4.1. Temporary Accessibility in the Health Area
The result of calculating the access time from each population entity and isolated tourist establishments to the Son Espases University Hospital, the reference hospital, and the regional health center configures a time cost matrix.
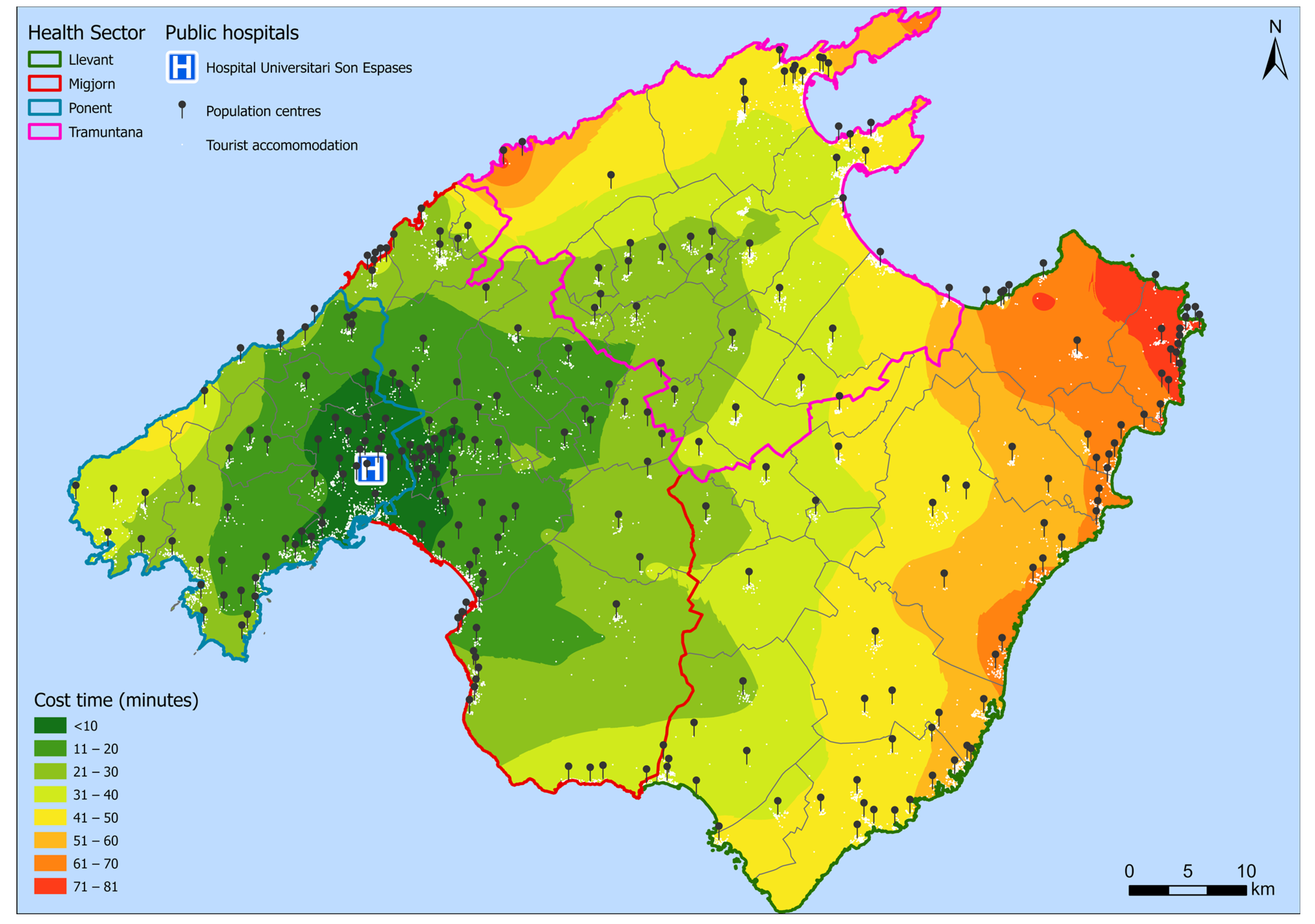
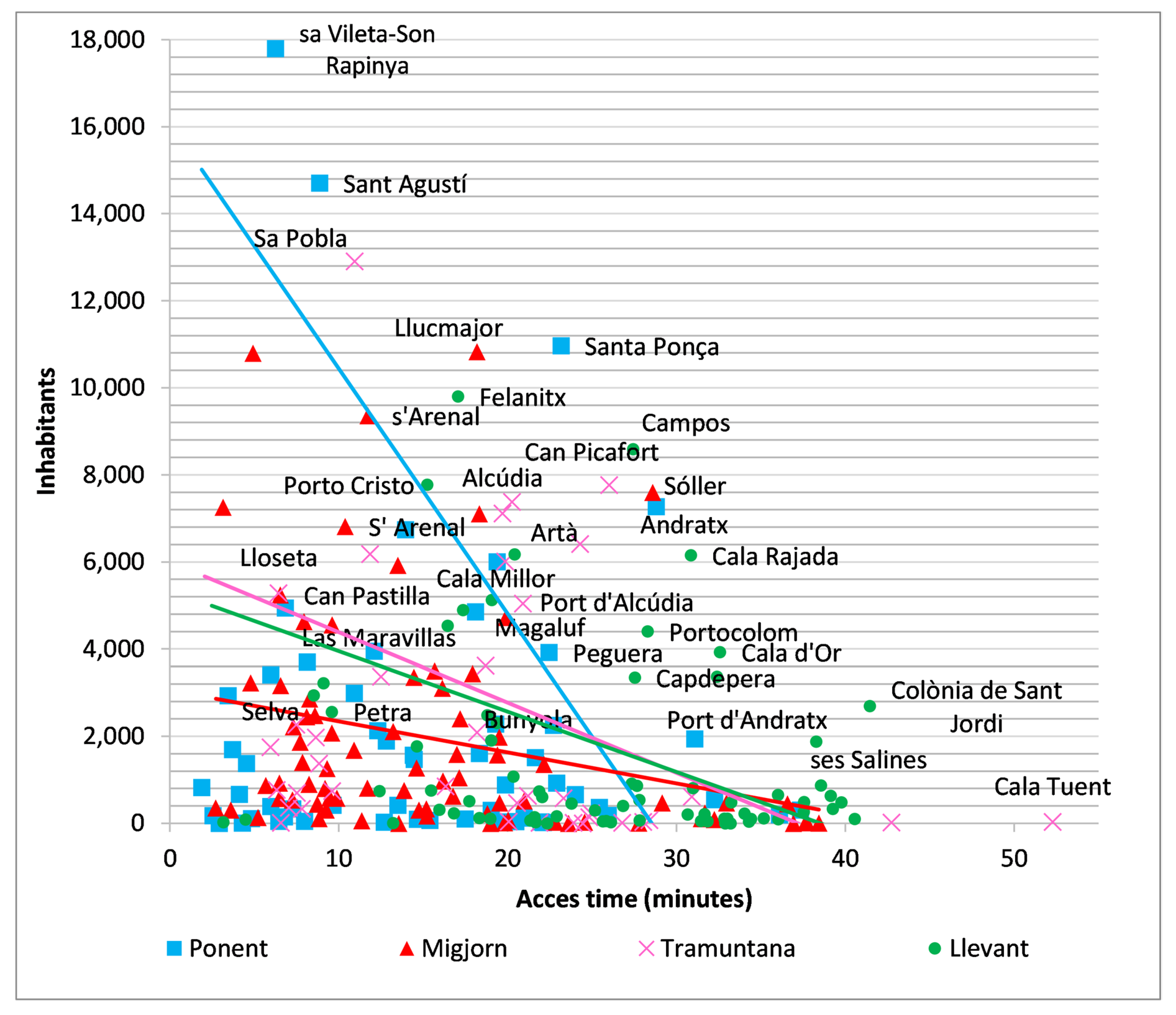
Figure 8 shows the access time of each population entity to the reference hospital (Son Espases). It is observed that the greatest accessibility is for the Ponent and Migjorn Sectors, with values that mostly do not exceed 30 min, with the exception of the most distant areas that occasionally reach 48 min. The Tramuntana Sector is further away, with trips reaching up to 52 min. Finally, the Llevant Sector is the furthest from the university hospital of Son Espases, although the travel time does not exceed 1 h and a half.
It is observed that the values of accessibility in minutes to the reference hospital divide the island into eight areas of 10 min intervals. A close spatial–temporal relationship is evident, which reproduces the radial arterial system of the main road network and high-capacity roads.
