
The 4R Model of Mood and Emotion for Sustainable Mental Health in Organisational Settings


Abstract
:1. Introduction
1.1. Sustainable Mental Health in Organisations
1.2. Mood and Emotion
1.3. Mood and Emotion in Organisations
- To our knowledge, no models exist that facilitate the systematic application of theory relating to mood and emotion in organisational contexts.
1.4. Method
- We searched the peer-reviewed literature in psychology, neuroscience, and evolutionary biology for data or theory relating to distinctions between mood and emotion. In doing so, while being aware of the relative paucity of clear distinctions, especially in the neuroscience literature, we were guided by criteria proposed in previous review papers in cognitive psychology [11,48]. For example, when an idea such as background emotion was proposed by an author [49], and when this idea appeared to meet the structural and functional criteria proposed for mood in previous cognitive psychology reviews but was also associated with a novel perspective—a neurobiological role in homeostasis—we noted that proposal and sought further triangulation.
- We further developed this synthesis into an evidence-based and coherent model aimed at enhancing mental health and mental performance in organisations This builds on previous applied research by the authors of this paper [26,52,53,54,55], other research in emotion and mood regulation [56,57,58,59,60], and anecdotal experience emerging from the professional practice of the authors. This framework is characterised by differentiated strategies for moods and emotions, which represents a novel contribution to the affect regulation literature and to mental health practice in organisations.
- We developed brief guidelines for the application of the model in organisations.
2. Underpinning Theory
2.1. Moods and Emotions from a Top-Down (Cognitive) Perspective
2.2. Moods and Emotions from a Bottom-Up (Biological) Perspective
2.2.1. Mood and Homeostasis
2.2.2. Emotion and Homeostasis
- Increased metabolic resources such as oxygen and blood sugar availability [112].
- Modification of resource allocation such as increased blood flow to muscles and reduced blood flow to the viscera [113]
- Modification of regulatory processes in anticipation of homeostatic challenges such as increased sweat production and increased threshold for pain sensation [114].
- Increased mechanical potential for initiating and maintaining movement, such as increased motor cortex activity, motor unit recruitment, and reduced neural inhibition [115].
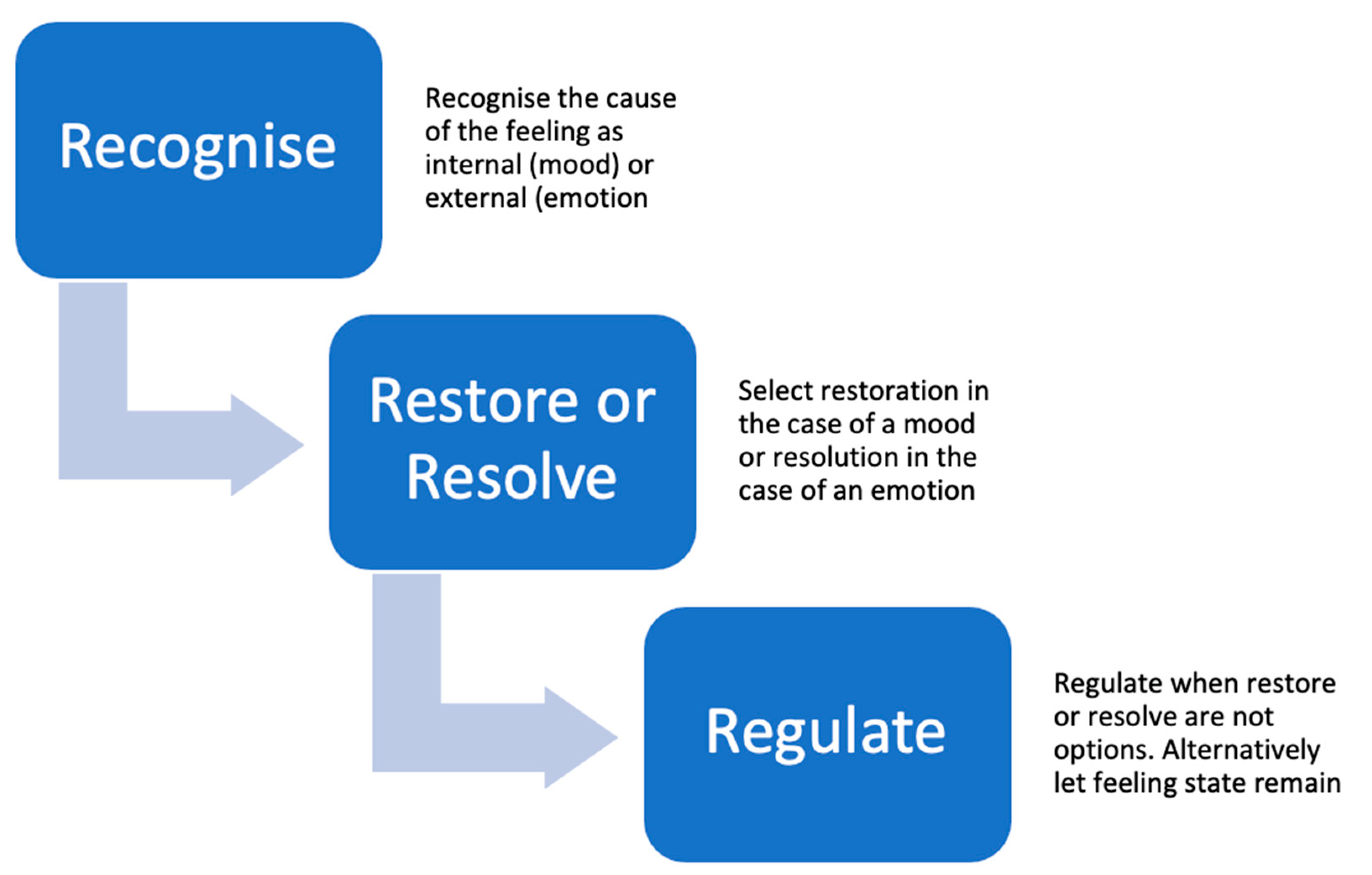
3. The 4R Model of Differentiated Mood and Emotion in Organisations
3.1. Stage 1: Recognition of the Cause of a Mood or Emotion
- Interoceptively: “Am I feeling something?”
- Perceptually: “What exactly am I feeling?”
- Contextually: “What might be the cause of the feeling?”
3.2. Stage 2: Restoration of Mood
- Reducing energy expenditure by resting to allow homeostasis to be restored without the challenge of providing energy for movement, removing metabolic waste, or regulating temperature (note the link between the words rest and restore) [128].
- Eating to restore energy, maintain nutrient balance, and maintain metabolic and anabolic processes (a distinction must be made between homeostatic and hedonistic eating in this context [129]; the former restores mood via the restoration of homeostasis, the latter by directly modifying emotional responses via several neurotransmitter systems) [130].
- Exercising and physical activity (note that physical activity refers to any type of voluntary movement), which may have direct effects on homeostasis by raising body temperature, increasing blood flow, and modifying blood glucose levels, as well as direct effects on brain biochemistry such as increased brain-derived neurotrophic factor (BDNF) levels [134] and opioid neurotransmission [135] that might have acute effects such as pain reduction [136] and chronic effects such as the maintenance of neural connectivity and plasticity [137].
