
Habitual Activities for People with Dementia: The Role of Interiors in Supporting Their Development after Relocating to a Care Environment

Abstract
:1. Introduction
2. Methods
2.1. Setting
2.2. Participants
- The participant is willing and able to give informed consent to participate in the study.
- Dementia has been diagnosed.
- The participant possesses the verbal ability to conduct an interview and the acting ability to observe.
- The participant has been living there for more than six months (because six months is a critical period for older people to become acquainted with the care environment).
2.3. Data Collection
2.4. Transcript and Analysis
2.5. Researcher Characteristics and Reflexivity
3. Results
3.1. Safety, Comfortable and Less Physical Effort as Basic Requirements
3.1.1. Safety
“Safety is the most important thing, and it’s important to make sure that they [people with dementia] don’t run into any danger or get injured while doing their activities ......”(Interview of the head of the institution)
“Now I’m not too worried about him ...... the doors here are not very obvious, and the windows are all locked, he can’t open them easily. So, it’s still very safe here ....... He can do more ......”(Interview of Li’s wife)
“It is safer than the previous (Wang’s home)......”(Interview of Wang’s daughter)
3.1.2. Comfortable
“We are glad that this place has a better environment compared to other care facilities... It’s not messy, it’s clean. The colors of the rooms are also warm, and the sofas and all this are very comfortable... He likes to do what he likes to do here.”(Interview of Li’s wife)
