

The Behavioral Intention of Hospitals to Promote Sustainable Development of Green Healthcare from the Perspective of Organizational Stakeholders during the COVID-19 Epidemic: A Case Study of Hospitals in Taiwan


Abstract
:1. Introduction
2. Theoretical Background
3. Aim and Scope
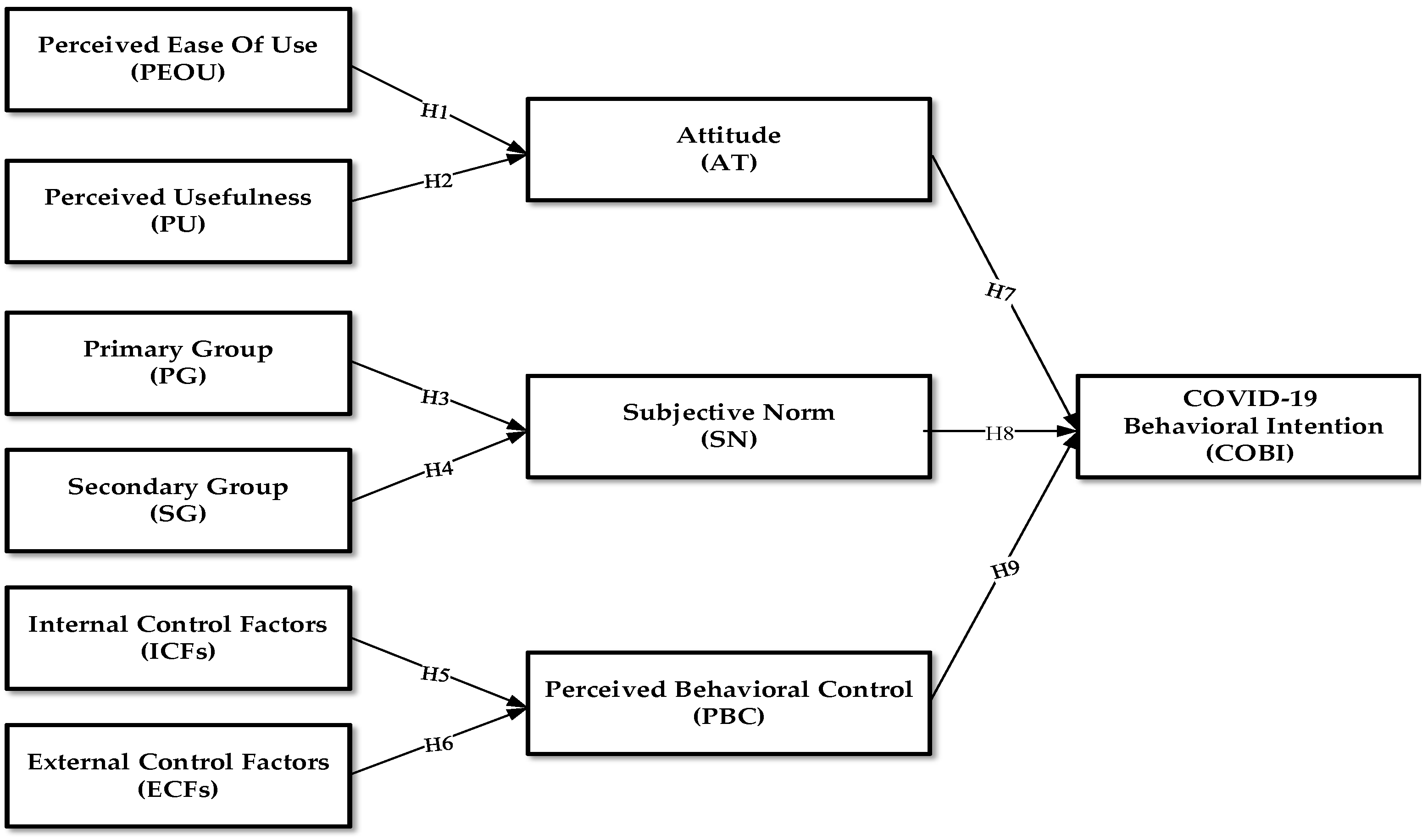
4. Hypotheses Development
5. Materials and Methods
5.1. Variables and Measurements
5.2. Samples and Procedures
5.3. Statistical Analyses
6. Results