- Exposure to physical environmental factors such as natural light, which over and above has direct effects on energy homeostasis [138] and chronobiology [139] and also triggers neurotransmitter systems such as serotonin [140] that might reduce anxiety and promote melatonin production, thereby enhancing subsequent sleep quality. Even exposure to natural sounds and scents can be restorative [141].
3.3. Stage 3: Resolution of the Cause of an Emotion
3.4. Stage 4: Regulation of the Mood or Emotion
3.5. Why Restoration and Resolution Are Preferable to Regulation
- Largely helpful, such as exercise, socialisation, spending time in natural environments, and enjoying entertainment such as film and music [60].
4. Do We Need to Distinguish Mood from Emotion?
5. Potential Benefits of Discriminating Mood from Emotion in Organisations
5.1. Improved Mental Health
5.2. Reduced Interpersonal Bias and Conflict
5.3. Reduced Risk of Cardiovascular, Metabolic, and Neurological Disease
6. Conclusions
7. Empirical Tests of the 4-R Model
- Recognise: people will be able to distinguish their moods from their emotions.
- Restore: people experiencing moderate to intense mood will find strategies aimed at restoration more effective than those aimed at resolution.
- Resolve: people experiencing moderate to intense emotion will find strategies aimed at resolution more effective than those aimed at restoration.
- Regulate: strategies aimed at regulation will be significantly more effective when people experience intense feelings without being able to recognise it as mood or emotion or when restoration or resolution strategies are not options.
8. Implications for Practice in Teams and Organisations
- Systematically ‘check-in’ with their feelings through the use of a self-report tool at least once per week, but ideally more often.
- Think about their feelings in granular terms; to move beyond ‘good mood’ and ‘bad mood’ to not only more precisely label the feeling (for example irritability can feel a lot like anxiety until interrogated), but also the intensity of the feeling.
- Reflect on possible causes and potentially effective responses. Are they feeling irritable because the situation is legitimately irritating, or are they simply tired or otherwise low on resources making them feel irritable about everything? How does this affect their responses, both internal/psychological and external/behavioural? What can they do to modify their current irritability, and what can they do to reduce the chance of a recurrence?
- Communicate their feelings systematically and honestly to their colleagues when possible; for example, before a meeting people can complete an emotion/mood profile and share this with other attendees (this is now common practice in a number of organisations). This allows the person themselves to be aware of the emotions/moods they are experiencing—and if needs be to respond empathically—but also allows other attendees to accommodate these feelings into their meeting strategy where necessary. It should not be forgotten that, in the workplace, both talking and listening are therapeutic in themselves [126,127].
- Extending the above, people can employ ‘reverse profiling’, in which people rate each other’s moods and emotional responses. While this strategy is often only helpful between people or among teams with existing trust, it can nonetheless provide a powerful feedback loop and can further enhance emotional awareness and granularity.
- Anonymously monitor and measure the feelings of employees at an organisational level, ideally routinely, for example every 3 months, but especially during periods of high stress. This often provides a powerful indicator of the mood of an organisation, turning what is often a metaphor into a metric.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Promoting Mental Health: Concepts, Emerging Evidence, Practice: Summary Report; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- Iasiello, M.; van Agteren, J. Mental health and/or mental illness: A scoping review of the evidence and implications of the dual-continua model of mental health. Evid. Base A J. Evid. Rev. Key Policy Areas 2020, 1–45. [Google Scholar] [CrossRef]
- Bohlmeijer, E.T.; Westerhof, G.J. A new model for sustainable mental health: Integrating well-being into psychological treatment. In Making an Impact on Mental Health; Routledge: Abingdon-on-Thames, UK, 2020; pp. 153–188. [Google Scholar]
- Iasiello, M.; van Agteren, J.; Keyes, C.L.M.; Cochrane, E.M. Positive mental health as a predictor of recovery from mental illness. J. Affect. Disord. 2019, 251, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Ipsen, C.; Karanika-Murray, M.; Nardelli, G. Addressing mental health and organisational performance in tandem: A challenge and an opportunity for bringing together what belongs together. Work Stress 2020, 34, 1–4. [Google Scholar] [CrossRef]
- Petitta, L.; Probst, T.M.; Ghezzi, V.; Barbaranelli, C. Cognitive failures in response to emotional contagion: Their effects on workplace accidents. Accid. Anal. Prev. 2019, 125, 165–173. [Google Scholar] [CrossRef]
- Bohlmeijer, E.; Westerhof, G. The Model for Sustainable Mental Health: Future Directions for Integrating Positive Psychology Into Mental Health Care. Front. Psychol. 2021, 12, 747999. [Google Scholar] [CrossRef]
- Alexander, R.; Aragón, O.R.; Bookwala, J.; Cherbuin, N.; Gatt, J.M.; Kahrilas, I.J.; Kästner, N.; Lawrence, A.; Lowe, L.; Morrison, R.G.; et al. The neuroscience of positive emotions and affect: Implications for cultivating happiness and wellbeing. Neurosci. Biobehav. Rev. 2021, 121, 220–249. [Google Scholar] [CrossRef]
- Niedziela, M.M.; Ambroze, K. Chapter 17—Neuroscience tools: Using the right tool for the right question. In Emotion Measurement, 2nd ed.; Meiselman, H.L., Ed.; Woodhead Publishing: Sawston, UK, 2021; pp. 559–592. [Google Scholar]
- Lajante, M.; Lux, G. Perspective: Why Organizational Researchers Should Consider Psychophysiology When Investigating Emotion? Front. Psychol. 2020, 11, 1705. [Google Scholar] [CrossRef]
- Beedie, C.; Terry, P.; Lane, A. Distinctions between emotion and mood. Cogn. Emot. 2005, 19, 847–878. [Google Scholar] [CrossRef]
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef]
- Attridge, M. A Global Perspective on Promoting Workplace Mental Health and the Role of Employee Assistance Programs. Am. J. Health Promot. 2019, 33, 622–629. [Google Scholar] [CrossRef] [Green Version]
- Leka, S.; Nicholson, P.J. Mental health in the workplace. Occup. Med. 2019, 69, 5–6. [Google Scholar] [CrossRef] [PubMed]
- Jeanguenat, A.M.; Dror, I.E. Human factors effecting forensic decision making: Workplace stress and well-being. J. Forensic Sci. 2018, 63, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Nash-Wright, J. Dealing with anxiety disorders in the workplace: Importance of early intervention when anxiety leads to absence from work. Prof. Case Manag. 2011, 16, 55–59. [Google Scholar] [CrossRef] [PubMed]
- Michailidis, E.; Banks, A.P. The relationship between burnout and risk-taking in workplace decision-making and decision-making style. Work Stress 2016, 30, 278–292. [Google Scholar] [CrossRef]
- Pfeffer, J.; Williams, L. Mental health in the workplace: The coming revolution. McKinsey Q. 2020, 8. Available online: https://www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/mental-health-in-the-workplace-the-coming-revolution (accessed on 22 June 2022).