“I was scared that this was a hospital. But not here ...... It makes me feel comfortable and at ease. It makes me want to live like at home, the ones I’ve been doing ......”(Interview of Wang)
“It’s bright, clean, tidy and very harmonious ...... You can do so much more ......”(Interview of Zhang)
3.1.3. Less Physical Effort
“I can’t walk too far because my legs are no longer good, but here allows me to use the wheelchair all the time and allows me to walk from my room to the living room, which makes it easier for me to do what I want to do ....”(Interview of Zhang)
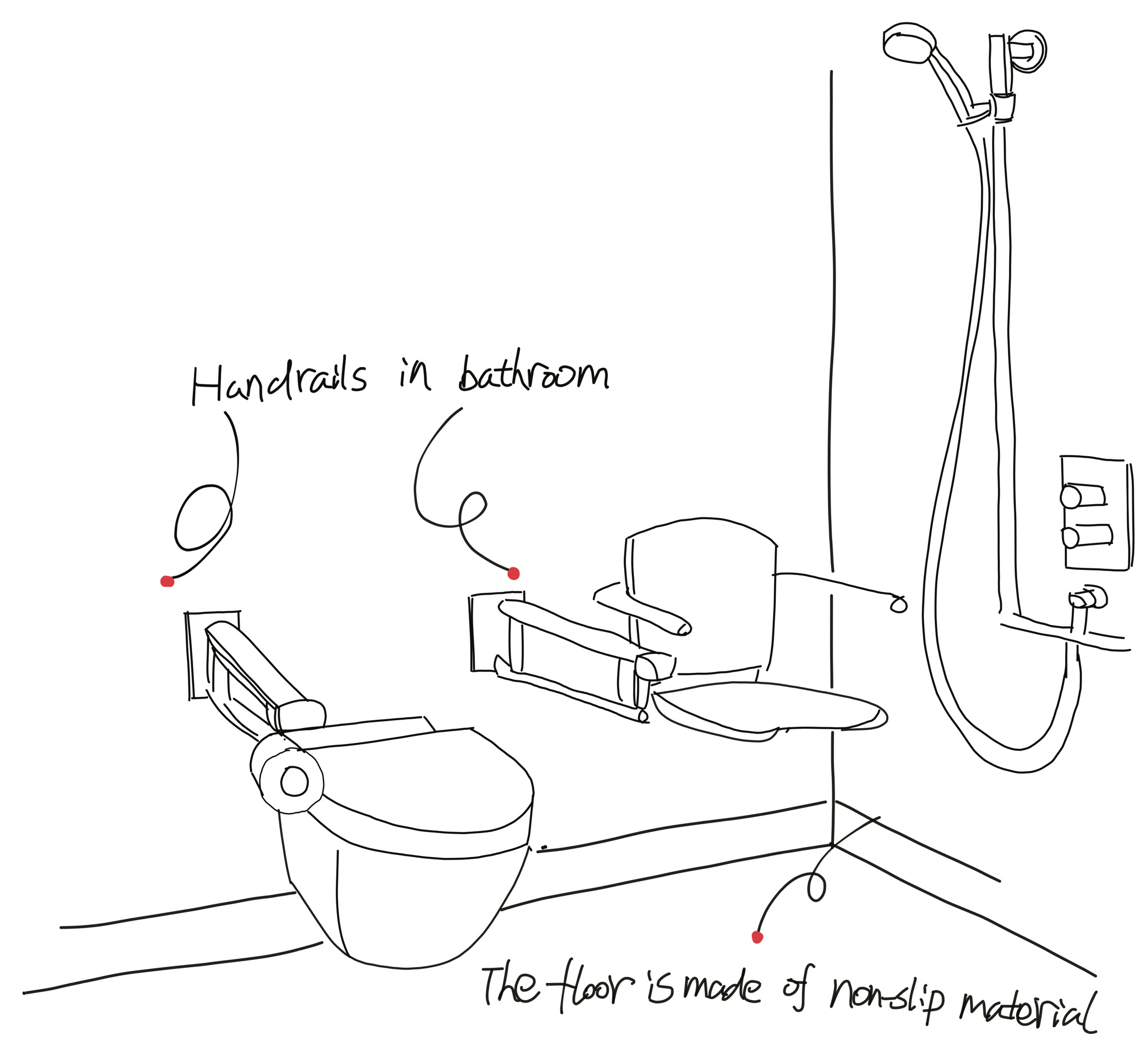
“Our facilities have many aids, such as beds to support getting up, accessible toilets and various handrails. These are all designed to help them with some of their daily activities.”(Interview of the head of the institution)
3.2. Familiar Information and Orderly Guidance (Continuing Habitual Activities Fluidly)
“I was the one who brought it (the old bamboo chair) here, it’s an old piece. Now, I brought it here......, He continued as before (watching TV, eating and napping in his seat) ...... I didn’t need to tell him, it happened naturally ......”(Interview of Li’s wife)
“I put all he needs in front of him, and he can easily see them ...... So he doesn’t have to hesitate when he does.”(Interview of Li’s wife)
“It’s the same set up as before, and he thinks it’s the original one (the balcony). He naturally continued what he was doing (watering the plants), just as he used to do at home ......”(Interview of Li’s wife)
