

Understanding Consumer Panic Buying Behaviors during the Strict Lockdown on Omicron Variant: A Risk Perception View
Abstract
:1. Introduction
2. Theoretical Background
2.1. Risk Perception and Its Dimensions: The Cognitive and Affective Scale
2.2. The PADM Theory
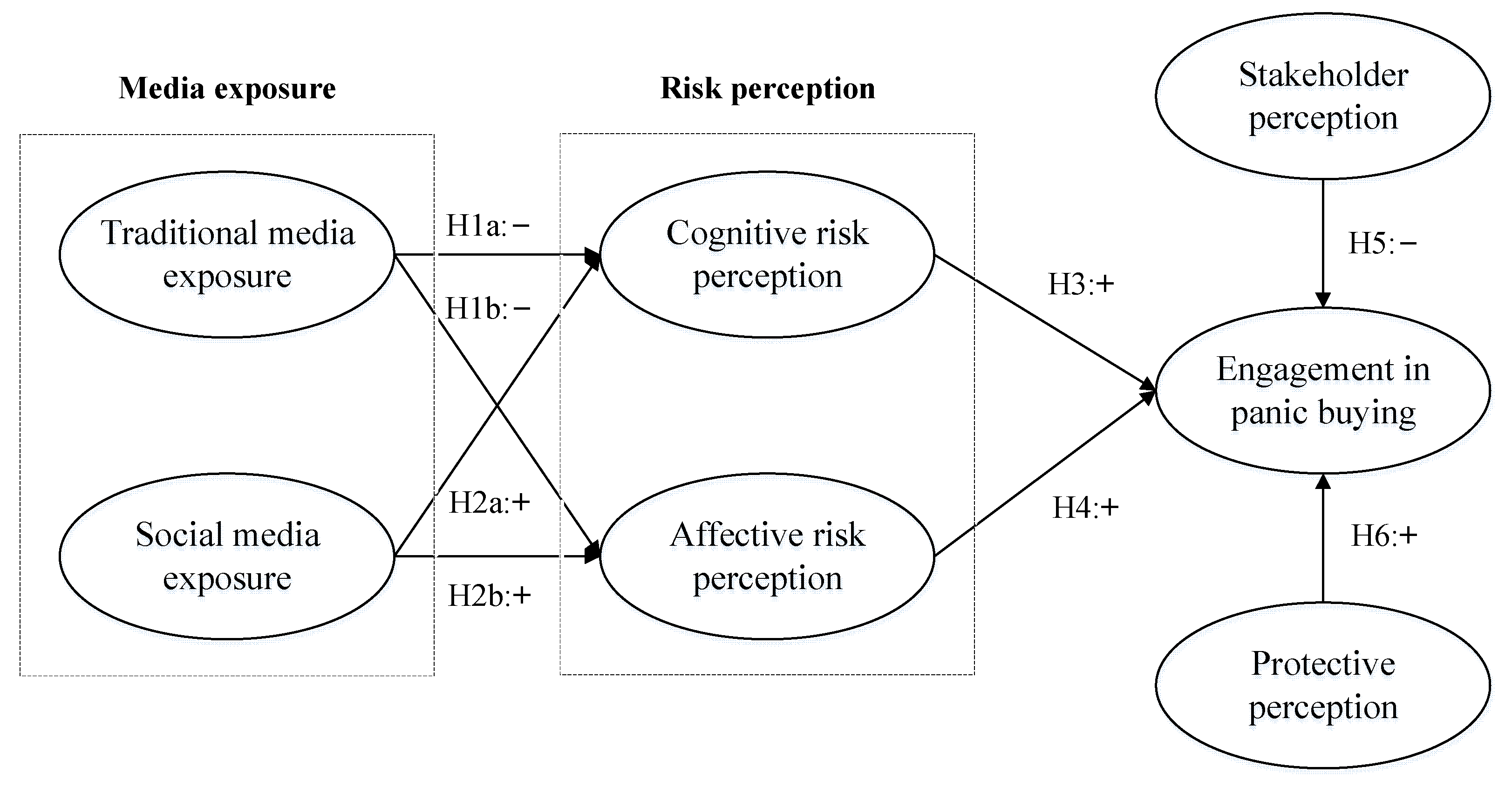
3. Hypotheses
3.1. Media Exposure and Risk Perception
3.2. Risk Perception and Panic Buying Behavior
3.3. Stakeholder Perception and Panic Buying
3.4. Protective Perception and Panic Buying
4. Data and Methods
4.1. Sample and Data Collection
4.2. Measures
5. Results
5.1. Reliability and Validity
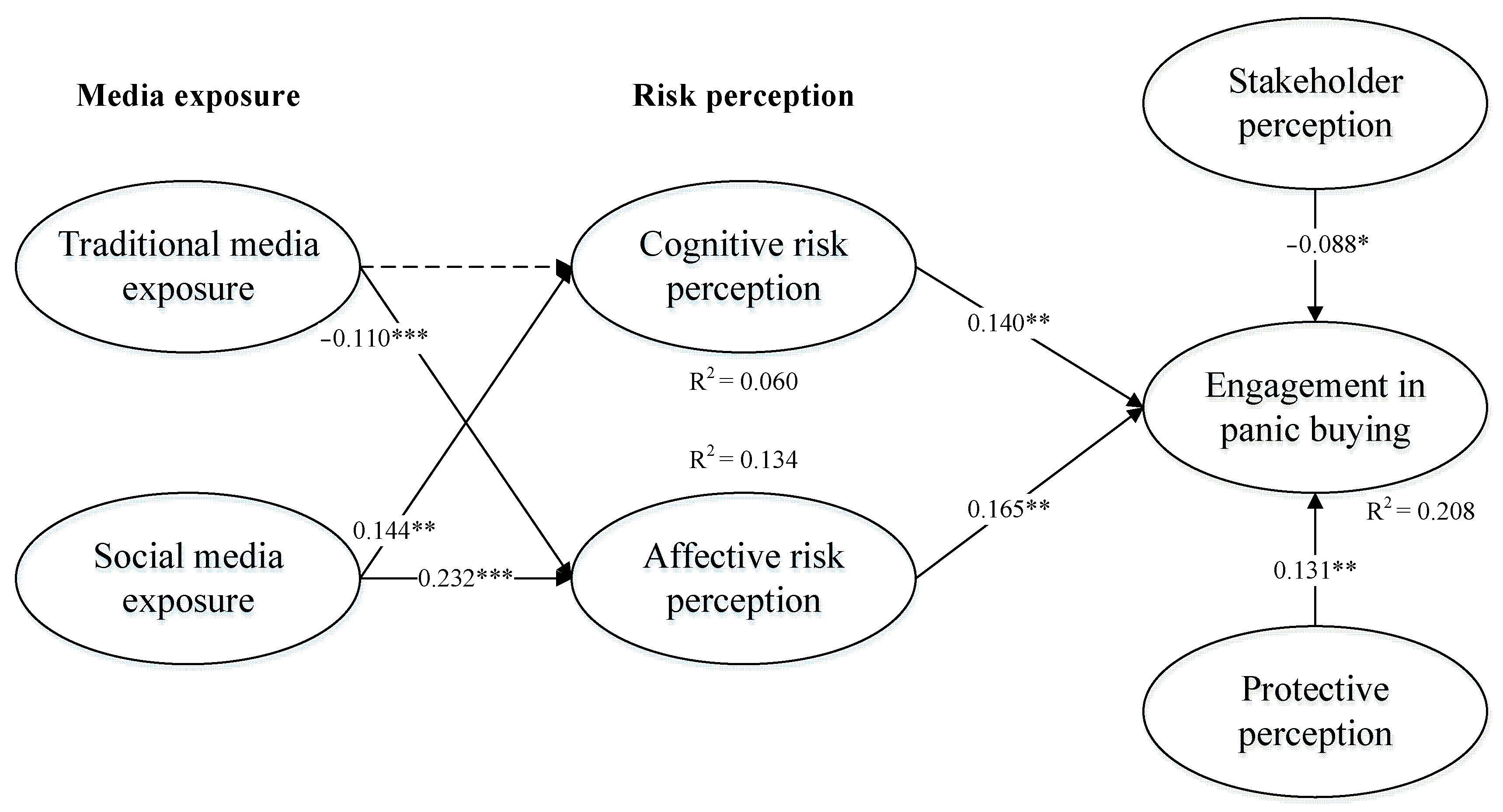
5.2. Hypotheses Testing
6. Discussion and Conclusions
6.1. Discussion
6.2. Contributions and Implications
7. Limitations and Research Prospect
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Measurement Items
References
