

Impact of Exposure to Indoor Air Chemicals on Health and the Progression of Building-Related Symptoms: A Case Report
 ,
,  , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. The Patient and Home Environment
2.2. Indoor Air Sampling and Analysis
- The electronic piano was present in the living room with the children’s book.
- The electric piano was present in the living room without the children’s book and after 30 min of ventilation (i.e., opening the windows).
- The floor heating system was switched on, and the electronic piano was present in the living room without the children’s book.
- The electronic piano, clay toys, game cards, and children’s book were present in the living room, and the floor heating system was switched on.
- The air conditioner and humidifier were switched on, and the electronic piano was present in the living room without the clay toys, game cards, and children’s book.
- Staff lounge at the university.
- Outdoor air was sampled as a control.
- The patient’s office at the university.
- The electronic piano was kept inside the living room without the clay toys, game cards, and children’s book.
- The electronic piano was removed from the living room.
- The electronic piano was present in the living room along with the children’s book.
2.3. Analysis of Indoor Air and Emission Resource Test
2.4. Evaluation by Human Sensory Perception
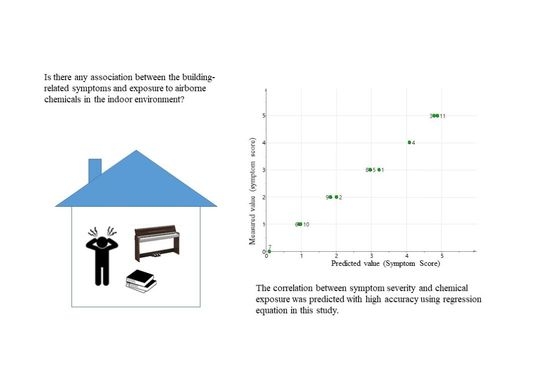
2.5. Statistical Analysis
2.6. Medical Research Ethics
3. Results
4. Discussion
- 1.
- 2014–2016
- 2.
- 2017–2018
- 3.
- 2019–2022 (Present)
- 4.
- Family members
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hu, J.; He, Y.; Hao, X.; Li, N.; Su, Y.; Qu, H. Optimal temperature ranges considering gender differences in thermal comfort, work performance, and sick building syndrome: A winter field study in university classrooms. Energy Build. 2022, 254, 111554. [Google Scholar] [CrossRef]
- WHO. Indoor Air Pollutants: Exposure and Health Effects. EURO Rep. Stud. 1983, 78, 1. [Google Scholar]
- Wang, B.L.; Takigawa, T.; Yamasaki, Y.; Sakano, N.; Wang, D.H.; Ogino, K. Symptom definitions for SBS (sick building syndrome) in residential dwellings. Int. J. Hyg. Environ. Health 2008, 211, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Jafari, M.J.; Khajevandi, A.A.; Mousavi Najarkola, S.A.; Yekaninejad, M.S.; Pourhoseingholi, M.A.; Omidi, L.; Kalantary, S. Association of sick building syndrome with indoor air parameters. Tanaffos 2015, 14, 55–62. [Google Scholar] [PubMed]
- Murphy, M. Sick Building Syndrome and the Problem of Uncertainty. Available online: https://www.dukeupress.edu/sick-building-syndrome-and-the-problem-of-uncertainty (accessed on 25 July 2022).