Accessibility is almost less than 30 min in the Sectors of Ponent and Migjorn, with some exceptions in the most peripheral nuclei, while, in Tramuntana, accessibility is distributed between 21 and 50 min. Finally, in the Llevant Sector, only a few nuclei are under 30 min, with the nuclei of the eastern coast standing out as the farthest locations from the reference hospital, which are around 1 h or more away. This distribution is justified if it is considered in relation to the resident population, an essential aspect, since the objective of health facilities is to provide services to people.
Table 5 shows the proportion of the resident population, the tourist population, and the sum of both included within each isochrone. It can be seen how the location of the Son Espases University Hospital, despite being located significantly to the west with respect to the geometric center of the island, is less than 10 min from 48.9% of the resident population, and can be reached by 76.4% of the population in less than 30 min, which means about 640,000 people. At the other extreme, 3.8% of the population, just over 31,000 inhabitants, is more than 60 min away from the reference hospital.
In terms of tourist accommodation, the distribution of accessibility changes substantially, with only 5% of tourist accommodations being within 10 min of the hospital, and 42% of the tourist accommodations being in the 30 min isochronous zone. At the other end of the scale, the areas located more than 60 min from the hospital account for almost 71,000 bed places, representing 17.7% of tourist accommodations, and 48% of the tourist bed places are located over 40 min away.
Finally, the potential population shows an intermediate distribution between the two previous ones, since the 10 min isochrone includes 34.7% of the population, and in the first 30 min it reaches 65.3%. After 60 min, the relative weight of the potential population is 8.3%.
4.2. Accessibility by Health Sectors
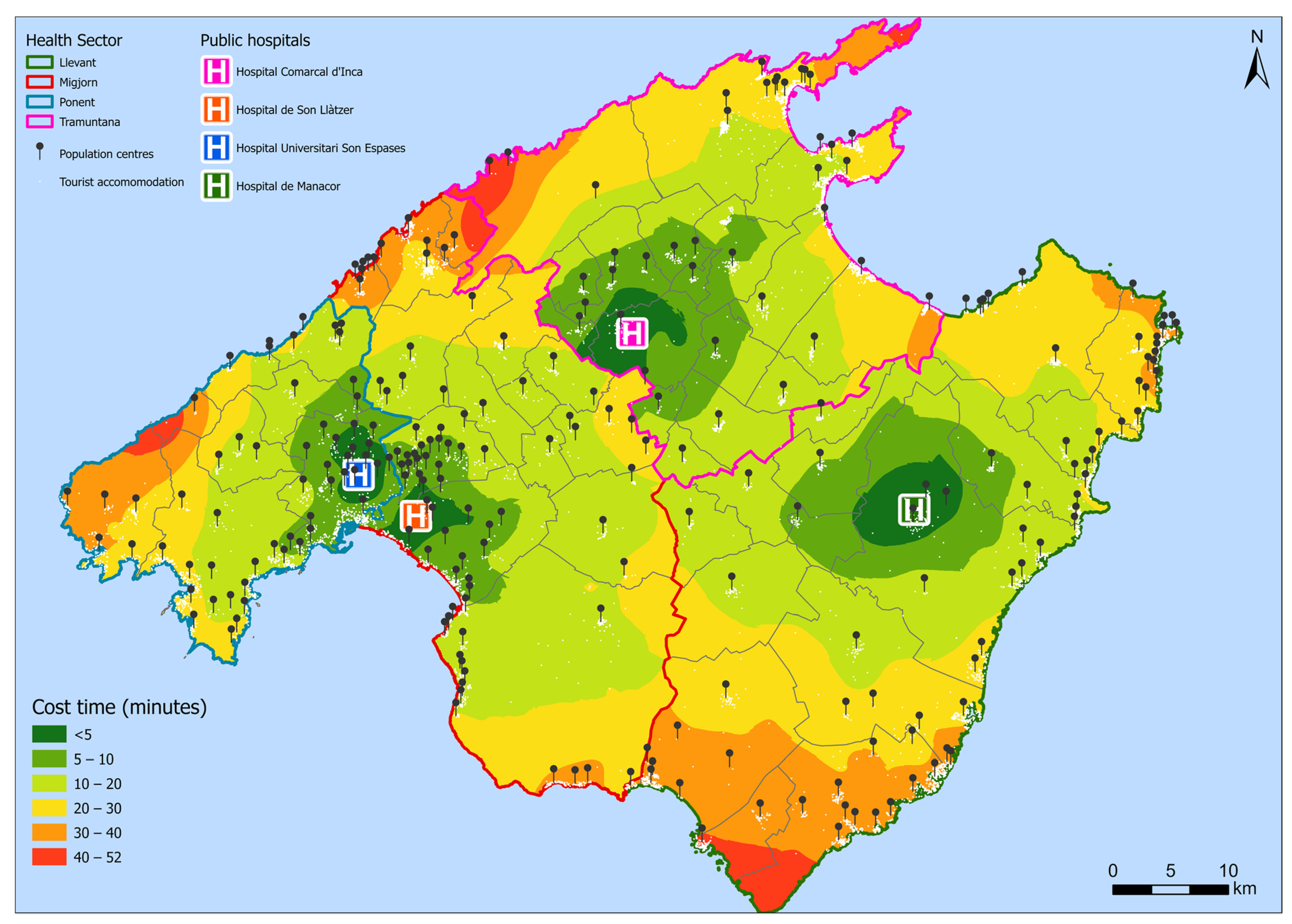
The results of the time cost matrix for each of the island’s Health Sectors can be seen in
Figure 9. In this case, the distribution of accessibility is notoriously better than in the case of the Health Area; however, the patterns observed previously in the more peripheral nuclei are maintained. Thus, in the Ponent Sector, with Son Espases, accessibility is less than 12 min for the main nuclei of the municipality of Palma and its peri-urban area, while this time increases to 31–40 min in the northwest coastal strip in the nuclei of Estellencs, Sant Elm, and S’Arracó. In the intermediate strip, there is a considerable number of towns with an access time ranging between 11 and 20 min.
In terms of accessibility by relative population (
