1. Introduction
Historically, people have traveled to other geographical destinations for medical treatment not available at home since ancient times. Health-improving trips have been popular since the earliest times of Greek, Romanian, and Chinese civilizations [
1]. Recently, the convergence of healthcare and tourism has become a profitable new service industry from the supply side with the ability to provide medical treatment and tourism attractions to other geographical destinations, and, at the same time, from the demand side, to have diverse experiences with the cultural and technological differences along with medical care. Medical care has successfully been packaged into much more customized tourism products and marketed to cross-border consumers in both developed and developing countries. Thus, medical tourism has become a growing new blue ocean, global niche market with a high sustainability value, especially for the leaders of developing countries. Due to the strong ethnic ties and cultural background in Central Asia, Uzbekistan has also promoted the medical and recreational industry as the 6th industry, combined with medical technologies, providing medical services as well as entertaining tourism experiences, to boost the national economy. Based on the Decree of the President on complex measures for radical enhancement of the healthcare system and the Concept of Health System Development in the years 2019–2025 [
2], the Uzbekistani government has promoted the emerging subcategory of medical tourism by the essential legislative base, and the organizational changes to support this new sector of the 6th industry to be one of the leading medical tourism players in Central Asia.
Nonetheless, compared to this ambitious goal, the current status of the medical industry in Uzbekistan is not satisfactory and thus the mission to be a medical hub has become much tougher over time. As shown in
Figure 1, the gap between the number of inbound and outbound medical tourists has not been significantly reduced, while the total number of patients is increasing [
3,
4]. Even worse, during the period 2016 to 2018, there were more outbound tourists than inbound tourists. The number of inbound tourists visiting Uzbekistan for treatment purposes doubled after the governmental initiatives for medical tourism in 2017 and 2018, but at the same time, the outbound visitors increased much more sharply in 2018, resulting in a narrower gap between the inbound and outbound medical tourists.
As shown in
Figure 2, there were 55,490 inbound tourists who came to the country for treatment purposes in 2019, and 37,168 outbound tourists visited other medical tourism destinations. In other words, over time, more Uzbekistan patients are preferring to going abroad even if it is financially burdensome. This result implies that the local healthcare system and supporting policy measures lack sustainable governance. Here, governance is defined as the workable mechanism for sustainable performance [
5]. It could be a negative signal for the Uzbekistani medical industry because it loses competitiveness, resulting in a continuous outflow of foreign currency. Thus, our research question arises in terms of why government policies result in a lack of governance: Is it feasible for the Uzbekistani government to provide good governance to create a medical hub in central Asia? To answer this research question, it is very important to evaluate the patients’ needs in deciding on medical tourism abroad and to suggest sustainable governance issues for the medical policy measures. That is the purpose of our research. We shall evaluate the decision criteria for outbound Uzbekistani patients to get a glimpse of the sustainable governance issues and find the implications and suggestions from these governance issues shown in the empirical results.
The unique contributions of this study are summarized as follows. First, very few studies have been conducted on sustainable governance for potential tourists deciding on medical tourism. As mentioned above, Uzbekistani people prefer going abroad to obtain medical services to domestic medical services. Therefore, the empirical results of this study may explain how and what factors make Uzbekistani people go overseas for medical tourism. Second, by incorporating perceived value as a mediating variable, we analyze and compare both direct and indirect models, such that they will clarify the role of patients’ perceived value as the modulator on sustainable governance. Implications from this empirical result shall shed the light for policymakers on the governance of the policy measures.
The remainder of this paper is structured as follows.
Section 2 reviews the related literature concerning the medical tourism industry;
Section 3 develops hypotheses and presents methodology and data.
Section 4 presents the empirical results of the study. Finally,
Section 5 summarizes the implications of the research and offers insightful policy suggestions.
2. Conceptual Characteristics of Medical Tourism
Researchers in medical tourism marketing and management elucidate the diverse issues existing in this relatively new scientific field. In most cases, the research is focused on the demand side of marketing activities. Connell [
6] defined medical tourism as a subcategory of tourism where traveling for treatment is voluntary with a mass tourism nature, and the main flows of foreign patients come from diasporic communities or neighboring countries due to the psychological safety, implying that private information is important in this highly risky tourism. Bookman and Bookman [
7] described medical tourism as an economic phenomenon with a fusion provision of health and concierge services to foreigners, with more focus on the tourism factors. The World Tourism Organization defines medical tourism as a subset of tourism that entails the utilization of evidence-based medical resources and services (both invasive and non-invasive) and includes diagnosing, treating, curing, preventing, and rehabilitating procedures at the core of medical tourism [
8]. All these demand-oriented studies focus on the satisfaction with medical tourism from consumer perspectives. As another approach on the supply side of medical tourism, the suppliers of medical services offer excellent quality of medical care and tourism activities for foreign visitors to the international market, generating diverse sources of revenues and encouraging the growth of concierge businesses. The marketing strategies of those suppliers are based on the prediction of peoples’ service desires in terms of medical factors, and research on the decision-making processes or purchase intention.
In this study, we define medical tourism as a convenient provision of integrated medical and tourism services to international visitors and, thus, we focus on the purchase intention from the suppliers’ perspective, and on the satisfaction of the medical patients from the marketing or demand perspectives. It sheds light on the effect of policy measures on the internal capacity of the medical tourism industry as well as the surrounding conditions of medical tourism. It results in an insightful evaluation of the sustainable governance of the policy measures for the medical tourism industry.
Based on the literature review on medical tourism as the combination of two-dimensional services of healthcare services and entertaining tourism experiences, we evaluate the main influential factors predicting the willingness to obtain foreign medical services in the following section. Most of the papers in the field of medical tourism used the supply side of medical factors as a push variable, and the demand side of tour factors as a pull variable. In particular, medical tourism should be based on the harmonized cooperation between the host country hospitals, host country government’s promotional policies, and easy access to medical tourism in the home country of the patients, resulting in the importance of a global public and private partnership (PPP) [
9]. In general, due to the perceived difference in the quality of medical services between home and host countries, the patients may choose medical tourism, if the host country is physically or psychologically close to the home country. However, the medical factor is not a unique factor, of course, because one of the best benefits from medical tourism is the entertaining sightseeing in the host country. It is very feasible for patients to go far away from the home country if the host country also provides UNESCO heritage sites, famous amusement parks, and entertaining grand hotels. Of course, medical tourism is still expensive and somewhat luxurious services with high risks are involved in the medical treatment, and thus information sharing for reliable medical tourism is the core of medical tourism, implying the important role of information sharing for sustainable governance in a PPP. Thus, based on the common factors of these integrated studies on medical tourism, our research model evaluates the three-dimensional factors of medical factors, tourism factors, and information sharing factors as the input variables, and the selection process of each variable for this research is explained in the following section, based on the comparison of the previous studies on medical tourism.