- Grabowski, F.; Kochańczyk, M.; Lipniacki, T. The spread of SARS-CoV-2 variant Omicron with a doubling time of 2.0–3.3 days can be explained by immune evasion. Viruses 2022, 14, 294. [Google Scholar] [CrossRef] [PubMed]
- Mefsin, Y.; Chen, D.; Bond, H.S.; Lin, Y.; Cheung, J.K.; Wong, J.Y.; Ali, S.T.; Lau, E.H.Y.; Wu, P.; Leung, G.M.; et al. Epidemiology of infections with SARS-CoV-2 Omicron BA. 2 variant in Hong Kong, January–March 2022. Emerg. Infect. Dis. 2022, 28, 1856–1858. [Google Scholar] [CrossRef] [PubMed]
- People’s Daily Online. China’s Quest for New Ways to Handle Omicron. Available online: http://en.people.cn/n3/2022/0329/c90000-10077212.html (accessed on 7 May 2022).
- Yang, Q.C.; Yang, F.; Zhou, C. What health-related information flows through you every day? A content analysis of microblog messages on air pollution. Health Educ. 2015, 115, 438–454. [Google Scholar] [CrossRef]
- Islam, T.; Pitafi, A.H.; Arya, V.; Wang, Y.; Akhtar, N.; Mubarik, S.; Xiaobei, L. Panic buying in the COVID-19 pandemic: A multi-country examination. J. Retail. Consum. Serv. 2021, 59, 102357. [Google Scholar]
- Yuen, K.F.; Wang, X.; Ma, F.; Li, K.X. The Psychological Causes of Panic Buying Following a Health Crisis. Int. J. Environ. Res. Public Health 2020, 17, 3513. [Google Scholar] [CrossRef]
- Ding, H. Rhetorics of alternative media in an emerging epidemic: SARS, censorship, and extra-institutional risk communication. Tech. Commun. Q. 2009, 18, 327–350. [Google Scholar] [CrossRef]
- Leung, C.C.; Lam, T.H.; Cheng, K.K. Mass masking in the COVID-19 epidemic: People need guidance. Lancet 2020, 395, 945. [Google Scholar] [CrossRef]
- Omicron Makes Hong Kong’s ’COVID-Zero’ Unworkable. Available online: https://dailybrief.oxan.com/Analysis/DB267975/Omicron-makes-Hong-Kongs-COVID-zero-unworkable (accessed on 16 March 2022).