- Mentese, S.; Mirici, N.A.; Elbir, T.; Palaz, E.; Mumcuoğlu, D.T.; Cotuker, O.; Bakar, C.; Oymak, S.; Otkun, M.T. A long-term multi-parametric monitoring study: Indoor air quality (IAQ) and the sources of the pollutants, prevalence of sick building syndrome (SBS) symptoms, and respiratory health indicators. Atmos. Pollut. Res. 2020, 11, 2270–2281. [Google Scholar] [CrossRef]
- Runeson-Broberg, R.; Norbäck, D. Sick building syndrome (SBS) and sick house syndrome (SHS) in relation to psychosocial stress at work in the Swedish workforce. Int. Arch. Occup. Environ. Health 2013, 86, 915–922. [Google Scholar] [CrossRef]
- Imai, N.; Imai, Y. Psychosocial Factors that Aggravate the Symptoms of Sick Building Syndrome and a Cure for Them. In Sick Building Syndrome; Springer: Berlin/Heidelberg, Germany, 2011; pp. 105–111. [Google Scholar]
- Kim, J.; Jang, M.; Choi, K.; Kim, K. Perception of indoor air quality (IAQ) by workers in underground shopping centers in relation to sick-building syndrome (SBS) and store type: A cross-sectional study in Korea. BMC Public Health 2019, 19, 632. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, N.; Nakaoka, H.; Nakayama, Y.; Tsumura, K.; Takaguchi, K.; Takaya, K.; Eguchi, A.; Hanazato, M.; Todaka, E.; Mori, C. Association between sum of volatile organic compounds and occurrence of building-related symptoms in humans: A study in real full-scale laboratory houses. Sci. Total Environ. 2021, 750, 141635. [Google Scholar] [CrossRef]
- Nakaoka, H.; Todaka, E.; Seto, H.; Saito, I.; Hanazato, M.; Watanabe, M.; Mori, C. Correlating the symptoms of sick-building syndrome to indoor VOCs concentration levels and odour. Indoor Built Environ. 2014, 23, 804–813. [Google Scholar] [CrossRef]
- Araki, A.; Kawai, T.; Eitaki, Y.; Kanazawa, A.; Morimoto, K.; Nakayama, K.; Shibata, E.; Tanaka, M.; Takigawa, T.; Yoshimura, T.; et al. Relationship between selected indoor volatile organic compounds, so-called microbial VOC, and the prevalence of mucous membrane symptoms in single family homes. Sci. Total Environ. 2010, 408, 2208–2215. [Google Scholar] [CrossRef] [Green Version]
- Sahlberg, B.; Gunnbjörnsdottir, M.; Soon, A.; Jogi, R.; Gislason, T.; Wieslander, G.; Janson, C.; Norback, D. Airborne molds and bacteria, microbial volatile organic compounds (MVOC), plasticizers and formaldehyde in dwellings in three north European cities in relation to sick building syndrome (SBS). Sci. Total Environ. 2013, 444, 430–440. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.Y.; Tsai, M.C.; Muo, C.H.; Kuo, Y.H.; Sung, F.C.; Wu, C.C. Personal, psychosocial and environmental factors related to sick building syndrome in official employees of Taiwan. Int. J. Environ. Res. Public Health 2017, 15, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Runeson-Broberg, R. Sick Building Syndrome (SBS), Personality, Psychosocial Factors and Treatment; Springer: Singapore, 2020; pp. 283–302. [Google Scholar]
- Suzuki, N.; Nakayama, Y.; Nakaoka, H.; Takaguchi, K.; Tsumura, K.; Hanazato, M.; Hayashi, T.; Mori, C. Risk factors for the onset of sick building syndrome: A cross-sectional survey of housing and health in Japan. Build. Environ. 2021, 202, 107976. [Google Scholar] [CrossRef]
- Ghaffarianhoseini, A.; AlWaer, H.; Omrany, H.; Ghaffarianhoseini, A.; Alalouch, C.; Clements-Croome, D.; Tookey, J. Sick building syndrome: Are we doing enough? Archit. Sci. Rev. 2018, 61, 99–121. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Li, B.; Yang, Q.; Yu, W.; Wang, H.; Norback, D.; Sundell, J. Odors and sensations of humidity and dryness in relation to sick building syndrome and home environment in Chongqing, China. PLoS ONE 2013, 8, 72385. [Google Scholar] [CrossRef]
- Claeson, A.S.; Lidén, E.; Nordin, M.; Nordin, S. The role of perceived pollution and health risk perception in annoyance and health symptoms: A population-based study of odorous air pollution. Int. Arch. Occup. Environ. Health 2013, 86, 367–374. [Google Scholar] [CrossRef]
- 2020 Global Status Report for Buildings and Construction: Towards a Zero-emissions, Efficient and Resilient Buildings and Construction Sector—Executive Summary. Available online: https://wedocs.unep.org/handle/20.500.11822/34572;jsessionid=923C31364EAF7F4B094170F140934C27 (accessed on 25 July 2022).
