1. Introduction
Organizations are perceived as having a unique identity by their employees, and this new identity has the potential to influence employee behavior. According to the concept of organizational health, employees are dedicated to their organizations, their roles are defined and valuable, and they experience exceptional performance and a sense of belonging to their work. To build a healthy society, health organizations must be established that are defined by continuity, survival in their environment, adaptation, and upgrading and growing their adaptive potential (Charoghchian Khorasani et al., 2020) [
1].
Organizational health (OH) has been an actively examined topic with increasing importance and magnitude in academia and industry.
A healthy organization improves employee performance and productivity, thereby positively promoting an organization’s image (Ikechukwu, et al., 2019) [
2]. In [
3], it is noted that in healthy organizations, culture, climate, and excellent practices create an environment that can support employee health and safety as well as organizational effectiveness. According to (Grawitch and Ballard, 2016) [
4], a healthy organization is conducive to a healthy and successful business, emphasizing the significant link between organizational profitability and worker well-being (Arnoux-Nicolas et al., 2016) [
5]. According to (Tantry & Ali, 2020) [
6], a healthy organization supports high employee performance, and employees have an interest in the organization’s future success. In line with the findings of (Gilani et al., 2023) [
7], organizational efficiency shows positive, relevant, and direct connections with indices of organizational health.
1.1. A Need for a Holistic Scale for Measuring Organizational Health
Organizational health has been identified as a critical factor in determining a company’s ability to establish, communicate, and implement a unified business strategy while sustaining highly engaged employees. In this paper, organizational health is defined as “the ability of an organization to cope with change and continue to function with a high performance by maintaining sustainable workplace culture.”
In [
8], it is mentioned that the long-term performance of an organization depends on its capacity to achieve strategic goals and align around them. To manage organizational health, the Organizational Health Index (OHI) emphasizes logical consistency, which includes quantitative evaluations, diagnostics, and success techniques that enable leaders to calculate and achieve the organizational health goals needed to sustain long-term performance. According to (Bridges, M. 2019) [
9], senior leaders may assess and attain the organizational health necessary to maintain long-term performance with the help of our quantitative diagnostics and tested formulas for success. In [
10], it is emphasized that to measure the health of any organization, a gauge must be used to compute the well-being of the company and its personnel in order to monitor the system’s performance and also the behavior of the employees.
Governments, the private sector, nonprofit organizations, and academics have all developed a variety of assessment and diagnostic frameworks that are currently in use to enhance organizational health and performance. Some are quantitative, while others are qualitative, but a framework that encompasses both qualitative and quantitative techniques of assessment is required to cover all of the important dimensions of organizational health and behavior. As a result, our scale was separated into two subscales: “Subscale A” for quantitative measurements and “Subscale B” for qualitative measurements. The combination of the two approaches can improve the credibility, validity, and application of this study while also contributing to the field of organizational health behavior research. Thus, the current study developed a construct for organizational health and behavior on unexplored features in previously published research.
1.2. Organizational Health Behavior Index—A Tool for Measuring Organizational Health
This paper attempts to propose a model and a tool for measuring the health of an organization called the OHBI.
The Organizational Health Behavior Index (OHBI) is a scale that measures the organizational health of any facility based on three needs (basic needs, corporate needs, and strategic needs) and eight factors (awareness, relations, appreciation, internal communication, engagement, employee persona, employee voice, and organizational culture) that lead to a healthy organizational culture, excellence in performance, and achievement of strategic objectives. It gives an accessible yet effective road map for leaders and managers to follow in order to promote organizational health (see
Appendix A).
The OHBI model will help the health of any public or private organization by detecting where the problem lies and repairing the system as a whole by studying trends and behavior.
A main indicator of an organization’s capacity to deliver consistent performance is the Organizational Health Index score. Based on our unique organizational effectiveness results and management practices, it assesses the health of the organization.
The term “index,” which is used interchangeably with “scale,” can be described as a specific type of scale composed of various indicators that are added together to generate a single summary score in order to reflect a theoretical construct. (Carmines & Woods 2004) [
11]. A scale, however, “takes advantage of differences in intensity among the attributes of the same variable to identify distinct patterns of response” (Babbie, 2003) [
12].