“On the side of the balcony near the window, there are a few potted plants, which are in the most prominent position on the balcony, so Li can easily see them. Next to the potted plants are some watering tools, like a watering can and a small spade. These items are hung neatly on the right side of the plant so that [he] (Li) can easily reach them. A chair is placed directly opposite the plant for Li to sit on after watering.”(Observation notes)
“These (clothes) are placed by the bed every morning, which reminds me to put them on ...... It’s one of the most important things to do when you get up in the morning ......”(Interview of Wang)
“I would try to place her clothes in the order she wears them ........ For example, the top clothes are placed on the chair in order from inside out, while the bottom clothes, such as trousers and socks, are usually hitched to the back of the chair like this ....... This makes the process of dressing her easier. She only has to put them all on one by one. ....... ”(Interview of professional caregiver 2)
“......we try to put these things as neatly as possible, so they won’t be impossible to find.”(Interview of professional caregiver 3)
3.3. Visual Connection & Meaningful Resonance (Incorporating Positive Interaction into Habitual Activities)
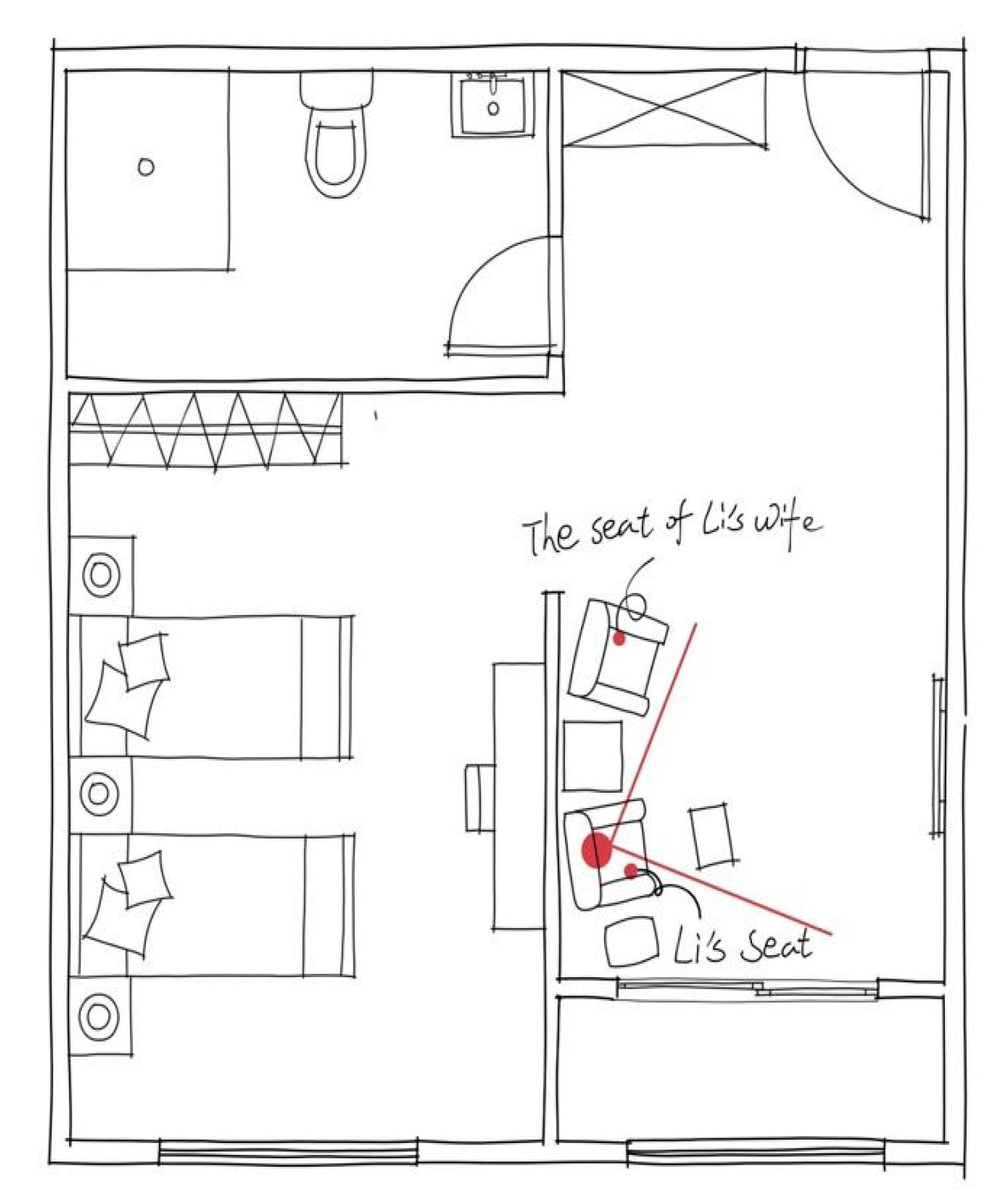
“His wife would sit in this chair and watch TV with him (Li) after doing her chores. As this chair was close to Li’s seat, this allowed Li to hold his wife’s hand and Li’s wife to help him sort out his clothes ......, and when others sat on it, he would show obvious displeasure and always pushed them away.”(Observation notes)
“She would always show me these things of hers and share stories from them. It made her want to open up with me ...... I could always find something to talk to her about too.”(Interview of professional caregiver 2)