- Röck, M.; Saade, M.R.M.; Balouktsi, M.; Rasmussen, F.N.; Birgisdottir, H.; Frischknecht, R.; Habert, G.; Lützkendorf, T.; Passer, A. Embodied GHG emissions of buildings—The hidden challenge for effective climate change mitigation. Appl. Energy 2020, 258, 114107. [Google Scholar] [CrossRef]
- Hoisington, A.J.; Stearns-Yoder, K.A.; Schuldt, S.J.; Beemer, C.J.; Maestre, J.P.; Kinney, K.A.; Postolache, T.T.; Lowry, C.A.; Brenner, L.A. Ten questions concerning the built environment and mental health. Build. Environ. 2019, 155, 58–69. [Google Scholar] [CrossRef]
- Aftab, W.; Siddiqui, F.J.; Tasic, H.; Perveen, S.; Siddiqi, S.; Bhutta, Z.A. Implementation of health and health-related sustainable development goals: Progress, challenges and opportunities—A systematic literature review. BMJ Glob. Health 2020, 5, e002273. [Google Scholar] [CrossRef]
- Miller, C.S.; Prihoda, T.J. The environmental exposure and sensitivity inventory (EESI): A standardized approach for measuring chemical intolerances for research and clinical applications. Toxicol. Ind. Health 1999, 15, 370–385. [Google Scholar] [CrossRef]
- Miller, C.S.; Prihoda, T.J. A controlled comparison of symptoms and chemical intolerances reported by Gulf War veterans, implant recipients and persons with multiple chemical sensitivity. Toxicol. Ind. Health 1999, 15, 386–397. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, L.; Byrne, T.; Johansson, E.; Trygg, J.; Vikström, C. Multi- and Megavariate Data Analysis Basic Principles and Applications. Available online: https://books.google.co.jp/books/about/Multi_and_Megavariate_Data_Analysis_Basi.html?id=58qLBQAAQBAJ&redir_esc=y (accessed on 25 July 2022).
- Japanese Ministry of Health, Labour, and Welfare. Air Quality Guidelines 2019. Available online: http://www.nihs.go.jp/mhlw/chemical/situnai/hyou.html (accessed on 25 July 2022).
- Hojo, S.; Ishikawa, S.; Kumano, H.; Miyata, M.; Sakabe, K. Clinical characteristics of physician-diagnosed patients with multiple chemical sensitivity in Japan. Int. J. Hyg. Environ. Health 2008, 211, 682–689. [Google Scholar] [CrossRef] [PubMed]
- Hojo, S.; Sakabe, K.; Ishikawa, S.; Miyata, M.; Kumano, H. Evaluation of subjective symptoms of Japanese patients with multiple chemical sensitivity using QEESI. Environ. Health Prev. Med. 2009, 14, 267–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azuma, K.; Ikeda, K.; Kagi, N.; Yanagi, U.; Osawa, H. Evaluating prevalence and risk factors of building-related symptoms among office workers: Seasonal characteristics of symptoms and psychosocial and physical environmental factors. Environ. Health Prev. Med. 2017, 22, 38. [Google Scholar] [CrossRef] [Green Version]
- Edvardsson, B.; Stenberg, B.; Bergdahl, J.; Eriksson, N.; Lindén, G.; Widman, L. Medical and social prognoses of non-specific building-related symptoms (Sick Building Syndrome): A follow-up study of patients previously referred to hospital. Int. Arch. Occup. Environ. Health 2008, 81, 805–812. [Google Scholar] [CrossRef]
- Kipen, H.M.; Fiedler, N. Environmental factors in medically unexplained symptoms and related syndromes: The evidence and the challenge. Environ. Health Perspect. 2002, 110 (Suppl. 4), 597–599. [Google Scholar] [CrossRef] [Green Version]
- Veenaas, C.; Ripszam, M.; Glas, B.; Liljelind, I.; Claeson, A.S.; Haglund, P. Differences in chemical composition of indoor air in rooms associated/not associated with building related symptoms. Sci. Total Environ. 2020, 720, 137444. [Google Scholar] [CrossRef]