Healthy organizations produce overall returns to shareholders that are three times higher than unhealthy organizations, according to a McKinsey study. Alternatively, a company with poor organizational health has low employee engagement, retention challenges, and low morale, which have a negative snowball impact on teams and the company as a whole [
13]. As a result, it is critical to assess organizational health using an index that includes both qualitative and quantitative measuring approaches so that the results can assist organizations in responding to difficulties and capitalizing on opportunities in a changing business environment. The OHBI is a novel tool that can help improve organizational culture and employee engagement by contributing to the study of organizational behavior.
In the current research, the validation of the Organizational Health Behavior Index using a mix of qualitative and quantitative measures of assessment is supported by contextualized findings and useful implications that improve the study’s credibility, validity, and applicability as well as its contribution to the field of organizational health behavior research.
3. Methods
3.1. General Overview of Methodology
To improve the rigor and credibility of this study on the OHBI, this paper adopts a complete and systematic methodology. To ensure the validity and reliability of the produced measuring tool, the technique is structured across various phases and sample groups, integrating both quantitative and qualitative approaches (
Table 1).
3.2. Subscale A (Quantitative Scale)
In the first phase, Study 1 involved creating items and enlisting the help of eight subject experts to validate them for Subscale A. These professionals provided their knowledge to assure the scale’s relevancy and comprehensiveness. The second study was conducted on a sample of 496 people. The scale’s underlying structure was discovered via exploratory factor analysis.
The second phase began with Study 3, which used a larger sample of 3510 respondents to establish the scale’s dependability. CFA, performed with the same sample group in Study 4, served to validate the factor structure discovered in the EFA.
In the third phase, to establish criterion validity in Study 5, a second sample of 218 respondents was used. By linking the generated scale with external criteria, this phase proved that it accurately measured the targeted constructs.
3.3. Subscale B (Qualitative Scale)
Fourth Phase: The qualitative component of the investigation began with study 6, where item generation for Subscale B took place. The created items were reviewed by 5 subject experts to ensure content validity, confirming that the scale’s items covered all the desired dimensions.
Fifth Phase: Study 7 was carried out on a sample of 50 respondents to conduct content analysis for Subscale B. This stage dug into the qualitative comments, gleaning significant insights and trends. Interrater reliability was demonstrated in Study 8 by incorporating three subject experts, which increased the credibility of the qualitative analysis.
The multiphase structure of the research demonstrated a well-thought-out strategy that blended quantitative and qualitative methods. The study not only verified the established measuring tool but also enriched our understanding of organizational health behavior by integrating subject specialists and utilizing varied sample groups. The study’s robustness was enhanced by this methodological approach, which ensured that the OHBI is a complete and trustworthy instrument for analyzing organizational health behavior determinants.
In the validation phase, the researchers ensured that the sample included a diverse group of employees working in various sectors to ensure that the OHBI was applicable to various groups. Moreover, the researchers ran statistical analyses to determine if there were any significant differences in the responses to the OHBI based on five demographics: gender, sector, domicile, tenure, and managerial level. These analyses helped ensure that the OHBI was not biased against any group of people.
Overall, the researchers were intentional in ensuring that equity, diversity, and inclusion were given due consideration throughout the development and validation of the OHBI. By doing so, the scale is inclusive and applicable to a diverse range of employees, which is essential for improving organizational health behavior and promoting employee well-being. Therefore, to address the objective of the current study, the authors attempted to develop an organizational health behavior measure that can incorporate both qualitative and quantitative methods of assessment to cover all the significant domains of organizational health and behavior. Therefore, the scale was divided into two subscales: “Subscale A” as a quantitative measure and “Subscale B” as a qualitative measure. The rationale for using both qualitative and quantitative assessment methods is as follows.
Organizational health behavior is a complex concept with many facets, including social, psychological, and physical components. Research can obtain a more complete knowledge of corporate health behavior by using both qualitative and quantitative metrics [
47]. The viewpoints, experiences, and interpretations of participants can be thoroughly explored using qualitative methods. These revelations can offer a rich framework for creating a quantitative subscale that accounts for all pertinent dimensions.