- Wharton, A.S. Work and emotions. In Handbook of the Sociology of Emotions: Volume II; Springer: Berlin/Heidelberg, Germany, 2014; pp. 335–358. [Google Scholar]
- Bledow, R.; Schmitt, A.; Frese, M.; Kühnel, J. The affective shift model of work engagement. J. Appl. Psychol. 2011, 96, 1246. [Google Scholar] [CrossRef]
- Ashkanasy, N.M.; Dorris, A.D. Emotions in the workplace. Annu. Rev. Organ. Psychol. Organ. Behav. 2017, 4, 67–90. [Google Scholar] [CrossRef]
- Cristofaro, M.; Giardino, P.L.; Malizia, A.P.; Mastrogiorgio, A. Affect and cognition in managerial decision making: A systematic literature review of neuroscience evidence. Front. Psychol. 2022, 13, 762993. [Google Scholar] [CrossRef]
- Kraynak, T.E.; Marsland, A.L.; Gianaros, P.J. Neural mechanisms linking emotion with cardiovascular disease. Curr. Cardiol. Rep. 2018, 20, 128. [Google Scholar] [CrossRef]
- Kinnunen, M.-L.; Kokkonen, M.; Kaprio, J.; Pulkkinen, L. The associations of emotion regulation and dysregulation with the metabolic syndrome factor. J. Psychosom. Res. 2005, 58, 513–521. [Google Scholar] [CrossRef]
- Seidler, A.; Nienhaus, A.; Bernhardt, T.; Kauppinen, T.; Elo, A.L.; Frölich, L. Psychosocial work factors and dementia. Occup. Environ. Med. 2004, 61, 962. [Google Scholar] [CrossRef] [Green Version]
- Terry, P.C.; Parsons-Smith, R.L. Mood Profiling for Sustainable Mental Health among Athletes. Sustainability 2021, 13, 6116. [Google Scholar] [CrossRef]
- Vigo, D.; Thornicroft, G.; Atun, R. Estimating the true global burden of mental illness. Lancet Psychiatry 2016, 3, 171–178. [Google Scholar] [CrossRef]
- Kessler, R.C. Psychiatric epidemiology: Selected recent advances and future directions. Bull World Health Organ. 2000, 78, 464–474. [Google Scholar] [PubMed]
- Bharadwaj, P.; Pai, M.M.; Suziedelyte, A. Mental health stigma. Econ. Lett. 2017, 159, 57–60. [Google Scholar] [CrossRef]
- Marshall, R.E.; Milligan-Saville, J.; Petrie, K.; Bryant, R.A.; Mitchell, P.B.; Harvey, S.B. Mental health screening amongst police officers: Factors associated with under-reporting of symptoms. BMC Psychiatry 2021, 21, 135. [Google Scholar] [CrossRef]
- Violanti, J.M.; Owens, S.L.; McCanlies, E.; Fekedulegn, D.; Andrew, M.E. Law enforcement suicide: A review. Polic. Int. J. 2019, 42, 141–164. [Google Scholar] [CrossRef]
- Novo, R.; Gonzalez, B.; Roberto, M. Beyond personality: Underreporting in high-stakes assessment contexts. Personal. Individ. Differ. 2022, 184, 111190. [Google Scholar] [CrossRef]
- Locke, E.A. Attain Emotional Control by Understanding What Emotions Are. In Handbook of Principles of Organizational Behavior; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2012; pp. 143–159. [Google Scholar] [CrossRef]
- Sutton, A.; Williams, H.M.; Allinson, C.W. A longitudinal, mixed method evaluation of self-awareness training in the workplace. Eur. J. Train. Dev. 2015, 39, 610–627. [Google Scholar] [CrossRef]
- Simcock, G.; McLoughlin, L.T.; De Regt, T.; Broadhouse, K.M.; Beaudequin, D.; Lagopoulos, J.; Hermens, D.F. Associations between Facial Emotion Recognition and Mental Health in Early, Adolescence. Int. J. Environ. Res. Public Health 2020, 17, 330. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y.; Liu, K.; Li, S.; Shu, M. Social Media Activities Emotion Regulation Strategies, Their Interactions on People’s Mental Health in COVID-Pandemic. Int. J. Environ. Res. Public Health 2020, 17, 8931. [Google Scholar] [CrossRef]
- Barfoot, K.; Forster, R.; Lamport, D. Mental Health in New Mothers. A Randomised Controlled Study into the Effects of Dietary Flavonoids on Mood and Perceived Quality of Life. Nutrients 2021, 13, 2383. [Google Scholar] [CrossRef] [PubMed]
- Maung, T.M.; Tan, S.Y.; Tay, C.L.; Kabir, M.S.; Shirin, L.; Chia, T.Y. Mental Health Screening during COVID-Pandemic among School Teachers in Malaysia A. Cross-Sectional Study. Sustainability 2022, 14, 664. [Google Scholar] [CrossRef]
- Bressane, A.; Negri, R.G.; Junior, I.D.B.; Medeiros, L.C.D.C.; Araújo, I.L.L.; Silva, M.B.; Galvão, A.L.d.S.; da Rosa, G.C.S. Association between Contact with Nature Anxiety, Stress Depression Symptoms. A Primary Survey in Brazil. Sustainability 2022, 14, 506. [Google Scholar] [CrossRef]
- Rezaei, M.; Kim, D.; Alizadeh, A.; Rokni, L. Evaluating the mental-health positive impacts of agritourism; A case study from South Korea. Sustainability 2021, 13, 8712. [Google Scholar] [CrossRef]
- Beedie, C. In search of empirical distinctions between emotion and mood: A subjective contextual model. In Mood and Human Performance: Conceptual, Measurement, and Applied Issues; Lane, A., Ed.; Nova: New York, NY, USA, 2007; pp. 63–88. [Google Scholar]
- Beedie, C.; Terry, P.C.; Lane, A.M.; Devonport, T.J. Differential assessment of emotions and moods: Development and validation of the Emotion and Mood Components of Anxiety Questionnaire. Personal. Individ. Differ. 2011, 50, 228–233. [Google Scholar] [CrossRef]
- Butts, M.M.; Becker, W.J.; Boswell, W.R. Hot Buttons and Time Sinks: The Effects of Electronic Communication During Nonwork Time on Emotions and Work-Nonwork Conflict. Acad. Manag. J. 2015, 58, 763–788. [Google Scholar] [CrossRef]
- Caldwell, J.A.; Caldwell, J.L.; Thompson, L.A.; Lieberman, H.R. Fatigue and its management in the workplace. Neurosci. Biobehav. Rev. 2019, 96, 272–289. [Google Scholar] [CrossRef]
- Kober, H. Emotion regulation in substance use disorders. In Handbook of Emotion Regulation, 2nd ed.; The Guilford Press: New York, NY, USA, 2014; pp. 428–446. [Google Scholar]
- Buchanan, B.; Coyle, J.C. The Path to Lawyer Well-Being: Practical Recommendations for Positive Change; American Bar Association National Task Force on Lawyer Well-Being: Chicago, IL, USA, 2017. [Google Scholar]
- Rogelberg, S.G. The SAGE Encyclopedia of Industrial and Organizational Psychology, 2nd ed.; SAGE Publications, Inc.: Thousand Oaks, CA, USA, 2017. [Google Scholar] [CrossRef]
- Ekman, P.E.; Davidson, R.J. The Nature of Emotion: Fundamental Questions; Oxford University Press: Oxford, UK, 1994. [Google Scholar]
- Damasio, A.; Carvalho, G.B. The nature of feelings: Evolutionary and neurobiological origins. Nat. Rev. Neurosci. 2013, 14, 143–152. [Google Scholar] [CrossRef]
