According to the previous study, to increase the ESR significantly, a blood sample was prepared by adding normal RBCs into various concentrations of dextran solution (
Cdex = 2, 5, 8, and 10 mg/mL). Because the hematocrit of the blood sample flowing in the microfluidic channel varied continuously over time, RBC aggregation or blood viscosity tended to vary continuously [
19]. In this study, under blood perfusion with a sinusoidal flow-rate pattern, the contribution of hematocrit to blood viscoelasticity and ESR was quantified by varying the hematocrit. To induce the ESR in a driving syringe, plasma was used as the diluent. In other words, blood samples (
Hct = 30%, 40%, 50%, and 60%) were prepared by adding normal RBCs into the plasma.
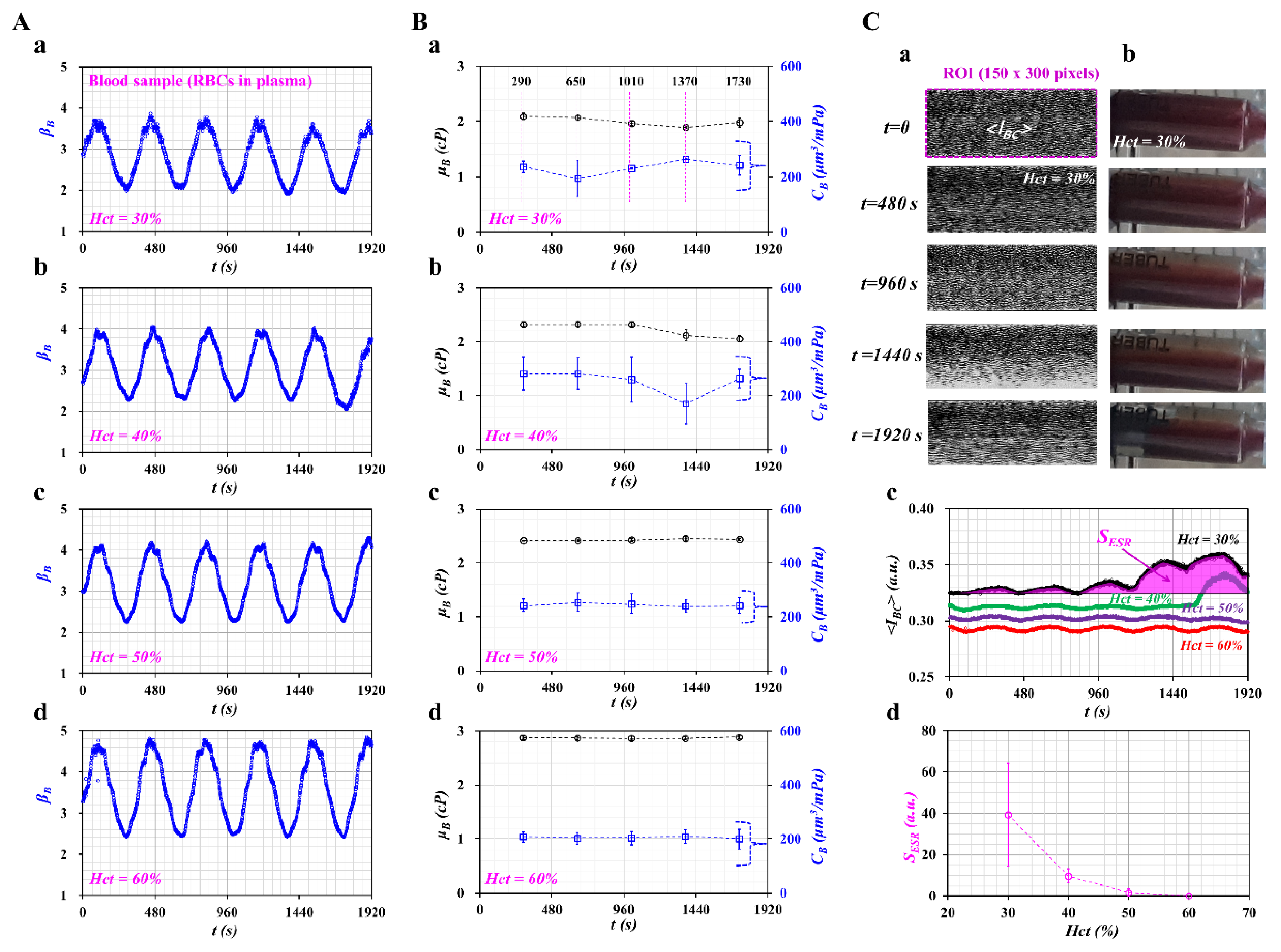
Figure 4A showed temporal variations of
βB with respect to hematocrit ((a)
Hct = 30%, (b)
Hct = 40%, (c)
Hct = 50%, and (d)
Hct = 60%). Using temporal variations of
βB, blood viscosity and compliance were obtained at an interval of a specific period. As shown in
Figure 4B, temporal variations of
μB and
CB were obtained with respect to hematocrit ((a)
Hct = 30%, (b)
Hct = 40%, (c)
Hct = 50%, and (d)
Hct = 60%). Both parameters were obtained as mean ± standard deviation at a specific time (
t = 290, 650, 1010, 1370, and 1730 s).