Table 6), accessibility is very good, since 84.2% of the population of the Ponent Sector is less than 10 min away, and 99.3% of the inhabitants are below the 30 min isochrone. However, these values are altered by the use of the centroids of each population center, since more than 310,000 people live in the center of Palma and account for 72% of the population, and this area is just 7 min away.
On the other hand, the tourist weight of the Ponent Sector is relatively low, with 92,750 vacancies, which does not alter, roughly speaking, the accessibility of the potential tourist population. These vacancies are distributed mainly in the isochrones between 11 and 30 min, since 96% of them are in this range.
Next, the Migjorn Sector, despite covering a very large area, generally has an access time of less than 20 min, bringing together a notable group of nuclei of the peri-urban area of Palma that are under 10 min. As far as the extremes are concerned, there are two regions with an accessibility of between 31 and 40 min, which is explained by the Euclidean distance from the hospital, Son Llàtzer, in this case, but also due to the orography in the north of the island, where the nuclei of Sóller, Fornalutx, or Deià are located, which makes the road network difficult, with considerable slopes in some cases. On the other hand, the peripheral location of the southern nuclei, far from the main guiding nuclei of the area, has led to the underdevelopment of the road network, resulting in poorer accessibility.
In the Migjorn Health Sector, the distribution of the population by time intervals (
Table 7), again, is not proportional to the spatial distribution of these intervals, since the relative weight of the inhabitants between the isochrones of 6–10 and 11–20 stands out, totaling 77.8% of the population, while the next band with more relative weight is the population that is less than 5 min away and that gathers 14.5% of the population of the Sector, totaling 92.3% in the first 20 min. Next, the 30 min isochrone includes 6.7%, and, anecdotally, 1% of the population has a longer travel time than 30 min, including those in towns such as Deià or Fornalutx on the northern slope of the Serra de Tramuntana. In terms of tourist vacancies, 52% are concentrated in the 6–10 min isochrone, specifically in the nucleus of Las Maravillas, with 24,265 tourist vacancies, which together with S’Arenal (10,081 vacancies just over 11 min away) make up the tourist destination of Playa de Palma. Additionally, this extends to other nuclei adjacent to those mentioned, thus forming the main destination of the island. Subsequently, the number of places decreases as the access time increases, until it reaches the isochronous 40–45 min zone, where there are only six tourist places. Thus, in terms of potential population, 10.3% of the population, mostly residents, is less than 5 min from the hospital, while in the first 20 min from the hospital, 91.5% of the potential population is reached. At the other extreme, 1.9% of this population is more than 30 min away.
