
An Intelligent Health Care System in Fog Platform with Optimized Performance
 ,
, 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- It has been suggested that fog computing could be used as an example of a generalized system design for the advancement of collaborative deep learning.
- HealthFog uses deep learning to automatically analyze cardiac patient data.
- HealthFog was deployed with the FogBus framework so that it could integrate with IoT-edge-cloud to perform real-time data processing.
- Performance characteristics, such as accuracy, reaction time, and network capacity, are demonstrated and studied for the HealthFog deployment.
2. Literature Review
- A real time application based on the concept of IoT in healthcare that can manage a huge amount of data collected from patients, with reduced latency and minimized power consumption.
- Fog computing scenarios need a well-organized resource scheduling mechanism to accomplish user workloads and meet deadlines.
- A deep learning-based fog computing algorithm can accurately assess heart disease severity.
3. Proposed Model
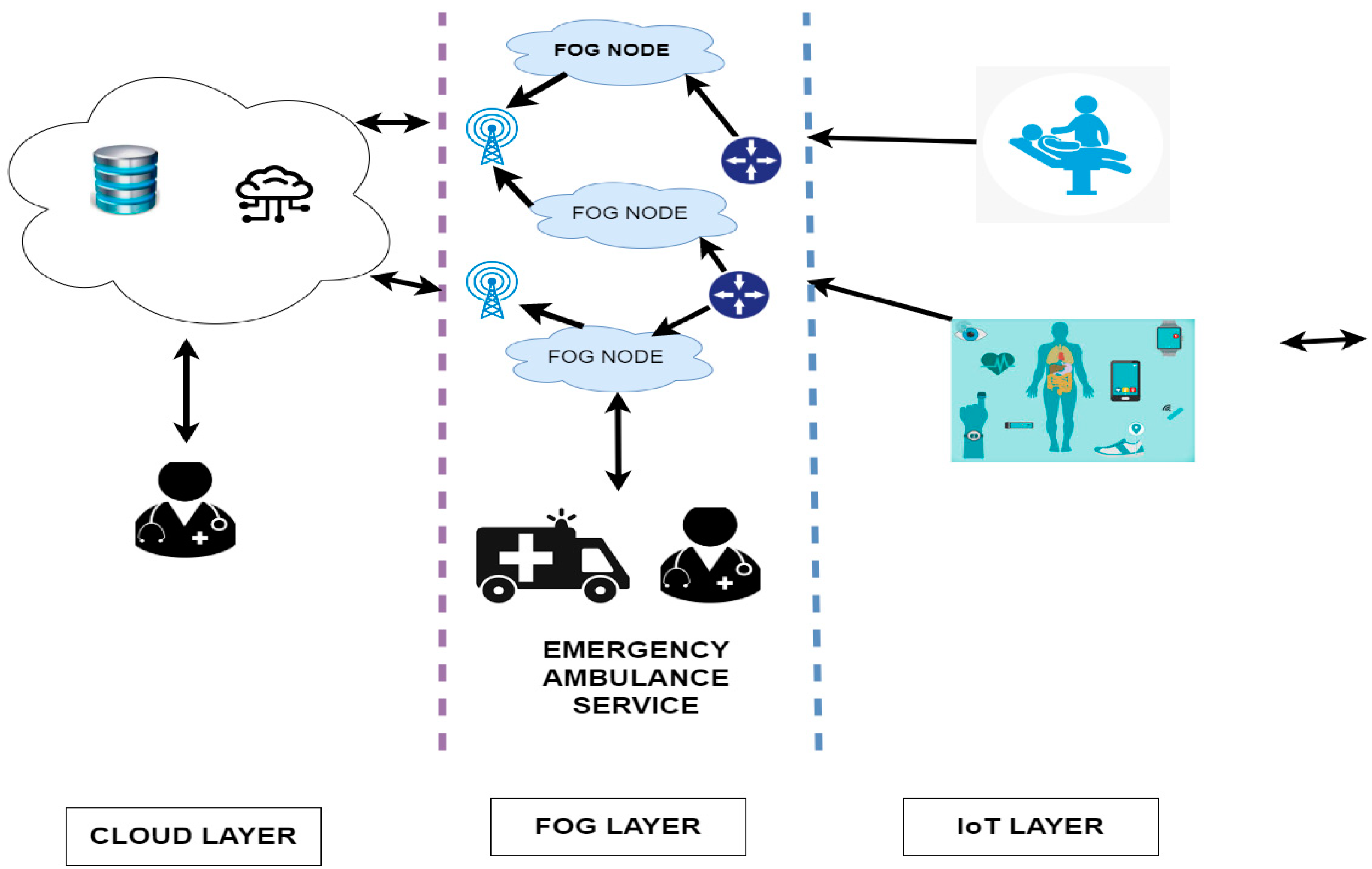
3.1. System Architecture
- Sensors and Actuators: Signals from this body and environment can be collected using the continuous identification, sensing, and transmission capabilities, as well as biomedical and perspective signals. Networks of intelligent e-Health, which use wireless or wired communication protocols, such as Bluetooth and Wi-Fi, to help transmit the data to the access.
- Gateways: This layer is formed after a number of intelligent e-Health gateways that are geographically distributed, similar to creating a simulated fog. Each gateway facilitates different transmission protocols by acting as a source of communication between the sensor nodes and the regional router or Web. The data from various sub-networks and the bearings’ protocol conversion must be provided in order for the higher-level features, such as data aggregation, filtering, and dimensionality depletion, to be received [27,28,29,30].
- Back-End System: This back-end strategy results in a cloud computing program that runs streaming, data warehouse, and data analytics. Lastly, it can be used as an addition to the web client’s GUI for the output and feedback. This available health, as well as environmental, data can be used as a source of huge data [31,32,33,34,35,36] for the statistical and epidemiological forecasting of upcoming epidemic diseases.
3.2. Fog-Based Data Management and Analytics
4. Fog Based Smart Healthcare Components
4.1. Hardware Component
- Network of Body Area Sensor devices: This element consists of three main sensing components: environmental sensors, activity sensors, and health sensors. Medical sensors include electrocardiogram (ECG) sensors, electroencephalogram (EEG) sensors, electromyogram (EMG) sensors, respiration sensors, thermocouple sensors, and differential pressure sensors with potentiometric sensors. Through related gateway devices, these components are in charge of the transmission of data from the patient’s body.