- Kontaris, I.; East, B.S.; Wilson, D.A. Behavioral and neurobiological convergence of odor, mood and emotion: A review. Front Behav Neurosci 2020, 14, 35. [Google Scholar] [CrossRef]
- Russell, J.A.; Barrett, L.F. Core affect, prototypical emotional episodes, and other things called emotion: Dissecting the elephant. J. Personal. Soc. Psychol. 1999, 76, 805–819. [Google Scholar] [CrossRef]
- Beedie, C.; Lane, A.; Terry, P. Distinguishing emotion and mood components of pre-competition anxiety among professional rugby players. J. Sports Sci. 2004, 22, 169–170. [Google Scholar]
- Lane, A.M.; Terry, P.C.; Beedie, C.J.; Curry, D.A.; Clark, N. Mood and performance: Test of a conceptual model with a focus on depressed mood. Psychol. Sport Exerc. 2001, 2, 157–172. [Google Scholar] [CrossRef]
- Terry, P. The efficacy of mood state profiling with elite performers: A review and synthesis. Sport Psychol. 1995, 9, 309–324. [Google Scholar] [CrossRef]
- Lane, A.M.; Beedie, C.J.; Jones, M.V.; Uphill, M.; Devonport, T.J. The BASES expert statement on emotion regulation in sport. J. Sports Sci. 2012, 30, 1189–1195. [Google Scholar] [CrossRef] [PubMed]
- Gross, J.J.; Thompson, R.A. Emotion Regulation: Conceptual Foundations. In Handbook of Emotion Regulation; Guilford Press: New York, NY, USA, 2007; pp. 3–24. [Google Scholar]
- Price, C.J.; Hooven, C. Interoceptive Awareness Skills for Emotion Regulation: Theory and Approach of Mindful Awareness in Body-Oriented Therapy (MABT). Front. Psychol. 2018, 9, 798. [Google Scholar] [CrossRef]
- Tamir, M. What Do People Want to Feel and Why? Pleasure and Utility in Emotion Regulation. Curr. Dir. Psychol. Sci. 2009, 18, 101–105. [Google Scholar] [CrossRef]
- Tamir, M. Why Do People Regulate Their Emotions? A Taxonomy of Motives in Emotion Regulation. Personal. Soc. Psychol. Rev. 2015, 20, 199–222. [Google Scholar] [CrossRef]
- Thayer, R.E. Calm Energy: How People Regulate Mood with Food and Exercise; Oxford University Press: Cary, NC, USA, 2003. [Google Scholar]
- Kolb, D.A. Experiential Learning: Experience as the Source of Learning and Development; FT Press: Upper Saddle River, NJ, USA, 2014. [Google Scholar]
- Lilienfeld, S.O.; Strother, A.N. Psychological measurement and the replication crisis: Four sacred cows. Can. Psychol. Psychol. Can. 2020, 61, 281. [Google Scholar] [CrossRef]
- Tackett, J.L.; Brandes, C.M.; King, K.M.; Markon, K.E. Psychology’s replication crisis and clinical psychological science. Annu. Rev. Clin. Psychol. 2019, 15, 579–604. [Google Scholar] [CrossRef] [Green Version]
- Frijda, N.H. Varieties of affect: Emotions and episodes. Moods and sentiments. In The Nature of Emotion; Ekman, P., Davidson, P.R., Eds.; Oxford University Press: Oxford, UK, 1994; pp. 59–67. [Google Scholar]
- Goldman, H.H.; Drake, R.E. Mood disorders and workplace performance: Half a loaf. Am. J. Psychiatry 2006, 163, 1490–1491. [Google Scholar] [CrossRef]
- Thompson, R.A. Emotion dysregulation: A theme in search of definition. Dev. Psychopathol. 2019, 31, 805–815. [Google Scholar] [CrossRef] [PubMed]
- MacCormack, J.K.; Lindquist, K.A. Feeling hangry? When hunger is conceptualized as emotion. Emotion 2019, 19, 301. [Google Scholar] [CrossRef] [PubMed]
- Doyle, J.N.; Campbell, M.A.; Gryshchuk, L. Occupational stress and anger: Mediating effects of resiliency in first responders. J. Police Crim. Psychol. 2021, 36, 463–472. [Google Scholar] [CrossRef] [PubMed]
- Passe, D.H. Effect of Dehydration on Cognitive Function, Perceptual Responses, and Mood. In Fluid Balance, Hydration, and Athletic Performance; Meyer, F., Szygula, Z., Wilk, B., Eds.; CRC Press: Boca Raton, FL, USA, 2016; pp. 155–198. [Google Scholar]
- Lazarus, R.S.; Smith, C.A. Knowledge and appraisal in the cognition—emotion relationship. Cogn. Emot. 1988, 2, 281–300. [Google Scholar] [CrossRef]
- Suri, G.; Gross, J.J. What is an emotion? A connectionist perspective. Emot. Rev. 2022, 14, 99–110. [Google Scholar] [CrossRef]
- Tamietto, M.; De Gelder, B. Neural bases of the non-conscious perception of emotional signals. Nat. Rev. Neurosci. 2010, 11, 697–709. [Google Scholar] [CrossRef]
- Golubitsky, M.; Stewart, I.; Antoneli, F.; Huang, Z.; Wang, Y. (Eds.) Input-Output Networks, Singularity Theory, and Homeostasis; Springer International Publishing: Berlin/Heidelberg, Germany, 2020; pp. 31–65. [Google Scholar]
- Ramsay, D.S.; Woods, S.C. Clarifying the roles of homeostasis and allostasis in physiological regulation. Psychol. Rev. 2014, 121, 225–247. [Google Scholar] [CrossRef]
- Khalsa, S.S.; Adolphs, R.; Cameron, O.G.; Critchley, H.D.; Davenport, P.W.; Feinstein, J.S.; Feusner, J.D.; Garfinkel, S.N.; Lane, R.D.; Mehling, W.E.; et al. Interoception and Mental Health: A Roadmap. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2018, 3, 501–513. [Google Scholar] [CrossRef]
- Chen, W.G.; Schloesser, D.; Arensdorf, A.M.; Simmons, J.M.; Cui, C.; Valentino, R.; Gnadt, J.W.; Nielsen, L.; Hillaire-Clarke, C.S.; Spruance, V.; et al. The Emerging Science of Interoception: Sensing, Integrating, Interpreting, and Regulating Signals within the Self. Trends Neurosci. 2021, 44, 3–16. [Google Scholar] [CrossRef]
- Pace-Schott, E.F.; Amole, M.C.; Aue, T.; Balconi, M.; Bylsma, L.M.; Critchley, H.; Demaree, H.A.; Friedman, B.H.; Gooding, A.E.K.; Gosseries, O.; et al. Physiological feelings. Neurosci. Biobehav. Rev. 2019, 103, 267–304. [Google Scholar] [CrossRef]
- Paulus, M.P.; Stein, M.B. Interoception in anxiety and depression. Brain Struct. Funct. 2010, 214, 451–463. [Google Scholar] [CrossRef] [PubMed]
- Quadt, L.; Critchley, H.D.; Garfinkel, S.N.; Tsakiris, M.; De Preester, H. Interoception and emotion: Shared mechanisms and clinical implications. Interoceptive Mind Homeost. Aware. 2018, 123, 123–143. [Google Scholar]
- van der Kolk, B.A. The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma; Viking: New York, NY, USA, 2014; p. 443. [Google Scholar]
- Pollatos, O.; Schandry, R.; Auer, D.P.; Kaufmann, C. Brain structures mediating cardiovascular arousal and interoceptive awareness. Brain Res. 2007, 1141, 178–187. [Google Scholar] [CrossRef]
- Damasio, A. The Strange Order of Things: Life, Feeling, and the Making of Cultures; Pantheon: New York, NY, USA, 2018. [Google Scholar]
