
Barriers and Facilitators for the Romanian Older Adults in Enjoying Physical Activity Health-Related Benefits

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
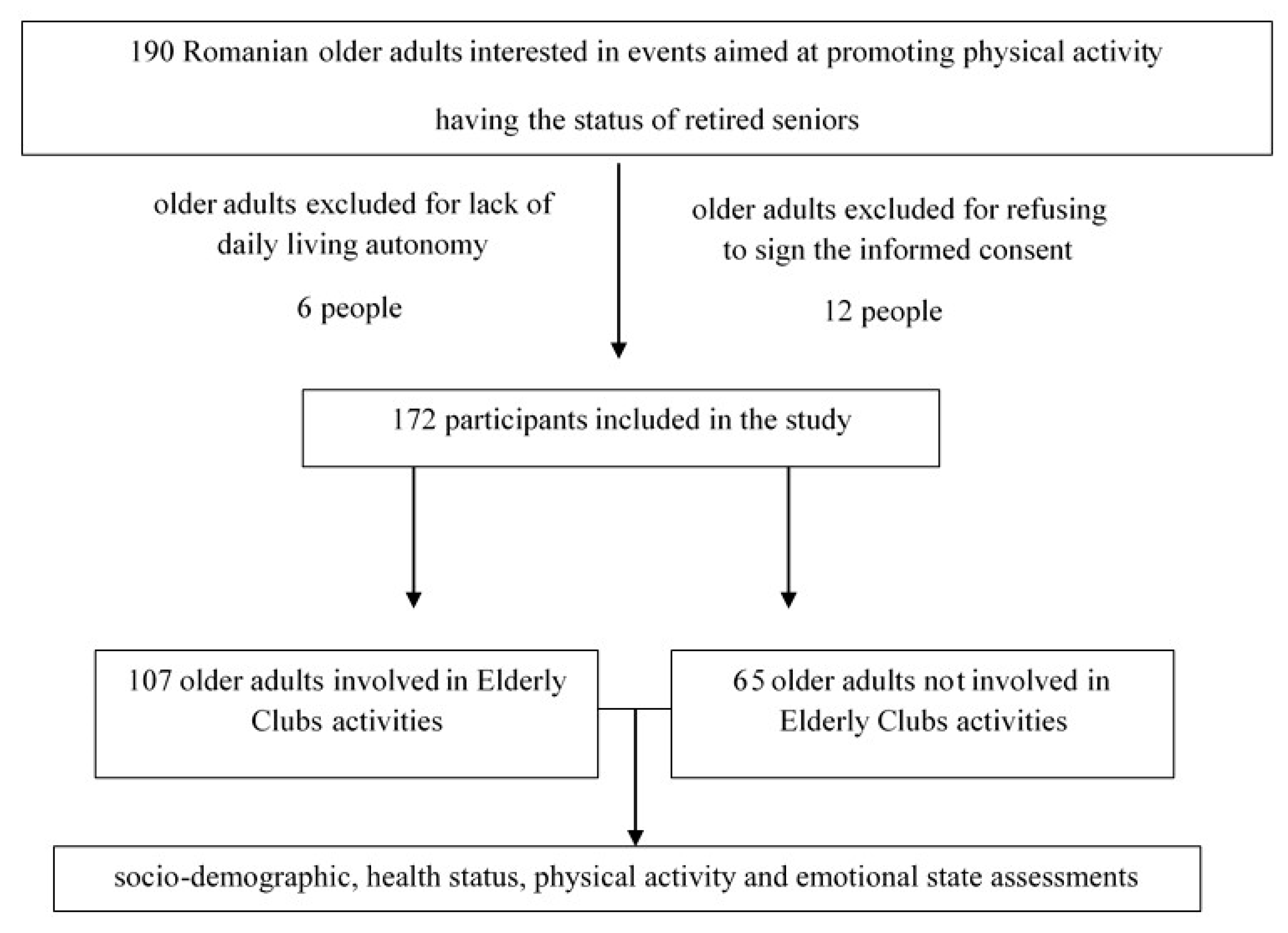
2.1. Participants
2.2. Procedure
2.3. Statistics
3. Results
3.1. Socio-Demographic Analysis
3.2. Health Condition Analysis
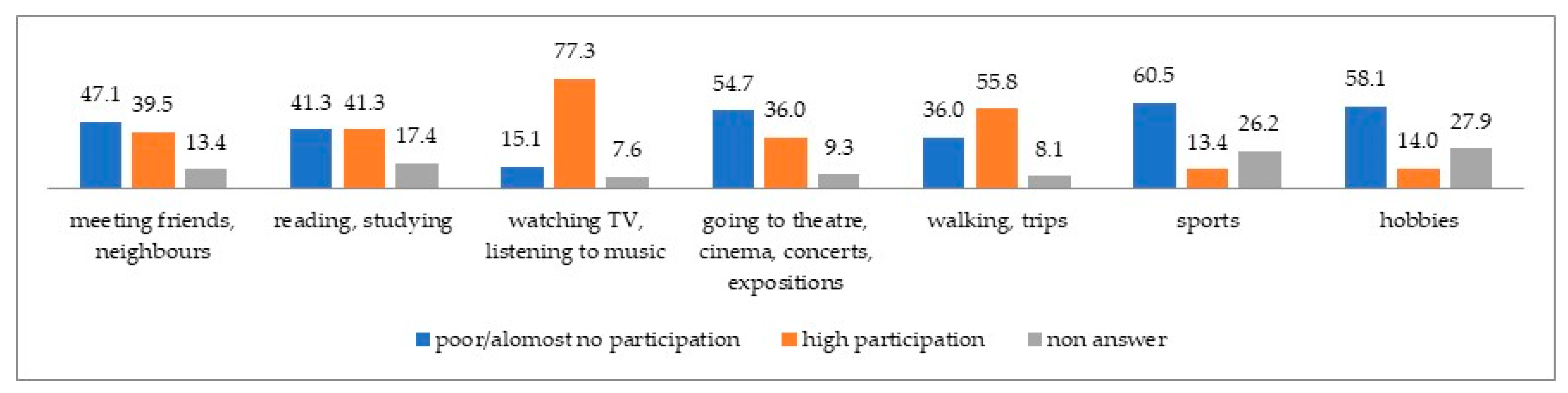
3.3. Leisure Preferences
3.4. PASE Analysis
3.5. DASS Analysis
3.6. Regression Model
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variables and Subgroups of Participants | Mean Difference | Std. Error | Sig. | 95% Confidence Interval | ||
|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | |||||
| PASE leisure activity | ||||||
| MPEC | WPEC | 8.61 | 5.96 | 0.479 | −7.35 | 24.58 |
| MNPEC | 12.84 | 6.03 | 0.161 | −3.30 | 28.98 | |
| WNPEC | 18.34 * | 5.81 | 0.016 | 2.713 | 33.96 | |
| WPEC | MPEC | −8.61 | 5.96 | 0.479 | −24.58 | 7.35 |
| MNPEC | 4.23 | 3.52 | 0.628 | −5.01 | 13.46 | |
| WNPEC | 9.72 * | 3.12 | 0.012 | 1.58 | 17.87 | |
| MNPEC | MPEC | −12.84 | 6.03 | 0.161 | −28.98 | 3.30 |
| WPEC | −4.23 | 3.52 | 0.628 | −13.46 | 5.01 | |
| WNPEC | 5.49 | 3.25 | 0.338 | −3.11 | 14.09 | |
| WNPEC | MPEC | −18.34 * | 5.81 | 0.016 | −33.96 | −2.71 |
| WPEC | −9.72 * | 3.12 | 0.012 | −17.87 | −1.58 | |
| MNPEC | −5.49 | 3.25 | 0.338 | −14.09 | 3.11 | |
| PASE household activity | ||||||
| MPEC | WPEC | 4.52 | 9.94 | 0.968 | −22.01 | 31.04 |
| MNPEC | 8.72 | 11.32 | 0.868 | −21.27 | 38.71 | |
| WNPEC | −0.70 | 10.90 | 1.000 | −29.60 | 28.21 | |
| WPEC | MPEC | −4.52 | 9.94 | 0.968 | −31.04 | 22.01 |
| MNPEC | 4.21 | 8.31 | 0.957 | −17.80 | 26.21 | |
| WNPEC | −5.21 | 7.73 | 0.906 | −25.57 | 15.15 | |
| MNPEC | MPEC | −8.72 | 11.32 | 0.868 | −38.71 | 21.27 |
| WPEC | −4.21 | 8.31 | 0.957 | −26.21 | 17.80 | |
| WNPEC | −9.42 | 9.44 | 0.751 | −34.35 | 15.51 | |
| WNPEC | MPEC | 0.70 | 10.90 | 1.000 | −28.21 | 29.60 |
| WPEC | 5.21 | 7.73 | 0.906 | −15.15 | 25.57 | |
| MNPEC | 9.42 | 9.44 | 0.751 | −15.51 | 34.35 | |
| PASE total score | ||||||
| MPEC | WPEC | 13.13 | 14.08 | 0.788 | −24.65 | 50.91 |
| MNPEC | 21.56 | 15.12 | 0.490 | −18.71 | 61.83 | |
| WNPEC | 17.64 | 14.85 | 0.638 | −21.97 | 57.25 | |
| WPEC | MPEC | −13.13 | 14.08 | 0.788 | −50.91 | 24.65 |
| MNPEC | 8.43 | 9.35 | 0.804 | −16.26 | 33.13 | |
| WNPEC | 4.51 | 8.91 | 0.957 | −18.94 | 27.96 | |
| MNPEC | MPEC | −21.56 | 15.12 | 0.490 | −61.83 | 18.71 |
| WPEC | −8.43 | 9.35 | 0.804 | −33.13 | 16.26 | |
| WNPEC | −3.92 | 10.48 | 0.982 | −31.58 | 23.73 | |
| WNPEC | MPEC | −17.64 | 14.85 | 0.638 | −57.25 | 21.97 |
| WPEC | −4.51 | 8.91 | 0.957 | −27.96 | 18.94 | |
| MNPEC | 3.92 | 10.48 | 0.982 | −23.73 | 31.58 | |
| Variables and Subgroups of Participants | Mean Difference | Std. Error | Sig. | 95% Confidence Interval | |||
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| PASE leisure | |||||||
| PEC Stable Partner | PEC without Stable Partner | −1.02 | 3.10 | 0.988 | −9.21 | 7.18 | |
| NPEC Stable Partener | −16.57 * | 4.96 | 0.008 | −29.71 | −3.42 | ||
| NPEC without Stable Partener | −6.51 | 3.50 | 0.252 | −15.64 | 2.62 | ||
| PEC without Stable Partner | PEC Stable Partner | 1.02 | 3.10 | 0.988 | −7.18 | 9.21 | |
| NPEC Stable Partner | −15.55 * | 4.86 | 0.013 | −28.49 | −2.62 | ||