- Gateway: Fog nodes, which include cell phones, laptops, and tablets, collect the data from the sensors throughout the environment and relay that information to the Broker/Worker units for in-depth analysis.
- Cloud Data Center: If the fog framework becomes saturated, services are latency-sensitive, or, if the length of the incoming data is significantly longer than usual, this fog-enabled innovative health makes use of the fog infrastructure or cloud data center resources.
4.2. Software Components
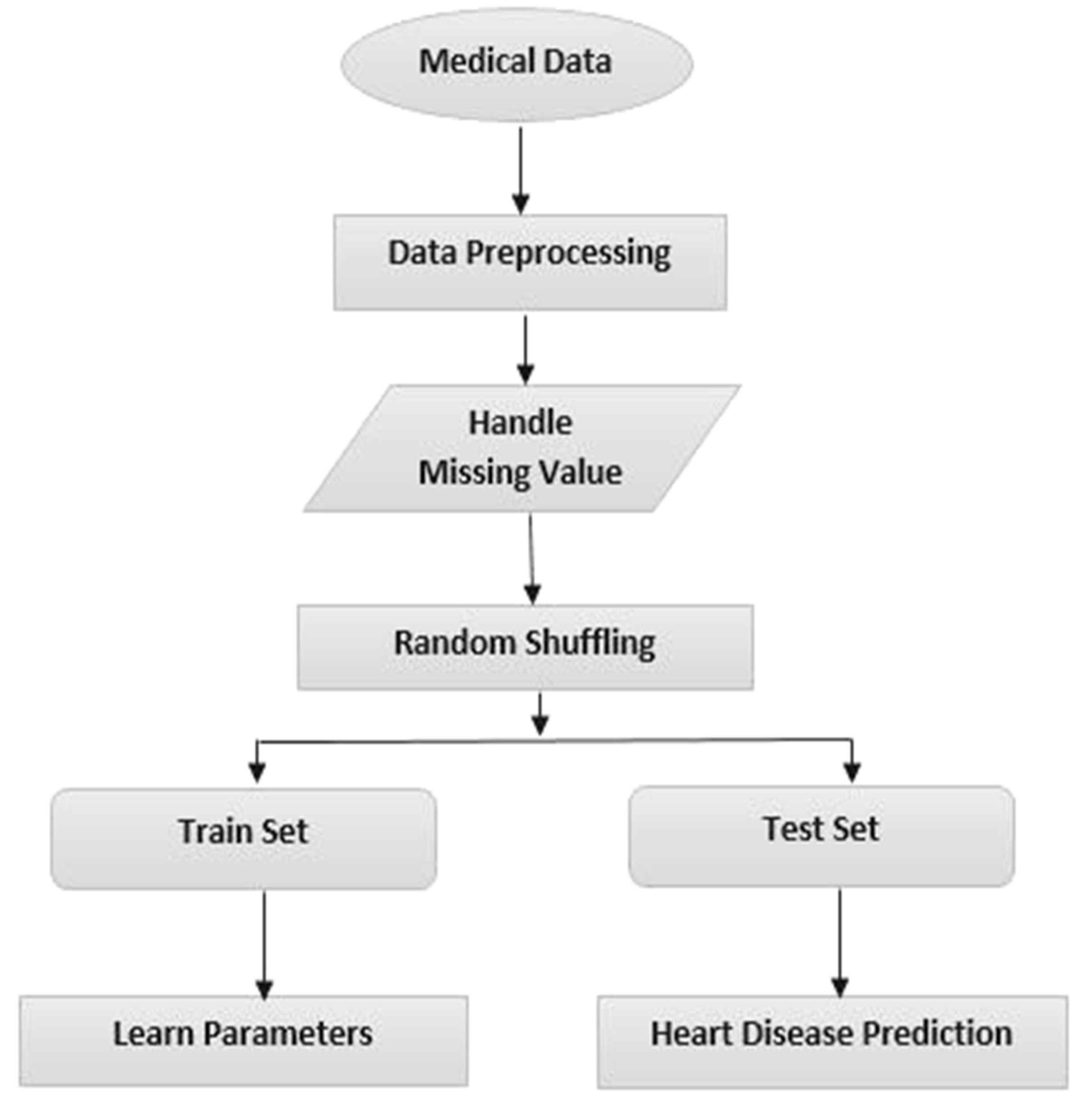
- Data cleaning and pre-processing: preprocessing begins as soon as the data are submitted in order to filter the information, which also includes the use of data analytics technologies. In order to obtain the essential components of the data feature vectors that influence patient health conditions, the filtered data are condensed to a lower size, adopting Principal Component Analysis (PCA) and utilizing Set Partition [28,29] and are protected using the Singular Value Decomposition (SVD) method [30]. It immediately draws a conclusion from the input data, recommends medication and the relevant checkups based on the continuously trained healthcare experts who deal with the data, and then saves it in a database for future training, as needed.
- Resource supervisor: the two elements that constitute this framework are the workload management and arbitration modules [27]. The task queues and job requests for data processing are monitored by this workload manager. The fog or cloud resources that have been supplied for the processing tasks that have been planned and handled by this workload supervisor are assigned by the arbitration component. The Arbitration element, which is connected with this Broker end node, decides whether the cloud data center, the fog worker end node, or the fog computing node must provide this information in order to determine the results [27]. The main goal is to distribute the duties among several devices in order to balance the load and guarantee optimal performance. Fog-enabled innovative health permits users to tailor their load balancing and arbitration methods depending on the necessities of their applications.