3. Theoretical Framework and Hypotheses
To study the factors influencing patients to search for international medical services, we decided to develop our theoretical model based on the most widely used model for the explanation of the push and pull concept of tourists’ motivation, introduced by Dann [
10]. Push factors describe people’s inner forces to travel, while pull factors cause people to go on trips, caused by external forces generated by the tourism destination’s attractiveness. A systematic review of medical tourism literature by Hanefeld et al. [
11] confirms the popularity of investigating medical tourists’ decisions on international travel from the perspective of the push and pull concept. In medical tourism research, the push and pull factors studied have included accessibility [
12,
13], the cost of desired healthcare [
14,
15], safety and security [
7,
16], and knowledge and awareness of the country [
13,
14]. In the present study, we develop survey constructs referring to the abovementioned literature.
3.1. Medical Factors
Medical factors imply diverse aspects related to the quality of medical services, the cost of treatment, the reputation of the hospital, severity of illness, etc. Concerning each factor explaining medical factors, the quality of medical services is one of the most significant and common components in medical tourism services [
6,
17,
18]. In general, patients will decide whether they take the local treatment or go abroad based on this level of medical service. The cost-effectiveness of medical services is regarded as one of the determining factors to choose a medical tourism destination [
17,
19]. Since the medical cost could be burdensome for patients compared with the local treatment, whether it is affordable or not is crucial for medical tourism abroad. The reputation of medical services is also an important factor in choosing the destination of medical tourism because medical tourism abroad involves much higher risks compared with local treatment [
20]. Zhang and Lee [
21] argue that the reputation of the medical facilities in a host country is the strongest determinant of the intentions for medical tourism. Cham et al. [
22] found hospital branding as an influential factor in increasing the reputation of hospitals and trustworthiness for medical tourists, resulting in a positive influence on behavioral intention. Adams et al. [
23] argued that the complexity of the disease is the determining factor in choosing a special hospital in the host country of the medical tourism destination, where the patients can get appropriate, precise treatment in time. Zhang and Lee [
21] found that people with serious diseases considering medical treatment prefer healthcare services in economically advanced countries, while respondents considering treatment for relatively minor diseases choose countries with a low psychological distance. Based on these previous studies, we chose four items, service quality, cost competitiveness, facility level, and seriousness of illness, to assess medical factors in medical tourism (see
Appendix A). These medical factors generally showed a positive relation to behavioral intention or a customer’s perceived value in previous studies [
20,
21,
24].
3.2. Tourism Factors
If the medical factors are the internal condition of patients to undertake medical tourism, diverse tourism factors could consist of the environmental conditions of medical tourism for patients to choose special destinations as the host country [
7]. Though medical tourists consider the medical treatment to be most important, the environmental conditions surrounding medical tourism may boost the sufficient condition for tourists’ willingness to visit specific destinations for medical tourism [
25]. In particular, when we consider sustainable governance of medical tourism, the tourism factors are important to create the overall perceived value coming from the hospitality of the host country. Therefore, to represent the hospitality of the host country with pleasant memories, tourism factors may include almost all aspects of satisfying factors.
Based on the selective concentration among the potential variables, the tourism factors in our research consist of four elements: the attractiveness of the destination, infrastructure, accessibility of the country, and safety [
25]. The attractiveness of a location is frequently referred to as the customer’s perception of a destination’s capability to meet their requirements for travel [
26], which includes all forms of attractions, such as historical and cultural attractions, tangible and non-tangible values, natural and anthropogenic resources, national cuisine and music, etc. Infrastructure means facilities such as roads and housing, airports, water supply, and energy-generating capacity, and easy access to all these infrastructures [
7]. Johnson et al. [
27] argued the importance of continuous diplomatic relationships and the provision of an effective medical visa issuing process for medical tourists to gain easy access to the country, and Sonmez and Graefe [
28] insisted that safety is a critical factor in host country selection. Based on these arguments, our research model is based on these four items to assess tourism factors (see
Appendix A). Generally, tourism factors play an important role in the behavioral intention of medical tourists to go abroad [
20] and loyalty [
29].
3.3. Information Sharing
Since medical tourism involves many organizations and agents, information sharing is much more important in the decision for patients to go overseas than use local treatment. Information sharing is a transmission of data through all existing channels, such as the internet, public announcements, and viral communications with others, as an essential factor for medical tourists to become accustomed to the medical destination and its facilities. Tai [
30] argued that information sharing is very influential on the formation of good relationships in business interactions and helpful for customer loyalty. The importance of information sharing by medical intermediaries at all medical service provision stages has been mentioned in many studies [
31,
32], and this value is usually significant for behavioral intention or satisfaction [
33,
34]. The value of provided data to medical tourists, based on the easy, effective, and reliable access to full information sources online and offline, is also significant in the decision-making process for medical tourism [
31]. In particular, the reliability of information providers, such as official medical institutions, promotional materials, facilitators, friends, and family, and trustworthiness in the context of the provided information are also regarded as crucial factors in choosing a medical destination. Based on these arguments, four items, easy and convenient access, trust in the provider, trustworthiness of the provided information, and quality of information, are used to assess medical factors (see
Appendix A).
3.4. Behavioral Intention
Since we do not collect the data from the medical tourists who have previously undertaken medical tourism, our research is based on the future intention to take a medical trip if all the conditions of the survey match with their level of expectation. Thus, the behavioral intention to undertake medical tourism is our output or dependent variable of the empirical model for medical tourism. Here, behavioral intention is defined as a patient’s willingness to engage in a particular behavior and make plans for an actual medical tour in the future. Most studies on medical tourism support that the predictive nature of behavioral intention can be found in the causal relationship with satisfaction or loyalty [
29], service quality [
21,
24], quality of e-health services [
32], perceived value, and overall satisfaction [
17,
19,
24]. Thus, it is used as a dependent variable for this research as well in that we evaluate medical tourists’ willingness in terms of the subjective intention level of predisposition, confidence in visiting, and the level of recommendation to others.