For the blood sample with
Hct = 30%, compliance (
CB) fluctuated greatly over time. It tended to decrease after
t = 290 s, but it tended to increase between
t = 650 and
t = 1370 s. After
t = 1370 s, it remained constant over time. Blood viscosity tended to decrease after
t = 650 s. In other words, the ESR of RBCs in a driving syringe accelerated over time. In other words, after a certain time, the hematocrit of the blood sample tended to decrease. Thus,
μB tended to decrease, and
CB tended to increase with an elapse of time. For the blood sample with
Hct = 40%, blood viscosity tended to decrease after
t = 1010 s. Compliance remained constant for up to
t = 1010 s. After that, it fluctuated over time. When the hematocrit increased from
Hct = 30% to
Hct = 40%, the time when
CB had the minimum value tended to increase substantially. However, for the blood samples with high hematocrit (
Hct = 50%, 60%), blood viscosity and compliance remained constant over time. The blood viscosity tended to increase at a higher hematocrit. The compliance tended to decrease at a higher hematocrit. According to a previous study, blood elasticity tended to increase with respect to hematocrit [
16]. When compared with the previous result, compliance tended to decrease with respect to the hematocrit. The experimental results can be considered reasonable, because compliance had the reciprocal of elasticity (i.e., compliance ~ 1/elasticity).
To quantify the ESR that occurred in a driving syringe, the microscopic image intensities of the blood sample were obtained over time. A driving syringe was installed horizontally. Because of the ESR in the driving syringe, the hematocrit of the blood sample flowing in a microfluidic channel tended to decrease over time. Here, variations of hematocrit were used by monitoring the image intensity of the blood sample [
26].
Figure 4C-a showed microscopic images of the blood sample (
Hct = 30%) flowing in the blood sample channel over time (
t = 0, 480, 960, 1440, and 1920 s). After
t = 960 s, the number of RBCs tended to decrease significantly. The image intensity tended to increase. At
t = 1920 s, the image intensity tended to decrease as RBCs tended to increase significantly. The contrast of each image was enhanced by conducting image processing with the software Image-J (NIH, Maryland, USA). A specific ROI (300 x 150 pixels) in the blood sample channel was selected to quantify the image intensity (<
IBC>). To visualize the ESR in a driving syringe, a side view of a syringe filled with a blood sample (
Hct = 30%) was captured sequentially with a smartphone camera (Galaxy A5, Samsung, Korea). As lower level of hematocrit exhibited higher value of
<IBC>, the results of blood sample (
Hct = 30%) was selected and summarized at a specific time.
Figure 4C-b showed snapshots of a driving syringe over time (
t) (
t = 0, 480, 960, 1440, and 1920 s). Before
t = 480 s, there was no indication of the ESR occurring in a driving syringe, because the RBCs were distributed uniformly. After
t = 960 s, because of the continuous ESR, the blood sample inside the syringe was separated into two regions: an RBC-rich region (i.e., lower layer) and an RBC-free region (i.e., upper layer). As shown in
Figure 4C-a, the ESR in the driving syringe caused a reduced number of RBCs in the microfluidic channel. To quantify the decrease in hematocrit resulting from ESR in the driving syringe, the image intensity of the blood sample (<
IBC>) was obtained over time.