Utilizing qualitative data collection techniques offers the chance to investigate the conceptual underpinnings and underlying meaning of organizational health behavior. Qualitative measurements offer insightful information about the particular organizational context that may influence health behavior. This contextualization makes sure that the Organizational Health Behavior Index is applicable and relevant across a range of organizational settings. The study’s goal of offering practical implications to businesses is aligned with the inclusion of both qualitative and quantitative assessment measures. The study can provide complete insights and evidence-based suggestions to enhance organizational health behavior by combining both techniques.
In conclusion, the choice to create and validate the Organizational Health Behavior Index using a mix of qualitative and quantitative measures of assessment is supported by the need to accurately reflect the comprehensive nature of organizational health behavior, ensure contextualized findings, and offer useful implications. The two methodologies are combined, which improves the study’s credibility, validity, and applicability, as well as its contribution to the field of organizational health behavior research.
The methods and phases of development and validation are given in detail in the following sections.
5. Discussion
Organizations are a vital component of modern society and the national economy, and the health and well-being of their employees are critical for good customer service, a better society, and the sustainability of the organization. The most vital resource of any organization is the human resources—the employees. A conducive work environment enhances employee performance, increases a firm’s productivity, and thus promotes its image positively (Ikechukwu, et al., 2019) [
61]. In recent years, the COVID-19 pandemic significantly impacted organizational health behavior (Ranka, et al., 2020 [
62]; Shoss, 2021 [
63]; Sinclair, et al., 2021) [
64]. The pandemic underlined the significance of corporate health behavior in preserving employee well-being and productivity as firms were compelled to switch to remote work or adapt to new health and safety standards (Ekpanyaskul, & Padungtod, 2021) [
65]. Additionally, the pandemic revealed flaws in organizational health practices, notably regarding worker security, work–life balance, appreciation, relations, healthy engagements, communication, internal culture, and environment [
66]. There have been cases of insufficient safety precautions and exorbitant task demands as firms hurried to implement new policies and processes to protect personnel (D’Angelo, et al., 2022) [
67]. Additionally, managing professional and home duties while undertaking remote work has presented additional difficulties for employees, raising questions about burnout and mental health. Given these challenges, policymakers, managers, and CEOs are now prioritizing the improvement of organizational health behavior as a critical aspect of maintaining employee well-being and productivity in the post-pandemic era (Khurana, et al., 2021) [
68]. Organizations are investing in new strategies to support employee mental health, promote work-life balance, and create safe and supportive work environments (Fazal, et al., 2022) [
69]. This renewed focus on organizational health behavior reflects a growing recognition of its importance in fostering a healthy, engaged, and productive workforce (Kirsten 2022 [
70], Arief, et al., 2021) [
71]). Therefore, the concept of organizational health has become increasingly important as it helps organizations to achieve their objectives, enhance their competitive edge, and promote employee satisfaction and well-being. The current study aimed to develop and validate a multidimensional framework, a comprehensive measure of an organization’s health behavior, to gauge organizational health behavior determinants. The OHBI consists of two subscales: the quantitative Subscale A and the qualitative Subscale B. To ensure the reliability and validity of the OHBI, it was developed and validated using rigorous techniques.
Development of the OHBI: A comprehensive study of the available literature, expert consultations, and in-depth qualitative open-ended questions with organizational stakeholders were all part of the process of developing the OHBI. While professional discussions helped assure content validity and relevance, the literature study assisted in the identification of essential organizational health behavior aspects and indicators. The qualitative questions provide insightful information regarding how employees perceived and dealt with health behavior in the workplace. Additionally, a significant index of organizational health behavior was supplied by the quantitative items.
The study came out with an original two-subscale measure: the quantitative 5-point Likert type Subscale A of 16 items in five dimensions (awareness, appreciation, relations, employee engagement, and internal communication), and a qualitative Subscale B of 10 items in three dimensions (employee persona, organizational culture, and employee voice) called the Organization Health Behavior Index (OHBI).