- Wesseler, J. Storage policies: Stockpiling versus immediate release. J. Agric. Food Ind. Organ. 2020, 18, 20190055. [Google Scholar] [CrossRef]
- Zheng, R.; Shou, B.; Yang, J. Supply disruption management under consumer panic buying and social learning effects. Omega 2020, 101, 102238. [Google Scholar] [CrossRef]
- Lindell, M.K.; Perry, R.W. Communicating Environmental Risk in Multiethnic Communities; Sage Publications: London, UK, 2003; Volume 7. [Google Scholar]
- Lindell, M.K.; Perry, R.W. The protective action decision model: Theoretical modifications and additional evidence. Risk Anal. Int. J. 2012, 32, 616–632. [Google Scholar] [CrossRef]
- Lindell, M.K.; Perry, R.W. Behavioral Foundations of Community Emergency Planning; Hemisphere Publishing Corp: Washington, DC, USA, 1992. [Google Scholar]
- Trumbo, C.W. Communicating the significance of risk. In Communication and Engagement with Science and Technology: Issues and Dilemmas; Gilbert, J.K., Stocklmayer, Routledge, S.M., Eds.; Taylor & Francis Group: New York, NY, USA, 2013. [Google Scholar]
- Birkholz, S.; Muro, M.; Jeffrey, P.; Smith, H.M. Rethinking the relationship between flood risk perception and flood management. Sci. Total Environ. 2014, 478, 12–20. [Google Scholar] [CrossRef]
- Brewer, N.T.; Chapman, G.B.; Gibbons, F.X.; Gerrard, M.; McCaul, K.D.; Weinstein, N.D. Meta-analysis of the relationship between risk perception and health behavior: The example of vaccination. Health Psychol. 2007, 26, 136. [Google Scholar] [CrossRef] [Green Version]
- Meyer, R.; Broad, K.; Orlove, B.; Petrovic, N. Dynamic simulation as an approach to understanding hurricane risk response: Insights from the Stormview lab. Risk Anal. 2013, 33, 1532–1552. [Google Scholar] [CrossRef]
- Terpstra, T.; Lindell, M.K. Citizens’ perceptions of flood hazard adjustments: An application of the protective action decision model. Environ. Behav. 2013, 45, 993–1018. [Google Scholar] [CrossRef] [Green Version]
- Gaube, S.; Lermer, E.; Fischer, P. The concept of risk perception in health-related behavior theory and behavior change. In Perceived Safety; Springer: Cham, Switzerland, 2019; pp. 101–118. [Google Scholar]
- Horney, J.A.; MacDonald, P.D.; Van Willigen, M.; Berke, P.R.; Kaufman, J.S. Individual actual or perceived property flood risk: Did it predict evacuation from Hurricane Isabel in North Carolina, 2003? Risk Anal. Int. J. 2010, 30, 501–511. [Google Scholar] [CrossRef]
- Loewenstein, G.F.; Weber, E.U.; Hsee, C.K.; Welch, N. Risk as feelings. Psychol. Bull. 2001, 127, 267. [Google Scholar] [CrossRef]
- Altarawneh, L.; Mackee, J.; Gajendran, T. The influence of cognitive and affective risk perceptions on flood preparedness intentions: A dual-process approach. Procedia Eng. 2018, 212, 1203–1210. [Google Scholar] [CrossRef]
- Slovic, P.; Finucane, M.L.; Peters, E.; MacGregor, D.G. Risk as analysis and risk as feelings: Some thoughts about affect, reason, risk, and rationality. Risk Anal. Int. J. 2004, 24, 311–322. [Google Scholar] [CrossRef]
- Van der Linden, S. On the relationship between personal experience, affect and risk perception: The case of climate change. Eur. J. Soc. Psychol. 2014, 44, 430–440. [Google Scholar] [CrossRef] [Green Version]
- Trumbo, C.W.; Peek, L.; Meyer, M.A.; Marlatt, H.L.; Gruntfest, E.; McNoldy, B.D.; Schubert, W.H. A cognitive-affective scale for hurricane risk perception. Risk Anal. 2016, 36, 2233–2246. [Google Scholar] [CrossRef]
- Epstein, S. Integration of the cognitive and the psychodynamic unconscious. Am. Psychol. 1994, 49, 709. [Google Scholar] [CrossRef]
- Nerb, J.; Spada, H. Evaluation of environmental problems: A coherence model of cognition and emotion. Cogn. Emot. 2001, 15, 521–551. [Google Scholar] [CrossRef]
- Trumbo, C.W. Influence of risk perception on attitudes and norms regarding electronic cigarettes. Risk Anal. 2018, 38, 906–916. [Google Scholar] [CrossRef] [PubMed]
- Becker, J.S.; Paton, D.; Johnston, D.M.; Ronan, K.R. Salient beliefs about earthquake hazards and household preparedness. Risk Anal. 2013, 33, 1710–1727. [Google Scholar] [CrossRef] [PubMed]
- Lazo, J.K.; Bostrom, A.; Morss, R.E.; Demuth, J.L.; Lazrus, H. Factors affecting hurricane evacuation intentions. Risk Anal. 2015, 35, 1837–1857. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Ouyang, Z.; Cheng, P. Predicting consumers’ adoption of electric vehicles during the city smog crisis: An application of the protective action decision model. J. Environ. Psychol. 2019, 64, 30–38. [Google Scholar] [CrossRef]
- Wei, J.; Zhao, M.; Wang, F.; Cheng, P.; Zhao, D. An empirical study of the Volkswagen crisis in China: Customers’ information processing and behavioral intentions. Risk Anal. 2016, 36, 114–129. [Google Scholar] [CrossRef]
- World Health Organization. Infection Prevention and Control during Health Care When Novel Coronavirus (nCoV) Infection is Suspected: Interim Guidance, 25 January 2020; World Health Organization: Geneva, Switzerland, 2020.