Thirdly, the Tramuntana Sector has some peculiar isochrones, while the region itself also has a population distribution different from the rest. The area of influence of the Hospital d’Inca has, roughly speaking, a first isochrone of 5 min that includes the nucleus of Inca. Then, in the transition between 6 and 7 min, there are up to four more nuclei, some of them with a relatively important regional weight such as Lloseta, or to a lesser extent Búger. Next, the isochrone of 11 to 20 min includes another eight nuclei slightly further away from the city of Inca, among which are Sa Pobla or Muro. Next, there is a relative vacuum of nuclei until the most peripheral ones appear with respect to the capital of the foothills of the island, which are found within the 21–30 min isochrone, and which are characterized by either being coastal nuclei (to the northwest) or nuclei with an important rural and inland component. In addition, the Sector includes the nucleus located in the “heart” of the Serra de Tramunatana, Escorca, as well as the two coastal nuclei of this municipality: la Calobra and Cala Tuent, which together make up 51 inhabitants and 111 tourist places, and which, because of the sinuosity of its road network and its peripheral location in the mountainous area of the island, are 42 and 52 min away, respectively, from the regional hospital of Inca. Finally, it is also worth mentioning Son Serra de Marina, which is located at the eastern end of the region, and has a population of 613 resident inhabitants and 939 tourist places.
If we compare the percentage of the population in each time interval (
Table 8), we can see the importance of the town of Inca, with a little more than 30,000 inhabitants, as the head of the region, since this town accounts for 26% of the population of the Sector, which represents 26.2% of the population living within 5 min from the hospital. Next, the Sector comprising the isochronous 6–10 min covers 13.2% of the population, including the nuclei of the surroundings of Inca as mentioned above. Next, the isochrone with the greatest relative weight is the 11–20 min isochrone, with 35.7% of the population being situated there, mainly due to the population weight of the towns of Sa Pobla (10.9%) and Muro (5.2%), or coastal enclaves such as Alcúdia (6%) and its beach (5.1%) in the northeast. Next, and below 30 min, 24.4% of the population is concentrated in urbanized areas, mainly coastal, in the municipality of Pollença (Pollença—6.2%; Port de Pollença—5.4%, as the two main ones) in the extreme northeast, as well as other coastal towns such as the port of Alcúdia (4.7%) or Ca’n Picafort (6.6%) in the center of the bay, developed from the tourist growth of the area. Thus, the tourist places show a great concentration in the isochrones between 11 and 30 min, encompassing 92.3% of the tourist places in the Sector, and emphasizing the area that includes the localities located between 21 and 30 min, where 62.2% of the places are located in coastal nuclei such as Platja de Muro, Port d’Alcúdia, Port de Pollença, or Ca’n Picafort, where, besides hotels, there is a great selection of houses for vacation rentals too. Thus, the potential population presents an increasing distribution as one moves away from the hospital of Inca until they reach the 30 min isochrone where 99.1% of the population is located. While in the first 5 min 14.8% are included, followed by 9.3% in the first 10 min, and 33.1% between 11 and 20 min, the main relative weight of the potential population is between 21 and 30 min with 41.9% weight.