3.5. Perceived Value as a Mediator
Most survey-based research uses perceived value as a mediator because medical tourism consists of complicated procedures for patients to decide on the compromise between the benefits and risks of going overseas [
34,
35,
36,
37,
38,
39,
40]. In this decision process, the most important mediator is the perceived values created by all the push and pull factors for good governance on the networking of the activities of the PPP. Perceived value could be defined as a unique psychological construct actively stimulating a potential customer to choose a favorable good or service, and the driving power of value perception generates a strong confidence level for clients in preferable decision making [
37]. In general, it has been evaluated in terms of functional or utilitarian performance with cost, time, and efforts before, during, or after utilizing the services or products [
35]. Therefore, many studies have used perceived value to explore tourists’ behavioral intentions, such as satisfaction [
35,
37,
38] and loyalty [
39,
40]. Perceived value, in particular, takes a mediating role between independent variables and dependent variables in many tourism research areas [
30,
35,
37], supporting the feasibility of this study’s model.
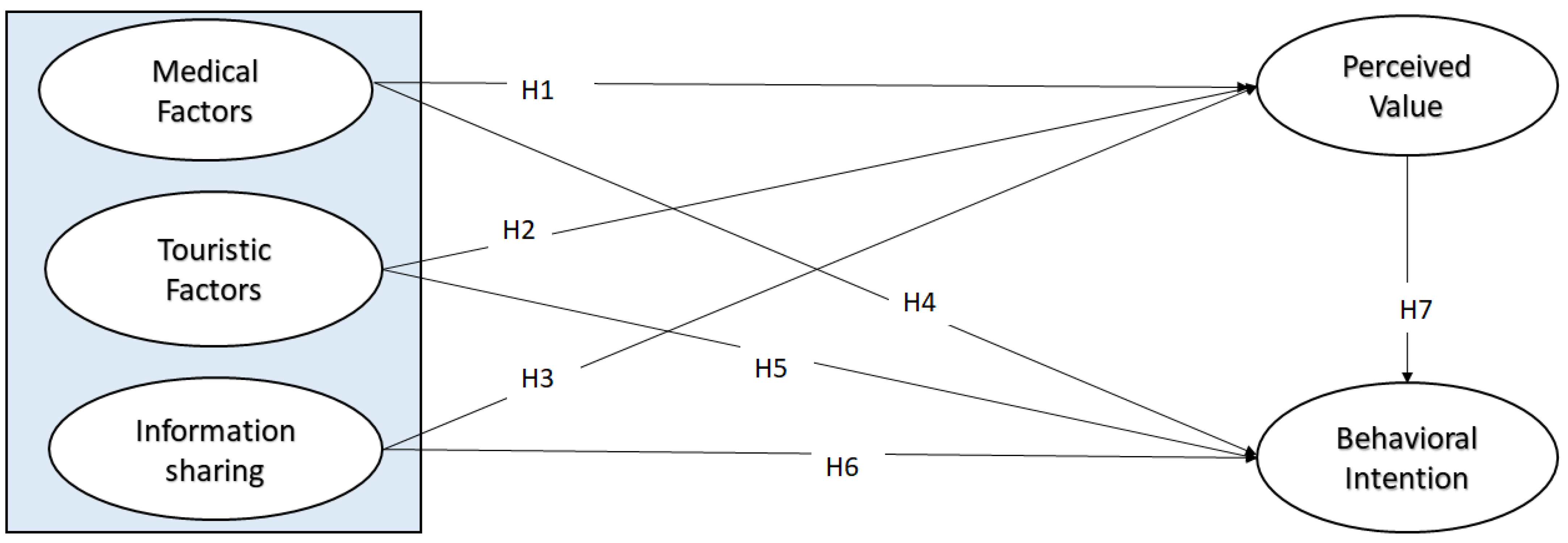
Therefore, based on the arguments for these three independent variables, one mediating variable, and one dependent variable with their causal relations, the following seven hypotheses are empirically tested.
Hypothesis 1 (H1). The medical factors positively impact behavioral intention.
Hypothesis 2 (H2). The tourism factors positively impact behavioral intention.
Hypothesis 3 (H3). Information sharing positively impacts behavioral intention.
Hypothesis 4 (H4). Information sharing positively impacts the perceived value.
Hypothesis 5 (H5). The medical factors positively impact the perceived value.
Hypothesis 6 (H6). The tourism factors positively impact the perceived value.
Hypothesis 7 (H7). The perceived value positively impacts behavioral intention.
Figure 3 presents our research model framework of the abovementioned hypotheses. We set perceived value as the mediating variable of medical factors, tourism factors, and information sharing inputs, and ascertain whether it reacts with the behavioral intention. Therefore, in this research, we postulate the above hypotheses with behavioral intention (direct model) and perceived value as the mediator (indirect model).
3.6. Data Collection and Methodology
The constructs for the questionnaire were adopted from different studies. Medical factors representing the key construct of medical quality were empirically investigated in many studies [
19,
20,
21]; treatment cost is considered as an important factor [
7,
15,
20]; hospital reputation is also an important factor, as reiterated in several papers [
12,
22]; illness severity is one the determinants of choosing specific treatment abroad [
21,
23]. Constructs for tourism factors are developed using constructs from previous research, including attractiveness of the destination [
15,
18,
21]; infrastructure [
15]; accessibility of the country [
18]; safety [
18]. Information sharing factors consist of accessibility of information [
20,
30]; reliability of information providers [
30,
40]; reliability of content; sufficiency of information [
40]. The construct of perceived value is represented by functional value [
38,
39]; emotional value [
40]; informational value [
25]. Constructs for behavioral intention consist of predisposition [
21,
35,
36,
37]; confidence [
21,
35]; recommendation [
19,
21].
For the purpose of the evaluation of our theoretical suggestions on medical tourism, we developed a questionnaire survey. All the constructs were adapted from the observed literature. For a better fit to the objective of this study, some modifications were made. The original construct items were developed in English. The native researcher translated the questionnaire into Uzbek, then it was translated from Uzbek into English by a professional interpreter according to the back-translation method [
41]. The researchers who are native in Uzbek and fluent in English compared the translations of both interpretations and they did not find any significant difference influencing the meaning. The survey was converted into an electronic version and posted on Google Forms. The pilot testing of the questionnaire was carried out by posting the link to this survey in an Uzbekistani graduate students’ Telegram group for those studying in Korea. The pilot study outcomes from thirty students showed that all the constructs in the questionnaire were relevant, unambiguous, and the translation was clear; thus, the validity of all variables in the study was determined.