“He’s here every day, and even though he just sits there...... we always interact with him when we’re not busy.”(The interview of professional caregiver 1)
“They both enjoyed playing chess and whenever he (Zhang) started fiddling with the board, it seemed to attract his (another resident’s desire to join in) ……”(Interview of professional caregiver 3)
3.4. Spatial Orientation & Temporal Orientation (Carrying out Habitual Activities Regularly)
“Probably because these places (Li’s activity areas) are all close together, he can easily find these places to do what he usually does.”(Interview of Li’s wife)
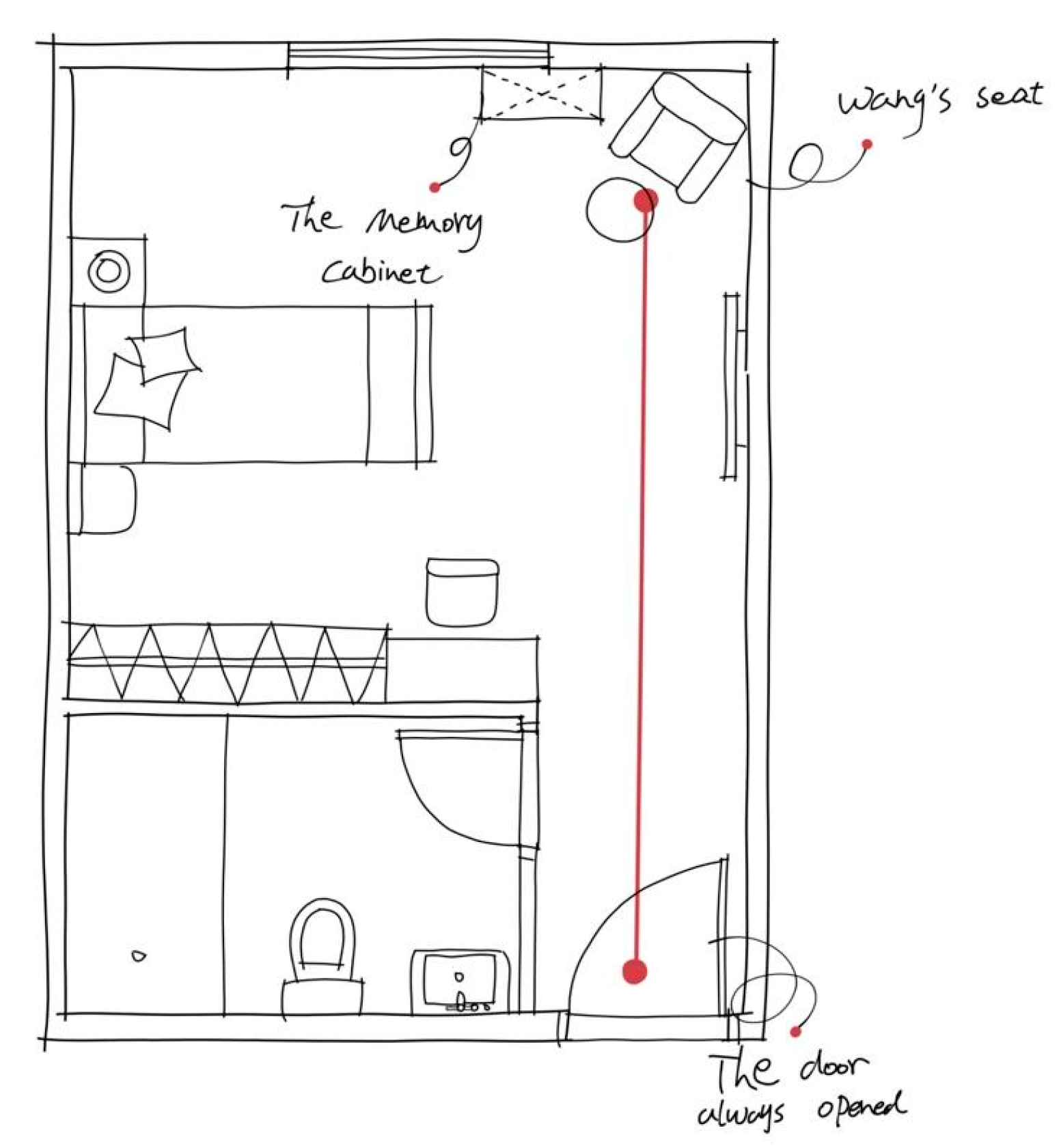
“I know very well, I need to be there can do what, even if sometimes I forget, these things (furniture and objects) can remind me.”(Interview of Wang)
“It’s not difficult (for morning activities); they (areas) are right next to each other.”(Interview of Wang)
“I become less sensitive to time, but it (bedspread) ...... tell me I shouldn’t be sleeping right now.”(Interview of Wang)
“I know where I’m going to do something, just hold on to the railing here (in the corridor) and keep going ...... It’s where you eat and where you watch TV… The doorways are marked. It’s not that hard.”(Interview of Zhang)
“When we start setting up, they know it’s time to eat.”(Interview of professional caregiver 3)
4. Discussion
5. Implications for Practice
- Creating home-living scenarios that are safe, comfortable, and have less physical effort for dementia residents.
- Ensuring the interior of the home-living scenario is familiar and orderly for residents with dementia.