6.1. Reliability and Validity of the Research Model
6.2. Structural Model Analysis of Research Framework
6.3. Comparative Analysis of Structural Models of Different Intra-Organizational Stakeholders
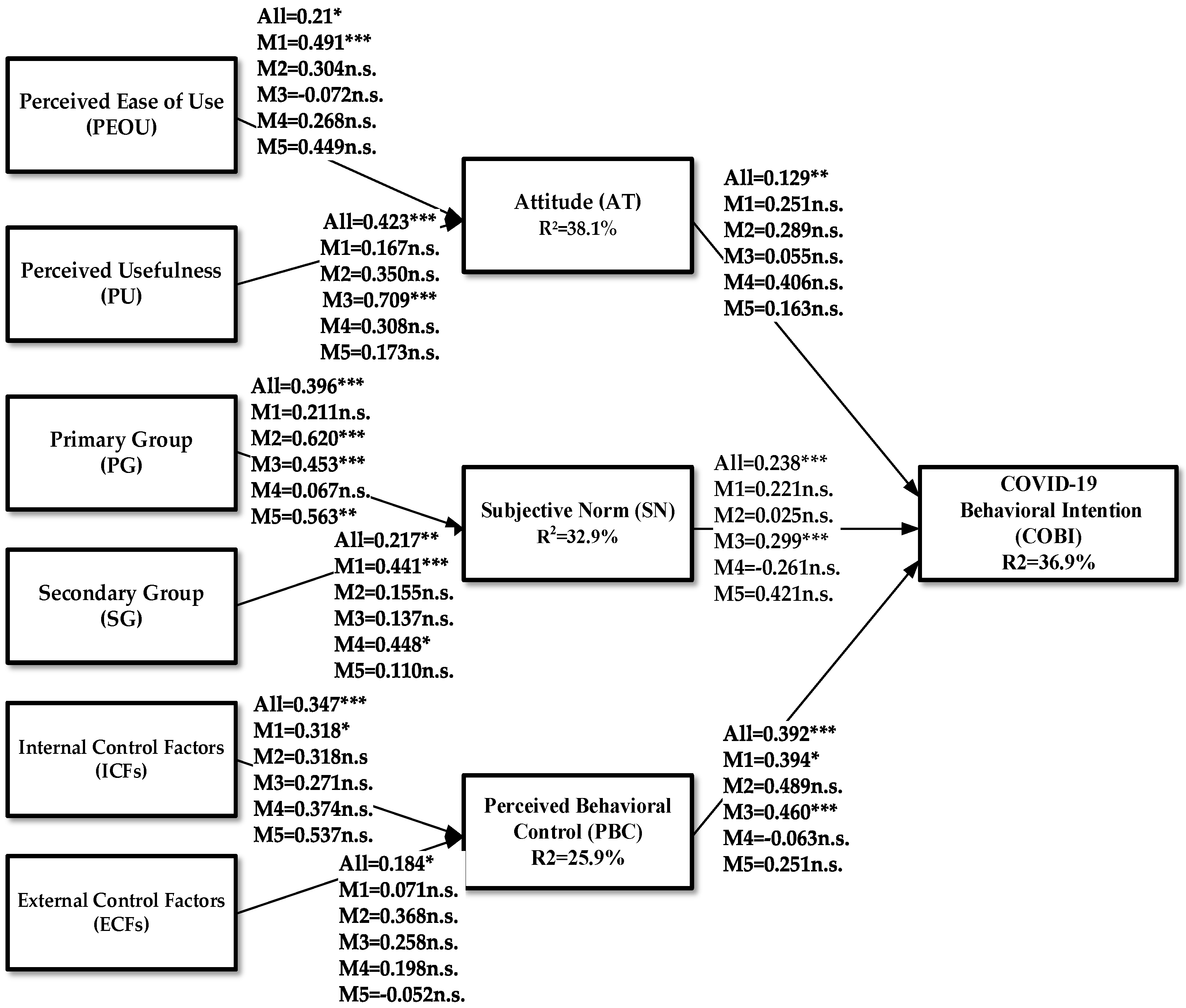
- Pathway H1 (PEOU → AT): Among the different intra-organizational stakeholders, only “medical administrators” (M1 = 0.491 ***) believed in the PEOU for promoting green hospitals; there was a positive and significant correlation with “attitude (AT)” and the rest were not significant.