| NPEC without Stable Partner | −5.49 | 3.36 | 0.366 | −14.31 | 3.33 | ||
| NPEC Stable Partner | PEC Stable Partner | 16.57 * | 4.96 | 0.008 | 3.42 | 29.71 | |
| PEC without Stable Partner | 15.55 * | 4.86 | 0.013 | 2.62 | 28.49 | ||
| NPEC without Stable Partner | 10.06 | 5.12 | 0.213 | −3.47 | 23.60 | ||
| NPEC without Stable Partner | PEC Stable Partner | 6.51 | 3.50 | 0.252 | −2.62 | 15.64 | |
| PEC without Stable Partner | 5.49 | 3.36 | 0.366 | −3.33 | 14.31 | ||
| NPEC Stable Partner | −10.06 | 5.12 | 0.213 | −23.60 | 3.47 | ||
| PASE household | |||||||
| PEC Stable Partner | PEC without Stable Partner | 16.24 | 9.17 | 0.298 | −8.05 | 40.54 | |
| NPEC Stable Partener | −6.07 | 10.09 | 0.931 | −32.64 | 20.49 | ||
| NPEC without Stable Partener | 11.30 | 7.60 | 0.451 | −8.66 | 31.26 | ||
| PEC without Stable Partner | PEC Stable Partner | −16.24 | 9.17 | 0.298 | −40.54 | 8.05 | |
| NPEC Stable Partner | −22.32 | 10.46 | 0.155 | −49.99 | 5.35 | ||
| NPEC without Stable Partner | −4.95 | 8.10 | 0.928 | −26.57 | 16.67 | ||
| NPEC Stable Partner | PEC Stable Partner | 6.07 | 10.09 | 0.931 | −20.49 | 32.64 | |
| PEC without Stable Partner | 22.32 | 10.46 | 0.155 | −5.35 | 49.99 | ||
| NPEC without Stable Partner | 17.37 | 9.12 | 0.238 | −6.76 | 41.50 | ||
| NPEC without Stable Partner | PEC Stable Partner | −11.30 | 7.61 | 0.451 | −31.26 | 8.66 | |
| PEC without Stable Partner | 4.95 | 8.10 | 0.928 | −16.67 | 26.57 | ||
| NPEC Stable Partner | −17.37 | 9.12 | 0.238 | −41.50 | 6.76 | ||
| PASE Total | |||||||
| PEC Stable Partner | PEC without Stable Partner | 15.23 | 9.86 | 0.418 | −10.83 | 41.28 | |
| NPEC Stable Partener | −22.64 | 13.60 | 0.351 | −58.61 | 13.32 | ||
| NPEC without Stable Partener | 4.80 | 8.76 | 0.947 | −18.20 | 27.79 | ||
| PEC without Stable Partner | PEC Stable Partner | −15.23 | 9.86 | 0.418 | −41.28 | 10.83 | |
| NPEC Stable Partner | −37.87 * | 13.46 | 0.034 | −73.57 | −2.17 | ||
| NPEC without Stable Partner | −10.44 | 8.55 | 0.616 | −33.13 | 12.26 | ||
| NPEC Stable Partner | PEC Stable Partner | 22.64 | 13.60 | 0.351 | −13.32 | 58.61 | |
| PEC without Stable Partner | 37.87 * | 13.46 | 0.034 | 2.17 | 73.57 | ||
| NPEC without Stable Partner | 27.43 | 12.68 | 0.148 | −6.30 | 61.17 | ||
| NPEC without Stable Partner | PEC Stable Partner | −4.80 | 8.76 | 0.947 | −27.79 | 18.20 | |
| PEC without Stable Partner | 10.44 | 8.55 | 0.616 | −12.26 | 33.13 | ||
| NPEC Stable Partner | −27.43 | 12.69 | 0.148 | −61.7 | 6.30 | ||
| Model | Unstandardised Coefficients | Standardised Coefficients | t | Sig. | ||
|---|---|---|---|---|---|---|
| B | Std. Error | Beta | ||||
| 1 | (Constant) | 18.669 | 25.872 | 0.722 | 0.472 | |
| Age | −0.469 | 0.329 | −0.141 | −1.425 | 0.158 | |
| DASS depresion | 0.295 | 0.778 | 0.038 | 0.380 | 0.705 | |
| EC Participation/non participation | 4.474 | 4.342 | 0.112 | 1.031 | 0.305 | |
| Sex | −1.920 | 3.767 | −0.047 | −0.510 | 0.612 | |
| Friends | 4.691 | 4.008 | 0.114 | 1.170 | 0.245 | |
| Reading, studying | −2.324 | 3.909 | −0.058 | −0.595 | 0.554 | |
| Watching TV, listening to music | −5.982 | 5.932 | −0.099 | −1.008 | 0.316 | |
| Going to cultural events | 1.270 | 4.809 | 0.030 | 0.264 | 0.792 | |
| Walks, trips | 13.462 | 4.295 | 0.336 | 3.134 | 0.002 | |
| Sports | 1.581 | 5.866 | 0.026 | 0.269 | 0.788 | |
| Hobbies | 8.745 | 6.053 | 0.153 | 1.445 | 0.152 | |