- Shahzad, S.S.; Brennan, J.; Theodossopoulos, D.; Hughes, B.; Calautit, J.K.; Bergman, M.M. Building-related symptoms, energy, and thermal control in the workplace: Personal and open plan offices. Sustainability 2016, 8, 331. [Google Scholar] [CrossRef] [Green Version]
- Mečiarová, Ľ.; Vilčeková, S.; Krídlová Burdová, E.; Kapalo, P.; Mihaľová, N. The real and subjective indoor environmental quality in schools. Int. J. Environ. Health Res. 2018, 28, 102–123. [Google Scholar] [CrossRef]
- Magnavita, N. Work-related symptoms in indoor environments: A puzzling problem for the occupational physician. Int. Arch. Occup. Environ. Health 2015, 88, 185–196. [Google Scholar] [CrossRef]
- Savelieva, K.; Elovainio, M.; Lampi, J.; Ung-Lanki, S.; Pekkanen, J. Psychosocial factors and indoor environmental quality in respiratory symptom reports of pupils: A cross-sectional study in Finnish schools. BMJ Open 2020, 10, e036873. [Google Scholar] [CrossRef] [PubMed]
- Finell, E.; Tolvanen, A.; Pekkanen, J.; Minkkinen, J.; Ståhl, T.; Rimpelä, A. Psychosocial problems, indoor air-related symptoms, and perceived indoor air quality among students in schools without indoor air problems: A longitudinal study. Int. J. Environ. Res. Public Health 2018, 15, 1497. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, Å.M.; Meyer, H.W.; Gyntelberg, F. Building-related symptoms and stress indicators. Indoor Air 2008, 18, 440–446. [Google Scholar] [CrossRef]
- Norbäck, D. An update on sick building syndrome. Curr. Opin. Allergy Clin. Immunol. 2009, 9, 55–59. [Google Scholar] [CrossRef]
- Wolkoff, P.; Wilkins, C.K.; Clausen, P.A.; Nielsen, G.D. Organic compounds in office environments—Sensory irritation, odor, measurements and the role of reactive chemistry. Indoor Air 2006, 16, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Wolkoff, P. Indoor air humidity, air quality, and health—An overview. Int. J. Hyg. Environ. Health 2018, 221, 376–390. [Google Scholar] [CrossRef]
- Wolkoff, P.; Nielsen, G.D. Effects by inhalation of abundant fragrances in indoor air—An overview. Environ. Int. 2017, 101, 96–107. [Google Scholar] [CrossRef]
- Nitmetawong, T.; Boonvisut, S.; Kallawicha, K.; Chao, H.J. Effect of indoor environmental quality on building-related symptoms among the residents of apartment-type buildings in Bangkok area. Hum. Ecol. Risk Assess. An Int. J. 2020, 26, 2663–2677. [Google Scholar] [CrossRef]
- Sun, Y.; Hou, J.; Cheng, R.; Sheng, Y.; Zhang, X.; Sundell, J. Indoor air quality, ventilation and their associations with sick building syndrome in Chinese homes. Energy Build. 2019, 197, 112–119. [Google Scholar] [CrossRef]
- Nagata, Y. Measurement of Odor Threshold by Triangle Odor Bag Method. Odor Meas. Rev. 2003, 118, 118–127. [Google Scholar]
- Rosenkranz, H.S.; Cunningham, A.R. Environmental odors and health hazards. Sci. Total Environ. 2003, 313, 15–24. [Google Scholar] [CrossRef]
- Barmark, M. Social determinants of the sick building syndrome: Exploring the interrelated effects of social position and psychosocial situation. Int. J. Environ. Health Res. 2015, 25, 490–507. [Google Scholar] [CrossRef] [PubMed]
- Miškulin, M.; Matić, M.; Beneš, M.; Vlahović, J. The significance of psychosocial factors of the working environment in the development of sick building syndrome. J. Health Sci. 2014, 4, 136–142. [Google Scholar] [CrossRef] [Green Version]
- Take Action for the Sustainable Development Goals-United Nations Sustainable Development. Available online: https://www.un.org/sustainabledevelopment/sustainable-development-goals/ (accessed on 25 July 2022).