The gathering process of Uzbekistani citizens’ responses was done from 15 December 2020 to 25 January 2021. We shared the link of this survey on social media outlets, such as Facebook, Telegram, and IMO, randomly to people living in different regions of Uzbekistan who had the intention to obtain treatment abroad, and sent it directly to patients who obtained treatment abroad; these contacts were obtained from a medical agency coordinator. Additionally, the sample was collected without any preconditions, such as age, geographical region, ethnic background, or income. We received 568 questionnaire responses and, after removing 70 unusable or inappropriate responses, 498 questionnaires were finally obtained. In
Table 1, the number of participating female and male respondents is almost equal, at 51% and 49%, respectively. Since we can see the highest percentage of 40% among the 20–30 age group, a strong potential group for medical tourism, it seemed appropriate to carry out an empirical test on the respondents. The full data according to the socio-demographic characteristics are shown in
Table 1.
We adopted a seven-point Likert scale, ranging from 1 (“entirely disagree”) to 7 (“entirely agree, in this study.
Appendix A presents detailed measurement items. For the structural equation modeling (SEM) with survey questionnaires, SPSS22.0 and AMOS22.0 were used to assess hypotheses about the relationship between variables.
4. Empirical Results and Its Implications
4.1. Reliability Test
For the appropriateness of the variable selection with the questions on the survey, we used the goodness-of-fit statistical test. The goodness-of-fit test is a set of various measures defining the appropriateness of the sample’s data to the given theoretical distribution, which examines the difference between observed values and expected values in hypothesis testing. In SEM, due to presence of statistical error, we used several statistical dimensions to evaluate the model appropriateness at the same time. The appropriateness of a model as a whole is measured by different goodness-of-fit indices recommended by many researchers, such as descriptive measures of overall model fit: the root mean of the square error of approximation (RMSEA), incremental goodness-of-fit index (IFI); descriptive measures based on model comparisons: goodness-of-fit index (GFI), comparative goodness-of-fit index (CFI) [
42,
43,
44]. The measurement model in terms of GFI is an acceptable fit as the value of the goodness-of-fit indices of both models (direct and indirect) and thus it showed a good model fit with the recommended guidelines. The CFI indicator of both models was also over 0.9, implying the model fit was acceptable as well. The results of the abovementioned goodness-of-fit test are shown in
Table 2.
The proposed model must be reliable and valid for statistical fidelity as well. For the purpose of reliability, we used Cronbach’s alpha coefficient, the corrected item-total correlation coefficient, and the composite reliability coefficient. The Cronbach’s alpha coefficient helped us to check the internal consistency of items in each variable set. It should be over 0.6. The corrected item-total correlation coefficient proves that items of each variable are correlated and it should be over 0.5. The composite reliability coefficient measuring internal consistency in scale items was applied to overcome the Cronbach’s alpha coefficient’s limitation which underestimates the reliability of latent variables. The consistency feature of reliability should stay stable when the study is conducted under the same conditions. The reliability test coefficients were over 0.6, 0.5, and 0.7, respectively, as shown in
Table 3, surpassing the advised cut-off points and indicating that inter-correlation was satisfied within the items in every set of variables.
Additionally, we conducted exploratory factor analysis (EFA) for the following reasons. First of all, to reduce the number of variables, arranging them from high to low. Secondly, to establish the underlying dimensions between measured variables and constructs and, finally, to provide construct validity evidence. Two important aspects of EFA are the Kaiser–Meyer–Olkin (KMO) index and Bartlett’s test of sphericity. KMO is a measure of sampling adequacy that is recommended for checking the case to variable ratio for the analysis being conducted. While the KMO ranges from 0 to 1, it is generally accepted when it is more than 0.6. Bartlett’s test of sphericity is related to the significance of the study and thereby shows the validity and suitability of the responses collected to the problem being addressed throughout the study. It can test whether the correlation matrix is an identity matrix or not and, hence, would suggest if the factor model is an appropriate one or not. For factor analysis to be considered suitable, Bartlett’s test of sphericity must be less than 0.05. According to the EFA result, all indices met the above requirements, implying that all factors explained the variable well and there was no need to reduce factors.
4.2. Validity Test
The rationality of proper usage of the variable measures was tested by validity checking. The sub-components of each factor, representativeness of the concepts in the survey, and concept validity were checked by validity analysis [
45].
For assessment of the good representation of measured variables in constructs, we used confirmatory factor analysis (CFA). If the estimation of the standardized factor loadings (SFL) and the average variance extracted (AVE) of the sub-components are remarkably higher than the 0.5 cut-off point with their relative constructs, then we can confirm the convergent validity of items [
45]. The convergent validity results were obtained with CFA. As shown in
Table 4, all factor loadings and AVEs for all components were significantly higher than 0.5, implying the strong convergent validity of the measurement scale.
The estimation number of the standardized factor loadings (SFLs) should be statistically above 0.5, as recommended by Fornell and Larcker [
46]. At this point, the convergent validity of the constructs is evaluated using the average variance extracted (AVE). As shown in
Table 4, the AVEs of the four constructs (tourism factors, information sharing, perceived value, and behavioral intention) are all above the critical value of 0.5. Although medical factors show the AVE value to be less than 0.5, the convergent validity of the construct could be adequate when the composite reliability meets the acceptable level of 0.6 [
42]. Therefore, we accepted the AVE result of the medical factor which was less than 0.5 Thus, we confirm that the convergent reliability of the constructions was acceptable. Meanwhile, the square root of the AVE for the constructs was greater than any of the corresponding inter-construct correlations, indicating that discriminant validity was accomplished as well. This discriminant validity is shown in
Table 5.