| 2 | (Constant) | 19.299 | 25.632 | 0.753 | 0.453 | |
| Age | −0.479 | 0.325 | −0.145 | −1.475 | 0.144 | |
| DASS depresion | 0.289 | 0.774 | 0.037 | 0.374 | 0.709 | |
| EC Participation/non participation | 4.959 | 3.916 | 0.124 | 1.266 | 0.209 | |
| Sex | −1.891 | 3.746 | −0.046 | −0.505 | 0.615 | |
| Friends | 4.730 | 3.985 | 0.115 | 1.187 | 0.238 | |
| Reading, studying | −2.049 | 3.748 | −0.051 | −0.547 | 0.586 | |
| Watching TV, listening to music | −5.883 | 5.891 | −0.097 | −0.999 | 0.321 | |
| Walks, trips | 13.764 | 4.119 | 0.343 | 3.342 | 0.001 | |
| Sports | 1.534 | 5.834 | 0.025 | 0.263 | 0.793 | |
| Hobbies | 8.746 | 6.022 | 0.153 | 1.452 | 0.150 | |
| 3 | (Constant) | 20.120 | 25.315 | 0.795 | 0.429 | |
| Age | −0.477 | 0.323 | −0.144 | −1.475 | 0.144 | |
| DASS depresion | 0.275 | 0.768 | 0.036 | 0.358 | 0.721 | |
| EC Participation/non participation | 5.100 | 3.860 | 0.127 | 1.321 | 0.190 | |
| Sex | −2.000 | 3.705 | −0.049 | −0.540 | 0.591 | |
| Friends | 4.729 | 3.966 | 0.115 | 1.193 | 0.236 | |
| Reading, studying | −1.959 | 3.714 | −0.049 | −0.528 | 0.599 | |
| Watching TV, listening to music | −5.826 | 5.857 | −0.096 | −0.995 | 0.322 | |
| Walks, trips | 13.959 | 4.032 | 0.348 | 3.462 | 0.001 | |
| Hobbies | 8.940 | 5.947 | 0.157 | 1.503 | 0.136 | |
| 4 | (Constant) | 23.252 | 23.642 | 0.984 | 0.328 | |
| Age | −0.508 | 0.310 | −0.153 | −1.638 | 0.105 | |
| EC Participation/non participation | 5.369 | 3.768 | 0.134 | 1.425 | 0.157 | |
| Sex | −1.936 | 3.684 | −0.048 | −0.526 | 0.600 | |
| Friends | 4.447 | 3.868 | 0.108 | 1.150 | 0.253 | |
| Reading, studying | −1.918 | 3.695 | −0.048 | −0.519 | 0.605 | |
| Watching TV, listening to music | −5.236 | 5.594 | −0.086 | −0.936 | 0.352 | |
| Walks, trips | 13.739 | 3.966 | 0.343 | 3.464 | 0.001 | |
| Hobbies | 8.396 | 5.723 | 0.147 | 1.467 | 0.146 | |
| 5 | (Constant) | 23.551 | 23.545 | 1.000 | 0.320 | |
| Age | −0.541 | 0.302 | −0.163 | −1.792 | 0.076 | |
| EC Participation/non participation | 5.251 | 3.747 | 0.131 | 1.401 | 0.164 | |
| Sex | −1.970 | 3.669 | −0.048 | −0.537 | 0.593 | |
| Friends | 4.343 | 3.849 | 0.106 | 1.128 | 0.262 | |
| Watching TV, listening to music | −5.057 | 5.562 | −0.083 | −0.909 | 0.366 | |
| Walks, trips | 13.745 | 3.951 | 0.343 | 3.479 | 0.001 | |
| Hobbies | 7.754 | 5.567 | 0.136 | 1.393 | 0.167 | |
| 6 | (Constant) | 20.322 | 22.680 | 0.896 | 0.372 | |
| Age | −0.539 | 0.301 | −0.163 | −1.792 | 0.076 | |
| EC Participation/non participation | 5.062 | 3.717 | 0.126 | 1.362 | 0.176 | |
| Friends | 3.957 | 3.767 | 0.097 | 1.051 | 0.296 | |
| Watching TV, listening to music | −4.752 | 5.513 | −0.078 | −0.862 | 0.391 | |
| Walks, trips | 14.115 | 3.876 | 0.352 | 3.642 | 0.000 | |
| Hobbies | 7.462 | 5.520 | 0.131 | 1.352 | 0.180 | |
| 7 | (Constant) | 15.720 | 22.014 | 0.714 | 0.477 | |
| Age | −0.591 | 0.294 | −0.178 | −2.009 | 0.047 | |
| EC Participation/non participation | 5.622 | 3.655 | 0.140 | 1.538 | 0.127 | |
| Friends | 3.539 | 3.731 | 0.086 | 0.949 | 0.345 | |
| Walks, trips | 14.263 | 3.867 | 0.356 | 3.688 | 0.000 | |
| Hobbies | 6.481 | 5.394 | 0.114 | 1.202 | 0.232 | |
| 8 | (Constant) | 17.401 | 21.931 | 0.793 | 0.429 | |
| Age | −0.574 | 0.294 | −0.173 | −1.953 | 0.054 | |
| EC Participation/non participation | 6.056 | 3.624 | 0.151 | 1.671 | 0.098 | |