- Pathway H2 (PU → AT): Among the different intra-organizational stakeholders, only “nursing staff” (M3 = 0.709 ***) believed in PU for promoting green hospitals through AT showed a positive and significant correlation, and the rest were not significant.
- Pathway H3 (PG → SN): Among the different intra-organizational stakeholders, “doctors” (M2 = 0.620 ***), “nursing staff” (M3 = 0.453 ***), and “other outsourced personnel” (M5 = 0.563 **) showed a positive and significant correlation with the “subjective norm (SN)” for the PG belief in promoting green hospitals, among which “physician” (M2 = 0.620 ***) had the most significant effect.
- Pathway H4 (SG → SN): Among the different intra-organizational stakeholders, “medical administrators” (M1 = 0.441 ***) and “medical examinations and medical personnel” (M4 = 0.448 *) were the most important in promoting green hospitals’ SG beliefs and showed a positive and significant correlation with the SN among which “medical administrators” (M1 = 0.441 ***) had the most significant effect.
- Pathway H5 (ICFs → PBC): Among the different intra-organizational stakeholders, only “medical administrators” (M1 = 0.318 *) believe in ICFs promoting green hospitals through “perception behavioral control (PBC)” showed a positive and significant correlation, while the rest had no significant correlation.
- Pathway H6 (ECFs → PBC): Any group of employees among the different intra-organizational stakeholders has a strong impact on the beliefs of ECFs that promote green hospitals, and PBC showed a positive correlation; however, the correlation was not significant.
- Pathway H7 (AT → COBI): The “COVID-19 behavioral intention (COBI)” of any group of employees in promoting green hospitals is positively affected by AT, but the effect was not significant for any group.
- Pathway H8 (SN → COBI): Among the different intra-organizational stakeholders, only “nursing staff” (M3 = 0.299 ***) had the COBI for promoting green hospitals, which was positively and significantly affected by the SN and the rest were not significant.
- Pathway H9 (PBC → COBI): Among the different intra-organizational stakeholders, “medical administrators” (M1 = 0.394 *) and “nursing staff” (M3 = 0.460 ***) were the most important in promoting green hospitals. Their COBI was positively and significantly affected by PBC among which “nursing staff” (M3 = 0.460 ***) was more significant.
7. Discussion
8. Conclusions and Policy
9. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Cities and Local Governments. Millennium Development Goals; United Cities and Local Governments; United Cities and Local Governments: Barcelona, Spain, 2010. [Google Scholar]
- World Health Organization. Monitoring Health for the SDGs; World Health Organization: Geneva, Switzerland, 2022.
- Internal Finance Corporation. Who Cares Wins 2005 Conference Report: Sustainability Investing for Long-Term Value; Internal Finance Corporation: Washington, DC, USA, 2005. [Google Scholar]
- Eckelman, M.J.; Sherman, J. Environmental Impacts of the U.S. Health Care System and Effects on Public Health. PLoS ONE 2016, 11, e0157014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Health Care Without Harm. Leading the Global Movement for Environmentally Responsible Health Care; Health Care Without Harm: Brussels, Belgium, 2008. [Google Scholar]
- Health Care without Harm (HCWH). Health Care’s Climate Footprint: How the Health Sector Contributes to the Global Climate Crisis and Opportunities for Action. 2019. Available online: https://noharm-global.org/sites/default/files/documents-files/5961/HealthCaresClimateFootprint_092319.pdf (accessed on 4 August 2022).
- IEA. Global Energy Review. Assessing the Effects of Economic Recoveries on Global Energy Demand and CO2 Emissions; International Energy Agency Publications: Paris, France, 2021. [Google Scholar]
- World Health Organization (WHO). Global Analysis of Health Care Waste in the Context of COVID-19; World Health Organization: Geneva, Switzerland, 2022.