4.3. Structural Model Results
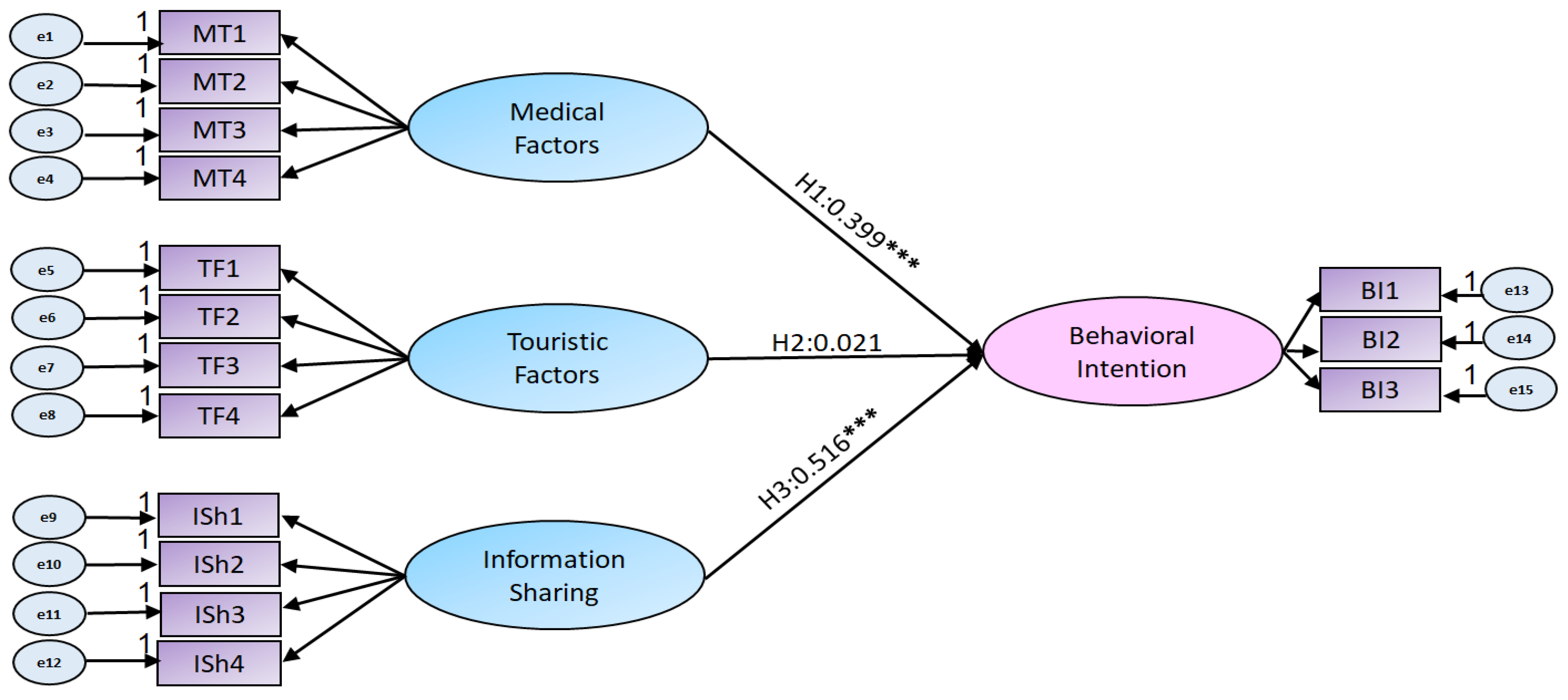
The result of the direct model, which excludes the mediator of perceived value, is shown in
Figure 4. In this direct model, the causal relationship of three independent variables of medical factors, tourism factors, and information sharing are tested with the final dependent variable of behavioral intention. At 99% statistical significance level, medical factors (H1) and information sharing (H3) show a strongly significant influence on behavioral intention with a coefficient value of 0.399 and 0.516, respectively. This implies these two factors are primary or necessary factors to undertake medical tourism. This result is coherent with previous studies exploring the relationship between two factors and behavioral intention [
20,
21,
24]. Meanwhile, the tourism factor (H2) is rejected due to its impact on behavioral intention. This result indicates initial success in medical tourism can be promoted by the medical factors and information sharing, while tourism factors are not influential, at least in the initial stage of medical tourism. For most cases from Uzbekistan, patients take a medical tour to neighboring countries, such as Russia, due to the fact that they speak the language and due to psychological intimacy, implying that they are not concerned with sightseeing during the medical tour, as shown in
Figure 4. Since many previous studies have shown a positive relation between touristic factors and behavioral intention [
15,
21], this result presents unique implications which are discussed in the following section.
In order to evaluate the role of the mediating effect, we compare the statistical significance of the input variables in the direct model with the indirect model. Here, input variables must meet the next conditions for the full mediating effects: they must be strongly related to the mediating variable and influence them significantly; then the effect of the independent variables on the dependent variables must weaken due to the existence of the mediator. According to Baron and Kenny [
47], the direct effect of the input variables on the final output variable must disappear or be statistically insignificant due to the full mediation via the mediator. When all conditions are met, the influence of the independent variables is presumed to be “completely” or “fully” dependent on the mediator. However, if the mediator satisfies all conditions, but the effect on the dependent variable is still significant, it is said to be “partially mediated” [
48].
We tested the indirect model of the causal relationship between the three independent variables and behavioral intention by using the stepwise mediator variable of “perceived value”. First of all, as shown in
Figure 5 and
Table 6, we could see that perceived value and behavioral intention have a strong significant relation (H7). This result is coherent with previous studies [
35,
37]. Since H7 was supported, we could examine the mediating effect.
Information sharing (H3) directly and positively influences the behavioral intention (p < 0.1) and has a considerable positive effect on perceived value (p < 0.01). This result implies that information sharing is “partially mediated” by perceived value. It directly influences the behavioral intention, as well as indirectly via the mediator of perceived value, implying that Uzbekistani patients do not expect a high level of subjective satisfaction coming from the perceived value.
In contrast to information sharing, medical factors (H4) show a significant and positive impact on perceived value after the advent of perceived value, while the direct influence on the behavioral intention (H1 is rejected. This means that perceived value takes a “full mediating role” between medical factors and behavioral intention. As shown in
Figure 5, patients from Uzbekistan undertake medical tourism with much focus on medical factors via perceived values. The lack of the touristic factors’ impact on medical tourism implies that medical tourism in Uzbekistan is in its initial stage, going abroad for medical treatment, at most; patients are not concerned about sightseeing in another country, because most of those patients go to Russia (32% in
Figure 1), and they think they are familiar with this psychologically neighboring country. Interestingly, similar to the direct model, the tourism factor (H2) did not show a positive impact on perceived value, which is a different result from previous studies [
15,
21] that support a positive relation between the two variables.
4.4. Discussion and Policy Implications
Based on the empirical result of this study, we found that medical tourism can be promoted by medical factors and information sharing, while tourism factors are not influential, at least in the initial stage of medical tourism. Since two positive factors show a high coefficient value, policy support for these two variables should be strengthened. The promotion policies in the medical industries as well as the positive openness of developing countries such as Uzbekistan will bring successful medical tourism. At the same time, it implies that the qualitative gap of medical services between home and host countries for Uzbekistani patients is so huge that it promotes medical tourism abroad. The Uzbekistani government should make more practical efforts to enhance the level of medical factors. Due to the massive requirement for investment in the medical industry, it cannot be carried out in a short time, but if the Uzbekistani government specializes in some strategic fields of medical services by “selective concentration”, there might be a good chance to become a customized hub for that field of medical tourism. In contrast to these two variables, unfortunately, we found that tourism factors are not very influential for patients going overseas. When patients in developing countries such as Uzbekistan consider medical tourism, the tourism benefits, such as heritage sightseeing or adventure attractions, may not be a necessary condition, but just sufficient or additional conditions only. Even if many developing countries are emphasizing their tourism advantages with strong promotional efforts, the efforts of the government are not sustainable at all, at least in medical tourism, and thus the core factors of the workable mechanism of medical tourism, from a tourism perspective, should be more precisely adjusted towards convenient, comfortable trips, rather than luxurious package tours, as the 6th industry of promotional activities. The insignificance of tourism factors for medical tourists is consistent with the outcome of the study of Wang et al. [
20], confirming no influential relationship between tourism attractions and the intention to revisit. Wang et al. explained this result with the specific purpose of medical tourists traveling abroad. While vacation travelers look for leisure activities in the foreign country they want to go to, medical tourists search for necessary treatment abroad wherever they can. The essentiality of medical services for medical tourists puts their priorities in medical tourism factors. After satisfaction with medical services as the primary need for traveling, medical tourists can enjoy touristic attractiveness.
