1. Introduction
The heating, ventilation, and air-Conditioning (HVAC) system of a hospital operating theatre determines the level of sepsis that can be achieved in the surgical field [
1]. There is a correlation between ventilation systems and the degree of contamination of the surgical wound [
2,
3]. Thus, high-performance hospital operating rooms have the appropriate HVAC system, usually unidirectional flow [
4], to develop complex surgeries due to the high level of sepsis reached in the surgical field. Indoor air quality (IAQ) of a surgical room is directly related to the risk of acquiring a nosocomial infection [
5]. A minimum level of microbiological load is needed in operating theatres to avoid surgical site Infections (SSI) [
6,
7], therefore international standards include recommended maximum values. SSIs are mainly caused by airborne bioparticles [
8]. The risk of getting a nosocomial infection is conditioned by several factors—the patient himself, due to his state of health (immune system), the characteristics of the room where he/she is (degree of cleanliness and presence of contaminants), factors relating to medical procedures (techniques and their application, clothing and protective elements, etc.), factors relating to HVAC system (air changes per hour, air movement pattern, air residence time, etc.) [
4], sectioning of the surgical block, and construction works in the facilities [
9]. SSI rate is one of the indicators used internationally to quantify the quality of medical services [
10].
Airborne bioparticles’ origin can be twofold—emitted by people inside the room and/or coming from the outside environment through HVAC system supply air [
11,
12]. Medical staff on site wear clothing that minimizes the spreading of particles from their own body, however, the patient is undressed. In this way, particles generated by both can get into the surgical wound and cause an SSI. This is aggravated if an adequate level of preoperative room cleanliness has not been achieved [
13,
14]. Main pathogens present in operating theatres are bacteria, such as
Staphylococcus aureus, and fungi, as
Aspergillus sp. [
15]. These pathogens are distributed in air using airborne bioparticles emitted by people within the room as a vector [
16]. In order to prevent bioparticles’ entrance through the drive system, the number of recommended filter stages and their efficiency are defined in the high-performance air-conditioning standards.
IAQ requirements go beyond ensuring comfortable thermohygrometric conditions. Monitoring additional environmental parameters in order to meet asepsis level and air quality required by operating room users is necessary for high-performance air-conditioning systems. There are differing requirements regarding thermohygrometric conditions since heating and cooling are demanded independently of the external seasonal regime because of specifications of certain surgeries, for instance, heart surgery, which requires low ambient temperatures. Surgical interventions on patients with immune system disorders require a protective environment in the room they occupy so complexity increases. High-performance operating theatres are suitable for organ transplantation, cardiac and aortic surgery, and orthopedic surgery. Therefore, HVAC systems become an effective tool for controlling SSI in high-performance operating rooms. Water source heat pump (WSHP) systems can integrate to meet the demand for air-conditioning operating rooms safely [
17].
According to the American Society of Heating, Refrigerating, and Air-Conditioning Engineers (ASHRAE), the distribution of temperature, relative humidity, air velocity values, and pollution levels in the room environment determine its IAQ [
18]. Positive differential pressure in the room with respect to adjacent spaces is established to promote operating room protection and prevent microorganisms’ entrance from adjoining rooms (cross-contamination). Air movement from the protected area—the operating theatre—towards the outside is achieved. In addition, controlling aerosols, anesthetic gases, and surgical smoke concentration is necessary to ensure adequate IAQ [
19]. The parameters that must be controlled in high-performance air-conditioning for operating rooms are temperature, relative humidity (RH), air changes per hour (ACH), outdoor air (OA), pressurization, levels of filtering, air movement pattern, air movement among rooms, and microbiological loads. The relative humidity in indoor air must be controlled to reduce the risk of airborne infections [
20].
IAQ of a high-performance operating theatre can be evaluated on the basis of the thermal comfort felt by personnel inside. For this purpose, “predicted mean vote” and “predicted percentage of dissatisfied” derived from the Fanger’s comfort equation are usually calculated [
21]. However, these methods are usually applied to air-conditioning where thermal comfort prevails over other criteria. Medical–surgical criteria must prevail over thermal comfort criteria in surgical suites. SSI over the total number of surgical operations performed in a given room is another criterion for evaluating HVAC system performance. As a disadvantage, this criterion is applied posteriori, so it is not useful to prevent SSI. Nevertheless, computational fluid dynamics (CFD) technology allows us to model air pattern, its thermohygrometric conditions, and bioparticle transport phenomena produced by the air movement in the room. CFD is a utility to evaluate the effectiveness of HVAC system applied to the air-conditioning of high-performance operating rooms during the design phase [
22].