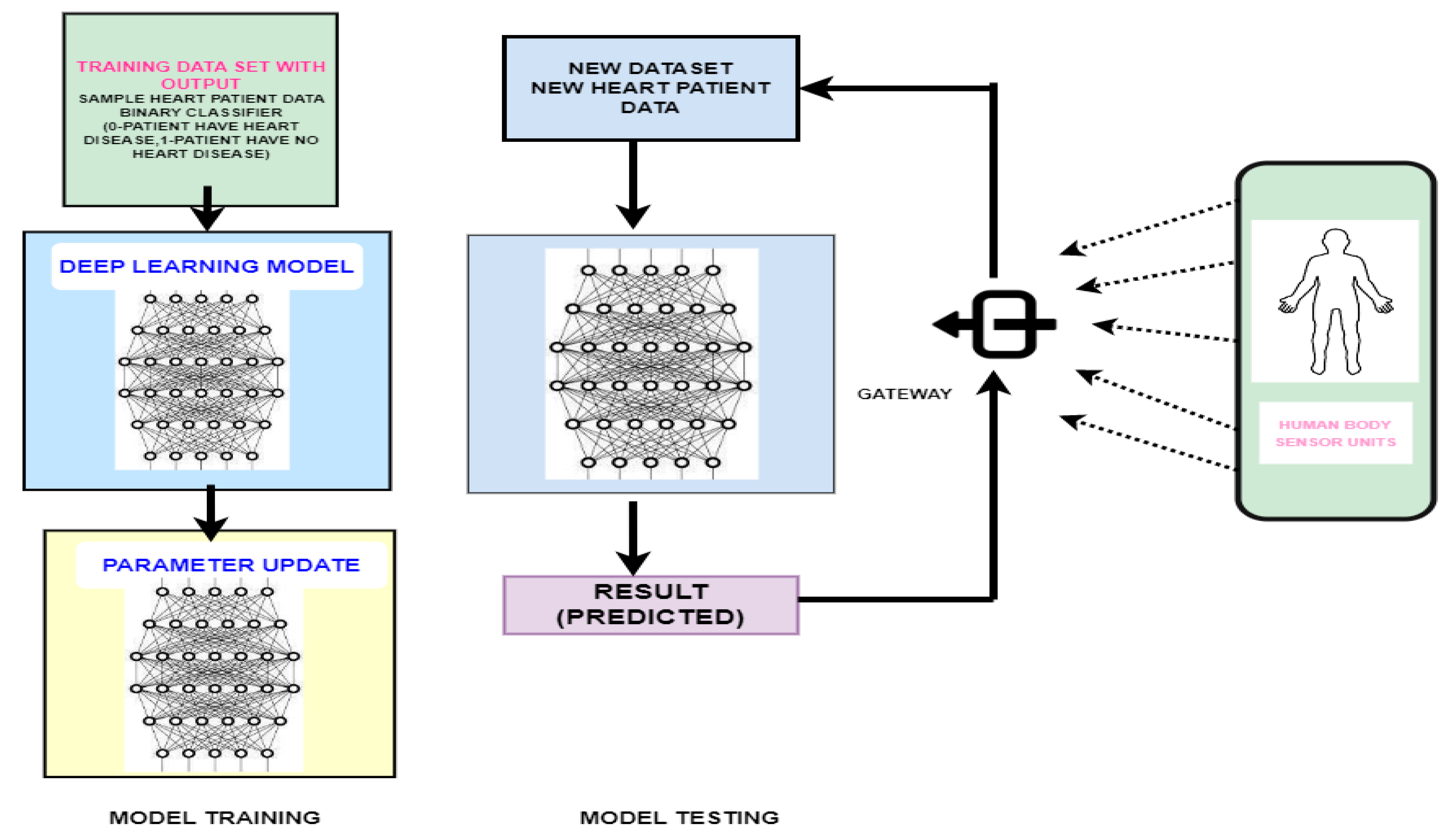
- Deep learning Module: The dataset is utilized to build a computational framework for locating data endpoints, which will contain the vectors created after pre-processing the data acquired from this wireless body area network. This forecasts and processes the output for the information acquired from these intelligent gateway devices based on the task assigned by the resource supervisor.
- Ensemble Module: This component estimates the output class, or if the individual has cardiac dysfunction, utilizes the polling data from a variety of models. The feature, which is hosted on the task’s FogBus node, is responsible for conveying the accumulated dependable out-run through many worker end nodes.
5. Implementation
5.1. Data Processing Phase of Heart Patient
5.2. Application of Deep Learning Ensemble
5.3. Proposed Deep Q Learning Based Prediction
| Algorithm 1 Proposed algorithm |
| function DQN |
| Input: |
| Output: |
| Initialize: |
| Set of states |
| Set of actions |
| Probability of transitioning the present state |
| Set of rewards |
| Reward discount factor |
| Compute: |
| for do |
| ifanddo |
| end if |
| end for |
| return |
| Exit |
6. Experimental Setup
6.1. Dataset
6.2. Performance Metrics
- Efficiency: as these fog nodes are nearer to the end user, it is closely integrated with the individual needs, which improves the performance and the efficiency of the entire framework. Combining the computational and storage resources across end-user devices and the cloud can also increase the performance [37,38].