Meanwhile, in the process of policy implementation, it should be noted that medical services are also services, and thus must be approached in terms of patients’ subjective evaluation. Hence, patients’ perceived value could have a key role in making medical services successful in a more sustainable way. For this sustainable governance, we further examined the path analysis with indirect effects of this perceived value to ascertain its role as the mediator.
From this process, we could find that information sharing is “partially mediated” by perceived value. Therefore, objective information coming from friends or reliable SNS may guarantee convenient and trustworthy medical services even under much lower or negligible perceived value. Unfortunately, this information sharing is partially mediated by the perceived value, implying that the perceived value from medical tourism is much lower or negligible. To promote the sustainable performance of medical tourism, information sharing should be fully mediated by the perceived value [
34]. For this purpose, the government should provide easy and reliable access to information to create value from this information sharing. For example, the government may create inbound/outbound public websites for medical tour initiatives with diverse sponsorships by public support for transportation, the visa process, easy access to the home/host country hospitals, etc. This convenient and reliable access to information is crucial for Uzbekistan to be a medical tourism hub in Central Asia. To create more perceived value from information sharing, the government may invite individual bloggers to spread this medical tourism information with reliable video and text content authorized by the government, and advise private medical tour agencies and hospitals to use real-time chatbots and virtual reality technology on their web sites and social media. All these efforts will form and increase the perceived value which directly strengthens behavioral intention as the full mediator to achieve sustainable governance for medical tourism. Meanwhile, we found that perceived value takes a “full mediating role” between medical factors and behavioral intention. Therefore, the Uzbekistani medical industry could and should enhance the overall quality of medical services in terms of the level of doctors and medical infrastructure, which can increase patients’ trust and satisfaction. A higher quality of medical services could narrow the gap between the advantages of medical tourism abroad, resulting in better recruitment of inbound medical tourists in Uzbekistan. Interestingly, the tourism factor did not show a positive impact on perceived value. This implies that Uzbekistani patients totally ignore the enjoyment of tours when they go abroad for medical services. This may stem from the fact that many of them have an operation to cure a serious illness. Therefore, we may suggest that for inbound medical tourism promotion, the advantages of the tourism factors should not be necessary. Instead, the government should make more effort not for tourist attractions, but for the competitiveness of the medical factors, such as customized treatment and/or selective concentration on the strategic field of medical tourism.
5. Conclusions
Under the much closer global economy with the WTO, it has become a natural trend for patients to choose medical services regardless of national boundaries. In particular, patients from developing countries proactively go abroad for better medical services. In Uzbekistan, this trend is much stronger. In 2018, the number of outbound tourists was much larger than that of inbound tourists, implying that Uzbekistani people prefer foreign medical services to domestic medical treatment. Despite this negative situation, Uzbekistan is trying to be a hub of medical tourism in Central Asia. Therefore, understanding Uzbekistani patients’ needs concerning medical tourism is a very important task for this mission, because inbound and outbound medical tourists are just two sides of the same coin. In this research, we analyzed how the three factors of medical, tourism, and information sharing variables influence the behavioral intention via the perceived value as the mediator for potential Uzbekistani patients. The main findings and implications are summarized as follows.
First, in the indirect model, among the three independent variables, the information sharing and medical factors are very important factors with a high coefficient value of 0.516 and 0.399, respectively. In contrast to these two factors, the tourism factor is identified as unnecessary, but has sufficient or additional influence on behavioral intention, implying no need to boost the tourism advantages at the initial stage, at least for the medical tourism industry.
Second, in the indirect model, we find that perceived value takes a fully mediating role between medical factors and behavioral intention and takes a partially mediating role between information sharing and behavioral intention, implying that more effort in information sharing is desperately needed for Uzbekistan to be a medical hub. Convenient and reliable access to information about medical tourism shall certainly enhance the perceived value in the collaborative networks of the PPP on medical tourism. In this perspective of information sharing, government initiative is very important, at least at the initial stage to become a medical hub for developing countries [
49]. However, this does not mean the government should take all the responsibility, because our research shows the most important factors to be the medical factors, and thus the PPP among all the related parties should proactively participate in advanced medical services for sustainable governance.
This study may have some limitations to explore, especially in the COVID-19 pandemic era. We could not test Uzbekistani inbound medical tourists in South Korea due to the pandemic situation and restrictions on cross-border travel. This situation limited the complete knowledge of medical tourists’ behavioral intentions towards international medical destinations. In the era of COVID-19, all international travel, including medical tours, have been suspended for a while, and the industry has been changing rapidly to reflect this “untact” era. However, it has many insightful lessons for medical tourism. For example, New York City has announced that it will give a free vaccine for COVID-19 to all international tourists as a new proposal for this pandemic era. This kind of new proposal certainly encourages tourists to consider medical tourism besides holidays. By the same token, if any country guarantees safer, better sightseeing incentives with medical treatment, certainly many patients from developing countries, including Uzbekistan, would take this kind of new of protected medical tourism as well. This kind of proposal will certainly improve the implications and suggestions of our research in the future.
Author Contributions
The authors contributed to each part of the paper by: conceptualization, Y.C.; methodology and software, H.L.; validation, Z.A.; formal analysis, H.L.; investigation, Z.A.; resources and data collection, Z.A.; writing—original draft preparation, Z.A.; writing—review and editing, Y.C. and H.L.; supervision, Y.C.; project administration, Y.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
- I.
Factors influencing for behavioral intention of prosperous medical tourists.