| Walks, trips | 15.098 | 3.764 | 0.377 | 4.011 | 0.000 | |
| Hobbies | 6.562 | 5.391 | 0.115 | 1.217 | 0.226 | |
| 9 | (Constant) | 26.330 | 20.718 | 1.271 | 0.207 | |
| Age | −0.640 | 0.289 | −0.193 | −2.214 | 0.029 | |
| EC Participation/non participation | 6.734 | 3.590 | 0.168 | 1.876 | 0.064 | |
| Walks, trips | 16.594 | 3.566 | 0.414 | 4.653 | 0.000 | |
References
- World Health Organization. Global Health and Aging. 2021. Available online: https://www.who.int/ageing/publications/global_health.pdf (accessed on 3 July 2021).
- HelpAge International Network. Global AgeWatch Index 2015. Insight Report. 2015. Available online: https://www.helpage.org/global-agewatch/reports/global-agewatch-index-2015-insight-report-summary-and-methodology/ (accessed on 3 July 2021).
- Rădoi, S.; Mondiru, D.; Logofătu, G. Projection of the Romanian Elderly Population, at Territorial Level, at the Horizon of 2060. Iagar EM, Edition Coord: Pisică, S.; Ioniță, A., Institutul National de Statistică. 2018. National Institute of Statistics, Bucharest. Available online: https://insse.ro/cms/ro/content/proiectarea-popula%C8%9Biei-v%C3%A2rstnice-rom%C3%A2niei-%C3%AEn-profil-teritorial-la-orizontul-anului-2060 (accessed on 3 July 2021).
- Eurostat. Populations Projections. Europop 2019. Population on 1 January by Age, Sex and Type of Projection. European Commission. 2019. Available online: https://ec.europa.eu/eurostat/data/database?node_code=proj (accessed on 3 July 2021).
- Matei, R.; Saghin, D.; Dumitrache, L.; Nae, M. Multidimensional Approach on Sustainability of Ageing in Romanian Residential Care Centres for Elders. Sustainability 2018, 10, 3336. [Google Scholar] [CrossRef] [Green Version]
- Hunter, W.; Wang, W.; Worsley, A. Retirement planning and expectations of Australian babyboomers: Are they ready to retire? Ann. N. Y. Acad. Sci. 2007, 1114, 267–278. [Google Scholar] [CrossRef]
- Park, J.-A.; Choi, B. Factors Affecting the Intention of Multi-Family House Residents to Age in Place in a Potential Naturally Occurring Retirement Community of Seoul in South Korea. Sustainability 2021, 13, 8922. [Google Scholar] [CrossRef]
- Eurostat. Tables by Benefits—Old Age Function. 2021. Available online: https://ec.europa.eu/eurostat/databrowser/view/spr_exp_fol/default/table?lang=en (accessed on 25 September 2021).
- Eurostat. Social Protection Statistics—Pension Expenditure and Pension Beneficiaries. 2020. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Social_protection_statistics_-_pension_expenditure_and_pension_beneficiaries (accessed on 26 September 2021).
- Institutul National de Statistica [National Institut of Statistics]. Numarul de Pensionari si Pensia Medie Lunara in Anul 2020 [The Number of Pensionars and the Medium Pension per Month in 2020]. 2021. Available online: insse.ro/cms/ro/tags/comunicat-numarul-de-pensionari-si-pensie-medie-lunara (accessed on 25 September 2021).
- European Commission. Semestrul European—Fisa Tematica. Adecvarea si Sustenabilitatea Pensiilor [European Semester—Thematic Factsheet. Adequacy and Sustainability of Pensions]. 2017. Available online: https://ec.europa.eu/info/sites/default/files/file_import/european-semester_thematic-factsheet_adequacy-sustainability-pensions_ro.pdf (accessed on 26 September 2021).