Quantitative Analysis on Subscale A: Subscale A was established to collect quantitative information on several organizational health behavior dimensions. It was composed of carefully crafted Likert-scale questions that were based on the outcomes of the literature and expert consultations. To ensure its generalizability, the survey was given to sizable sample groups of workers from various industries and sizes of organizations. The fundamental elements influencing organizational health behavior were found using exploratory factor analysis. Confirmatory factor analysis was used to further support the findings, demonstrating the scale’s capacity to assess a variety of variables and guaranteeing the construct validity of the scale.
Validation: Several actions were performed to validate the OHBI. First, internal consistency analyses for Subscale A were performed. The results showed high Cronbach’s alpha values, which indicate a high level of internal reliability.
Additionally, the criterion-related validity of the OHBI was evaluated by comparing its results with the QISO. A significant relationship between the OHBI and QISO was shown, demonstrating the validity of the OHBI.
The OHBI is a scale that assesses an organization’s health behavior, which includes the attitudes, actions, and routines that support worker productivity and well-being. For subscale A, a quantitative Likert-type pool of 43 items was identified during the item generation phase, which was the first step in the creation of the OHBI. From Study 1 of the content validity analysis, 36 items were kept for additional examination. The succeeding stages of the OHBI’s development are covered in this chapter, including the reliability analysis, exploratory and confirmatory factor analyses, and the scale’s final iteration.
The development and calculation of the psychometric properties of the OHBI involved several phases. The first phase started with the item generation phase, where the authors identified 43 potential items. In Study 1, the 43-item pool was shared with field experts to carry out a content validity analysis, and 36 items were retained for further validation. In the second phase, data were taken on the 36-item set from a sample of 496 participants employed in the IT sector in Saudi Arabia. The data were assessed on skewness and kurtosis statistics to test the range of normality.