Finally, the Llevant Sector (
Table 9) is the one that occupies the largest area, while at the same time it is the one with the most dispersed population centers in the territory, both inland and along the southwest coast of the island. In terms of accessibility, the Manacor Hospital shows an area of influence that in the first 5 min only covers the nucleus of Manacor itself, as well as two small population entities, Son Mas and Son Talent. Then, the isochrone of 6–10 min covers three nuclei, all of them inland and relatively close to the main nucleus. However, these first two areas of influence, unlike the previous Sectors, only reach 27.7% of the population. Thus, the greatest relative weight is found in the isochrone that includes the nuclei located between 11 and 20 min, with 32.4%, since this service area includes, in addition to several considerable inland nuclei such as Felanitx (7.3%) or Porreres (3.6%), a large number of coastal nuclei such as Portocristo (8.8%) or Cala Millor (3.8%). It also includes up to nine other nuclei that do not present large volumes of population, since they generally do not exceed 1%, although with some exceptions, but which together represent a high relative weight. Among these nuclei are Sa Coma, S’Illot, Cala Anguila or s’Estany de’n Mas, distributed among the municipalities of Manacor, Sant Llorenç, and Son Servera, and among which are some of the important tourist developments on the island. In the following interval, between 21 and 30 min, and with 21.7% of the population, there are, once again, a large number of coastal towns in the east, such as Cala Bona, Colònia de Sant Pere, Canyamel, Cales de Mallorca. There are also coastal towns in the southwest, such as Portocolom (3.2%), as well as other inland nuclei such as Campos, which houses 6.4% of the regional population, and also Felanitx (7.3%) in the south, and Artà (4.6%) and Capdepera (2.5%) in the east. Thus, it is so that in the isochrone between 21 and 30 min, 21.7% of the population is found. In the isochrone of 31 to 40 min, 16.2% of the population is included, and it is characterized by including the coastal nuclei of the municipality of Capdepera in the eastern end of the island, as well as a strip to the south where nuclei such as Santanyí (2.5%) or Cala d’Or (2.9%) are located. Finally, this is the Sector with the largest number of people more than 40 min away from the regional hospital, with 2790 people representing 2.1% of the Sector and being concentrated in Colònia de Sant Jordi to the west of the southern end of the island.
Next, if tourist sites are added, accessibility worsens, since in the first 10 min only 8.8% of the tourist sites are found, and it is not until reaching the 30 min mark that 60% of the sites are exceeded. This is due to the fact that 86.9% of the vacancies are located in the aforementioned coastal nuclei, which are between 11 and 40 min away. As far as the potential population is concerned, this trend of predominance of the intervals between 11 and 40 min is maintained, where 78.8% of the potential population is covered, and, in the first 10 min, barely 18% of the potential population is reached. At the other extreme, up to 27.7% of the potential population is more than 30 min away from the county hospital, and 3.2% is more than 50 min away.
4.3. Equity in Accessibility
As already mentioned, the Gini index and the Lorenz curve are two of the most widely used statistical techniques to evaluate equity or inequality in accessibility. In the present study, both are applied to the access time from each nucleus to the corresponding hospital, and this is carried out at both Sector and Health Area levels.
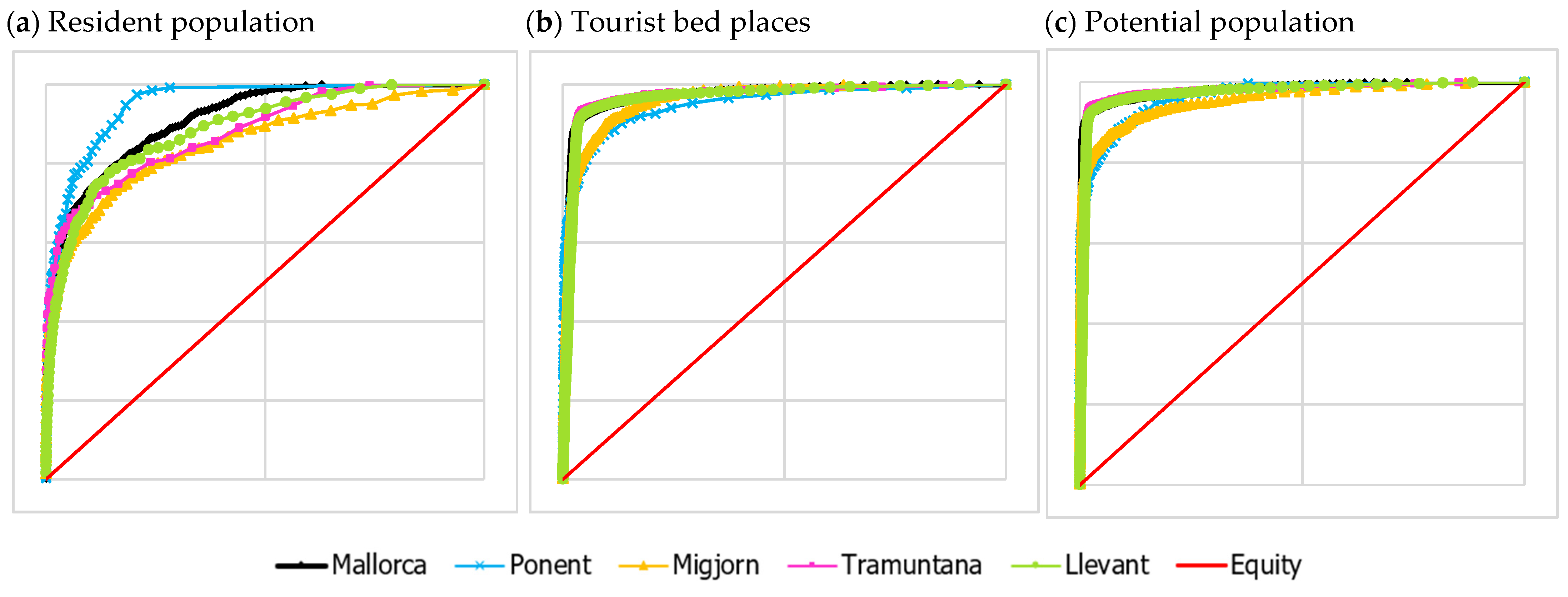
Figure 10 shows the Lorenz curves for each of the Sectors, together with the curve for the Health Area of Mallorca, and the line of perfect equity. In addition,
Table 3 shows the results of the calculation of the Gini index for each of the territorial units analyzed.