- Khahro, S.H.; Kumar, D.; Siddiqui, F.H.; Ali, T.H.; Raza, M.S.; Khoso, A.R. Optimizing Energy Use, Cost and Carbon Emission through Building Information Modelling and a Sustainability Approach: A Case-Study of a Hospital Building. Sustainability 2021, 13, 3675. [Google Scholar] [CrossRef]
- Yang, Y.; Zeng, N.; Shen, M.; Sun, Z. Development of green hospitals home and abroad. J. Cent. South Univ. 2013, 38, 949–953. [Google Scholar] [CrossRef]
- Health Care Without Harm (HCWH). Green Guide for Health Care. 2022. Available online: https://noharm-global.org/issues/global/green-guide-health-care (accessed on 4 February 2022).
- Health Care without Harm (HCWH). Global Green and Healthy Hospitals: A Comprehensive Environmental Health Agenda for Hospitals and Health Systems around the World. 2011. Available online: http://noharm.org/lib/downloads/building/GGHHA.pdf (accessed on 4 February 2022).
- Chang, C.H. Taiwanese People’s Research on the Construction and Investigation of Green Hospital Indicators; National Kaohsiung Normal University Press: Kaohsiung, Taiwan, 2011. [Google Scholar]
- Shen, S.T. The Factors to Influence Patients’ Intention to Adopt Medical Service in Green Hospitals: An Example of Green Hospitals in North Taiwan. J. Des. Sci. 2015, 18, 73–97. [Google Scholar] [CrossRef]
- Shen, S.T. The Factors to Influence Staffs’ Intention to Adopt Environmental Behavior in Green Hospitals. Ph.D. Thesis, Chung Yuan Christian University, Taoyuan City, Taiwan, 2019. [Google Scholar] [CrossRef]
- Ajzen, I. From Intentions to Action: A Theory of Planned Behavior. In Action-Control: From Cognition to Behavior; Kuhl, J., Beckmann, J., Eds.; Springer: Berlin/Heidelberg, Germany, 1985; pp. 11–39. [Google Scholar]
- Fishbein, M. An Investigation of the Relationships Between Beliefs About an Object and the Attitude Toward the Object. Hum. Relat. 1963, 16, 233–240. [Google Scholar] [CrossRef]
- Ajzen, I.; Fishbein, M. Belief, Attitude, Intention, and Behavior: An Introduction to Theory and Research; Addison-Wesley: Reading, MA, USA, 1975; pp. 53–89. [Google Scholar]
- Ajzen, I.; Fishbein, M. Understanding Attitudes and Predicting Social Behavior; Prentice-Hall: Englewood Cliffs, NJ, USA, 1980. [Google Scholar]
- Yuriev, A.; Dahmen, M.; Paillé, P.; Boiral, O.; Guillaumie, L. Pro-environmental behaviors through the lens of the theory of planned behavior: A scoping review. Resour. Conserv. Recycl. 2020, 155, 104660. [Google Scholar] [CrossRef]
- Ajzen, I.; Madden, T.J. Prediction of goal-directed behavior: Attitudes, intentions and perceived behavioral control. J. Exp. Soc. Psychol. 1986, 22, 453–474. [Google Scholar] [CrossRef]
- Ajzen, I. Attitudes, Personality, and Behavior; The Dorsey Press: Chicago, IL, USA, 1988. [Google Scholar]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Lin, W.C.; Tung, S.C.; Chiu, P.H. Employeess’ Cognition of Green Hospitals and Health Promoting Hospitals. J. Environ. Educ. 2013, 10, 99–128. [Google Scholar] [CrossRef]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1898, 13, 319–340. [Google Scholar] [CrossRef] [Green Version]
- Davis, F.D.; Bagozzi, R.P.; Warshaw, P.R. User acceptance of computer technology: A comparison of two theoretical models. Manag. Sci. 1989, 35, 982–1003. [Google Scholar] [CrossRef] [Green Version]
- Taylor, S.; Todd, P.A. Understanding information technology usage: A test of competing models. Inf. Syst. Res. 1995, 6, 144–176. [Google Scholar] [CrossRef]
- National Health Bureau of the Ministry of Health and Welfare. Green Hospitals, Green Living, Green Earth: A Handbook for Sharing Experiences in Green Hospital Promotion; Bureau of Health Promotion, Department of Health: Taipei, Taiwan, 2010.