- Animasahun, V.J.; Chapman, H.J. Psychosocial health challenges of the elderly in Nigeria: A narrative review. Afr. Health Sci. 2017, 17, 575–583. [Google Scholar] [CrossRef]
- Mondor, L.; Maxwell, C.J.; Hogan, D.B.; Bronskill, S.E.; Gruneir, A.; Lane, N.E.; Wodchis, W.P. Multimorbidity and healthcare utilization among home care clients with dementia in Ontario, Canada: A retrospective analysis of a population-based cohort. PLoS Med. 2017, 14, e1002249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Research Council. Grand Challenges of Our Aging Society: Workshop Summary; Smith, A., Ed.; Center for Economic, Governance, and International Studies, Division of Behavioral and Social Sciences and Education; The National Academies Press: Washington, DC, USA, 2010. [Google Scholar]
- Lyons, A.; Alba, B.; Heywood, W.; Fileborn, B.; Minichiello, V.; Barrett, C.; Hinchliff, S.; Malta, S.; Dow, B. Experiences of ageism and the mental health of older adults. Aging Ment. Healths 2018, 22, 1456–1464. [Google Scholar] [CrossRef]
- Martins, R.; Neto, M.J.; Andrade, A.; Albuquerque, C. Abuse and maltreatment in the elderly. Aten. Primaria 2014, 46 (Suppl. 5), 206–209. [Google Scholar] [CrossRef] [Green Version]
- Zaidi, A.; Gasior, K.; Hofmarcher, M.M.; Lelkes, O.; Marin, B.; Rodrigues, R.; Schmidt, A.; Vanhuysse, P.; Zólyomi, E. Active Ageing Index 2012. Concept, Methodology and Final Results. 2012. Available online: https://www.euro.centre.org/downloads/detail/1542 (accessed on 3 July 2021).
- United Nations Economic Commission of Europe (2018) Active Ageing Index. Analytical Report. Available online: https://unece.org/fileadmin/DAM/pau/age/Active_Ageing_Index/ACTIVE_AGEING_INDEX_TRENDS_2008-2016_web_with_cover.pdf (accessed on 3 July 2021).
- Hallal, P.C.; Andersen, L.B.; Bull, F.C.; Guthold, R.; Haskell, W.; Ekelund, U.; Group LPASW. Global physical activity levels: Surveillance progress, pitfalls, and prospects. Lancet 2012, 380, 247–257. [Google Scholar] [CrossRef]
- Franco, M.R.; Tong, A.; Howard, K.; Sherrington, C.; Ferreira, P.H.; Pinto, R.Z.; Ferreira, M.L. Older people’s perspectives on participation in physical activity: A systematic review and thematic synthesis of qualitative literature. Br. J. Sports Med. 2015, 49, 1268–1276. [Google Scholar] [CrossRef]
- Rada, C. Spending leisure time when approaching retirement and during retirement. J. Phychol. 2018, 64, 15. [Google Scholar]
- Baert, V.; Gorus, E.; Mets, T.; Geerts, C.; Bautmans, I. Motivators and barriers for physical activity in the oldest old: A systematic review. Ageing Res. Rev. 2011, 10, 464–474. [Google Scholar] [CrossRef] [PubMed]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.; Martin, B.W.; Lancet Physical Activity Series Working Group. Correlates of physical activity: Why are somes people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Moschny, A.; Platen, P.; Klaassen-Mielke, R.; Trampisch, U.; Hinrichs, T. Barriers to physical activity in older adults in Germany: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 121. [Google Scholar] [CrossRef] [Green Version]
- Chávez-Moreno, D.V.; Infante-Sierra, H.; Serralde-Zúñiga, A.E. Sarcopenia y funcionalidad en el adulto mayor hospitalizado [Sarcopenia and functionality in elderly inpatient]. Nutr. Hosp. 2015, 31, 1660–1666. [Google Scholar] [CrossRef] [PubMed]
- Bembom, O.; van der Laan, M.; Haight, T.; Tager, I. Leisure-time physical activity and all-cause mortality in an elderly cohort. Epidemiology (Cambridge Mass.) 2009, 20, 424–430. [Google Scholar] [CrossRef] [Green Version]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Fiatarone Singh, M.A.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and Physical Activity for Older Adults. Med. Sci. Sports Exerc. 2009, 41, 1510–1530. [Google Scholar] [CrossRef]
- McPhee, J.S.; French, D.P.; Jackson, D.; Nazroo, J.; Pendleton, N.; Degens, H. Physical activity in older age: Perspectives for healthy ageing and frailty. Biogerontology 2016, 17, 567–580. [Google Scholar] [CrossRef]
- Thomas, E.; Battaglia, G.; Patti, A.; Brusa, J.; Leonardi, V.; Palma, A.; Bellafiore, M. Physical activity programs for balance and fall prevention in elderly: A systematic review. Medicine 2019, 98, e16218. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Argüelles, E.L.; Rodríguez-Mansilla, J.; Antunez, L.E.; Garrido-Ardila, E.M.; Muñoz, R.P. Effects of dancing on the risk of falling related factors of healthy older adults: A systematic review. Arch. Gerontol. Geriatr. 2015, 60, 1–8. [Google Scholar] [CrossRef]
- Li, J.; Hsu, C.C.; Lin, C.T. Leisure Participation Behavior and Psychological Well-Being of Elderly Adults: An Empirical Study of Tai Chi Chuan in China. Int. J. Environ. Res. Public Health 2019, 16, 3387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Verghese, J.; Lipton, R.B.; Katz, M.J.; Hall, C.B.; Derby, C.A.; Kuslansky, G.; Ambrose, A.F.; Sliwinski, M.; Buschke, H. Leisure activities and the risk of dementia in the elderly. N. Engl. J. Med. 2003, 348, 2508–2516. [Google Scholar] [CrossRef] [Green Version]