- Yang, H.; Nie, H.; Zhou, D.; Wang, Y.; Zuo, W. The effect of strict lockdown on Omicron SARS-CoV-2 variant transmission in Shanghai. Vaccines 2022, 10, 1392. [Google Scholar] [CrossRef]
- Wu, J.T.; Leung, K.; Leung, G.M. Nowcasting and forecasting the potential domestic and international spread of the 2019-nCoV outbreak originating in Wuhan, China: A modelling study. Lancet 2020, 395, 689–697. [Google Scholar] [CrossRef] [Green Version]
- Kasperson, R.E.; Renn, O.; Slovic, P.; Brown, H.S.; Emel, J.; Goble, R.; Ratick, S. The social amplification of risk: A conceptual framework. Risk Anal. 1988, 8, 177–187. [Google Scholar] [CrossRef] [Green Version]
- Vyncke, B.; Perko, T.; Van Gorp, B. Information sources as explanatory variables for the Belgian health-related risk perception of the Fukushima nuclear accident. Risk Anal. 2017, 37, 570–582. [Google Scholar] [CrossRef]
- Oh, S.H.; Lee, S.Y.; Han, C. The effects of social media use on preventive behaviors during infectious disease outbreaks: The mediating role of self-relevant emotions and public risk perception. Health Commun. 2021, 36, 972–981. [Google Scholar] [CrossRef]
- Fung, T.K.; Namkoong, K.; Brossard, D. Media, social proximity, and risk: A comparative analysis of newspaper coverage of avian flu in Hong Kong and in the United States. J. Health Commun. 2011, 16, 889–907. [Google Scholar] [CrossRef]
- Ng, Y.J.; Yang, Z.J.; Vishwanath, A. To fear or not to fear? Applying the social amplification of risk framework on two environmental health risks in Singapore. J. Risk Res. 2018, 21, 1487–1501. [Google Scholar] [CrossRef]
- Han, G.; Zhang, J.; Chu, K.; Shen, G. Self–other differences in H1N1 flu risk perception in a global context: A comparative study between the United States and China. Health Commun. 2014, 29, 109–123. [Google Scholar] [CrossRef]
- Niu, C.; Jiang, Z.; Liu, H.; Yang, K.; Song, X.; Li, Z. The influence of media consumption on public risk perception: A meta-analysis. J. Risk Res. 2022, 25, 21–47. [Google Scholar] [CrossRef]
- Koné, D.; Mullet, E. Societal risk perception and media coverage. Risk Anal. 1994, 14, 21–24. [Google Scholar] [CrossRef]
- Heilmann, S. (Ed.) China’s Political System; Rowman & Littlefield: Washington, DC, USA, 2016. [Google Scholar]
- Li, P.P.; Zhong, F. A Study on the Correlation Between Media Usage Frequency and Audiences’ Risk Perception, Emotion and Behavior. Front. Psychol. 2021, 12, 822300. [Google Scholar] [CrossRef]
- Chen, Y.; Ji, H.; Chen, L.J.; Jiang, R.; Wu, Y.N. Food safety knowledge, attitudes and behavior among dairy plant workers in Beijing, northern China. Int. J. Environ. Res. Public Health 2018, 15, 63. [Google Scholar] [CrossRef] [Green Version]
- Kolbitsch, J.; Maurer, H.A. The transformation of the Web: How emerging communities shape the information we consume. J. UCS 2006, 12, 187–213. [Google Scholar]