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef] [PubMed]
- Triandis, H.C. International Behavior; Brooks/Cole: Monterey, CA, USA, 1977. [Google Scholar]
- Triandis, H.C. Values, Attitudes, and Interpersonal Behavior. In Nebraska Symposium on Motivation; University of Nebraska Press: Lincoln, NE, USA, 1979. [Google Scholar]
- Fu, Q.; Ghardallou, W.; Comite, U.; Siddique, I.; Han, H.; Arjona-Fuentes, J.M.; Ariza-Montes, A. The Role of CSR in Promoting Energy-Specific Pro-Environmental Behavior among Hotel Employees. Sustainability 2022, 14, 6574. [Google Scholar] [CrossRef]
- Notani, A.S. Moderators of Perceived Behavioral Controls’s Predictiveness in the Theory of Planned Behavior: A Meta-Analysis. J. Consum. Psychol. 1998, 7, 247–271. [Google Scholar] [CrossRef]
- Li, D.; Zhao, L.; Ma, S.; Shao, S.; Zhang, L. What influences an individual’s pro-environmental behavior? A literature review. Resour. Conserv. Recycl. 2019, 146, 28–34. [Google Scholar] [CrossRef]
- Banjarnahor, A.R. Technology Acceptance Model and Theory of Planed Behavior: Mapping Literature Review. Gold. Ratio Mapp. Idea Lit. Format 2021, 1, 134–168. [Google Scholar] [CrossRef]
- AlQudah, A.A.; Al-Emran, M.; Shaalan, K. Technology Acceptance in Healthcare: A Systematic Review. Appl. Sci. 2021, 11, 10537. [Google Scholar] [CrossRef]
- Adebayo, T.S.; Ullah, S.; Kartal, M.T.; Ali, K.; Pata, U.K.; Ağa, M. Endorsing sustainable development in BRICS: The role of technological innovation, renewable energy consumption, and natural resources in limiting carbon emission. Sci. Total Environ. 2023, 859, 160181. [Google Scholar] [CrossRef]
- Zhen, Z.; Ullah, S.; Shaowen, Z.; Irfan, M. How do renewable energy consumption, financial development, and technical efficiency change cause ecological sustainability in European Union countries. Energy Environ. Spec. Issue Adv. Methods 2022, 1–19. [Google Scholar] [CrossRef]
- Ullah, S.; Luo, R.; Adebayo, T.S.; Kartal, M.T. Dynamics between environmental taxes and ecological sustainability: Evidence from top-seven green economies by novel quantile approaches. Sustain. Dev. 2022, 1–15. [Google Scholar] [CrossRef]
- Akman, I.; Mishra, A. Sector diversity in Green Information Technology practices: Technology Acceptance Model perspective. Comput. Hum. Behav. 2015, 49, 477–486. [Google Scholar] [CrossRef]
- Anser, M.K.; Yousaf, Z.; Zaman, K. Green technology acceptance model and green logistics operations: “to see which way the wind is blowing”. Front. Sustain. 2020, 1, 3. [Google Scholar] [CrossRef]
- Chen, C.; Xu, X.; Arpan, L. Between the technology acceptance model and sustainable energy technology acceptance model: Investigating smart meter acceptance in the United States. Energy Res. Soc. Sci. 2017, 25, 93–104. [Google Scholar] [CrossRef]
- Tsaur, R.C.; Lin, Y.-H. Exploring the Consumer Attitude of Building-Attached Photovoltaic Equipment Using Revised Technology Acceptance Model. Sustainability 2018, 10, 4177. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.F.; Anderson, R.E.; Tatham, R.L.; Black, W.C. Multivariate Data Analysis, 5th ed.; Macmillan: New York, NY, USA, 1998. [Google Scholar]