As can be seen in
Figure 10 and
Table 10, the degree of equity in the distribution of accessibility is quite similar, generally tending towards a very unequal distribution. However, there are notable differences between the resident population, tourists, and the aggregate of tourists and residents.
First, the resident population shows the least inequality, with the exception of the Ponent Sector (Gini = 0.9). This is due to a relatively dispersed distribution throughout the space covered by each Sector, with varying population figures among these nuclei, but always depending on the county seat, which is where the hospital is located and which concentrates a greater amount of the population; this causes this tendency to inequity, since a large amount of the population benefits from better accessibility. This is not the case in the Ponent Sector, as the nucleus of Palma concentrates a vast majority of the population in a short access time, which generates a positive inequity. In the case of the Health Area of Mallorca (Gini = 0.83), the high demographic weight of Palma and its surroundings together with the proximity to the reference hospital are the causes of this greater inequity with respect to the other Sectors with the exception of Ponent.
On the other hand, the distribution of tourist vacancies has an eminently coastal component, as we have already seen, which means an increase in travel time from the origin to the destination hospital, an effect that is exacerbated in the Tramuntana and Llevant Sectors, where the highest Gini values are found, 0.94 in both cases. This wide dispersion of tourist vacancies along the coast generates a greater effect of inequality in accessibility than in the previous case of the concentration of residents around the hospital, since, in this case, the main nuclei or groups of nuclei with the highest concentration of tourist vacancies are located at a similar distance from the hospital. On the other hand, in the Ponent and Migjorn Sectors, the proximity of tourist vacancies to hospitals is maintained, which generates Gini indices of 0.9 and 0.93, respectively.
In terms of the potential population, the Ponent and Migjorn Sectors show the lowest inequality due to the large number of towns in the metropolitan area of Palma with a high potential population, which are close to the corresponding county hospitals; even so, the values of the Gini index are very close to the total inequality (Ponent = 0.94 and Migjorn = 0.91). On the other hand, the Tramuntana and Llevant Sectors include the most rural areas of the island, for which the main centers of the county capitals barely exceed 30,000 inhabitants, since, in these two Sectors, inequality is higher (Tramuntana = 0.96 and Llevant = 0.95) due to the importance of the development of the coastal centers, concentrating a large amount of the potential population within a similar distance nucleus. Finally, the Gini index for the island of Mallorca is 0.96, the highest of the five records, since, in this case, the entire weight of the metropolitan area of Palma where more than half of the potential population of the island is located, and where there is good accessibility to the Son Espases hospital, causes this high concentration of accessibility in a large social majority.
Thus, it is understood that inequality is a positive characteristic in social accessibility to health centers, since a social majority benefits from better accessibility to these facilities. The location of the Son Espases Hospital in Palma aims to offer the closest possible service to the greatest possible volume of population. In this case, the inequality in accessibility is understood as a positive factor, skewed by the greater demographic weight, since the lowest access times are concentrated in a few densely populated nuclei, while the highest access times correspond to more nuclei but are of low demographic weight or contain isolated tourist establishments.

 ,
, 













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}