- Barrett, L.F. How Emotions Are Made: The Secret Life of the Brain; Houghton Mifflin Harcourt: Boston, MA, USA, 2017; p. 425. [Google Scholar]
- Damasio, A. Looking for Spinoza: Joy, Sorrow, and the Feeling Brain; Harcourt: Orlando, FL, USA, 2003. [Google Scholar]
- Damasio, A.R. Emotion in the perspective of an integrated nervous system. Brain Res. Rev. 1998, 26, 83–86. [Google Scholar] [CrossRef]
- Panksepp, J.; Biven, L. The Archaeology of Mind: Neuroevolutionary Origins of Human Emotion; W. W. Norton & Company: New York, NY, USA, 2012; p. 562. [Google Scholar]
- Nesse, R.M. Good Reasons for Bad Feelings: Insights from the Frontier of Evolutionary Psychiatry; Dutton: New York, NY, USA, 2019. [Google Scholar]
- Nesse, R.M. Is Depression an Adaptation? Arch Gen Psychiatry 2000, 57, 14–20. [Google Scholar] [CrossRef]
- Nesse, R.M.; Berridge, K.C. Psychoactive Drug Use in Evolutionary Perspective. Science 1997, 278, 63. [Google Scholar] [CrossRef]
- Nesse, R.M.; Stein, D.J. How evolutionary psychiatry can advance psychopharmacology. Dialogues Clin. Neurosci. 2019, 21, 167–175. [Google Scholar] [CrossRef]
- Nesse, R.M.; Williams, G.C. Why We Get Sick the New Science of Darwinian Medicine; Random House: New York, NY, USA, 1996. [Google Scholar]
- McLean, P. The Triune Brain in Evolution: Role in Paleocerebral Functions; Plenum: New York, NY, USA, 1989. [Google Scholar]
- Viamontes, G.I.; Beitman, B.D. Mapping the unconscious in the brain. Psychiatr. Ann. 2007, 37, 243. [Google Scholar] [CrossRef]
- Valenzuela-Moguillansky, C.; Reyes-Reyes, A.; Gaete, M.I. Exteroceptive and Interoceptive Body-Self Awareness in Fibromyalgia Patients. Front. Hum. Neurosci. 2017, 11, 117. [Google Scholar] [CrossRef]
- Barrett, L.F. Feeling Is Perceiving: Core Affect and Conceptualization in the Experience of Emotion. In Emotion and Consciousness; The Guilford Press: New York, NY, USA, 2005; pp. 255–284. [Google Scholar]
- Madrid, H.P.; Patterson, M.G.; Leiva, P.I. Negative core affect and employee silence: How differences in activation, cognitive rumination, and problem-solving demands matter. J. Appl. Psychol. 2015, 100, 1887–1898. [Google Scholar] [CrossRef] [Green Version]
- Stiglbauer, B. Differential challenge and hindrance stressor relations with job-related core affect. Int. J. Stress Manag. 2018, 25, 62–80. [Google Scholar] [CrossRef]
- Dennett, D.C. Consciousness Explained; Little, Brown and Co: New York, NY, USA, 1991; p. 511. [Google Scholar]
- Gaebel, W.; Zielasek, J.; Reed, G.M. Mental and behavioural disorders in the ICD-11: Concepts, methodologies, and current status. Psychiatr. Pol. 2017, 51, 169–195. [Google Scholar] [CrossRef] [PubMed]
- Martin-Key, N.A.; Olmert, T.; Barton-Owen, G.; Han, S.Y.S.; Cooper, J.D.; Eljasz, P.; Farrag, L.P.; Friend, L.V.; Bell, E.; Cowell, D. The Delta Study–Prevalence and characteristics of mood disorders in 924 individuals with low mood: Results of the of the World Health Organization Composite International Diagnostic Interview (CIDI). Brain Behav. 2021, 11, e02167. [Google Scholar] [CrossRef] [PubMed]
- Ackermans, M.A.; Jonker, N.C.; Bennik, E.C.; de Jong, P.J. Hunger increases negative and decreases positive emotions in women with a healthy weight. Appetite 2022, 168, 105746. [Google Scholar] [CrossRef]
- Firth, J.; Gangwisch, J.E.; Borsini, A.; Wootton, R.E.; Mayer, E.A. Food and mood: How do diet and nutrition affect mental wellbeing? BMJ 2020, 369, m2382. [Google Scholar] [CrossRef]
- Wiehler, A.; Branzoli, F.; Adanyeguh, I.; Mochel, F.; Pessiglione, M. A neuro-metabolic account of why daylong cognitive work alters the control of economic decisions. Curr. Biol. 2022, 32, 3564–3575.e5. [Google Scholar] [CrossRef]
- Raglin, J.S.; Wilson, G.S. Overtraining in athletes. In Emotions in Sport; Human Kinetics: Champaign, IL, USA, 2000; pp. 191–207. [Google Scholar]
- Raven, F.; Van der Zee, E.A.; Meerlo, P.; Havekes, R. The role of sleep in regulating structural plasticity and synaptic strength: Implications for memory and cognitive function. Sleep Med. Rev. 2018, 39, 3–11. [Google Scholar] [CrossRef]
- Centanni, S.W.; Janes, A.C.; Haggerty, D.L.; Atwood, B.; Hopf, F.W. Better living through understanding the insula: Why subregions can make all the difference. Neuropharmacology 2021, 198, 108765. [Google Scholar] [CrossRef]
- Thagard, P.; Larocque, L.; Kajić, I. Emotional change: Neural mechanisms based on semantic pointers. Emotion 2021. [Google Scholar] [CrossRef]
- Barrett, L.F. Categories and Their Role in the Science of Emotion. Psychol. Inq. 2017, 28, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Moors, A.; Ellsworth, P.C.; Scherer, K.R.; Frijda, N.H. Appraisal Theories of Emotion: State of the Art and Future Development. Emot. Rev. 2013, 5, 119–124. [Google Scholar] [CrossRef]
- Barrett, L.F.; Simmons, W.K. Interoceptive predictions in the brain. Nat. Rev. Neurosci. 2015, 16, 419–429. [Google Scholar] [CrossRef] [PubMed]
- Frijda, N.H. Emotion, cognitive structure, and action tendency. Cogn. Emot. 1987, 1, 115–143. [Google Scholar] [CrossRef]
- Salovey, P.; Rothman, A.J.; Detweiler, J.B.; Steward, W.T. Emotional states and physical health. Am. Psychol. 2000, 55, 110. [Google Scholar] [CrossRef] [PubMed]
- Kreibig, S.D. Autonomic nervous system activity in emotion: A review. Biol. Psychol. 2010, 84, 394–421. [Google Scholar] [CrossRef]
- Rhudy, J.L.; Meagher, M.W. The role of emotion in pain modulation. Curr. Opin. Psychiatry 2001, 14, 241–245. [Google Scholar] [CrossRef]
- Lundberg, U.; Forsman, M.; Zachau, G.; Eklöf, M.; Palmerud, G.; Melin, B.; Kadefors, R. Effects of experimentally induced mental and physical stress on motor unit recruitment in the trapezius muscle. Work Stress 2002, 16, 166–178. [Google Scholar] [CrossRef]
- Pine, D.S.; Wise, S.P.; Murray, E.A. Evolution, emotion, and episodic engagement. Am. J. Psychiatry 2021, 178, 701–714. [Google Scholar] [CrossRef]
- Turan, I.; Chegut, A.; Fink, D.; Reinhart, C. The value of daylight in office spaces. Build. Environ. 2020, 168, 106503. [Google Scholar] [CrossRef]
- Schachter, S.; Singer, J. Cognitive, social, and physiological determinants of emotional state. Psychol. Rev. 1962, 69, 379–399. [Google Scholar] [CrossRef]