- Cheng, P.; Ouyang, Z.; Liu, Y. The effect of information overload on the intention of consumers to adopt electric vehicles. Transportation 2020, 47, 2067–2086. [Google Scholar] [CrossRef]
- Prentice, C.; Quach, S.; Thaichon, P. Antecedents and consequences of panic buying: The case of COVID-19. Int. J. Consum. Stud. 2022, 46, 132–146. [Google Scholar] [CrossRef]
- Scovell, M.; McShane, C.; Swinbourne, A.; Smith, D. Applying the Protective Action Decision Model to Explain Cyclone Shutter Installation Behavior. Nat. Hazards Rev. 2020, 22, 04020043. [Google Scholar] [CrossRef]
- Huang, S.K.; Lindell, M.K.; Prater, C.S. Multistage model of hurricane evacuation decision: Empirical study of Hurricanes Katrina and Rita. Nat. Hazards Rev. 2017, 18, 05016008. [Google Scholar] [CrossRef]
- Wachinger, G.; Renn, O.; Begg, C.; Kuhlicke, C. The risk perception paradox—Implications for governance and communication of natural hazards. Risk Anal. 2013, 33, 1049–1065. [Google Scholar] [CrossRef] [PubMed]
- Lindell, M.K.; Whitney, D.J. Correlates of household seismic hazard adjustment adoption. Risk Anal. 2000, 20, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.E.; Lemyre, L. A social-cognitive perspective of terrorism risk perception and individual response in Canada. Risk Anal. Int. J. 2009, 29, 1265–1280. [Google Scholar] [CrossRef]
- Miceli, R.; Sotgiu, I.; Settanni, M. Disaster preparedness and perception of flood risk: A study in an alpine valley in Italy. J. Environ. Psychol. 2008, 28, 164–173. [Google Scholar] [CrossRef]
- Terpstra, T. Emotions, trust, and perceived risk: Affective and cognitive routes to flood preparedness behavior. Risk Anal. Int. J. 2011, 31, 1658–1675. [Google Scholar] [CrossRef]
- Siegrist, M.; Gutscher, H. Flooding risks: A comparison of lay people’s perceptions and expert’s assessments in Switzerland. Risk Anal. 2006, 26, 971–979. [Google Scholar] [CrossRef]
- Wang, F.; Wei, J.; Shi, X. Compliance with recommended protective actions during an H7N9 emergency: A risk perception perspective. Disasters 2018, 42, 207–232. [Google Scholar] [CrossRef]
- Kruglanski, A.W.; Stroebe, W. The Influence of Beliefs and Goals on Attitudes: Issues of Structure, Function, and Dynamics. In The Handbook of Attitudes; Albarracin, D., Johnson, B.T., Zanna, M.P., Eds.; Erlbaum: Mahwah, NJ, USA, 2005; pp. 323–368. [Google Scholar]
- Demuth, J.L.; Morss, R.E.; Lazo, J.K.; Trumbo, C. The effects of past hurricane experiences on evacuation intentions through risk perception and efficacy beliefs: A mediation analysis. Weather Clim. Soc. 2016, 8, 327–344. [Google Scholar] [CrossRef]
- Ridgway, N.M.; Kukar-Kinney, M.; Monroe, K.B. An expanded conceptualization and a new measure of compulsive buying. J. Consum. Res. 2008, 35, 622–639. [Google Scholar] [CrossRef] [Green Version]