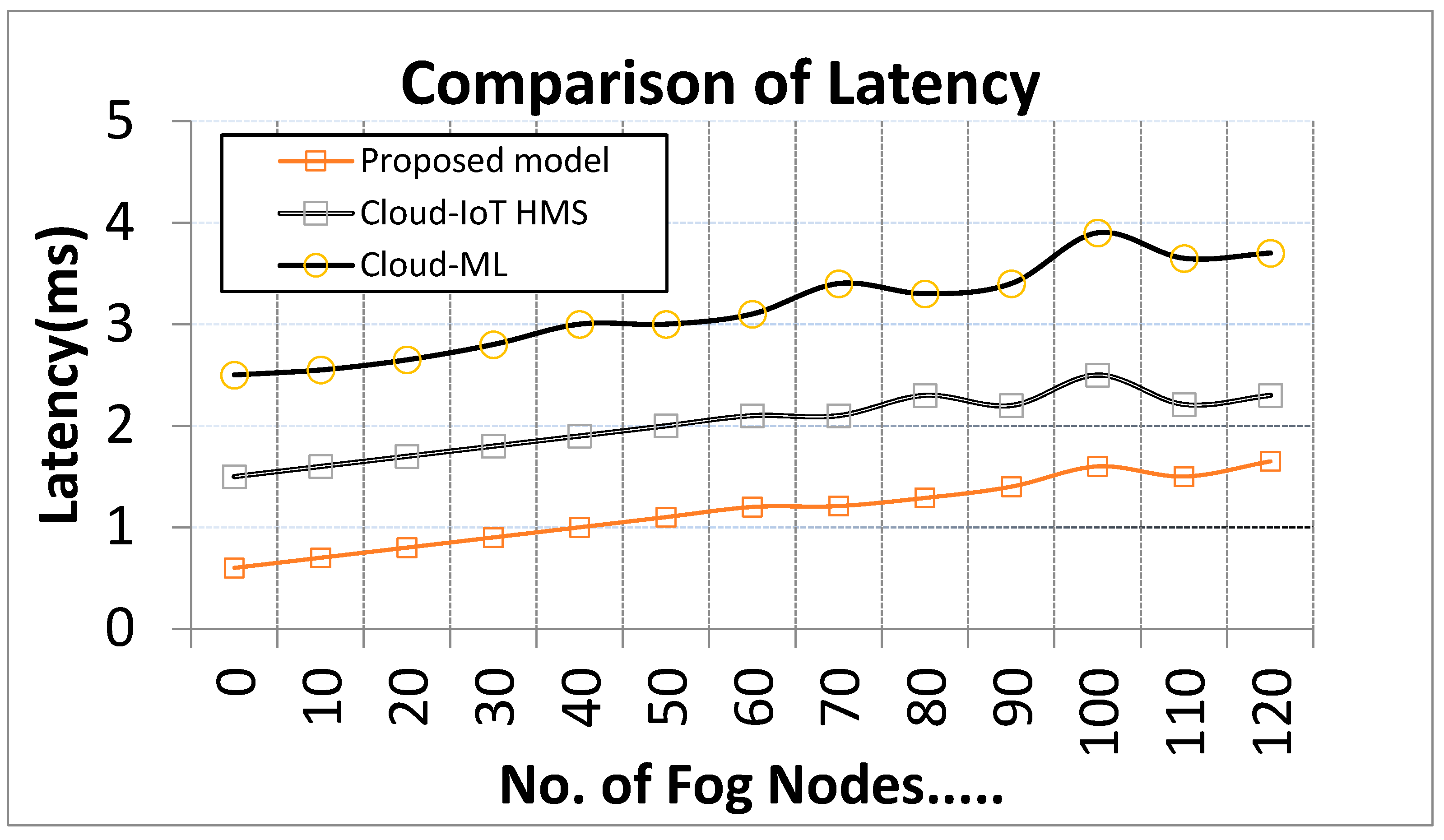
- Latency: certain essential services should not ever be suspended or deferred. Therefore, real-time stream processing for latency-sensitive applications, such as complicated event processing or stream mining, should be provided via fog computing to reduce the delay [39].
- Reliability: to decrease latency, the fog computing technique should be employed to provide real-time stream processing for latency-sensitive applications such as complicated event processing or stream mining [39]. A fog computing-based system should be dependable in that it can carry out its assigned tasks and deliver the correct results under predetermined conditions and within a specified time limit.
- Scalability: in the midst of increasing operational demands, such as a rise in the volume of service requests or the application of resources, a scalable system can maintain or improve its level of effectiveness and performance.
- Security: protecting the available cloud and fog data from threats using safe solutions is the major security problem in fog computing, along with device authentication at any gateway. An intrusion detection system (IDS) needs to be installed at each tier of the platform in order to address this issue [40].
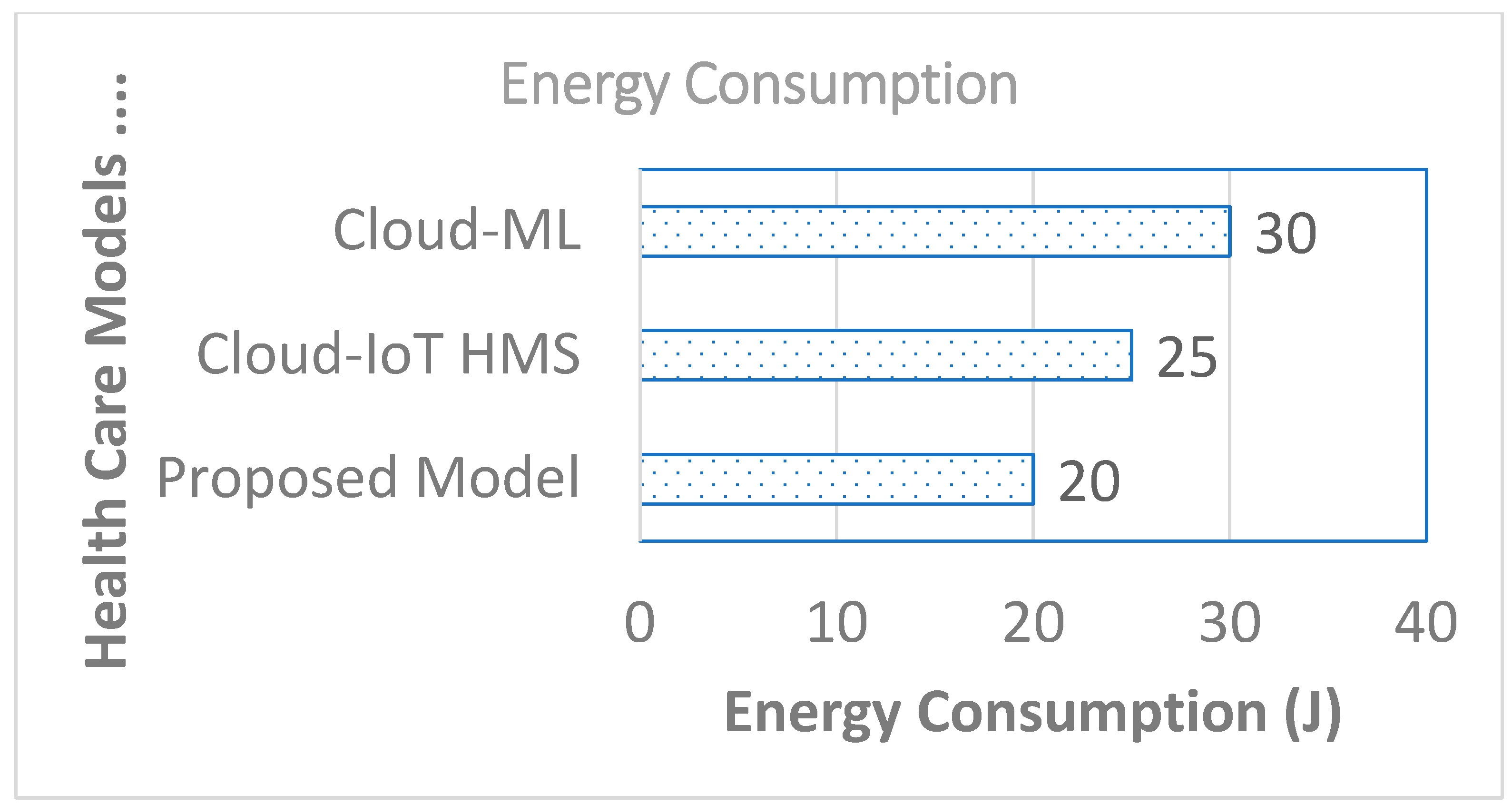
- Resource utilization: this describes the most effective use of a system’s resources and is crucial for maintaining efficiency.