- Tugade, M.M.; Fredrickson, B.L.; Feldman Barrett, L. Psychological Resilience and Positive Emotional Granularity: Examining the Benefits of Positive Emotions on Coping and Health. J. Personal. 2004, 72, 1161–1190. [Google Scholar] [CrossRef] [PubMed]
- Suvak, M.K.; Musicaro, R.M.; Hodgdon, H. Chapter 13—Emotional granularity in PTSD. In Emotion in Posttraumatic Stress Disorder; Tull, M.T., Kimbrel, N.A., Eds.; Academic Press: Cambridge, MA, USA, 2020; pp. 377–407. [Google Scholar]
- Smidt, K.E.; Suvak, M.K. A brief, but nuanced, review of emotional granularity and emotion differentiation research. Curr. Opin. Psychol. 2015, 3, 48–51. [Google Scholar] [CrossRef]
- Locke, E.A. It’s Time We Brought Introspection Out of the Closet. Perspect. Psychol. Sci. 2009, 4, 24–25. [Google Scholar] [CrossRef] [PubMed]
- Todd, J.; Aspell, J.E. Mindfulness, Interoception, and the Body. Brain Sci. 2022, 12, 696. [Google Scholar] [CrossRef]
- McNair, D.M.; Lorr, M.; Droppelman, L.F. Manual for the Profile of Mood States; Educational and Industrial Testing Services: San Diego, CA, USA, 1971. [Google Scholar]
- Terry, P.C.; Lane, A.M. User Guide for the Brunel Mood Scale; Peter Terry Consultants: Toowoomba, QLD, Australia, 2010. [Google Scholar]
- Torre, J.B.; Lieberman, M.D. Putting Feelings Into Words: Affect Labeling as Implicit Emotion Regulation. Emot. Rev. 2018, 10, 116–124. [Google Scholar] [CrossRef]
- Kluger, A.N.; Itzchakov, G. The power of listening at work. Annu. Rev. Organ. Psychol. Organ. Behav. 2022, 9, 121–146. [Google Scholar] [CrossRef]
- Peake, J.M. Recovery after exercise: What is the current state of play? Curr. Opin. Physiol. 2019, 10, 17–26. [Google Scholar] [CrossRef]
- Saper, C.B.; Chou, T.C.; Elmquist, J.K. The need to feed: Homeostatic and hedonic control of eating. Neuron 2002, 36, 199–211. [Google Scholar] [CrossRef]
- Watts, A.G.; Kanoski, S.E.; Sanchez-Watts, G.; Langhans, W. The physiological control of eating: Signals, neurons, and networks. Physiol. Rev. 2022, 102, 689–813. [Google Scholar] [CrossRef]
- Tononi, G.; Cirelli, C. Sleep and the price of plasticity: From synaptic and cellular homeostasis to memory consolidation and integration. Neuron 2014, 81, 12–34. [Google Scholar] [CrossRef] [Green Version]
- Franks, N.P.; Wisden, W. The inescapable drive to sleep: Overlapping mechanisms of sleep and sedation. Science 2021, 374, 556–559. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, A.N.; Walker, M.P. The Role of Sleep in Emotional Brain Function. Annu. Rev. Clin. Psychol. 2014, 10, 679–708. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.Z.; Nusslock, R. Exercise-Mediated Neurogenesis in the Hippocampus via BDNF. Front. Neurosci. 2018, 12, 52. [Google Scholar] [CrossRef]
- Dishman, R.K.; Berthoud, H.-R.; Booth, F.W.; Cotman, C.W.; Edgerton, V.R.; Fleshner, M.R.; Gandevia, S.C.; Gomez-Pinilla, F.; Greenwood, B.N.; Hillman, C.H.; et al. Neurobiology of Exercise. Obesity 2006, 14, 345–356. [Google Scholar] [CrossRef]
- Vaegter, H.B.; Fehrmann, E.; Gajsar, H.; Kreddig, N. Endogenous Modulation of Pain: The Role of Exercise, Stress, and Cognitions in Humans. Clin. J. Pain 2020, 36, 150–161. [Google Scholar] [CrossRef]
- Bettio, L.E.B.; Thacker, J.S.; Rodgers, S.P.; Brocardo, P.S.; Christie, B.R.; Gil-Mohapel, J. Interplay between hormones and exercise on hippocampal plasticity across the lifespan. Biochim. Biophys. Acta (BBA)—Mol. Basis Dis 2020, 1866, 165821. [Google Scholar] [CrossRef] [PubMed]
- Plano, S.A.; Casiraghi, L.P.; García Moro, P.; Paladino, N.; Golombek, D.A.; Chiesa, J.J. Circadian and Metabolic Effects of Light: Implications in Weight Homeostasis and Health. Front. Neurol. 2017, 8, 558. [Google Scholar] [CrossRef]
- Herman, J.H. Chapter 170—Chronobiologic Monitoring Techniques. In Principles and Practice of Sleep Medicine, 6th ed.; Kryger, M., Roth, T., Dement, W.C., Eds.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 1659–1670.e1654. [Google Scholar]
- Young, S.N. How to increase serotonin in the human brain without drugs. J. Psychiatry Neurosci. 2007, 32, 394–399. [Google Scholar]
- Garrison, J.L.; Knight, Z.A. Linking smell to metabolism and aging. Science 2017, 358, 718–719. [Google Scholar] [CrossRef]
- Krach, S.; Paulus, F.M.; Bodden, M.; Kircher, T. The rewarding nature of social interactions. Front. Behav. Neurosci. 2010, 4, 22. [Google Scholar] [CrossRef]
- Ben Simon, E.; Vallat, R.; Rossi, A.; Walker, M.P. Sleep loss leads to the withdrawal of human helping across individuals, groups, and large-scale societies. PLoS Biol. 2022, 20, e3001733. [Google Scholar] [CrossRef] [PubMed]
- Bowler, D.E.; Buyung-Ali, L.M.; Knight, T.M.; Pullin, A.S. A systematic review of evidence for the added benefits to health of exposure to natural environments. BMC Public Health 2010, 10, 456. [Google Scholar] [CrossRef] [PubMed]
- Berto, R. The role of nature in coping with psycho-physiological stress: A literature review on restorativeness. Behav. Sci 2014, 4, 394–409. [Google Scholar] [CrossRef] [PubMed]
- Jahncke, H.; Hygge, S.; Halin, N.; Green, A.M.; Dimberg, K. Open-plan office noise: Cognitive performance and restoration. J. Environ. Psychol. 2011, 31, 373–382. [Google Scholar] [CrossRef]
- Lee, K.E.; Williams, K.J.H.; Sargent, L.D.; Williams, N.S.G.; Johnson, K.A. 40-second green roof views sustain attention: The role of micro-breaks in attention restoration. J. Environ. Psychol. 2015, 42, 182–189. [Google Scholar] [CrossRef]
- Inagaki, T.K.; Eisenberger, N.I. Giving support to others reduces sympathetic nervous system-related responses to stress. Psychophysiology 2016, 53, 427–435. [Google Scholar] [CrossRef]
- Al-Shawaf, L.; Conroy-Beam, D.; Asao, K.; Buss, D.M. Human Emotions: An Evolutionary Psychological Perspective. Emot. Rev. 2015, 8, 173–186. [Google Scholar] [CrossRef]
- Nesse, R.M. Evolutionary explanations of emotions. Hum. Nat. 1990, 1, 261–289. [Google Scholar] [CrossRef]
- McRae, K.; Gross, J.J. Emotion regulation. Emotion 2020, 20, 1–9. [Google Scholar] [CrossRef]
- Brown, H.; Proulx, M.J.; Stanton Fraser, D. Hunger Bias or Gut Instinct? Responses to Judgments of Harm Depending on Visceral State Versus Intuitive Decision-Making. Front. Psychol. 2020, 11, 2261. [Google Scholar] [CrossRef]