Please select the number according to the 7-point scale:
1 Strongly Disagree, 2 Disagree; 3 Somewhat Disagree; 4 Neutral; 5 Somewhat Agree; 6 Agree; 7 Strongly Agree.
| Questions | Strongly Disagree…… Neutral …… Strongly Agree |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 |
| Medical factors |
| I expect the medical treatment level abroad to be much better than in Uzbekistan. (Service quality) | | | | | | | |
| I expect the cost of medical treatment to be “relatively” competitive considering the high level of medical performance. (Cost-competitiveness) | | | | | | | |
| The desired country has many international standard hospitals with board certified doctors and advanced technologies. (Facility level) | | | | | | | |
| I want to go abroad because my medical difficulty is serious. (Seriousness of illness) | | | | | | | |
| Tourism factors |
| The destination country may provide a variety of cultural and recreational attractions. | | | | | | | |
| Transportation, shopping opportunities, and accommodation are well developed in the destination country. | | | | | | | |
| Getting a medical visa and travel support is easy and reliable for the destination country. | | | | | | | |
| In general, there are no social and political risks in the destination country. | | | | | | | |
| Information sharing factors |
| It was easy and convenient to get the medical tourism information. (Easy and convenient access) | | | | | | | |
| I highly trust the information provider, which is my friend, agency, or the internet. (Trust in provider) | | | | | | | |
| Information on medical tourism from the above provider is reliable and trustworthy. (Trustworthiness of the provided information) | | | | | | | |
| The information I get from my provider is enough to make a decision. (Quality of information) | | | | | | | |
| Perceived value |
| I expect much better medical treatment in foreign countries compared to Uzbekistan. | | | | | | | |
| I will get high cultural enjoyment on the visit from famous tourism destinations during my medical trip. | | | | | | | |
| I am satisfied with the information on the real medical conditions abroad, because it will be equal to the real medical performance over there. | | | | | | | |
| I will be satisfied in my choice on the destination country for my medical trip. | | | | | | | |
| Behavioral intention |
| I am eager to travel to a foreign country to receive my medical treatment in the near future. | | | | | | | |
| I may choose the same medical tour again in the case of other illnesses in the future. | | | | | | | |
| I strongly recommend the country to others for their medical tourism. | | | | | | | |
| | | | | | | | | | | | | | |
References
- Medical-Tourism. History of Medical Tourism—From Ancient Times until Today. Available online: https://www.health-tourism.com/medical-tourism/history/ (accessed on 9 May 2021).
- УП-5590-сoн 07.12.2018. О Кoмплексных Мерах пo Кoреннoму Сoвершенствoванию Системы Здравooхранения Республики Узбекистан. Available online: https://www.lex.uz/docs/4096199 (accessed on 5 May 2021).
- Social Protection, Rights of Mothers and Children. The State Committee of Republic of Uzbekistan. Available online: https://stat.uz/uz/rasmiy-statistika/social-protection-2 (accessed on 13 May 2021).
- Main Health Indicators. Open Data Portal of the Republic of Uzbekistan. Available online: https://data.gov.uz/ru/datasets/13717 (accessed on 14 May 2021).
- Choi, Y. Regional Cooperation for the Sustainable Development and Management in Northeast Asia. Sustainability 2018, 10, 548. [Google Scholar] [CrossRef] [Green Version]
- Connell, J. Contemporary Medical Tourism: Conceptualisation, Culture and Commodification. Tour. Manag. 2013, 34, 1–13. [Google Scholar] [CrossRef]
- Bookman, M.Z.; Bookman, K.R. Medical Tourism in Developing Countries; Palgrave Macmillan: New York, NY, USA, 2007. [Google Scholar] [CrossRef]
- World Tourism Organization. Exploring Health Tourism—Executive Summary; World Tourism Organization: Madrid, Spain, 2018. [Google Scholar] [CrossRef]
- Medhekar, A. Government Policy Initiatives for Developing Sustainable Medical Tourism Industry. Gstf J. Bus. Rev. 2014, 3, 11. [Google Scholar] [CrossRef]
- Dann, G.M. Anomie, ego-enhancement and tourism. Ann. Tour. Res. 1977, 4, 184–194. [Google Scholar] [CrossRef]
- Hanefeld, J.; Smith, R.; Horsfall, D.; Lunt, N. What do we know about medical tourism? A review of the literature with discussion of its implications for the UK National Health Service as an example of a public health care system. J. Travel Med. 2014, 21, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.M.; Cham, T.H.; Sia, B.C. Medical tourists’ behavioral intention in relation to motivational factors and perceived image of the service providers. Int. Acad. J. Organ. Behav. Hum. Resour. Manag. 2018, 5, 1–16. [Google Scholar]
- Kim, S.S.; Lee, C.K.; Klenosky, D.B. The influence of push and pull factors at Korean national parks. Tour. Manag. 2003, 24, 169–180. [Google Scholar] [CrossRef]
- Musa, G.; Thirumoorthi, T.; Doshi, D. Travel behaviour among inbound medical tourists in Kuala Lumpur. Curr. Issues Tour. 2012, 15, 525–543. [Google Scholar] [CrossRef]
- Collins, A.; Medhekar, A.; Wong, H.Y.; Cobanoglu, C. Factors Influencing Outbound Medical Travel from the USA. Tour. Rev. 2019, 74, 463–479. [Google Scholar] [CrossRef] [Green Version]
- Awadzi, W.; Panda, D. Medical Tourism: Globalization and the marketing of medical services. Consort. J. Hosp. Tour. 2006, 11, 75–81. [Google Scholar]
- Jaapar, M.; Musa, G.; Moghavvemi, S.; Saub, R. Dental tourism: Examining tourist profiles, motivation and satisfaction. Tour. Manag. 2017, 61, 538–552. [Google Scholar] [CrossRef]
- Fetscherin, M.; Stephano, R.M. The medical tourism index: Scale development and validation. Tour. Manag. 2016, 52, 539–556. [Google Scholar] [CrossRef]