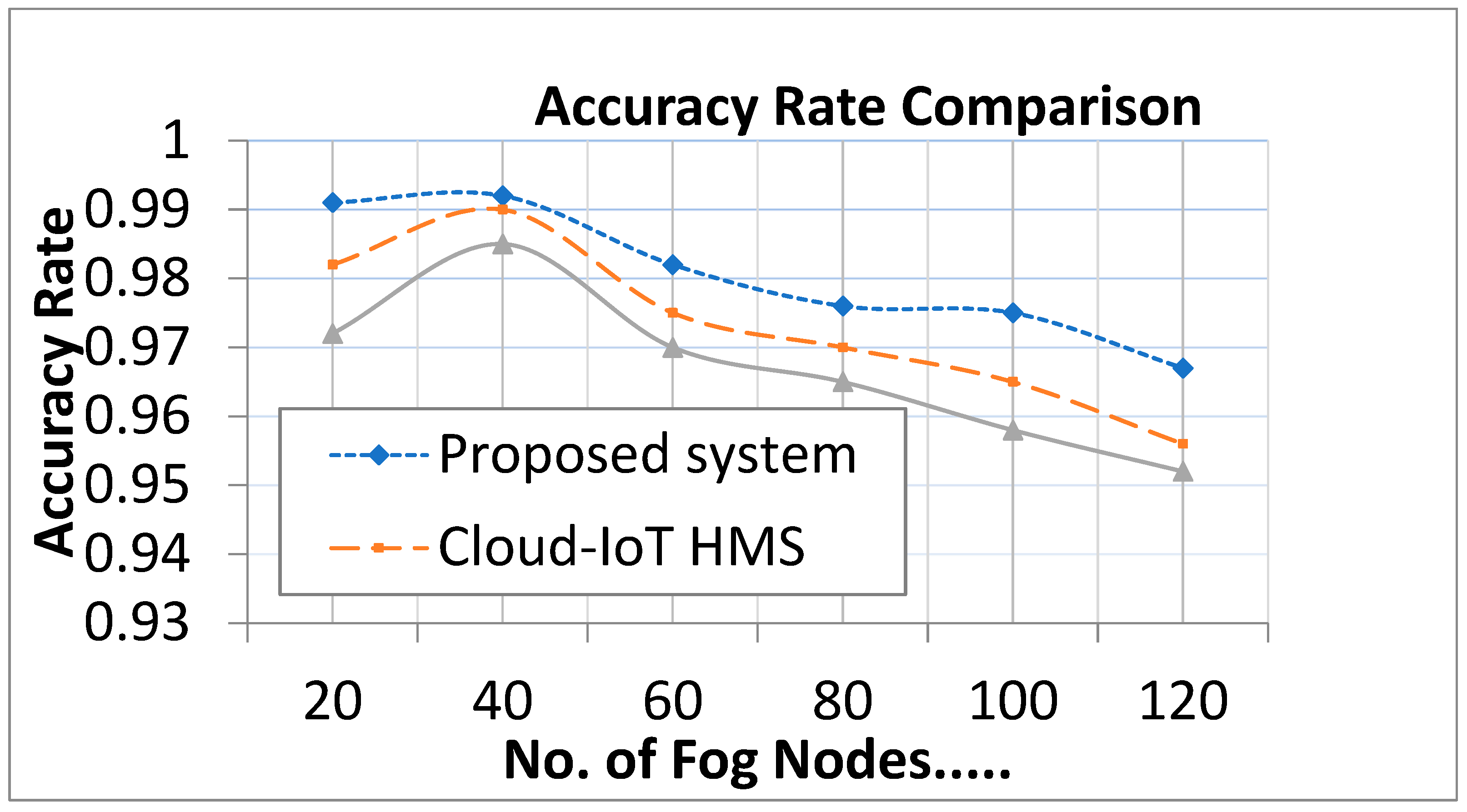
- Accuracy: this refers to any parameter that is close to the ideal value or the accepted benchmark. Each calculation must be completed accurately, and the output must be error-free.
- Precision/Recall: two significant criteria for evaluating models and algorithms are recall and precision. The first displays the proportion of all relevant results that the algorithm successfully classified, while the second displays the proportion of algorithmic findings that are connected to the chosen topic.