- Danziger, S.; Levav, J.; Avnaim-Pesso, L. Extraneous factors in judicial decisions. Proc. Natl. Acad. Sci. USA 2011, 108, 6889–6892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beedie, C.; Lane, A.M. The role of glucose in self-control: Another look at the evidence and an alternative conceptualization. Pers. Soc. Psychol. Rev. 2012, 16, 143–153. [Google Scholar] [CrossRef] [PubMed]
- Dvorak, R.D.; Sargent, E.M.; Kilwein, T.M.; Stevenson, B.L.; Kuvaas, N.J.; Williams, T.J. Alcohol use and alcohol-related consequences: Associations with emotion regulation difficulties. Am. J. Drug Alcohol Abus. 2014, 40, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Wadley, G.; Smith, W.; Koval, P.; Gross, J.J. Digital emotion regulation. Curr. Dir. Psychol. Sci. 2020, 29, 412–418. [Google Scholar] [CrossRef]
- Evers, C.; Marijn Stok, F.; de Ridder, D.T.D. Feeding your feelings: Emotion regulation strategies and emotional eating. Personal. Soc. Psychol. Bull. 2010, 36, 792–804. [Google Scholar] [CrossRef]
- Wang, K.; Burton, C.L.; Pachankis, J.E. Depression and substance use: Towards the development of an emotion regulation model of stigma coping. Subst. Use Misuse 2018, 53, 859–866. [Google Scholar] [CrossRef]
- Williams, A.D.; Grisham, J.R.; Erskine, A.; Cassedy, E. Deficits in emotion regulation associated with pathological gambling. Br. J. Clin. Psychol. 2012, 51, 223–238. [Google Scholar] [CrossRef]
- Wise, R.A.; Robble, M.A. Dopamine and Addiction. Annu. Rev. Psychol. 2020, 71, 79–106. [Google Scholar] [CrossRef]
- De Luca, M.A. Habituation of the responsiveness of mesolimbic and mesocortical dopamine transmission to taste stimuli. Front. Integr. Neurosci. 2014, 8, 21. [Google Scholar] [CrossRef]
- O’Connor, D.B.; Thayer, J.F.; Vedhara, K. Stress and Health: A Review of Psychobiological Processes. Annu. Rev. Psychol. 2021, 72, 663–688. [Google Scholar] [CrossRef]
- Kivimäki, M.; Steptoe, A. Effects of stress on the development and progression of cardiovascular disease. Nat. Rev. Cardiol. 2018, 15, 215–229. [Google Scholar] [CrossRef] [PubMed]
- Chandola, T.; Brunner, E.; Marmot, M. Chronic stress at work and the metabolic syndrome: Prospective study. BMJ 2006, 332, 521. [Google Scholar] [CrossRef] [PubMed]
- Djamshidian, A.; Lees, A.J. Can stress trigger Parkinson’s Disease? J. Neurol. Neurosurg. Psychiatry 2014, 85, 878. [Google Scholar] [CrossRef] [PubMed]
- Hemmerle, A.M.; Herman, J.P.; Seroogy, K.B. Stress, depression and Parkinson’s disease. Exp. Neurol. 2012, 233, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Arnold, M.B. Emotion and Personality; Columbia University Press: New York, NY, USA, 1960. [Google Scholar]


{kind=link}
| Criterion | Emotion | Mood |
|---|---|---|
| Anatomy | Related to the heart | Related to the mind |
| Awareness of cause | Individual is aware of cause | Individual may be unaware of cause |
| Cause | Caused by a specific event or object | Cause is less well defined |
| Clarity | Clearly defined | Nebulous |
| Consequences | Largely behavioural and expressive | Largely cognitive |
| Control | Not controllable | Controllable |
| Display | Displayed | Not displayed |
| Duration | Brief | Enduring |
| Experience | Felt | Thought |
| Intensity | Intense | Mild |
| Intentionality | About something | Not about anything in particular |
| Physiology | Distinct physiological patterning | No distinct physiological patterning |
| Stability | Fleeting and volatile | Stable |
| Timing | Rises and dissipates quickly | Rises and dissipates slowly |
| Criterion | Non-Academic | Academic |
|---|---|---|
| Cause | 65% | 31% |
| Duration | 40% | 62% |
| Control | 25% | - |
| Experience | 15% | - |
| Consequences | 14% | 31% |
| Display | 14% | - |
| Intentionality | 12% | 41% |
| Anatomy | 11% | - |
| Intensity | 11% | 17% |
| Timing | 8% | - |
| Function | 7% | 18% |
| Physiology | 7% | 8% |
| Stability | 7% | - |
| Awareness of cause | 4% | 13% |
| Clarity | 3% | - |
| Valence | 3% | - |
| Activity | Effects |
|---|---|
| Sleep | Restoration of cognitive function Restoration of emotional function Maintenance of circadian rhythm Tissue repair and synthesis Removal of neurobiological waste products Consolidation of neural connectivity |
| Eating (homeostatic) | Restoration of blood sugar Maintenance of circadian rhythm Provision of metabolic energy Maintenance of cellular and molecular growth and repair Increased opioid and dopamine signalling |
| Hydration (homeostatic) | Restoration of fluid and electrolyte balance Restoration of optimal temperature Improved cellular function Improved thermoregulation |
| Change in temperature | Restoration of optimal temperature Maintenance of circadian rhythm (sleep) Improved cellular function Reduced metabolic energy cost |
| Physical activity | Reduction in excessive arousal Increase in inadequate arousal Maintenance of circadian rhythm Increases metabolic activity/rate Increases oxygen transport Increases thermoregulation Increases endogenous opioid activity Modifies brain chemistry (BDNF) |
| Exposure to natural light | Improvement in sleep timing and quality Reduction in emotional arousal Maintenance of circadian rhythm Increased serotonin signalling Increased melatonin production |
| Receiving social support | Increased parasympathetic nervous system activation Increased endogenous opioid signalling Increased oxytocin signalling |
| Offering social support (altruism) | Reduced sympathetic nervous system activation [148] Increases endogenous opioid signalling Increased dopamine signalling Increases oxytocin signalling |
| Experience | Related Workplace Scenario |
|---|---|
| Exclusion/perceived exclusion | Left out of the final pitch to client/boss Not included in the decision-making process Not included in rewards for the team Information not being shared or being kept ‘out of the loop’ |
| Hostility/conflict | Argument with colleague Interrupted/spoken across Irritation with behaviours/habits |
| Embarrassment/humiliation | Mistakes/poor performance (publicly) highlighted Spoken down to (in front of others) Subject of jokes/unkind comments |