- Creating visual contact and meaningful resonance with others in home-living scenarios for residents with dementia.
- Establishing spatial and temporal orientation between home-living scenarios for residents with dementia.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Merleau-Ponty, M.; Landes, D.; Carman, T.; Lefort, C. Phenomenology of Perception; Routledge: London, UK, 2011; ISBN 978-0-203-72071-4. [Google Scholar]
- Squire, L.R.; Zola-Morgan, S. The Medial Temporal Lobe Memory System. Science 1991, 253, 1380–1386. [Google Scholar] [CrossRef] [Green Version]
- Fuchs, T. Body Memory and the Unconscious. In Founding Psychoanalysis Phenomenologically; Lohmar, D., Brudzinska, J., Eds.; Phaenomenologica; Springer: Dordrecht, The Netherlands, 2012; Volume 199, pp. 69–82. ISBN 978-94-007-1847-0. [Google Scholar]
- Lally, P.; Van Jaarsveld, C.H.M.; Potts, H.W.W.; Wardle, J. How Are Habits Formed: Modelling Habit Formation in the Real World. Eur. J. Soc. Psychol. 2010, 40, 998–1009. [Google Scholar] [CrossRef] [Green Version]
- Wood, W.; Quinn, J.M.; Kashy, D.A. Habits in Everyday Life: Thought, Emotion, and Action. J. Personal. Soc. Psychol. 2002, 83, 1281–1297. [Google Scholar] [CrossRef]
- Wood, W.; Rünger, D. Psychology of Habit. Annu. Rev. Psychol. 2016, 67, 289–314. [Google Scholar] [CrossRef] [Green Version]
- Orbell, S.; Verplanken, B. The Automatic Component of Habit in Health Behavior: Habit as Cue-Contingent Automaticity. Health Psychol. 2010, 29, 374–383. [Google Scholar] [CrossRef]
- Neal, D.T.; Wood, W.; Drolet, A. How Do People Adhere to Goals when Willpower Is Low? The Profits (and Pitfalls) of Strong Habits. J. Personal. Soc. Psychol. 2013, 104, 959–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, W.; Neal, D.T. A New Look at Habits and the Habit-Goal Interface. Psychol. Rev. 2007, 114, 843–863. [Google Scholar] [CrossRef]
- Wood, W.; Neal, D.T. The Habitual Consumer. J. Consum. Psychol. 2009, 19, 579–592. [Google Scholar] [CrossRef]
- Butters, N.; Heindel, W.C.; Salmon, D.P. Dissociation of Implicit Memory in Dementia: Neurological Implications. Bull. Psychon. Soc. 1990, 28, 359–366. [Google Scholar] [CrossRef] [Green Version]
- Fleischman, D.A.; Gabrieli, J.D.E. Repetition Priming in Normal Aging and Alzheimer’s Disease: A Review of Findings and Theories. Psychol. Aging 1998, 13, 88–119. [Google Scholar] [CrossRef] [PubMed]
- Randolph, C.; Tierney, M.C.; Chase, T.N. Implicit Memory in Alzheimer’s Disease. J. Clin. Exp. Neuropsychol. 1995, 17, 343–351. [Google Scholar] [CrossRef]
- Fleischman, D.A.; Wilson, R.S.; Gabrieli, J.D.E.; Schneider, J.A.; Bienias, J.L.; Bennett, D.A. Implicit Memory and Alzheimer’s Disease Neuropathology. Brain 2005, 128, 2006–2015. [Google Scholar] [CrossRef] [Green Version]
- Golby, A. Memory Encoding in Alzheimer’s Disease: An FMRI Study of Explicit and Implicit Memory. Brain 2005, 128, 773–787. [Google Scholar] [CrossRef] [Green Version]
- Harrison, B.E.; Son, G.-R.; Kim, J.; Whall, A.L. Preserved Implicit Memory in Dementia: A Potential Model for Care. Am. J. Alzheimer’s Dis. Other Dement. 2007, 22, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Kontos, P.C. Embodied Selfhood in Alzheimer’s Disease: Rethinking Person-Centred Care. Dementia 2005, 4, 553–570. [Google Scholar] [CrossRef]
- Kontos, P.C. Ethnographic Reflections on Selfhood, Embodiment and Alzheimer’s Disease. Ageing Soc. 2004, 24, 829–849. [Google Scholar] [CrossRef] [Green Version]