- Nilsson, I.; Häggström Lundevaller, E.; Fisher, A.G. The Reationship between Engagement in Leisure Activities and Self-Rated Health in Later Life. Act. Adapt. Aging 2017, 41, 175–190. [Google Scholar] [CrossRef]
- Almeida, O.P. Prevention of depression in older age. Maturitas 2014, 79, 136–141. [Google Scholar] [CrossRef]
- Casey, D.A. Depression in Older Adults: A Treatable Medical Condition. Prim. Care 2017, 44, 499–510. [Google Scholar] [CrossRef]
- De Oliveira, L.; Souza, E.C.; Rodrigues, R.; Fett, C.A.; Piva, A.B. The effects of physical activity on anxiety, depression, and quality of life in elderly people living in the community. Trends Psychiatry Psychother. 2019, 41, 36–42. [Google Scholar] [CrossRef]
- Beattie, E.; Pachana, N.; Franklin, S.J.; Franklin, S.J. Double jeopardy: Comorbid anxiety and depression in late life. Res. Gerontol. Nurs. 2010, 3, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Uchmanowicz, I.; Gobbens, R.J. The relationship between frailty, anxiety and depression, and health-related quality of life in elderly patients with heart failure. Clin. Interv. Aging 2015, 10, 1595–1600. [Google Scholar] [CrossRef] [Green Version]
- Andreescu, C.; Lee, S. Anxiety Disorders in the Elderly. Adv. Exp. Med. Biol. 2020, 1191, 561–576. [Google Scholar]
- Mohammadpour, A.; Sadeghmoghadam, L.; Shareinia, H.; Jahani, S.; Amiri, F. Investigating the role of perception of aging and associated factors in death anxiety among the elderly. Clin. Interv. Aging 2018, 13, 405–410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Billot, M.; Calvani, R.; Urtamo, A.; Sánchez-Sánchez, J.L.; Ciccolari-Micaldi, C.; Chang, M.; Roller-Wirnsberger, R.; Wirnsberger, G.; Sinclair, A.; Vaquero-Pinto, N.; et al. Preserving Mobility in Older Adults with Physical Frailty and Sarcopenia: Opportunities, Challenges, and Recommendations for Physical Activity Interventions. Clin. Interv. Aging 2020, 15, 1675–1690. [Google Scholar] [CrossRef] [PubMed]
- Böhm, A.W.; Mielke, G.I.; da Cruz, M.F.; Ramirez, V.V.; Wehrmesister, F.C. Social Support and Leisure-Time Physical Activity Among the Elderly: A Population-Based Study. J. Phys. Act. Health 2016, 13, 599–605. [Google Scholar] [CrossRef]
- Fulbright, S.A. Rates of depression and participation in senior centre activities in community-dwelling older persons. J. Psychiatr. Ment. Health Nurs. 2010, 17, 385–391. [Google Scholar] [CrossRef]
- Hadley, R. It’s most of my life—going to the pub or the group: The social networks of involuntarily childless older men. Ageing Soc. 2021, 41, 51–76. [Google Scholar] [CrossRef] [Green Version]
- Wright, M.R.; Brown, S.L. Psychological Well-Being among Older Adults: The Role of Partnership Status. J. Marriage Fam. 2017, 79, 833–849. [Google Scholar] [CrossRef]
- Broese van Groenou, M.; te Riele, S.; de Jong Gierveld, J. Receiving Support and Care in Older Age: Comparing LAT Relationships With First Marriages, Remarriages, and Cohabitation. J. Fam. Issues 2019, 40, 1786–1807. [Google Scholar] [CrossRef]
- Tasfiliz, D.; Selcuk, E.; Gunaydin, G.; Slatcher, R.B.; Corriero, E.F.; Ong, A.D. Patterns of perceived partner responsiveness and well-being in Japan and the United States. J. Fam. Psychol. 2018, 32, 355–365. [Google Scholar] [CrossRef] [Green Version]
- Caicedo-Velásquez, B.; Restrepo-Méndez, M.C. The role of individual, household, and area of residence factors on self-rated health in Colombian adults: A multilevel study. Efecto de las condiciones individuales, del hogar y del área de residencia en la autopercepción de su salud en adultos colombianos: Un estudio multinivel. Biomédica 2020, 40, 296–308. [Google Scholar] [CrossRef] [PubMed]
- Bolszak, S.; Casartelli, N.C.; Impellizzeri, F.M.; Maffiuletti, N.A. Validity and reproducibility of the Physical Activity Scale for the Elderly (PASE) questionnaire for the measurement of the physical activity level in patients after total knee arthroplasty. BMC Musculoskelet. Disord. 2014, 15, 46. [Google Scholar] [CrossRef] [Green Version]
- Curcio, F.; Liguori, I.; Cellulare, M.; Sasso, G.; Della-Morte, D.; Gargiulo, G.; Testa, G.; Cacciatore, F.; Bonaduce, D.; Abete, P. Physical Activity Scale for the Elderly (PASE) Score Is Related to Sarcopenia in Noninstitutionalized Older Adults. J. Geriatr. Phys. Ther. 2019, 42, 130–135. [Google Scholar] [CrossRef] [PubMed]
- Svege, I.; Kolle, E.; Risberg, M.A. Reliability and validity of the Physical Activity Scale for the Elderly (PASE) in patients with hip osteoarthritis. BMC Musculoskelet. Disord. 2012, 13, 26. [Google Scholar] [CrossRef] [Green Version]
- New England Research Institutes. Physical Activity Scale for the Elderly. Administration and Scoring Instruction Manual. NERI. 1991. Available online: https://meetinstrumentenzorg.nl/wp-content/uploads/instrumenten/PASE-handl.pdf (accessed on 25 January 2021).
- Psychology Fundation of Australia. Depression, Anxiety and Stress Scale. 2018. Available online: http://www2.psy.unsw.edu.au/dass/ (accessed on 25 January 2021).