- Choi, D.H.; Yoo, W.; Noh, G.Y.; Park, K. The impact of social media on risk perceptions during the MERS outbreak in South Korea. Comput. Hum. Behav. 2017, 72, 422–431. [Google Scholar] [CrossRef]
- Haas, C. Coronavirus and risk analysis. Risk Anal. 2020, 40, 660. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | N | Percentage (%) | |
|---|---|---|---|
| Age | Less Than 21 | 67 | 13.0% |
| 21~30 | 177 | 34.2% | |
| 31~40 | 181 | 35.0% | |
| 41~50 | 61 | 11.8% | |
| More Than 50 | 31 | 6.0% | |
| Gender | Female | 252 | 48.7% |
| Male | 265 | 51.3% | |
| Income | Less Than ¥30,000 | 43 | 8.3% |
| ¥30,000–¥70,000 | 133 | 25.7% | |
| ¥70,000–¥120,000 | 143 | 27.7% | |
| ¥120,000–¥200,000 | 152 | 29.4% | |
| Over ¥200,000 | 46 | 8.9% | |
| Education | Less Than High School | 46 | 8.9% |
| High School | 124 | 24.0% | |
| Vocational School | 96 | 18.6% | |
| College Graduate | 183 | 35.4% | |
| Master or PhD | 68 | 13.2% | |
| Models | Constrained Model (Corr. = 1) | Unconstrained Model (Corr. = Free) | Chi-Square Difference (Δχ2) | ||
|---|---|---|---|---|---|
| χ2 | df | χ2 | df | ||
| TME-SME | 1459.279 | 612 | 1122.829 | 611 | 336.450 |
| TME-CP | 1229.607 | 612 | 1007.993 | 611 | 221.614 |
| TME-AP | 1501.533 | 612 | 1143.956 | 611 | 357.577 |
| TME-SP | 1113.771 | 612 | 950.075 | 611 | 163.696 |
| TME-PP | 1413.497 | 612 | 1099.938 | 611 | 313.559 |
| TME-EPB | 1464.987 | 612 | 1125.683 | 611 | 339.304 |
| SME-CP | 1212.283 | 612 | 999.331 | 611 | 212.952 |
| SME-AP | 1163.939 | 612 | 975.159 | 611 | 188.780 |
| SME-SP | 1399.405 | 612 | 1092.892 | 611 | 306.513 |
| SME-PP | 1150.808 | 612 | 968.593 | 611 | 182.215 |
| SME-EPB | 1115.217 | 612 | 950.798 | 611 | 164.419 |
| CP-SP | 1263.497 | 612 | 1024.938 | 611 | 238.559 |
| CP-AP | 1210.595 | 612 | 998.487 | 611 | 212.108 |
| CP-PP | 1174.967 | 612 | 980.673 | 611 | 194.294 |
| CP-EPB | 1160.509 | 612 | 973.444 | 611 | 187.065 |
| AP-SP | 1457.307 | 612 | 1121.843 | 611 | 335.464 |
| AP-PP | 1210.085 | 612 | 998.232 | 611 | 211.853 |
| AP-EPB | 1182.963 | 612 | 984.671 | 611 | 198.292 |
| SP-PP | 1382.491 | 612 | 1084.435 | 611 | 298.056 |
| SP-EPB | 1438.895 | 612 | 1112.637 | 611 | 326.258 |
| PP-EPB | 1189.873 | 612 | 988.126 | 611 | 201.747 |
| Variables | Means | S.D. | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Traditional media exposure | 3.053 | 1.069 | 0.892 | |||||||||
| 2. Social media exposure | 3.088 | 0.874 | −0.237 ** | 0.851 | ||||||||
| 3. Cognitive risk perception | 3.192 | 0.821 | −0.021 | 0.126 ** | 0.822 | |||||||
| 4. Affective risk perception | 3.044 | 0.825 | −0.216 ** | 0.294 ** | 0.215 ** | 0.822 | ||||||
| 5. Engagement in panic buying | 3.133 | 0.932 | 0.069 | −0.138 ** | −0.005 | −0.137 ** | 0.833 | |||||
| 6. Stakeholder perception | 2.992 | 0.834 | −0.145 ** | 0.302 ** | 0.253 ** | 0.302 ** | −0.063 | 0.899 | ||||
| 7. Protective perception | 3.064 | 3.064 | −0.222 ** | 0.303 ** | 0.222 ** | 0.299 ** | −0.164 ** | 0.278 ** | 0.832 | |||