- Twigg, J. Clothing and Dementia: A Neglected Dimension? J. Aging Stud. 2010, 24, 223–230. [Google Scholar] [CrossRef]
- Öhman, A.; Nygård, L. Meanings and Motives for Engagement in Self-Chosen Daily Life Occupations among Individuals with Alzheimer’s Disease. OTJR Occup. Particip. Health 2005, 25, 89–97. [Google Scholar] [CrossRef]
- Phinney, A.; Dahlke, S.; Purves, B. Shifting Patterns of Everyday Activity in Early Dementia: Experiences of Men and Their Families. J. Fam. Nurs. 2013, 19, 348–374. [Google Scholar] [CrossRef]
- Van Dijkhuizen, M.; Clare, L.; Pearce, A. Striving for Connection: Appraisal and Coping among Women with Early-Stage Alzheimer’s Disease. Dementia 2006, 5, 73–94. [Google Scholar] [CrossRef]
- Brataas, H.V.; Bjugan, H.; Wille, T.; Hellzen, O. Experiences of Day Care and Collaboration among People with Mild Dementia: Care and Collaboration among People with Mild Dementia. J. Clin. Nurs. 2010, 19, 2839–2848. [Google Scholar] [CrossRef] [PubMed]
- Phinney, A. Living with Dementia from the Patient’s Perspective. J. Gerontol. Nurs. 1998, 24, 8–9. [Google Scholar] [CrossRef] [PubMed]
- Fuchs, T. Embodiment and Personal Identity in Dementia. In In Defence of the Human Being; Oxford University Press: Oxford, UK, 2021; pp. 196–216. ISBN 978-0-19-289819-7. [Google Scholar]
- Phinney, A.; Chesla, C.A. The Lived Body in Dementia. J. Aging Stud. 2003, 17, 283–299. [Google Scholar] [CrossRef]
- Chaudhury, H.; Cooke, H.A.; Cowie, H.; Razaghi, L. The Influence of the Physical Environment on Residents With Dementia in Long-Term Care Settings: A Review of the Empirical Literature. Gerontologist 2018, 58, e325–e337. [Google Scholar] [CrossRef]
- Davis, S.; Byers, S.; Nay, R.; Koch, S. Guiding Design of Dementia Friendly Environments in Residential Care Settings: Considering the Living Experiences. Dementia 2009, 8, 185–203. [Google Scholar] [CrossRef]
- Woodbridge, R.; Sullivan, M.; Harding, E.; Crutch, S.; Gilhooly, K.; Gilhooly, M.; McIntyre, A.; Wilson, L. Use of the Physical Environment to Support Everyday Activities for People with Dementia: A Systematic Review. Dementia 2018, 17, 533–572. [Google Scholar] [CrossRef] [Green Version]
- Kitwood, T. The Experience of Dementia. Aging Ment. Health 1997, 1, 13–22. [Google Scholar] [CrossRef]
- Calkins, M.P. From Research to Application: Supportive and Therapeutic Environments for People Living with Dementia. Gerontologist 2018, 58, S114–S128. [Google Scholar] [CrossRef]
- Verbeek, H.; van Rossum, E.; Zwakhalen, S.M.G.; Kempen, G.I.J.M.; Hamers, J.P.H. Small, Homelike Care Environments for Older People with Dementia: A Literature Review. Int. Psychogeriatr. 2009, 21, 252–264. [Google Scholar] [CrossRef]
- Bruin, S.R.D.; Oosting, S.J.; Kuin, Y.; Hoefnagels, E.C.M.; Blauw, Y.H.; Groot, L.C.P.G.M.D.; Schols, J.M.G.A. Green Care Farms Promote Activity Among Elderly People with Dementia. J. Hous. Elder. 2009, 23, 368–389. [Google Scholar] [CrossRef]
- de Boer, B.; Hamers, J.P.H.; Zwakhalen, S.M.G.; Tan, F.E.S.; Beerens, H.C.; Verbeek, H. Green Care Farms as Innovative Nursing Homes, Promoting Activities and Social Interaction for People with Dementia. J. Am. Med. Dir. Assoc. 2017, 18, 40–46. [Google Scholar] [CrossRef]