Figure 4C-c showed temporal variations of
<IBC> with respect to
Hct = 30%, 40%, 50%, and 60%. For a blood sample with
Hct = 30%, <
IBC> tended to increase after
t = 1190 s. For a blood sample with
Hct = 40%, image intensity tended to increase after
t = 1570 s. For blood samples with a high hematocrit (
Hct = 50%, 60%), the image intensity remained constant over time. This result showed that a lower hematocrit contributed to varying image intensity (or numbers of RBCs) of blood samples flowing in a microfluidic channel. According to a specific parameter (
SESR) suggested in a previous study [
20], variations of ESR were quantified with respect to
Hct. The
SESR was obtained as
. Here,
Imin represents the minimum value of <
IBC> within a specific duration,
t = 1920 s.
Figure 4C-d showed variations of
SESR with respect to
Hct. The
SESR tended to decrease substantially with respect to
Hct. The blood sample with
Hct = 30% showed the maximum value of
SESR. This result indicated that
SESR varied significantly depending on the hematocrit.
From the result, one can conclude that the viscoelasticity of the blood sample suggested by the present method can be varied with the hematocrit. In addition, it can be employed to quantify variations of the ESR occurring in the driving syringe by monitoring temporal variations of viscoelasticity.
3.4. Quantification of the Contribution of Hardened RBCs to Blood Viscoelasticity
Finally, the method was employed to quantify the contribution of hardened RBCs to the viscoelasticity of blood samples. According to previous studies [
27,
28], normal RBCs were hardened chemically with GA solution. The degree in rigidity increased gradually by varying concentrations of the GA solution. Normal RBCs were hardened chemically with three different concentrations of GA solution (
CGA) (
CGA = 4, 8, and 12 μL/mL). The hardened blood sample (
Hct = 50%) was then prepared by adding hardened RBCs into plasma.
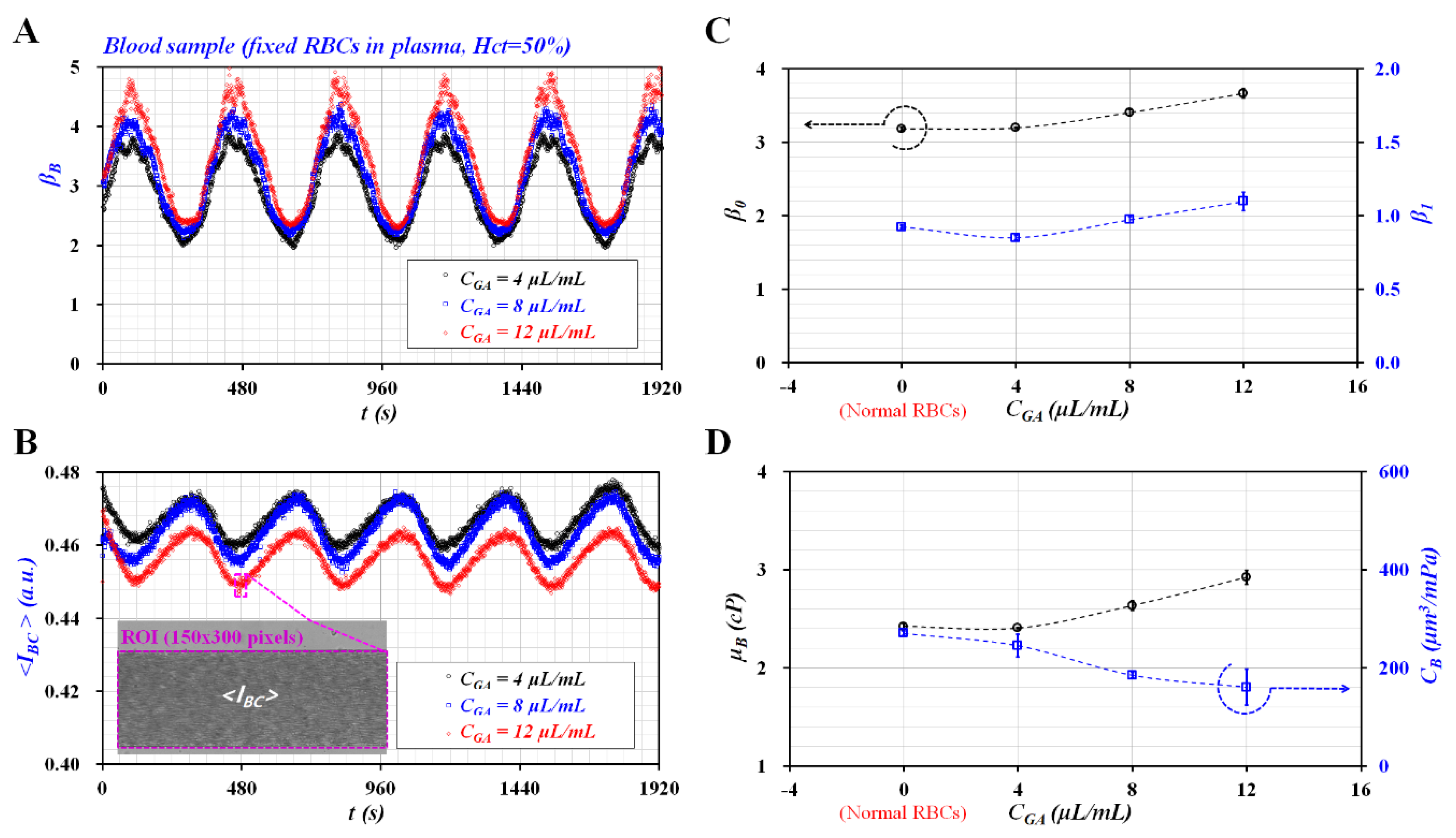
Figure 5A showed temporal variations of
βB with respect to
CGA. As the concentration of GA solution increased,
βB tended to increase gradually. In addition, the
βB exhibited steady and periodic variations over time.