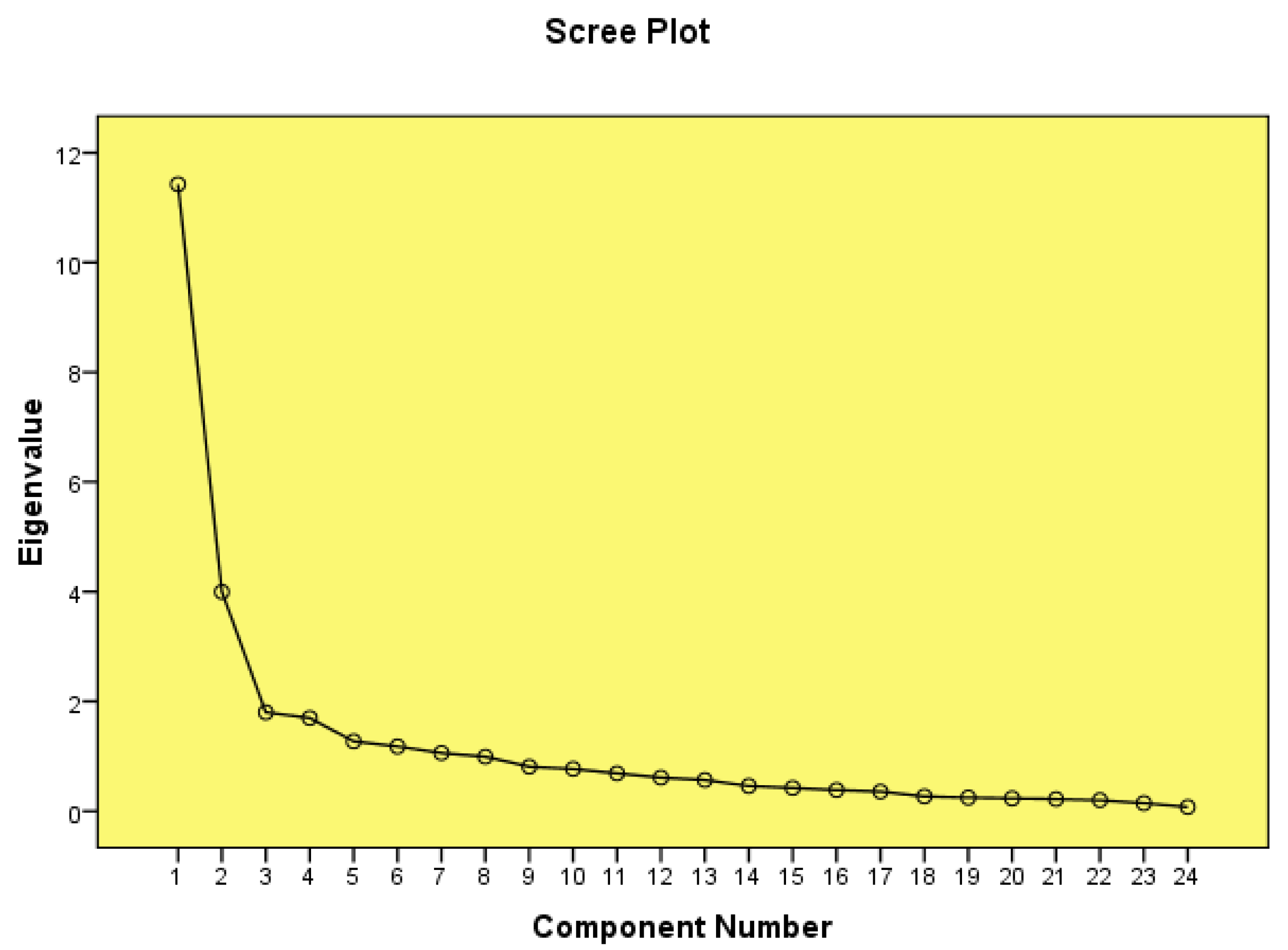
To find the latent factors for the OHBI model on the 36 items, exploratory factor analysis was used in the third phase. A 16-item, five-factor model was validated by the results of the exploratory factor analysis, and 20 items were dropped from the pool. The results of the exploratory factor analysis conducted in Study 2 supported a 16-item, five-factor model for the OHBI scale. The factors were (1) awareness, (2) appreciation, (3) relations, (4) employee engagement, and (5) internal communication. In the fourth phase, Study 3 evaluated the reliability of the OHBI model. All five factors had strong Cronbach’s alphas, ranging from 0.82 to 0.94.
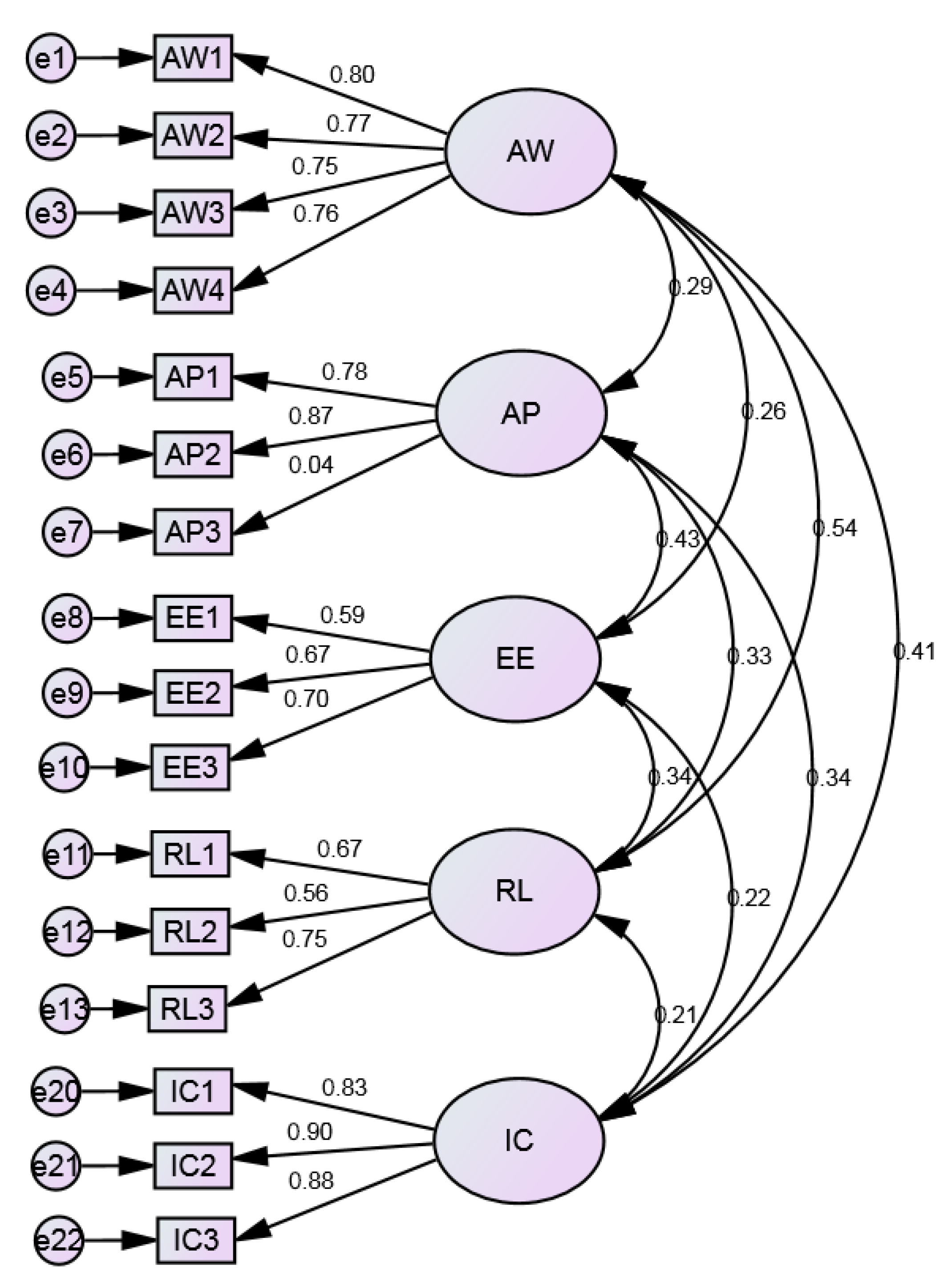
Confirmatory factor analysis in Study 4 was carried out in the fifth phase using a second sample of 3510 participants. The 16-item, five-factor model created during the exploratory factor analysis and reliability phase was confirmed by the findings of the confirmatory factor analysis. The model fit indices, including the chi-squared test, comparative fit index (CFI), Tucker–Lewis index (TLI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR), indicated a good fit for the model. The results provided evidence of the reliability and validity of the OHBI scale. The final version of Subscale A of the OHBI model consisted of 16 items in five dimensions.
In Study 5, concurrent validity was established in a third sample group. The seven subscales (39 items) of the QISO were used to establish correlations with five dimensions of the OHBI-16. The results showed good positive correlations between the dimensions of the OHBI and QISO, where all the coefficients ranged from 0.71 to 0.83.