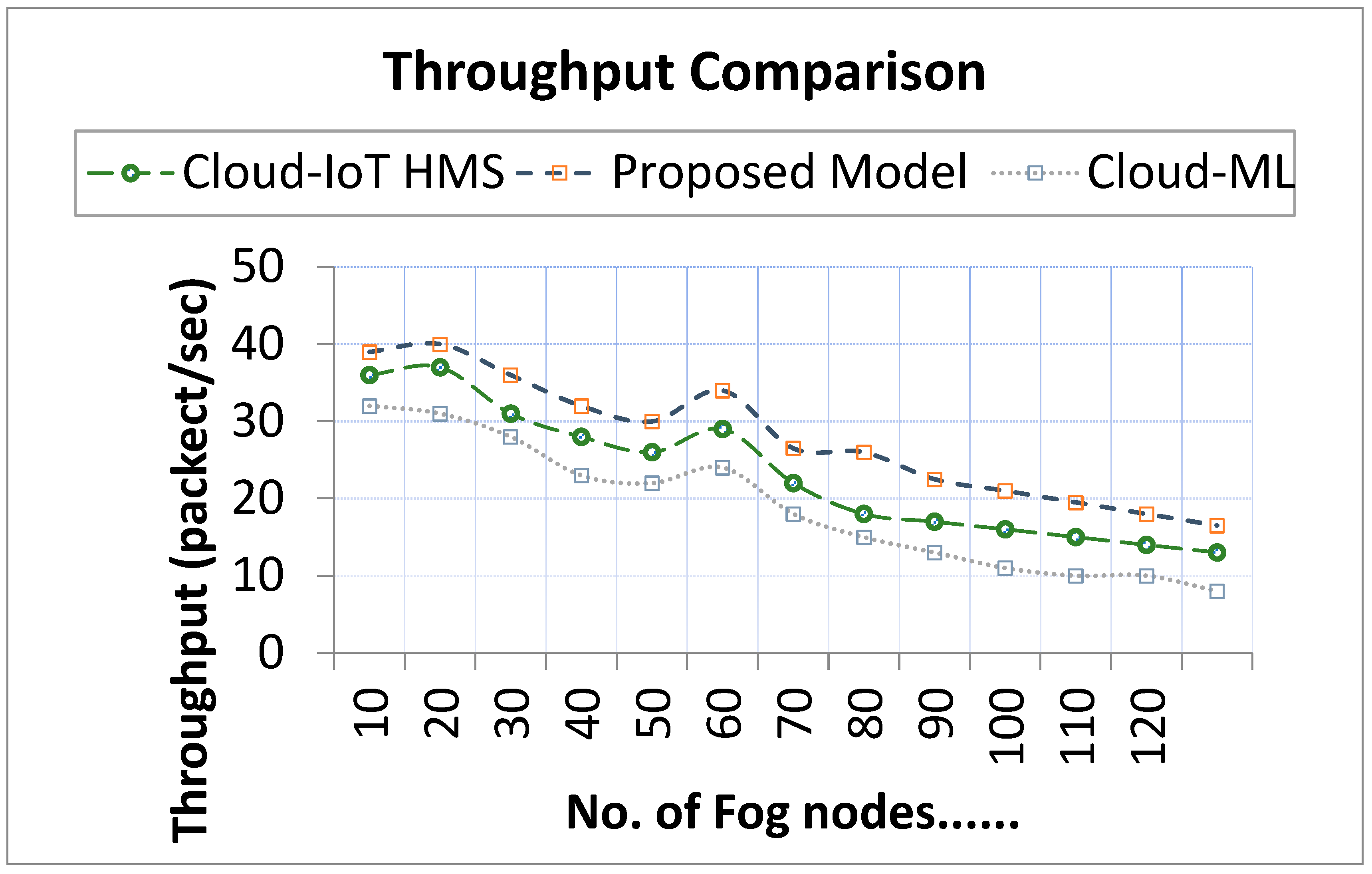
- Throughput: the term “throughput” specifies the greatest amount of data that can be sent from one point to another, or the most requested service rate that can be handled by the system in a specific amount of time.
- Response time: the time it takes for a system query to be replied to after being sent. For successful computing, quick response times could be essential.
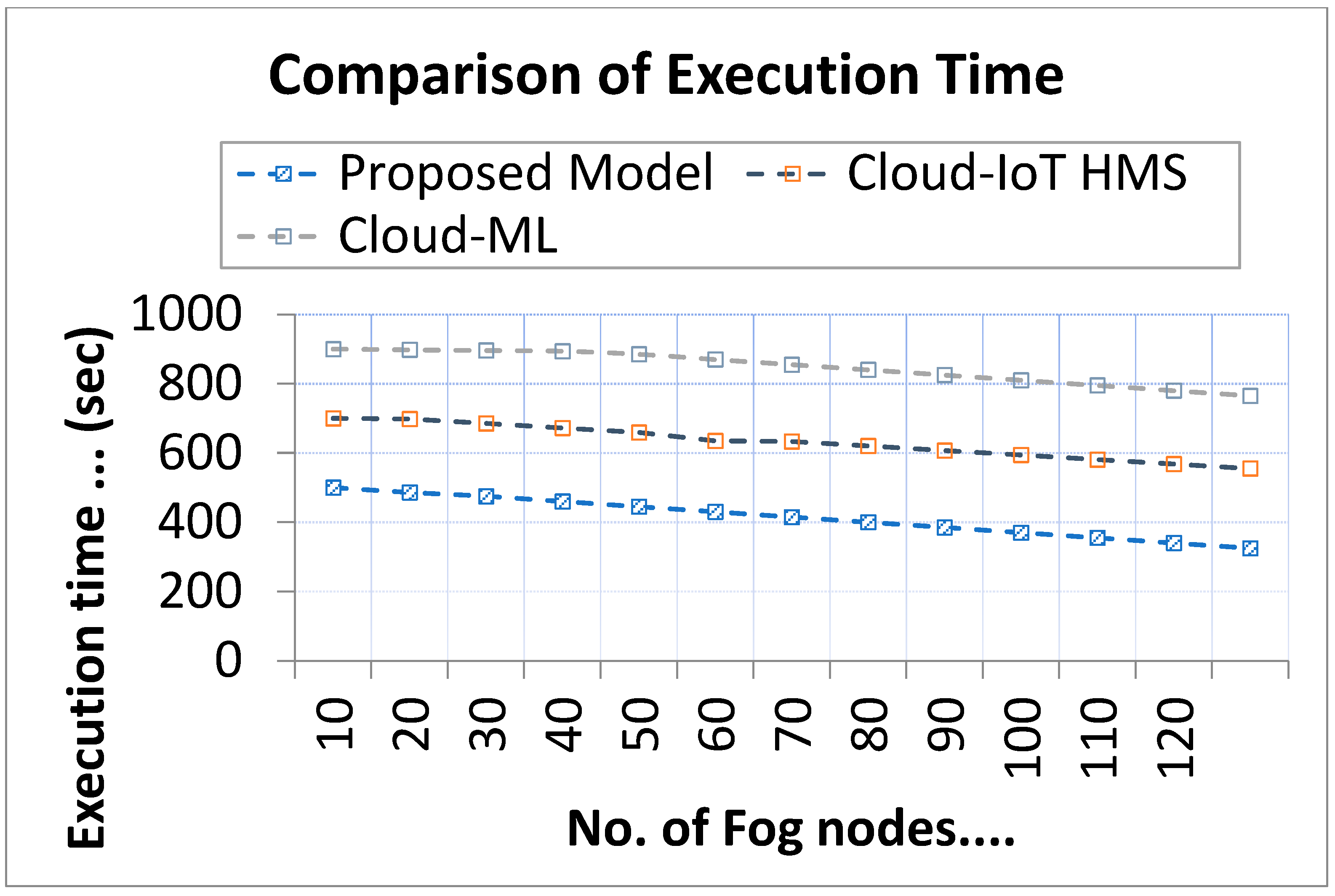
- Execution time: this is the amount of time that passes between when a program begins to run and when the user or operating system terminates it.