Figure 5B showed temporal variations of <
IBC> with respect to
CGA. The inset showed a microscopic image of the fixed blood sample (i.e., fixed RBCs with
CGA = 12 μL/mL) captured at
t = 480 s. The <
IBC> tended to decrease slightly at a higher concentration of GA solution. However, it exhibited steady and periodic variations over time. The result indicated that the fixed blood sample with
Hct = 50% did not induce the ESR in the driving syringe as shown in
Figure 4.
Figure 5C showed variations of
β0 and
β1 with respect to
CGA. Both parameters (
β0 and
β1) tended to increase substantially at a higher concentration of GA solution. Because the GA solution was employed to increase the rigidity of RBCs, both parameters presented distinctive variations of hardness. Based on Equations (18)–(20), variations of
μB and
CB were obtained at an interval of
T = 360 s. As
βB and <
IBC> showed stable variations over time,
μB and
CB remained constant over the specific duration of the test as shown in
Figure 5A,B. Thus,
μB and
CB were represented as average ± standard deviation (
n = 5).
Figure 5D showed variations of
μB and
CB with respect to
CGA. According to previous studies [
17,
18], blood viscosity and elasticity tended to increase at a higher concentration of GA solution. When compared with the previous results, blood viscosity exhibited consistent variations with respect to the concentration of GA solution. Because compliance was defined as the reciprocal of elasticity, the compliance also showed consistent variations with respect to the concentration of GA solution.
The results lead to the conclusion that the present method could be employed to monitor variations of the viscoelasticity of blood samples while the syringe pump was set to a pulsatile flow-rate pattern.
3.5. Quantificative Comparison of Viscoelasticty Obtained with Preesent Method and Conventional Viscometer
Using a conventional viscometer, viscoelasticity of cells was modeled with the linear Maxwell model. As shown in
Figure 6A-a, the viscoelasticity of each blood sample was modeled as a solid element and a fluid element connected in series. The corresponding constitutive expression of each element was given as
(solid element) and
(fluid element), respectively. Here,
G and
μ represented elasticity and viscosity, respectively.
τ and
γ denoted shear stress and shear strain. External shear strain was excited periodically as
. The governing equation was then derived as
. Here, the time constant of viscometry (
lcv) was expressed as
lcv = μ/G. The viscous effect of the viscometer was considered as negligible since the viscometer did not have an influence on relaxation time of the cells. The viscometer had operated at a wider range of frequency from ω = 0.3 rad/s to ω = 700 rad/s [
29]. The previous study indicated that the time constant of whole blood was obtained as
λcv = 1.5–13.4 ms for shear flow [
29], and
λcv = 114–259 ms for extensional flow [
30].
On the other hand, under periodic blood flow in the microfluidic system,
Figure 6A-b showed the simple fluidic circuit model of the microfluidic system. Based on electric circuit analysis, the governing equation of fluidic system was derived as
. Here,
Q represented the flow rate which passed through resistance element. Time constant (
λB) was derived as
λB =
RWB∙
CB.