The OHBI scale addressed all the essential psychometric properties of construction and validation, and is a valid and reliable measure of organizational health behavior. The scale’s internal consistency and construct validity is demonstrated by the scale’s 16-item, five-component model, which was created through exploratory factor analysis and validated through confirmatory factor analysis. The OHBI model’s five components represent important facets of organizational health behavior that might affect employee well-being and work.
Qualitative Analysis on Subscale B: The purpose of Subscale B, which focused on qualitative analysis, was to delve more deeply into employees’ qualitative experiences with corporate health behavior. Participants were able to share their perspectives, challenges, and experiences regarding health behavior in the organization through the use of open-ended questions. The qualitative data were subjected to thematic analysis, which allowed for the discovery of recurrent themes and patterns. The qualitative findings enhanced the understanding of organizational health behavior and gave the OHBI a relevant context by complementing the quantitative data.
The second subscale of the OHBI (Subscale B) was developed as a qualitative method to assess employee persona, organizational culture, and employee voice. In Study 6, the literature was thoroughly reviewed to generate 15 items. The preliminary subscale of 14 items was sent to five subject experts for review to ensure content validity. The experts approved 11 items for the subscale. In Study 7, the 11-item scale was administered to 50 employees taken from five sectors: agriculture, education, government, health, and logistics (10 from each sector). In Study 8, an interrater reliability was assessed by collecting reviews from three experts on the themes taken from the responses gathered on the 11-item pool. One item was deleted from organizational culture after the raters’ feedback, and a final pool of 10 items for Subscale B was developed. The three dimensions of Subscale B are employee persona (five items), organizational culture (three items), and employee voice (two open-ended items). Therefore, a final version of 10 items in three dimensions was developed for Subscale B.