- Howell, D.C. Statistical Methods for Psychology, 8th ed.; Chapter 2.5. Describing Distributions; Cengage Learning: Wadsworth, OH, USA, 2013; pp. 27–29. [Google Scholar]
- Morgan, G.A.; Leech, N.L.; Gloeckner, G.W.; Barrett, K.C. IBM SPSS for Introductory Statistics: Use and Interpretation; Chapter 3. Measurement and descriptive statistics; Routledge: New York, NY, USA, 2011; p. 52. [Google Scholar]
- Kline, R.B. Beyond Significance Testing. STATISTICS Reform in the Behavioral Sciences, 2nd ed.; Part II. Effect size estimation, Chapter 5. Continuous outcomes; American Psychological Association: Washington, DC, USA, 2013; p. 152. [Google Scholar]
- Field, A. Discovering Statistics Using SPSS, 5th ed; Chapter 12.5. Post hoc Procedures, Chapter 19.3 2. Pearson’s Chi-Square Test; Sage Publication Ltd.: London, UK, 2018; pp. 717, 1064. [Google Scholar]
- Matthews-López, L. Best Practices and Technical Issues in Cross-Lingual, Crosscultural Assessments: An Evaluation of a Test Adaptation; Chapter 3. Post-hoc Procedures; Ohio University: Athens, OH, USA, 2003; p. 99. [Google Scholar]
- Dunkler, D.; Plischke, M.; Leffondré, K.; Heinze, G. Augmented Backward Elimination: A Pragmatic and Purposeful Way to Develop Statistical Models. PLoS ONE 2014, 9, e113677. [Google Scholar]
- Taylor, D. Physical activity is medicine for older adults. Postgrad. Med. J. 2014, 90, 26–32. [Google Scholar] [CrossRef] [Green Version]
- Andrade-Gómez, E.; García-Esquinas, E.; Ortolá, R.; Martínez-Gómez, D.; Rodríguez-Artalejo, F. Watching TV has a distinct sociodemographic and lifestyle profile compared with other sedentary behaviors: A nationwide population-based study. PLoS ONE 2017, 12, e0188836. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Deluga, A.; Kosicka, B.; Dobrowolska, B.; Chrzan-Rodak, A.; Jurek, K.; Wrońska, I.; Ksykiewicz-Dorota, A.; Jędrych, M.; Drop, B. Lifestyle of the elderly living in rural and urban areas measured by the FANTASTIC Life Inventory. Ann. Agric. Environ. Med. AAEM 2018, 25, 562–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Department for Culture MaS. Adult Participation in Sport: Analysis of the Taking Part Survey. 2011. Available online: https://www.gov.uk/government/publications/adult-participation-in-sport-analysis-of-the-taking-part-survey (accessed on 3 July 2021).
- Nguyen, T.X.; Nguyen, T.X.; Pham, T.; Nguyen, C.T.; Vu, G.T.; Nguyen, L.H.; Tran, B.X.; Vu, H.; Latkin, C.A.; Ho, C.S.H.; et al. Establishing activity centers for elderly people in metropolitan areas of Vietnam: Preference and willingness-to-pay. J. Multidiscip. Healthc. 2019, 12, 795–802. [Google Scholar] [CrossRef] [Green Version]
- Notthoff, N.; Reisch, P.; Gerstorf, D. Individual Characteristics and Physical Activity in Older Adults: A Systematic Review. Gerontology 2017, 63, 443–459. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Wang, Y. The impacts of gender on seasonal retirement mobility and wellbeing. Ageing Soc. 2021, 41, 187–207. [Google Scholar] [CrossRef]
- Ong, A.D.; Uchino, B.N.; Wethington, E. Loneliness and Health in Older Adults: A Mini-Review and Synthesis. Gerontology 2016, 62, 443–449. [Google Scholar] [CrossRef]
- Holt-Lunstad, J.; Smith, T.B.; Baker, M.; Harris, T.; Stephenson, D. Loneliness and social isolation as risk factors for mortality: A meta-analytic review. Perspect. Psychol. Sci. A J. Assoc. Psychol. Sci. 2015, 10, 227–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kharicha, K.; Iliffe, S.; Harari, D.; Swift, C.; Gillmann, G.; Stuck, A.E. Health risk appraisal in older people 1: Are older people living alone an ‘at-risk’ group? Br. J. Gen. Pract. 2007, 57, 271–276. [Google Scholar]
- Ožic, S.; Vasiljev, V.; Ivkovic, V.; Bilajac, L.; Rukavina, T. Interventions aimed at loneliness and fall prevention reduce frailty in elderly urban population. Medicine 2020, 99, e19145. [Google Scholar] [CrossRef] [PubMed]
- Sugisawa, H.; Sugihara, Y.; Kobayashi, E.; Fukaya, T.; Liang, J. The influence of lifecourse financial strains on the later-life health of the Japanese as assessed by four models based on different health indicators. Ageing Soc. 2019, 39, 2631–2652. [Google Scholar] [CrossRef] [Green Version]
- Westerhof, G.J.; Miche, M.; Brothers, A.F.; Barrett, A.E.; Diehl, M.; Montepare, J.M.; Wahl, H.W.; Wurm, S. The influence of subjective aging on health and longevity: A meta-analysis of longitudinal data. Psychol. Aging 2014, 29, 793–802. [Google Scholar] [CrossRef] [PubMed]
- Jylhä, M. What is self-rated health and why does it predict mortality? Towards a unified conceptual model. Soc. Sci. Med. 2009, 69, 307–316. [Google Scholar] [CrossRef]
- Benyamini, Y.; Blumstein, T.; Murad, H.; Lerner-Geva, L. Changes over time from baseline poor self-rated health: For whom does poor self-rated health not predict mortality? Psychol. Health 2011, 26, 1446–1462. [Google Scholar] [CrossRef]
- Elsawy, B.; Higgins, K.E. Physical activity guidelines for older adults. Am. Fam. Physician 2010, 81, 55–59. [Google Scholar]
- Nguyen-Michel, V.H.; Pallanca, O.; Brion, A.; Vecchierini, M.F. Les habitudes de vie et de sommeil chez les patients âgés insomniaques [Sleep habits and lifestyle of elderly patients with insomnia] [Les habitudes de vie et de sommeil chez les patients âgés insomniaques]. Soins. Gerontol. 2019, 24, 38–42. [Google Scholar] [CrossRef]