6.3. Comparative Analysis
7. Challenges and Future Work
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mahmud, R.; Koch, F.L.; Buyya, R. Cloud-Fog Interoperability in IoT-enabled Healthcare Solutions. In Proceedings of the 19th International Conference on Distributed Computing and Networking (ICDCN ‘18), Varanasi, India, 4–7 January 2018; Article 32; pp. 1–10. [Google Scholar] [CrossRef]
- Islam, S.M.R.; Kwak, D.; Kabir, M.D.H.; Hossain, M.; Kwak, K.S. The internet of things for health care: A comprehensive survey. IEEE Access 2015, 3, 678–708. [Google Scholar] [CrossRef]
- Rahmani, A.M.; Gia, T.N.; Negash, B.; Anzanpour, A.; Azimi, I.; Jiang, M.; Liljeberg, P. Exploiting smart e-health gateways at the edge of healthcare internet-of-things: A fog computing approach. Future Gener. Comput. Syst. 2018, 78, 641–658. [Google Scholar] [CrossRef]
- Goyal, A.; Kahlon, P.; Jain, D.; Soni, R.K.; Gulati, R.; Chhabra, S.T.; Aslam, N.; Mohan, B.; Anand, I.; Patel, V.; et al. Trend in prevalence of coronary artery disease and risk factors over two decades in rural Punjab. Heart Asia 2017, 9, e010938. [Google Scholar] [CrossRef] [PubMed]
- Tuli, S.; Basumatary, N.; Buyya, R. Edgelens: Deep learning based object detection in integrated iot, fog and cloud computing environments. In Proceedings of the 4th IEEE International Conference on Information Systems and Computer Networks (ISCON 2019), Mathura, India, 21–22 November 2019. [Google Scholar]
- Mutlag, A.A.; Ghani, M.K.A.; Arunkumar, N.; Mohammed, M.A.; Mohd, O. Enabling technologies for fog computing in healthcare IoT systems. Future Gener. Comput. Syst. 2019, 90, 62–78. [Google Scholar] [CrossRef]
- Faust, O.; Hagiwara, Y.; Hong, T.J.; Lih, O.S.; Acharya, U.R. Deep learning for healthcare applications based on physiological signals: A review. Comput. Methods Programs Biomed. 2018, 161, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Tuli, S.; Basumatary, N.; Gill, S.S.; Kahani, M.; Arya, R.C.; Wander, G.S.; Buyya, R. HealthFog: An ensemble deep learning based Smart Healthcare System for Automatic Diagnosis of Heart Diseases in integrated IoT and fog computing environments. Future Gener. Comput. Syst. 2020, 104, 187–200. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.; Yang, K.; Chen, Q.; Peng, D.; Jiang, H.; Xu, X.; Shuang, X. Deep learning based mobile data offloading in mobile edge computing systems. Future Gener. Comput. Syst. 2019, 99, 346–355. [Google Scholar] [CrossRef]
- Lim, T.-S.; Loh, W.-Y.; Shih, Y.-S. A comparison of prediction accuracy, complexity, and training time of thirty-three old and new classification algorithms. Mach. Learn. 2000, 40, 203–228. [Google Scholar] [CrossRef]
- Gill, S.S.; Arya, R.C.; Wander, G.S.; Buyya, R. Fog-Based Smart Healthcare as a Big Data and Cloud Service for Heart Patients Using IoT. In International Conference on Intelligent Data Communication Technologies and Internet of Things; Springer: Cham, Switzerland, 2018; pp. 1376–1383. [Google Scholar]
- Juarez-Orozco, L.E.; Martinez-Manzanera, O.; Van Der Zant, F.M.; Knol, R.J.J.; Knuuti, J. 241 Deep learning in quantitative PET myocardial perfusion imaging to predict adverse cardiovascular events. Eur. Heart J. Cardiovasc. Imaging 2019, 20, jez145.005. [Google Scholar] [CrossRef]
- Acharya, U.R.; Fujita, H.; Oh, S.L.; Hagiwara, Y.; Tan, J.H.; Adam, M. Application of deep convolutional neural network for automated detection of myocardial infarction using ECG signals. Inf. Sci. 2017, 415, 190–198. [Google Scholar] [CrossRef]
- Azimi, I.; Takalo-Mattila, J.; Anzanpour, A.; Rahmani, A.M.; Soininen, J.-P.; Liljeberg, P. Empowering healthcare IoT systems with hierarchical edge-based deep learning. In Proceedings of the 2018 IEEE/ACM International Conference on Connected Health: Applications, Systems and Engineering Technologies (CHASE), Washington, DC, USA, 26–28 September 2018; pp. 63–68. [Google Scholar]
- Gia, T.N.; Thanigaivelan, N.K.; Rahmani, A.M.; Westerlund, T.; Liljeberg, P.; Tenhunen, H. Customizing 6LoWPAN networks towards Internet-of-Things based ubiquitous healthcare systems. In Proceedings of the NORCHIP 2014—32nd NORCHIP Conference: The Nordic Microelectronics Event, Tampere, Finland, 27–28 October 2014; pp. 1–6. [Google Scholar]
- Gómez, J.; Oviedo, B.; Zhuma, E. Patient monitoring system based on internet of things. Procedia Comput. Sci. 2016, 83, 90–97. [Google Scholar] [CrossRef] [Green Version]
- Fanucci, L.; Saponara, S.; Bacchillone, T.; Donati, M.; Barba, T.; Sanchez-Tato, I.; Carmona, C. Sensing devices and sensor signal processing for remote monitoring of vital signs in chf patients. IEEE Trans. Instrum. Meas. 2013, 62, 553–569. [Google Scholar] [CrossRef]
- Natarajan, K.; Prasath, B.; Kokila, P. Smart health care system using internet of things. J. Netw. Commun. Emerg. Technol. 2016, 6, 37–42. [Google Scholar]
- Abdelmoneem, R.M.; Benslimane, A.; Shaaban, E.; Abdelhamid, S.; Ghoneim, S. A Cloud-Fog Based Architecture for IoT Applications Dedicated to Healthcare. In Proceedings of the ICC 2019-2019 IEEE International Conference on Communications (ICC), Shanghai, China, 20–24 May 2019; pp. 1–6. [Google Scholar]