RWB and
CB represented fluidic resistance of the coflowing channel filled with only blood sample and compliance, respectively. As shown in
Figure 6A-b, a microfluidic system behaved as an
R-C low pass filer. To effectively infuse alternating components in the periodic flow rate into a microfluidic system, the period of the excitation flow rate should be much longer than the time constant of the microfluidic system (i.e.,
T >
λB). In addition, the syringe pump used in this study did not infuse blood samples during short periods. From the experimental results as shown in
Figure 3B, period (
T) of the sinusoidal flow rate was fixed as
T = 360 s.
The
λB was determined by
RWB and
CB. Flexible tubing and the PDMS channels tended to vary the time constant substantially [
11]. A microfluidic channel with different channel depths (
H) (
H = 4, 10, and 20 μm) was prepared to change
RWB. Here, 1x PBS was infused into a microfluidic channel to reduce or remove the viscoelastic effects. As shown in
Figure 6B-a, the corresponding time constant for each channel depth was obtained as
λB = 5.92 ± 0.81 s (
H = 4 μm),
λB = 6.11 ± 0.20 s (
H = 10 μm), and
lB = 3.64 ± 0.40 s (
H = 20 μm). In addition,
Figure 6B-b showed variations of
RWB and
CB with respect to
H. A lower channel depth contributed to increasing
RWB, and decreasing
CB. The result indicated that fluidic resistance (
RWB) had a strong influence on
CB. To find out the contribution of compliance element (
CB), the compliance of the microfluidic system increased intentionally by securing the air cavity inside the driving syringe. As shown in
Figure 6C, variations of
λB and
CB were obtained with respect to
Vair = 0 and 0.1 mL. When the air cavity of 0.1 mL existed inside the driving syringe,
λB and
CB increased considerably as
λB = 20.84 ± 3.42 s and
CB = 378.59 ± 62.11 s. From the result, the air cavity tended to increase
λB and
CB substantially. When compared with viscometry data, the time constant (
λB) increased about O (10
2) significantly because of the compliance effect of the microfluidic system (i.e., flexible tubing, PDMS channels, and the air cavities existing in the driving syringe). In addition, minimum threshold of
CB (i.e., detection limit) was estimated as 66.05 ± 7.30 μm
3/mPa at a specific condition (i.e.,
Vair = 0,
H = 20 μm). According to a previous study [
17], time constants obtained with two different systems (i.e.,
λPM: microfluidic system,
λCPV: conventional viscometer) were obtained and compared with respect to
Cglycerin = 10%, 20%, 30% and 40%. As glycerin solution did not include viscoelasticity, both time constants remained unchanged with respect to different concentrations of glycerin solution. However, the microfluidic system had a longer time constant with O (10
0). The ratio of time constant between
λCPV and
λPM was obtained as
λCPV/
λPM = O (10
2). To quantitatively determine elasticity obtained with both methods, a scatter plot was employed by plotting
GPM on the vertical axis and
GCPV on the horizontal axis. According to linear regression analysis, regression coefficient (
R2) had a higher value (
R2 = 0.9617). This result indicated that the elasticity obtained with microfluidic system exhibited consistent variations with respect to
Cglycrin when compared with elasticity obtained with conventional viscometer. Thus, the microfluidic system could be employed to measure viscoelasticity effectively. The slope of 0.0022 indicated that elasticity obtained with the microfluidic system was much less than that obtained with the conventional viscometer.
According to order analysis,
CB had an order of O (10
−13) from the analytical expression of time constant. Here, O represented order. According to experimental results as shown in
Figure 5, the blood sample (normal RBCs suspended in plasma,
Hct = 50%) had
λB = 36.084 ± 0.713 s,
μB = 2.422 ± 0.028 cP, and
RWB = 135.148 ± 2.03 TPa∙s/m
3. The compliance (
CB) was then obtained as
CB = 270.598 ± 4.63 μm
3/mPa. The corresponding order of each parameter was calculated as (1) O (10
1) for
λB, (2) O (10
0) for
μB, and O (10
12) for
RWB. As the unit of
CB was expressed as
μm3/mPa, the order of
CB was calculated as O (10
−18)/O (10
−3) = O (10
−15). Thus,
CB obtained for the blood sample had an order of O (10
−13). In order words, both approaches (i.e., analytical expression, and experimental data) exhibited the same order of O (10
−13). Thus, the present method could be used to monitor
CB of blood samples sufficiently.