- Jöreskog, K.G. Simultaneous factor analysis in several populations. Psychometrika 1971, 36, 409–426. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Evaluating structural equation models with unobservable variables and measurement error. J. Mark. Res. 1981, 18, 39–50. [Google Scholar] [CrossRef]
- Hair, J.F.; Ringle, C.M.; Sarstedt, M. PLS-SEM: Indeed a silver bullet. J. Mark. Theory Pract. 2011, 19, 139–152. [Google Scholar] [CrossRef]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M.A. Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM); Sage: Thousand Oaks, CA, USA, 2016. [Google Scholar]
- Widianto, S.; Kautsar, A.P.; Sriwidodo; Abdulah, R.; Ramadhina, R. Pro-environmental behaviour of healthcare professionals: A study applying theory of planned behaviour. Int. J. Bus. Glob. 2021, 28, 219–232. [Google Scholar] [CrossRef]
- Yoon, C. Extending the TAM for Green IT: A normative perspective. Comput. Hum. Behav. 2018, 83, 129–139. [Google Scholar] [CrossRef]
- Boiral, O.; Paillé, P.; Raineri, N. The Nature of Employees’ Pro-Environmental Behaviors. The Psychology of Green Organizations; Oxford Scholarship Online: Oxford, UK, 2015; pp. 12–32. [Google Scholar] [CrossRef]
- Jamil, M.N.; Rasheed, A.; Mukhtar, Z. Corporate Social Responsibility impacts sustainable organizational growth (firm performance): An empirical analysis of Pakistan stock exchange-listed firms. J. Environ. Sci. Econ. 2022, 1, 25–29. [Google Scholar] [CrossRef]
- Rocha, C.M.M.; Santamaria jotty, L.S. Statistical analysis of research in the study of the implementation of the circular economy in the preservation of water resources. Glob. Sustain. Res. 2022, 1, 32–40. [Google Scholar] [CrossRef]
- Maiwada, U.D.; Jamoh, A.A. Using Science, Technology, and Innovation (Sti); in Achieving Sustainable Development in Developing Countries (Dcs). J. Technol. Innov. Energy 2022, 1, 23–27. [Google Scholar] [CrossRef]
- Xu, B.; Gao, X.; Cai, W.; Jiang, L. How Environmental Leadership Boosts Employees’ Green Innovation Behavior? A Moderated Mediation Model. Front. Psychol. 2022, 12, 689671. [Google Scholar] [CrossRef] [PubMed]
- Dreyer, B.C.; Riemer, M.; Spadafore, B.; Marcus, J.; Fernandes, D.; Taylor, A.; Whitney, S.; Geobey, S.; Dennett, A. Fostering Cultures of Sustainability in a Multi-Unit Office Building: A Theory of Change. Front. Psychol. 2021, 12, 624311. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Construct | Item | Loading | Mean | STDEV | T Statistics |
|---|---|---|---|---|---|
| PEOU 1 | 0.889 | 0.889 | 0.017 | 51.301 | |
| Perceived Ease of Use (PEOU) | PEOU 2 | 0.92 | 0.919 | 0.01 | 88.538 |
| VIF = 4.736 | PEOU 3 | 0.908 | 0.908 | 0.013 | 67.641 |
| rho A = 0.963 | PEOU 4 | 0.786 | 0.786 | 0.03 | 26.492 |
| Cronbach’s α = 0.960 | PEOU 5 | 0.83 | 0.83 | 0.024 | 34.125 |
| Composite Reliability = 0.967 | PEOU 6 | 0.902 | 0.902 | 0.015 | 59.272 |