- Han, H.; Hyun, S.S. Customer Retention in the Medical Tourism Industry: Impact of Quality, Satisfaction, Trust, and Price Reasonableness. Tour. Manag. 2015, 46, 20–29. [Google Scholar] [CrossRef]
- Wang, J.H.; Feng, H.; Wu, Y. Exploring Key Factors of Medical Tourism and Its Relation with Tourism Attraction and Re-Visit Intention. Cogent Soc. Sci. 2020, 6. [Google Scholar] [CrossRef]
- Zhang, J.; Lee, H. A Study of Factors Influencing Chinese Customer Intention to Select an International Medical Tourism Destination. Korean J. Bus. Adm. 2015, 28, 1703–1723. [Google Scholar]
- Cham, T.H.; Cheng, B.L.; Low, M.P.; Cheok, J.B.C. Brand Image as the Competitive Edge for Hospitals in Medical Tourism. Eur. Bus. Rev. 2020, 33. [Google Scholar] [CrossRef]
- Adams, E.K.; Houchens, R.; Wright, G.E.; Robbins, J. Predicting Hospital Choice for Rural Medicare Beneficiaries: The Role of Severity of Illness. Health Serv. Res. 1991, 26, 583–612. [Google Scholar] [PubMed]
- Manaf, N.H.A.; Hussin, H.; Kassim, P.N.J.; Alavi, R.; Dahari, Z. Medical Tourism Service Quality: Finally Some Empirical Findings. Total Qual. Manag. Bus. Excel. 2015, 26, 1017–1028. [Google Scholar] [CrossRef]
- Tang, J.C.S.; Rochananond, N. Attractiveness as a Tourist Destination: A Comparative Study of Thailand and Selected Countries. Socioecon. Plann. Sci. 1990, 24, 229–236. [Google Scholar] [CrossRef]
- Hu, Y.; Ritchie, J.B. Measuring Destination Attractiveness: A Contextual Approach. J. Travel Res. 1993, 32, 25–34. [Google Scholar]
- Johnson, T.J.; Youngquist, J.S.; Garman, A.N.; Hohmann, S.; Cieslak, P.R. Factors Influencing Medical Travel into the United States. Int. J. Pharm. Healthc. Mark. 2015, 9, 118–135. [Google Scholar] [CrossRef]
- Sönmez, S.F.; Graefe, A.R. Influence of Terrorism Risk on Foreign Tourism Decisions. Ann. Tour. Res. 1998, 25, 112–144. [Google Scholar] [CrossRef] [Green Version]
- Mahmud, M.S.; Rahman, M.M.; Lima, R.P.; Annie, E.J. Outbound Medical Tourism Experience, Satisfaction and Loyalty: Lesson from a Developing Country. J. Hosp. Tour. Insights 2020. [Google Scholar] [CrossRef]
- Tai, Y.M. Perceived Value for Customers in Information Sharing Services. Ind. Manag. Data Syst. 2011, 111, 551–569. [Google Scholar] [CrossRef]
- Medhekar, A. The Role of Social Media for Knowledge Dissemination in Medical Tourism. Med. Tour. 2017, 132–161. [Google Scholar] [CrossRef]
- Hadwich, K.; Georgi, D.; Tuzovic, S.; Büttner, J.; Bruhn, M. Perceived Quality of E-Health Services: A Conceptual Scale Development of e-Health Service Quality Based on the C-OAR-SE Approach. Int. J. Pharm. Healthc. Mark. 2010, 4, 112–136. [Google Scholar] [CrossRef] [Green Version]
- Alghizzawi, M.; Habes, M.; Salloum, S.A. The Relationship Between Digital Media and Marketing Medical Tourism Destinations in Jordan: Facebook Perspective. Adv. Intell. Syst. Comput. 2020, 1058, 438–448. [Google Scholar] [CrossRef]
- Medhekar, A.; Wong, H.Y.; Hall, J.E. Health-Care Providers Perspective on Value in Medical Travel to India. Tour. Rev. 2020, 75, 717–731. [Google Scholar] [CrossRef]
- Wu, H.C.; Li, T.; Li, M.Y. A Study of Behavioral Intentions, Patient Satisfaction, Perceived Value, Patient Trust and Experiential Quality for Medical Tourists. J. Qual. Assur. Hosp. Tour. 2016. [CrossRef]
- Chaulagain, S.; Pizam, A.; Wang, Y. An integrated behavioral model for medical tourism: An American perspective. J. Travel Res. 2021, 60, 761–778. [Google Scholar] [CrossRef]
- Wang, H.Y. Value as a Medical Tourism Driver. Manag. Serv. Qual. 2012, 22, 465–491. [Google Scholar] [CrossRef]
- Petrick, J.F. Development of a Multi-Dimensional Scale for Measuring the Perceived Value of a Service. J. Leis. Res. 2002, 34, 119–134. [Google Scholar] [CrossRef]
- Yang, Z.; Peterson, R.T. Customer Perceived Value, Satisfaction, and Loyalty: The Role of Switching Costs. Psychol. Mark. 2004, 21, 799–822. [Google Scholar] [CrossRef] [Green Version]
- Pandža Bajs, I. Tourist Perceived Value, Relationship to Satisfaction, and Behavioral Intentions: The Example of the Croatian Tourist Destination Dubrovnik. J. Travel Res. 2015, 54, 122–134. [Google Scholar] [CrossRef]
- Brislin, R.W. Back-translation for cross-cultural research. J. Cross-Cult. Psychol. 1970, 1, 185–216. [Google Scholar] [CrossRef]
- Schermelleh-Engel, K.; Moosbrugger, H.; Müller, H. Evaluating the Fit of Structural Equation Models: Tests of Significance and Descriptive Goodness-of-Fit Measures. Mpr-Online 2003, 8, 23–74. [Google Scholar]
- Gerbing, D.W.; Anderson, J.C. Monte Carlo Evaluations of Goodness of Fit Indices for Structural Equation Models. Sociol. Methods Res. 1992, 21, 132–160. [Google Scholar] [CrossRef]
- Mulaik, S.A.; James, L.R.; Van Alstine, J.; Bennett, N.; Lind, S.; Stilwell, C.D. Evaluation of Goodness-of-Fit Indices for Structural Equation Models. Psychol. Bull. 1989, 105, 430–445. [Google Scholar] [CrossRef]
- Choi, Y.; Yu, Y. The Influence of Perceived Corporate Sustainability Practices on Employees and Organizational Performance. Sustainability 2014, 6, 348–364. [Google Scholar] [CrossRef] [Green Version]
- Fornell, C.; Larcker, D.F. Evaluating Structural Equation Models with Unobservable Variables and Measurement Error. J. Mark. Res. 1981, 18, 39. [Google Scholar] [CrossRef]
- Baron, R.M.; Kenny, D.A. The Moderator-Mediator Variable Distinction in Social Psychological Research. Conceptual, Strategic, and Statistical Considerations. J. Pers. Soc. Psychol. 1986, 51, 1173–1182. [Google Scholar] [CrossRef] [PubMed]
- Judd, C.M.; Kenny, D.A. Estimating Mediation in Treatment Evaluations CHARLES. Eval. Rev. 1981, 5, 602–619. [Google Scholar] [CrossRef]
- Allaberganov, A.; Preko, A. Inbound International Tourists’ Demographics and Travel Motives: Views from Uzbekistan. J. Hosp. Tour. Insights 2021. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}