- De Boer, B.; Beerens, H.; Katterbach, M.; Viduka, M.; Willemse, B.; Verbeek, H. The Physical Environment of Nursing Homes for People with Dementia: Traditional Nursing Homes, Small-Scale Living Facilities, and Green Care Farms. Healthcare 2018, 6, 137. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Son, G.-R.; Therrien, B.; Whall, A. Implicit Memory and Familiarity among Elders with Dementia. J. Nurs. Scholarsh. 2002, 34, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Chard, G.; Liu, L.; Mulholland, S. Verbal Cueing and Environmental Modifications: Strategies to Improve Engagement in Occupations in Persons with Alzheimer Disease. Phys. Occup. Ther. Geriatr. 2009, 27, 197–211. [Google Scholar] [CrossRef]
- Chen, J.; Gramegna, S.M.; Biamonti, A. A Sense of Home for People with Dementia in a Long-Term Care Facility: A Design Perspective. Health Place 2023, 79, 102957. [Google Scholar] [CrossRef]
- Harris, P.B.; McBride, G.; Ross, C.; Curtis, L. A Place to Heal: Environmental Sources of Satisfaction Among Hospital Patients1. J. Appl. Soc. Psychol. 2002, 32, 1276–1299. [Google Scholar] [CrossRef]
- Erickson, F. Some Approaches to Inquiry in School-Community Ethnography. Anthropol. Educ. Q. 1977, 8, 58–69. [Google Scholar] [CrossRef]
- Mehan, H. Structuring School Structure. Harv. Educ. Rev. 1978, 48, 32–64. [Google Scholar] [CrossRef]
- Mehus, S.E. Coordinating Care: A Microethnographic Investigation into the Interactional Practices of Childcare Workers. Doctoral Dissertation, The University of Texas at Austin, Austin, TX, USA, May 2006. [Google Scholar]
- Chen, Z.; Yang, X.; Song, Y.; Song, B.; Zhang, Y.; Liu, J.; Wang, Q.; Yu, J. Challenges of Dementia Care in China. Geriatrics 2017, 2, 7. [Google Scholar] [CrossRef] [Green Version]
- Dai, Y.; Zhao, J.; Li, S.; Zhao, C.; Gao, Y.; Johnson, C.E. Caregivers’ Dementia Knowledge and Care Approach in Residential Aged Care Facilities in China. Am. J. Alzheimer’s Dis. Other Dement. 2020, 35, 153331752093709. [Google Scholar] [CrossRef]
- Zhang, Y. Debating “Good” Care: The Challenges of Dementia Care in Shanghai, China. J. Assoc. Anthropol. Gerontol. 2020, 41, 52–68. [Google Scholar] [CrossRef] [Green Version]
- Palinkas, L.A.; Horwitz, S.M.; Green, C.A.; Wisdom, J.P.; Duan, N.; Hoagwood, K. Purposeful Sampling for Qualitative Data Collection and Analysis in Mixed Method Implementation Research. Adm. Policy Ment. Health Ment. Health Serv. Res. 2015, 42, 533–544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, J.C. The Clinical Dementia Rating (CDR): Current Version and Scoring Rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef] [PubMed]
- Fusch, P.I.; Fusch, G.E.; Ness, L.R. How to Conduct a Mini-Ethnographic Case Study: A Guide for Novice Researchers. Qual. Rep. 2017, 22, 923–942. [Google Scholar] [CrossRef]
- Patton, M.Q. Enhancing the Quality and Credibility of Qualitative Analysis. Health Serv. Res. 1999, 34, 1189–1208. [Google Scholar]
- Carter, N.; Bryant-Lukosius, D.; DiCenso, A.; Blythe, J.; Neville, A.J. The Use of Triangulation in Qualitative Research. Oncol. Nurs. Forum 2014, 41, 545–547. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T. A Beginner’s Guide to Ethnographic Observation in Nursing Research. Nurse Res. 2017, 24, 10–14. [Google Scholar] [CrossRef] [Green Version]
- Spradley, J.P. Participant Observation; Holt, Rinehart and Winston: Austin, TX, USA, 1980; ISBN 978-0-03-044501-9. [Google Scholar]
- Nowell, L.S.; Norris, J.M.; White, D.E.; Moules, N.J. Thematic Analysis: Striving to Meet the Trustworthiness Criteria. Int. J. Qual. Methods 2017, 16, 1609406917733847. [Google Scholar] [CrossRef]
- Clarke, V.; Braun, V.; Hayfield, N. Thematic Analysis. In Qualitative Psychology: A Practical Guide to Research Methods; SAGE: Washington, DC, USA, 2015; Volume 3, pp. 222–248. [Google Scholar]