| AVE = 0.784 | PEOU 7 | 0.915 | 0.915 | 0.013 | 69.804 |
| PEOU 8 | 0.924 | 0.924 | 0.01 | 89.806 | |
| Perceived Usefulness (PU) | PU 1 | 0.922 | 0.921 | 0.015 | 61.628 |
| VIF = 4.736 | PU 2 | 0.953 | 0.953 | 0.007 | 131.382 |
| rho A = 0.978 | PU 3 | 0.964 | 0.963 | 0.006 | 166.442 |
| Cronbach’s α = 0.978 | PU 4 | 0.962 | 0.961 | 0.007 | 135.293 |
| Composite Reliability = 0.982 | PU 5 | 0.958 | 0.957 | 0.009 | 109.21 |
| AVE = 0.902 | PU 6 | 0.94 | 0.94 | 0.012 | 76.011 |
| Primary Group (PG) | PG 1 | 0.938 | 0.939 | 0.009 | 103.016 |
| VIF = 2.185 | |||||
| rho A = 0.953 | |||||
| Cronbach’s α = 0.952 | PG 2 | 0.94 | 0.94 | 0.011 | 87.472 |
| Composite Reliability = 0.968 | PG 3 | 0.96 | 0.96 | 0.007 | 140.256 |
| AVE = 0.875 | PG 4 | 0.902 | 0.902 | 0.029 | 31.054 |
| Secondary Group (SG) | SG 1 | 0.925 | 0.926 | 0.022 | 41.969 |
| VIF = 2.185 | |||||
| rho A = 0.962 | |||||
| Cronbach’s α = 0.956 | SG 2 | 0.947 | 0.947 | 0.009 | 107.966 |
| Composite Reliability = 0.968 | SG 3 | 0.94 | 0.939 | 0.013 | 70.381 |
| AVE = 0.882 | SG 4 | 0.946 | 0.946 | 0.01 | 91.023 |
| Internal Control Factors (ICFs) | ICFs 1 | 0.913 | 0.912 | 0.037 | 24.709 |
| VIF = 3.012 | |||||
| rho A = 0.950 | |||||
| Cronbach’s α = 0.948 | ICFs 2 | 0.948 | 0.949 | 0.009 | 105.111 |
| Composite Reliability = 0.963 | ICFs 3 | 0.941 | 0.941 | 0.012 | 81.116 |
| AVE = 0.866 | ICFs 4 | 0.919 | 0.919 | 0.014 | 63.682 |
| External Control Factors (ECFs) | ECFs 1 | 0.945 | 0.945 | 0.013 | 72.53 |
| VIF = 3.012 | |||||
| rho A = 0.968 | |||||
| Cronbach’s α = 0.967 | ECFs 2 | 0.956 | 0.955 | 0.014 | 66.937 |
| Composite Reliability = 0.976 | ECFs 3 | 0.969 | 0.969 | 0.007 | 138.246 |
| AVE = 0.911 | ECFs 4 | 0.948 | 0.948 | 0.011 | 86.715 |
| Attitude (AT) | AT1 | 0.973 | 0.972 | 0.007 | 148.466 |
| VIF = 1.436 | |||||
| rho A = 0.985 | AT2 | 0.967 | 0.967 | 0.007 | 141.058 |
| Cronbach’s α = 0.985 | AT3 | 0.968 | 0.968 | 0.008 | 114.208 |
| Composite Reliability = 0.988 | AT4 | 0.974 | 0.974 | 0.006 | 149.867 |
| AVE = 0.942 | AT5 | 0.97 | 0.969 | 0.007 | 129.35 |
| Subjective Norm (SN) | SN1 | 0.945 | 0.945 | 0.009 | 106.95 |
| VIF = 1.436 | |||||
| rho A = 0.965 | |||||
| Cronbach’s α = 0.965 | SN2 | 0.949 | 0.949 | 0.009 | 108.48 |
| Composite Reliability = 0.974 | SN3 | 0.954 | 0.954 | 0.008 | 117.896 |
| AVE = 0.904 | SN4 | 0.955 | 0.955 | 0.009 | 106.552 |
| Perceived Behavioral Control (PBC) | PBC1 | 0.858 | 0.858 | 0.021 | 41.55 |
| VIF = 1.257 | |||||
| rho A = 0.908 | |||||
| Cronbach’s α = 0.903 | PBC2 | 0.92 | 0.92 | 0.011 | 82.342 |
| Composite Reliability = 0.932 | PBC3 | 0.884 | 0.884 | 0.022 | 40.776 |
| AVE = 0.775 | PBC4 | 0.858 | 0.856 | 0.029 | 30.055 |
| COVID-19 Behavioral Intention (COBI) | COBI 1 | 0.96 | 0.96 | 0.011 | 85.304 |
| Cronbach’s α = 0.976 | |||||
| rho A = 0.976 | COBI 2 | 0.95 | 0.95 | 0.018 | 52.486 |
| Composite Reliability = 0.982 | COBI 3 | 0.978 | 0.978 | 0.006 | 171.683 |
| AVE = 0.932 | COBI 4 | 0.974 | 0.974 | 0.006 | 165.842 |
| PEOU | PU | PG | SG | ICFs | ECFs | AT | SN | PBC | COBI | |