- Rajkomar, A.; Oren, E.; Chen, K.; Dai, A.M.; Hajaj, N.; Hardt, M.; Liu, P.J.; Liu, X.; Marcus, J.; Sun, M.; et al. Scalable and accurate deep learning with electronic health records. NPJ Digit. Med. 2018, 1, 18. [Google Scholar] [CrossRef]
- Pham, M.; Mengistu, Y.; Do, H.; Sheng, W. Delivering home healthcare through a cloud-based smart home environment (CoSHE). Future Gener. Comput. Syst. 2018, 81, 129–140. [Google Scholar] [CrossRef]
- Alam, G.R.; Munir, S.; Uddin, Z.; Alam, M.S.; Dang, T.N.; Hong, C.S. Edge-of-things computing framework for cost-effective provisioning of healthcare data. J. Parallel Distrib. Comput. 2019, 123, 54–60. [Google Scholar] [CrossRef]
- Moosavi, S.R.; Gia, T.N.; Nigussie, E.; Rahmani, A.M.; Virtanen, S.; Tenhunen, H.; Isoaho, J. End-to end security scheme for mobility enabled healthcare Internet of Things. Future Gener. Comput. Syst. 2016, 64, 108–124. [Google Scholar] [CrossRef]
- Alazeb, A.; Panda, B.; Almakdi, S.; Alshehri, M. Data Integrity Preservation Schemes in Smart Healthcare Systems That Use Fog Computing Distribution. Electronics 2021, 10, 1314. [Google Scholar] [CrossRef]
- Alesanco, A.; García, J. Clinical assessment of wireless ECG transmission in real-time cardiac telemonitoring. IEEE Trans. Inf. Technol. Biomed. 2010, 14, 1144–1152. [Google Scholar] [CrossRef]
- Fettweis, G.P. The tactile internet: Applications and challenges. IEEE Veh. Technol. Mag. 2014, 9, 64–70. [Google Scholar] [CrossRef]
- Kraemer, F.A.; Braten, A.E.; Tamkittikhun, N.; Palma, D. Fog computing in healthcare–a review and discussion. IEEE Access 2017, 5, 9206–9222. [Google Scholar] [CrossRef]
- Nath, S.B.; Gupta, H.; Chakraborty, S.; Ghosh, S.K. A survey of fog computing and communication: Current researches and future directions. arXiv 2018, arXiv:1804.04365. [Google Scholar]
- Steele, R.; Lo, A. Telehealth and ubiquitous computing for bandwidth-constrained rural and remote areas. Pers. Ubiquit. Comput. 2013, 17, 533–543. [Google Scholar] [CrossRef]
- Yi, S.; Hao, Z.; Qin, Z.; Li, Q. Fog computing: Platform and applications. In Proceedings of the 3rd IEEE Workshop on Hot Topics in Web Systems and Technologies (HotWeb), Washington, DC, USA, 12–13 November 2015; pp. 73–78. [Google Scholar]
- Yi, S.; Li, C.; Li, Q. A survey of fog computing: Concepts, applications and issues. In Proceedings of the 2015 Workshop on Mobile Big Data, Hangzhou, China, 21 June 2015; pp. 37–42. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Ahmid, M.; Kazar, O. A Cloud-IoT Health Monitoring System Based on Smart Agent for Cardiovascular Patients. In Proceedings of the 2021 International Conference on Information Technology (ICIT), Amman, Jordan, 14–15 July 2021; pp. 1–6. [Google Scholar] [CrossRef]
- Ahmed, M.R.; Mahmud, S.M.H.; Hossin, M.A.; Jahan, H.; Noori, S.R.H. A Cloud Based Four-Tier Architecture for Early Detection of Heart Disease with Machine Learning Algorithms. In Proceedings of the 2018 IEEE 4th International Conference on Computer and Communications (ICCC), Chengdu, China, 7–10 December 2018; pp. 1951–1955. [Google Scholar] [CrossRef]
- Secinaro, S.; Calandra, D.; Secinaro, A.; Muthurangu, V.; Biancone, P. The role of artificial intelligence in healthcare: A structured literature review. BMC Med. Inform. Decis. Mak. 2021, 21, 125. [Google Scholar] [CrossRef] [PubMed]
- Kar, U.K. The Future of Health and Healthcare in a World of Artificial Intelligence. Arch. Biomed. Eng. Biotechnol. 2018, 1, 1–7. [Google Scholar] [CrossRef]
- Rodriguez-Romero, V.; Bergstrom, R.F.; Decker, B.S.; Lahu, G.; Vakilynejad, M.; Bies, R.R. Prediction of Nephropathy in Type 2 Diabetes: An Analysis of the ACCORD Trial Applying Machine Learning Techniques. Clin. Transl. Sci. 2019, 12, 519–528. [Google Scholar] [CrossRef] [Green Version]
- Kwak, G.H.; Hui, P. DeepHealth: Review and Challenges of Artificial Intelligence in Health Informatics, No. Ml. 2019. Available online: http://arxiv.org/abs/1909.00384 (accessed on 7 October 2022).
- Yang, S.; Zhu, F.; Ling, X.; Liu, Q.; Zhao, P. Intelligent Health Care: Applications of Deep Learning in Computational Medicine. Front. Genet. 2021, 12, 607471. [Google Scholar] [CrossRef]
- Kaul, D.; Raju, H.; Tripathy, B.K. Deep Learning in Healthcare. Stud. Big Data 2022, 91, 97–115. [Google Scholar] [CrossRef]
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; Depristo, M.; Chou, K.; Cui, C.; Corrado, G.; Thrun, S.; Dean, J. A guide to deep learning in healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tripathy, S.S.; Rath, M.; Tripathy, N.; Roy, D.S.; Francis, J.S.A.; Bebortta, S. An Intelligent Health Care System in Fog Platform with Optimized Performance. Sustainability 2023, 15, 1862. https://doi.org/10.3390/su15031862
Tripathy SS, Rath M, Tripathy N, Roy DS, Francis JSA, Bebortta S. An Intelligent Health Care System in Fog Platform with Optimized Performance. Sustainability. 2023; 15(3):1862. https://doi.org/10.3390/su15031862
Chicago/Turabian StyleTripathy, Subhranshu Sekhar, Mamata Rath, Niva Tripathy, Diptendu Sinha Roy, John Sharmila Anand Francis, and Sujit Bebortta. 2023. "An Intelligent Health Care System in Fog Platform with Optimized Performance" Sustainability 15, no. 3: 1862. https://doi.org/10.3390/su15031862