- González-Martín, J.; Kraakman, N.J.R.; Pérez, C.; Lebrero, R.; Muñoz, R. A state–of–the-art review on indoor air pollution and strategies for indoor air pollution control. Chemosphere 2021, 262, 128376. [Google Scholar] [CrossRef]
- Sun, C.; Zhai, Z. The efficacy of social distance and ventilation effectiveness in preventing COVID-19 transmission. Sustain. Cities Soc. 2020, 62, 102390. [Google Scholar] [CrossRef]
- World Health Organization. Roadmap to Improve and Ensure Good Indoor Ventilation in the Context of COVID-19; World Health Organization: Geneve, Switzerland, 2021; ISBN 9789240021280. [Google Scholar]
- Elsaid, A.M.; Ahmed, M.S. Indoor air quality strategies for air-conditioning and ventilation systems with the spread of the global coronavirus (COVID-19) epidemic: Improvements and recommendations. Environ. Res. 2021, 199, 111314. [Google Scholar] [CrossRef]
- Morawska, L.; Allen, J.; Bahnfleth, W.; Bluyssen, P.M.; Boerstra, A.; Buonanno, G.; Cao, J.; Dancer, S.J.; Floto, A.; Franchimon, F.; et al. A paradigm shift to combat indoor respiratory infection. Science 2021, 372, 689–691. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID | Situation | Y/M/D | ΣVOCs μg/m3 | Temperature °C | Humidity % | Symptoms Description | Symptom Score | Odour Score |
|---|---|---|---|---|---|---|---|---|
| 1 | LR * with EP **, a book for children | 2014.11.18 | 457 | 21.5 | 51.1 | Shoulder pain, Ear pain, Joint pain Tolerable for 30 min | 3 | 0 |
| 2 | LR with EP after 30 min of ventilation | 2014.11.18 | 301 | 20.9 | 39.3 | Tolerable for 30 min | 2 | 0 |
| 3 | LR with EP, floor heating system on | 2014.11.18 | 594 | 24.3 | 45.4 | Shoulder pain, Heavy headed, Nausea, Cognitive decline, Intolerable | 5 | 0 |
| 4 | LR with EP, clay toys, game cards, a book and floor heating system on | 2014.11.18 | 554 | 23.6 | 43.7 | Heavy headed, Intolerable longer than 5 min | 4 | 0 |
| 5 | LR with EP, air conditioner, humidifier on | 2014.11.26 | 517 | 25.4 | 64.3 | Shoulder pain, Eye pain, Cognitive decline | 3 | 0 |
| 6 | Staff lounge of the university | 2014.12.02 | 236 | 22.6 | 50.5 | Few symptoms | 1 | 0 |
| 7 | Outdoor air | 2014.12.19 | 47 | 6.4 | 39.2 | No symptoms | 0 | 0 |
| 8 | Office of the university | 2014.12.19 | 119 | 15.6 | 31.0 | Shoulder pain, Strong sleepiness | 3 | 0 |
| 9 | LR with EP | 2015.02.27 | 633 | 19.6 | 48.5 | Slight shoulder pain, Eye pain, Tolerable | 2 | 0 |
| 10 | LR without EP | 2015.03.03 | 388 | 19.7 | 41.7 | Few symptoms | 1 | 0 |
| 11 | LR with EP and a book | 2015.10.05 | 622 | 26.7 | 55.7 | Shoulder pain, Heavy headed, Cognitive decline, Nausea, Eye pain, Intolerable | 5 | 0 |