To compare the relationship between
GB and
CB, it was assumed that
λcv of the conventional viscometer had the same
λB as the microfluidic system (i.e.,
). The time constant obtained by the microfluidic system was used to evaluate
GB and
CB simultaneously. The following relation was given as
. The analytical expression indicated that
GB and
CB had a reciprocal relationship (i.e.,
G ~ 1/
CB). Using experimental results as shown in
Figure 4,
GB and
CB were obtained with respect to
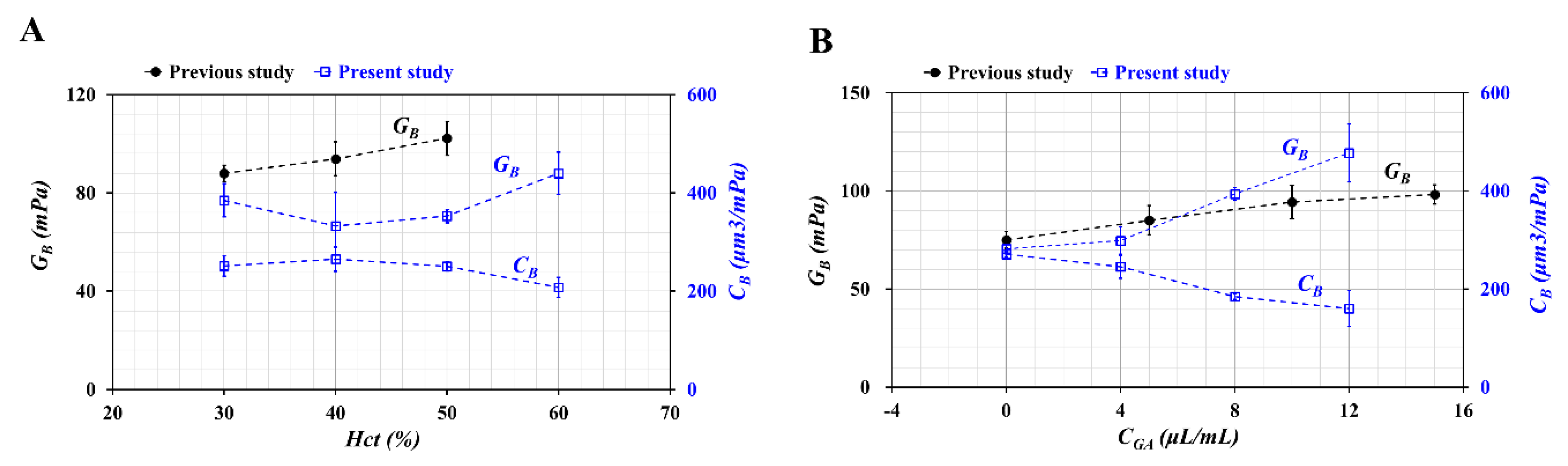
Hct = 30%, 40%, 50%, and 60%. Additionally, by referring to the previous study [
18], variations of
GB were represented with respect to
Hct = 30%, 40%, and 50%. Here, blood samples were prepared by adding normal RBCs into plasma. As shown in
Figure 7A, at
Hct > 40%,
GB tended to increase with respect to
Hct. Inversely,
CB tended to decrease with respect to
Hct. When compared with the previous study, the trend of
GB increased similarly with respect to
Hct. It can be inferred that different microfluidic systems contributed to differences of
GB between both studies. Additionally, variations of
CB and
GB were summarized with respect to
CGA as shown in
Figure 7B. Here, in the previous study [
4], fixed blood samples were prepared by adding fixed RBCs into 1x PBS instead of plasma.
GB of both studies tended to increase gradually with respect to
CGA. From quantitative comparisons between the previous study and the present study, elasticity (
GB) and compliance (
CG) had a reciprocal relationship. Additionally, they varied significantly when the rigidity of RBCs increased substantially.
Viscoelasticity (G) was represented as G = G1+ j G2. Here, G1 (storing modulus) and G2 (loss modulus) were expressed as and . Variations of G1 and G2 were represented with respect to radial frequency (ω). G1 and G2 tended to vary depending on ∙ω. However, as ∙ω showed a significant difference for both systems, it was apparent that both systems exhibited different variations of G1 and G2 with respect to ω. The microfluidic system and conventional viscometer showed different characteristics in terms of angular frequency (or period) and time constants. However, according to experimental results, the microfluidic system could be used effectively to evaluate the viscoelasticity of human blood when compared with conventional viscometers.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}