|---|---|---|---|---|---|---|---|---|---|---|
| Perceived Ease of Use (PEOU) | 0.888 | |||||||||
| Perceived Usefulness (PU) | 0.888 | 0.95 | ||||||||
| Primary Group (PG) | 0.581 | 0.613 | 0.935 | |||||||
| Secondary Group (SG) | 0.486 | 0.571 | 0.736 | 0.939 | ||||||
| Internal Control Factors (ICFs) | 0.562 | 0.535 | 0.506 | 0.452 | 0.93 | |||||
| External Control Factors (ECFs) | 0.496 | 0.464 | 0.423 | 0.401 | 0.817 | 0.954 | ||||
| Attitude (AT) | 0.586 | 0.61 | 0.515 | 0.46 | 0.361 | 0.296 | 0.97 | |||
| Subjective Norm (SN) | 0.55 | 0.513 | 0.555 | 0.508 | 0.495 | 0.449 | 0.472 | 0.951 | ||
| Perceived Behavioral Control (PBC) | 0.382 | 0.378 | 0.395 | 0.4 | 0.498 | 0.468 | 0.335 | 0.426 | 0.88 | |
| COVID-19 Behavioral Intention (COBI) | 0.445 | 0.498 | 0.404 | 0.452 | 0.473 | 0.45 | 0.372 | 0.465 | 0.536 | 0.966 |
| Hypotheses | All | Result | M1_ADM | M2_DOC | M3_NUR | M4_MED | M5_OTH | |
|---|---|---|---|---|---|---|---|---|
| H1 | PEOU → AT | 0.210 (2.095) * | Support | 0.491 *** | 0.304 n.s. | −0.072 n.s. | 0.268 n.s. | 0.449 n.s. |
| H2 | PU → AT | 0.423 (4.309) *** | Support | 0.167 n.s. | 0.350 n.s. | 0.709 *** | 0.308 n.s. | 0.173 n.s. |
| H3 | PG → SN | 0.396 (5.936) *** | Support | 0.211 n.s. | 0.620 *** | 0.453 *** | 0.067 n.s. | 0.563 ** |
| H4 | SG → SN | 0.217 (3.401) ** | Support | 0.441 *** | 0.155 n.s. | 0.137 n.s. | 0.448 * | 0.110 n.s. |
| H5 | ICF → PBC | 0.347 (4.269) *** | Support | 0.318 * | 0.318 n.s. | 0.271 n.s. | 0.374 n.s. | 0.537 n.s. |
| H6 | ECF → PBC | 0.184 (2.339) * | Support | 0.071 n.s. | 0.368 n.s. | 0.258 n.s. | 0.198 n.s. | −0.052 n.s. |
| H7 | AT → COBI | 0.129 (2.638) ** | Support | 0.251 n.s. | 0.289 n.s. | 0.055 n.s. | 0.406 n.s. | 0.163 n.s. |
| H8 | SN → COBI | 0.238 (3.680) *** | Support | 0.221 n.s. | 0.025 n.s. | 0.299 *** | −0.261 n.s. | 0.421 n.s. |
| H9 | PBC → COBI | 0.392 (6.518) *** | Support | 0.394 * | 0.489 n.s. | 0.460 *** | −0.063 n.s. | 0.251 n.s. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, P.-C.; Huang, C.-Y.; Huang, M.-H.; Hsu, M.-J. The Behavioral Intention of Hospitals to Promote Sustainable Development of Green Healthcare from the Perspective of Organizational Stakeholders during the COVID-19 Epidemic: A Case Study of Hospitals in Taiwan. Sustainability 2023, 15, 4521. https://doi.org/10.3390/su15054521
Lee P-C, Huang C-Y, Huang M-H, Hsu M-J. The Behavioral Intention of Hospitals to Promote Sustainable Development of Green Healthcare from the Perspective of Organizational Stakeholders during the COVID-19 Epidemic: A Case Study of Hospitals in Taiwan. Sustainability. 2023; 15(5):4521. https://doi.org/10.3390/su15054521
Chicago/Turabian StyleLee, Po-Chun, Ching-Yuan Huang, Min-Hsin Huang, and Meng-Jun Hsu. 2023. "The Behavioral Intention of Hospitals to Promote Sustainable Development of Green Healthcare from the Perspective of Organizational Stakeholders during the COVID-19 Epidemic: A Case Study of Hospitals in Taiwan" Sustainability 15, no. 5: 4521. https://doi.org/10.3390/su15054521