| VOC (µg/m3) | Guideline Values | S1 | S2 | S3 | S4 | S5 | S6 | S7 | S8 | S9 | S10 | S11 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Tetradecane | 330 | 1.1 | ND | 1.1 | 1.2 | 1.4 | 1.6 | ND | ND | 1.2 | 1.3 | 2.3 |
| Ethylbenzene | 3800 | 2.7 | 6.2 | 1.4 | 1.4 | 1.4 | 1.8 | ND | 2.9 | 3.2 | 1.2 | 2.6 |
| Styrene | 220 | ND | ND | ND | ND | 1.1 | ND | ND | ND | 8.7 | 1.1 | 1.4 |
| Toluene | 260 | 11 | 31 | 5.3 | 5.3 | 8.6 | 3.1 | 3.7 | 4.6 | 11 | 7.3 | 6.2 |
| Xylene | 870 | 2.3 | 4.9 | 1.7 | 1.6 | 1.5 | 5.2 | ND | 8.7 | 2.1 | 1.3 | 2.2 |
| p-Dichlorobenzene | 240 | ND | ND | ND | ND | ND | 2.1 | ND | ND | ND | ND | ND |
| Formaldehyde | 100 | 43 | 20 | 40 | 44 | 74 | 29 | 2.7 | 7.2 | 39 | 31 | 41.0 |
| Acetaldehyde | 48 | 14 | 9.4 | 14 | 23 | 21 | 16 | 1.5 | 3.5 | 30 | 13 | 6.5 |
| Di-2-ethylhexyl phthalate DEHP | 120 | 0.1 | - | - | - | - | 0.2 | ND | 0.3 | - | - | - |
| Dibutyl phthalate | 220 | 0.2 | - | - | - | - | 0.7 | 0.2 | 0.6 | - | - | - |
| Diazinon | 0.29 | ND | - | - | - | - | ND | ND | ND | - | - | - |
| Chlorpyrifos | 1 | ND | - | - | - | - | ND | ND | ND | - | - | - |
| Fenobcarb | 33 | ND | - | - | - | - | ND | ND | ND | - | - | - |
| TVOC | 400 | 370 | 220 | 520 | 460 | 390 | 100 | 37 | 69 | 550 | 330 | 530 |
| Compounds | Indoor Air | Surface of Interior Materials | |||
|---|---|---|---|---|---|
| Ceiling | Wall | Floor | Electronic Piano | ||
| Isododecane | 151.4 | 95.8 | 119.6 | 33.5 | 141.5 |
| 2-Ethyl-1-hexanol | 141.1 | 74.8 | 69.9 | 80.9 | 212.5 |
| Limonene | 74.9 | 27.4 | 20.3 | 15.3 | 19.7 |
| Toluene | 59.7 | 62.4 | 40.3 | 40.7 | 409.3 |
| D5 | 22.6 | 18.3 | 16.4 | 15.1 | 13.7 |
| Formaldehyde | 16.2 | 4.4 | 6.0 | 1.7 | 3.7 |
| Acetaldehyde | 2.6 | 1.3 | 2.2 | 1.1 | 2.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakaoka, H.; Suzuki, N.; Eguchi, A.; Matsuzawa, D.; Mori, C. Impact of Exposure to Indoor Air Chemicals on Health and the Progression of Building-Related Symptoms: A Case Report. Sustainability 2022, 14, 14421. https://doi.org/10.3390/su142114421
Nakaoka H, Suzuki N, Eguchi A, Matsuzawa D, Mori C. Impact of Exposure to Indoor Air Chemicals on Health and the Progression of Building-Related Symptoms: A Case Report. Sustainability. 2022; 14(21):14421. https://doi.org/10.3390/su142114421
Chicago/Turabian StyleNakaoka, Hiroko, Norimichi Suzuki, Akifumi Eguchi, Daisuke Matsuzawa, and Chisato Mori. 2022. "Impact of Exposure to Indoor Air Chemicals on Health and the Progression of Building-Related Symptoms: A Case Report" Sustainability 14, no. 21: 14421. https://doi.org/10.3390/su142114421