6. Conclusions
There have been several studies that have developed and validated similar scales in the organizational health context. Organizational health has been extensively measured within single sectors, for example, the business sector (De Smet, et al., 2007) [
72], the education sector (Johnson Perry, 2015) [
73], the social care sector (Potter et al., 2016) [
74], and the healthcare sector (Nicolay et al., 2019) [
75], the nursing questionnaire on organizational health, and general practice organizational health (Williams, et al., 2022) [
76]. These scales have provided additional evidence of the importance of measuring organizational health behavior and its impact on employee well-being and job performance. However, these scales also have some limitations. For example, these scales focused on specific aspects of organizational health, while neglecting other important dimensions. This limited scope did not provide a comprehensive understanding of organizational health behavior. Moreover, the existing scales have been developed and validated in specific sectors, which may limit their applicability to other sectors. There is, however, a relative dearth of research considering the measurement of organizational health from a wider perspective, considering various sectors of the work field. While considering these limitations, there arose scope for developing a new scale that can address these issues and provide a more comprehensive and specific assessment of organizational health behavior from different sectors: a new 26-item scale that included two subscales. Subscale A is a quantitative measure of five dimensions: awareness, appreciation, relations, employee engagement, and internal communication. Subscale B is a qualitative measure of three dimensions: employee persona, organizational culture, and employee voice. The items were more specific and tailored to the organizational context and were developed and validated in a range of cultural settings to ensure cross-cultural validity. Additionally, efforts were made to minimize response bias by ensuring the anonymity of participants and using validated techniques for data collection and analysis. Therefore, a new scale that addresses these limitations can provide a more accurate and useful assessment of organizational health behavior.
Long overdue is the understanding of the significance of upstream performance determinants inside the organizational field. We will be able to evaluate and objectively assess the relative provision of organizational elements necessary for excellent performance over the long term by using measurements such as the OHBI. Overall, the OHBI, with its 26 items in eight dimensions, is a valuable addition to the field of organizational health measurement and provides a comprehensive assessment of organizational health behavior.
Practical Implications: Organizations can identify areas that need improvement with the help of the OHBI. Managers can identify priority areas and apportion resources appropriately by looking at the ratings on the various organizational health behavior characteristics. Interventions can be crafted to target certain flaws when organizational health behavior is thoroughly measured. Therefore, to enhance the areas with lower scores, organizations can create specialized training programs, workshops, or projects.
Workforce engagement is probably higher in organizations with higher OHBI ratings. The index can be used as a guide to establish a supportive workplace that encourages worker happiness, productivity, and retention. Utilizing the index, organizations can assess how well their health behavior scores compare to industry standards or best practices. This contrast enables students to comprehend where they are in relation to others and gain insight into effective tactics. Consequently, the OHBI may affect the way of making strategic choices. Organizations can make themselves more efficient and long-lasting by aligning their objectives and strategies with the factors that influence overall health behavior the most. The index may be used as another performance measurement. A culture of continuous improvement can be promoted by recognizing and rewarding teams or departments for their good contributions to organizational health behavior. It can be utilized to track the effects of large organizational changes on health behavior. Similarly, it can be applied as a part of a process of ongoing learning and development. Regular evaluations can shed light on the success of previous efforts and inform future tactics. Moreover, it can be used by organizations to evaluate the influence of leadership on health behavior. It enables the identification of areas that may require leadership training and development in order to generate a more positive organizational culture.
The OHBI, in conclusion, offers insightful information regarding an organization’s general health behavior and pinpoints particular areas for development. With the aid of this tool, businesses may carry out focused interventions, boost worker engagement, and connect strategies with health behavior characteristics, ultimately ensuring a productive and long-lasting workplace.





{kind=link}
{kind=link}