- Bardach, S.H.; Schoenberg, N.E. The Role of Primary Care Providers in Encouraging Older Patients to Change Their Lifestyle Behaviors. Clin. Gerontol. 2018, 41, 326–334. [Google Scholar] [CrossRef]
- Vasiliadis, H.M.; Gontijo Guerra, S.; Berbiche, D.; Pitrou, I.E. The Factors Associated with 3-Year Mortality Stratified by Physical and Mental Multimorbidity and Area of Residence Deprivation in Primary Care Community-Living Older Adults. J. Aging Health 2021, 33, 545–556. [Google Scholar] [CrossRef]
- Moussavi, S.; Chatterji, S.; Verdes, E.; Tandon, A.; Patel, V.; Ustun, B. Depression, chronic diseases, and decrements in health: Results from the World Health Surveys. Lancet 2007, 370, 851–858. [Google Scholar] [CrossRef]
- Petkus, A.J.; Wetherell, J.L.; Stein, M.B.; Chavira, D.A.; Craske, M.G.; Sherbourne, C.; Sullivan, G.; Bystritsky, A.; Roy-Byrne, P. Age Differences in Death and Suicidal Ideation in Anxious Primary Care Patients. Clin. Gerontol. 2018, 41, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Byeon, H. Relationship between Physical Activity Level and Depression of Elderly People Living Alone. Int. J. Environ. Res. Public Health 2019, 16, 4051. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosulwit, L. Mental health status, including depression and quality of life among members of an elderly club in suburban Bangkok. J. Med. Assoc. Thail. 2012, 95 (Suppl. 1), S92–S101. [Google Scholar] [CrossRef]
- Coventry, P.A.; McMillan, D.; Clegg, A.; Brown, L.; van der Feltz-Cornelis, C.A.O.; Gilbody, S.; Ali, S. Frailty and depression predict instrumental activities of daily living in older adults: A population-based longitudinal study using the CARE75+ cohort. PLoS ONE 2020, 15, e0243972. [Google Scholar]


| Socio-Demographic Data | Whole Group N = 172 | PEC N = 107 | NPEC N = 65 |
|---|---|---|---|
| Age | 71 [56–86] years | 71.1 [58–86] years | 69.66 [56–83] years |
| Sex * | |||
| Female | 65.7 | 72 | 52.3 |
| Male | 34.3 | 28 | 47.7 |
| Residence * | |||
| Urban | 100 | 100 | 100 |
| Marital status * | |||
| Married | 39.0 | 27.3 | 66.7 |
| Divorced | 15.1 | 18.2 | 7.8 |
| Widowed | 39.5 | 47.9 | 19.6 |
| Single | 3.5 | 4.1 | 2.0 |
| Concubine | 2.9 | 2.5 | 3.9 |
| Stable life partner | 44.8 | 33.9 | 70.6 |
| Without stable life partner | 55.2 | 66.1 | 29.4 |
| Education * | |||
| Primary school | 1.7 | 0.8 | 3.9 |
| Lower secondary school | 26.7 | 28.9 | 21.6 |
| Upper secondary school | 23.3 | 24.8 | 19.6 |
| Foreman school in a profession/post-secondary | 19.2 | 16.5 | 25.5 |
| University degree | 27.3 | 27.3 | 27.5 |
| Other | 1.7 | 1.7 | 2.0 |
| Personal monthly income ** | |||
| Less than or equal to RON 1000 (EUR 209) | 17.4 | 21.5 | 7.8 |
| Between RON 1001–2000 (EUR 209–418) | 54.7 | 53.7 | 56.9 |
| Between RON 2001–3000 (EUR 418–628) | 20.3 | 17.4 | 27.5 |
| Between RON 3001–4000 (EUR 628–837) | 1.7 | 0.8 | 3.9 |
| Above RON 4000 (Above EUR 837) | 2.3 | 2.5 | 2.0 |
| Non answer | 3.5 | 4.1 | 2.0 |
| Health-Related Items | Treatment Received for Chronic Condition | Recommended Changes in Lifestyle | Implemented Recommended Changes | ||
|---|---|---|---|---|---|
| PEC | |||||
| Spearman’s rho | Self-reported health | 0.237 * | 0.216 * | −0.274 ** | |
| p | 0.014 | 0.025 | 0.004 | ||
| N | 107 | 107 | 107 | ||
| Treatment received for chronic condition | 0.263 ** | −0.265 ** | |||
| p | 0.006 | 0.003 | |||
| N | 107 | 107 | |||
| Recommended changes in lifestyle | −0.837 ** | ||||
| p | 0.000 | ||||
| N | 107 | ||||
| NPEC | |||||
| Spearman’s rho | Self-reported health | 0.508 ** | 0.276 * | −0.277 * | |
| p | 0.000 | 0.026 | 0.025 | ||
| N | 65 | 65 | 65 | ||
| Treatment received for chronic condition | 0.416 ** | −0.397 ** | |||
| p | 0.001 | 0.001 | |||
| N | 65 | 65 | |||
| Recommended changes in lifestyle | −0.890 ** | ||||
| p | 0.000 | ||||
| N | 65 | ||||
| Levene’s Test for Equality of Variances | t-Test for Equality of Means | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| F | Sig. | t | df | Sig. (2-tailed) | Mean Difference | Std. Error Difference | 95% Confidence Interval of the Difference | ||
| Lower | Upper | ||||||||
| PASE_leisure | 21.029 | 0.000 | −2.932 | 170 | 0.004 | −9.51 | 3.242 | −15.925 | −3.12 |
| −3.350 | 168.450 | 0.001 | −9.51 | 2.842 | −15.125 | −3.902 | |||
| PASE_household | 1.788 | 0.183 | −0.086 | 170 | 0.932 | −0.55 | 6.342 | −13.072 | 11.982 |
| −0.088 | 145.433 | 0.930 | −0.55 | 6.192 | −12.792 | 11.702 | |||
| PASE_Total | 4.371 | 0.038 | −1.272 | 170 | 0.205 | −10.06 | 7.913 | −25.683 | 5.558 |
| −1.357 | 161.188 | 0.177 | −10.06 | 7.417 | −24.709 | 4.584 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urzeala, C.; Popescu, V.; Courteix, D.; Mitrache, G.; Roco, M.; Teodorescu, S. Barriers and Facilitators for the Romanian Older Adults in Enjoying Physical Activity Health-Related Benefits. Sustainability 2021, 13, 12511. https://doi.org/10.3390/su132212511
Urzeala C, Popescu V, Courteix D, Mitrache G, Roco M, Teodorescu S. Barriers and Facilitators for the Romanian Older Adults in Enjoying Physical Activity Health-Related Benefits. Sustainability. 2021; 13(22):12511. https://doi.org/10.3390/su132212511
Chicago/Turabian StyleUrzeala, Constanta, Veronica Popescu, Daniel Courteix, Georgeta Mitrache, Mihaela Roco, and Silvia Teodorescu. 2021. "Barriers and Facilitators for the Romanian Older Adults in Enjoying Physical Activity Health-Related Benefits" Sustainability 13, no. 22: 12511. https://doi.org/10.3390/su132212511