| 8. Respondent age | 2.636 | 2.636 | 0.028 | −0.092 * | 0.044 | −0.027 | −0.023 | −0.054 | 0.047 | NA | ||
| 9. Respondent gender | 0.513 | 0.513 | 0.039 | −0.049 | −0.042 | −0.072 | 0.063 | −0.051 | −0.056 | 0.020 | NA | |
| 10. Respondent income | 3.048 | 3.048 | −0.077 | 0.049 | 0.176 ** | 0.021 | −0.093 * | 0.034 | 0.070 | 0.054 | −0.013 | NA |
| 11. Respondent education | 3.199 | 3.199 | 0.067 | 0.019 | 0.062 | −0.055 | 0.035 | −0.002 | −0.007 | 0.015 | −0.003 | 0.064 |
| Items | Factor Loading | S.E. | C.R. | p | Cronbach’s Alpha | Composite Reliability | AVE |
|---|---|---|---|---|---|---|---|
| TME1 | 0.892 | 0.043 | 24.092 | *** | 0.899 | 0.921 | 0.795 |
| TME2 | 0.894 | 0.041 | 23.820 | *** | |||
| TME3 | 0.888 | - | - | - | |||
| SME1 | 0.840 | 0.045 | 22.514 | *** | 0.929 | 0.929 | 0.725 |
| SME2 | 0.885 | 0.044 | 24.415 | *** | |||
| SME3 | 0.854 | 0.044 | 24.415 | *** | |||
| SME4 | 0.849 | 0.043 | 23.419 | *** | |||
| SME5 | 0.827 | - | - | - | |||
| CP1 | 0.843 | - | - | - | 0.893 | 0.913 | 0.676 |
| CP2 | 0.811 | 0.051 | 19.047 | *** | |||
| CP3 | 0.838 | 0.049 | 19.560 | *** | |||
| CP4 | 0.823 | 0.049 | 19.758 | *** | |||
| CP5 | 0.796 | 0.049 | 18.217 | *** | |||
| AP1 | 0.823 | 0.066 | 17.639 | *** | 0.922 | 0.925 | 0.675 |
| AP2 | 0.806 | 0.061 | 17.656 | *** | |||
| AP3 | 0.851 | 0.065 | 18.734 | *** | |||
| AP4 | 0.853 | 0.066 | 18.741 | *** | |||
| AP5 | 0.850 | 0.066 | 18.281 | *** | |||
| AP6 | 0.739 | - | - | - | |||
| SP1 | 0.902 | - | - | - | 0.893 | 0.927 | 0.808 |
| SP2 | 0.901 | 0.039 | 23.271 | *** | |||
| SP3 | 0.894 | 0.041 | 23.352 | *** | |||
| PP1 | 0.822 | 0.063 | 18.956 | *** | 0.929 | 0.931 | 0.693 |
| PP2 | 0.836 | 0.059 | 19.320 | *** | |||
| PP3 | 0.851 | 0.059 | 19.633 | *** | |||
| PP4 | 0.866 | 0.061 | 19.262 | *** | |||
| PP5 | 0.838 | 0.048 | 21.693 | *** | |||
| PP6 | 0.779 | - | - | - | |||
| EPB1 | 0.826 | - | - | - | 0.933 | 0.932 | 0.694 |
| EPB2 | 0.836 | 0.042 | 25.289 | *** | |||
| EPB3 | 0.851 | 0.048 | 22.027 | *** | |||
| EPB4 | 0.866 | 0.049 | 22.691 | *** | |||
| EPB5 | 0.838 | 0.049 | 21.101 | *** | |||
| EPB6 | 0.779 | 0.050 | 18.114 | *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, Y.; Ren, H.; Zhang, H. Understanding Consumer Panic Buying Behaviors during the Strict Lockdown on Omicron Variant: A Risk Perception View. Sustainability 2022, 14, 17019. https://doi.org/10.3390/su142417019
Yang Y, Ren H, Zhang H. Understanding Consumer Panic Buying Behaviors during the Strict Lockdown on Omicron Variant: A Risk Perception View. Sustainability. 2022; 14(24):17019. https://doi.org/10.3390/su142417019
Chicago/Turabian StyleYang, Yaodong, Huaqing Ren, and Han Zhang. 2022. "Understanding Consumer Panic Buying Behaviors during the Strict Lockdown on Omicron Variant: A Risk Perception View" Sustainability 14, no. 24: 17019. https://doi.org/10.3390/su142417019