- O’Brien, B.C.; Harris, I.B.; Beckman, T.J.; Reed, D.A.; Cook, D.A. Standards for Reporting Qualitative Research: A Synthesis of Recommendations. Acad. Med. 2014, 89, 1245. [Google Scholar] [CrossRef]
- Zanetti, O.; Zanieri, G.; Giovanni, G.D.; De Vreese, L.P.; Pezzini, A.; Metitieri, T.; Trabucchi, M. Effectiveness of Procedural Memory Stimulation in Mild Alzheimer’s Disease Patients: A Controlled Study. Neuropsychol. Rehabil. 2001, 11, 263–272. [Google Scholar] [CrossRef]
- Marquardt, G. Wayfinding for People with Dementia: A Review of the Role of Architectural Design. Health Environ. Res. Des. J. 2011, 4, 75–90. [Google Scholar] [CrossRef]
- Milke, D.L.; Beck, C.H.M.; Danes, S.; Leask, J. Behavioral Mapping of Residents’ Activity in Five Residential Style Care Centers for Elderly Persons Diagnosed with Dementia: Small Differences in Sites Can Affect Behaviors. J. Hous. Elder. 2009, 23, 335–367. [Google Scholar] [CrossRef]
- Kerkhof, Y.J.F.; Rabiee, F.; Willems, C.G. Experiences of Using a Memory Aid to Structure and Support Daily Activities in a Small-Scale Group Accommodation for People with Dementia. Dementia 2015, 14, 633–649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namazi, K.H.; Johnson, B.D. Physical Environmental Cues to Reduce the Problems of Incontinence in Alzheimer’s Disease Units. Am. J. Alzheimer’s Care Relat. Disord. Res. 1991, 6, 22–28. [Google Scholar] [CrossRef]
- Tanaka, M.; Hoshiyama, M. Effects of Environmental Stimulation on Recognition of Mealtimes in Patients with Dementia. Phys. Occup. Ther. Geriatr. 2014, 32, 112–122. [Google Scholar] [CrossRef]
- Calkins, M.P. The Physical and Social Environment of the Person with Alzheimer’s Disease. Aging Ment. Health 2001, 5, 74–78. [Google Scholar] [CrossRef]
- Cohen, U.; Weisman, G.D. Holding on to Home: Designing Environments for People with Dementia; Johns Hopkins University Press: Baltimore, MD, USA, 1991; ISBN 978-0-8018-4069-2. [Google Scholar]
- Fay, R.; Owen, C. ‘Home’ in the Aged Care Institution: Authentic or Ersatz. Procedia-Soc. Behav. Sci. 2012, 35, 33–43. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Participant | Participant Profile |
|---|---|
| Dementia residents | Li, Man, 85 years old, Alzheimer’s disease, CDR 2, 2 years of residence Wang, Woman, 83 years old, Mixed dementia, CDR 1, 1.5 years of residence Zhang, Man, 79 years old, Mixed dementia, CDR 1, 1.5 years of residence |
| Dementia residents’ relatives | Li’s wife Wang’s daughter Zhang’s nephew |
| Dementia care staffs | Professional caregiver 1 Professional caregiver 2 Professional caregiver 3 Head of Institution |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, J.; Gramegna, S.M.; Biamonti, A.; Cao, Y. Habitual Activities for People with Dementia: The Role of Interiors in Supporting Their Development after Relocating to a Care Environment. Sustainability 2023, 15, 12324. https://doi.org/10.3390/su151612324
Chen J, Gramegna SM, Biamonti A, Cao Y. Habitual Activities for People with Dementia: The Role of Interiors in Supporting Their Development after Relocating to a Care Environment. Sustainability. 2023; 15(16):12324. https://doi.org/10.3390/su151612324
Chicago/Turabian StyleChen, Jing, Silvia Maria Gramegna, Alessandro Biamonti, and Yuwei Cao. 2023. "Habitual Activities for People with Dementia: The Role of Interiors in Supporting Their Development after Relocating to a Care Environment" Sustainability 15, no. 16: 12324. https://doi.org/10.3390/su151612324