| Inequity/envy | Overlooked for pay increase when others receive one Witness a colleague(s) receiving praise/reward/success Witness favourable treatment of colleague(s) Learn of colleague claiming credit for your work |
| Uncertainty/anxiety | Unpredictable behaviour of colleague Unsure of expectations/task Contract expiration/negotiation |
| Shame/guilt | Treated a colleague poorly/spoken badly of a colleague Acted in a dishonest manner Broke the trust of a colleague |
| Activity | Example Behaviour | Effect on Event/Situation |
|---|---|---|
| Challenge | Ask the person to reconsider or rephrase something offensive | Prevents likelihood of event/behaviour occurring Reduces anger/hostility |
| Compensate | Ask the person to apologise Accept apology Apologise to another person Anticipate a likely issue and inform someone first to frame the situation | Reduces its emotional impact Reduces anger/hostility Reduces guilt Reduces emotional impact and reduces potential feelings of guilt |
| Reframe | Thinking “I would probably have done the same” | Reduces its emotional impact Reduces intensity of emotion |
| Feedback | Convey the effect on you of their criticism | Reduces chances of recurrence Reduces anxiety of future repeat of event/situation Reduces possibility of repeated negative emotion due to recall |
| Avoid/withdraw | Excuse yourself from the meeting | Removes it from immediate environment Avoids escalation of anger and might reduce intensity |
| Take control | Reset career goals Re-establish relationships Talk about feelings Seek counselling | Reduces its emotional impact Increases hope Catharsis |
| Strategy | Example Behaviour | Mechanism |
|---|---|---|
| Distraction | Film/music Socialisation Social media | Modified autonomic nervous system activity (excitement/relaxation) Increased dopamine activity (pleasure & reward) Increase endogenous opioid activity (euphoria and lower pain) Increase oxytocin activity (increased social bonds) |
| Stimulation | Play Performance art. Creative art Competitive sport Manual work | Modified autonomic nervous system activity (excitement/relaxation) Increased dopamine activity (pleasure & reward) Increase endogenous opioid activity (euphoria and lower pain) Increase oxytocin activity (increased social bonds) Increase endogenous opioid activity (euphoria and lower pain) |
| Eating (hedonistic) | High energy food Salty/fatty foods | Increased dopamine activity (pleasure & reward) Increase endogenous opioid activity (euphoria and lower pain) |
| Drinking (hedonistic) | Coffee Alcohol Energy drinks | Reduced adenosine signalling (reduced fatigue) (caffeine) Increased dopamine activity (pleasure) (caffeine & alcohol) Increased gamma-aminobutyric acid (GABA) activity (alcohol) |
| Catharsis | Sport/exercise Dance/performance arts Martial arts Manual work | Directly modified physiological arousal Increased metabolic activity/rate Increased oxygen transport Increased temperature & thermoregulation Increased endogenous opioid activity Increased brain-derived neurotrophic factor (BDNF) levels |
| Relaxation | Massage Stretching Systematic relaxation Yoga/tai-chi/pilates | Reduced nervous system activation (lower adrenaline) Reduced endocrine system activation (lower cortisol) Reduced motor stimulation (reduced muscle tension) Reduced skeletomuscular pain |
| Purposeful immersion | Meditation Creative arts Yoga/tai-chi/pilates | Reduced nervous system activation (lower adrenaline) Reduced endocrine system activation (lower cortisol) Increased dopamine and opioid activity Reduced cortisol and adrenaline |
| Purposeful altruism | Charity work Fundraising Community work | Increased dopamine activity (pleasure & reward) Increase endogenous opioid activity (euphoria and lower pain) Increase oxytocin activity (increased social bonds) |
| Recognition | Cause | Restoration Options | Resolution Options | Regulation Options |
|---|---|---|---|---|
| Anxiety ahead of interview | Memory of previous failure | N/A | Reframing/countering | Relaxation Exercise |
| Anxiety ahead of interview | Poor sleep Poor diet Low energy | Brief exercise Food/drink Rest | Reframing/countering | Relaxation Distraction |
| Anger with a colleague | Colleague behaving unprofessionally | N/A | Request that colleague desist or apologise | Relaxation Reframing Distraction Avoidance |
| Anger with a colleague | Poor sleep Poor diet Low energy | Walk in daylight Eat/drink Take break Find quiet place Rest | Reframing/countering | Relaxation Reframing Avoidance |
| Low-level persistent guilt | Not allocating time and energy to family | N/A | Reserve time for family Reserve energy for family Apologise to family | Exercise Distraction Reframing Avoidance |
| Low-level persistent guilt | Poor treatment of colleagues | N/A | Apologise to colleagues Build relationships Modify goals Modify expectations | Exercise Distraction Reframing Avoidance |
| Persistent anxiety/sadness/depression | Low work satisfaction Unmet goals | N/A | Modify expectations Modify goals (Only seek resolution if restoration is unsuccessful. If the emotion is not about your career, changes here could make things worse) | Exercise Distraction Reframing |
| Persistent anxiety/sadness/depression | Poor work relationships | Build relationships | Exercise Distraction Reframe | |
| Persistent anxiety/sadness/depression | Unsure as to cause | Improve sleep Improve diet Be physically active Seek social support Offer social support |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Beedie, C.J.; Lane, A.M.; Udberg, R.; Terry, P.C. The 4R Model of Mood and Emotion for Sustainable Mental Health in Organisational Settings. Sustainability 2022, 14, 11670. https://doi.org/10.3390/su141811670
Beedie CJ, Lane AM, Udberg R, Terry PC. The 4R Model of Mood and Emotion for Sustainable Mental Health in Organisational Settings. Sustainability. 2022; 14(18):11670. https://doi.org/10.3390/su141811670
Chicago/Turabian StyleBeedie, Christopher J., Andrew M. Lane, Robert Udberg, and Peter C. Terry. 2022. "The 4R Model of Mood and Emotion for Sustainable Mental Health in Organisational Settings" Sustainability 14, no. 18: 11670. https://doi.org/10.3390/su141811670