There is no single international standard describing technical recommendations applied to operating room HVAC systems design. Different countries or regions define their own standards. There are other standards related to the high-performance air-conditioning of cleanrooms. Recommendations for cleanrooms in pharmaceutical, microelectronics, and aerospace industries are commonly used in hospital environments. ISO 14644 series of standards are widely used as a reference in the surgical suite context. Cleanrooms and operating suites are compatible because they share technical and hygienic specifications. However, ISO 14644 is specific for industrial white rooms air-conditioning [
23].
The first standard for cleanroom air-conditioning was NASA standard for clean rooms and work station for medical controlled environment (NHB 5340.2) [
24]. Many standards arose from this that deal with filters’ efficiency or maximum microbiological load allowed in this type of rooms. For instance, France and Belgium, NF S 90-351: Clean rooms and related controlled environments in medical establishments [
25]; Germany, DIN 1946: Ventilation and air-conditioning Part 4: Ventilation in hospitals [
26]; Switzerland, SWKI 99-3: Heating, ventilation, and air-conditioning in hospitals [
27]; Japan, JIS-B 9920: Classification of air cleanliness for cleanrooms [
28]; Italy, UNI 11425:2011: Pollution-controlled air-conditioning and ventilation system (CCPV) for the operating block—Design, installation, commissioning, qualification, operation, and maintenance [
29]; United Kingdom and Ireland, HTM 01-03 Heating and ventilation systems: Specialized ventilation for healthcare premises [
30].
Melhado et al. reviewed standards about operating room ventilation systems design [
31]. Information provided in European and South American country standards and ASHRAE Standard was summarized. They analyzed the requirements and their relationship to infection risk. They concluded that defining the ideal values for each parameter was difficult because each standard proposes different values. Nastase et al. conducted a review of the main European standards on operating theatres’ HVAC systems design and operation with special treatment to those applicable in Romania [
32]. Lack of uniformity in existing standards do not impose strict values as would be appropriate and lack specifications of certain parameters were their conclusions. They suggest a re-edition of existing standards based on experience but considering current on-site issues. Balaras et al. collected recommendations from guidelines and standards about design, installation, commissioning, operation, and maintenance of HVAC facilities in hospital surgical rooms [
33]. They matched their work with the monitoring of 20 operating theatres of 10 Hellenic hospitals, detecting inadequate indoor thermal conditions, insufficient air renewals, and poor maintenance plans. Khodakarami and Nasrollahi presented a literature review about thermal comfort in hospitals [
34]. They concluded that existing studies do not consider people with different requirements being in the same room and, consequently, they propose research that reconciles this shortcoming. Iudicello and Fadda made a roadmap through the requirements of some European standards on the design of ventilation systems for operating suites [
35]. They highlighted the difficulty of evaluating an air diffusion system effectiveness in controlling SSI using a general abstract model. However, no precedent studies have been found where standardized design parameters of HVAC facilities for high-performance hospital operating rooms were compared.
The aim of this work is to carry out a comparative analysis of technical and hygienic requirements recommended by different international standards to achieve adequate indoor environmental conditions in high-performance hospital operating theatres. In addition, the difference in criteria is shown through a case study that makes it possible to determine the best choice in the design phase of hospital infrastructures. The results will be useful for designers, managers, and maintenance responsible for this type of installations.
2. Materials and Methods
National and international standards were studied to analyze technical and hygienic recommendations for designing HVAC systems applied to the conditioning of high-performance operating theatres. Specifically, technical and hygienic requirements from standards UNE 100713:2005
Air conditioning in Hospitals [
36], ASHRAE Standard 170-2017
Ventilation of Health Care Facilities [
37], and y EN 16244
Ventilation in Hospitals [
38] were presented, analyzed, and discussed. Furthermore, information published in guidelines, books, and papers was related to the current requirements for discussing its practical applicability.
The standard UNE 100713 is currently in force in Spain since September 2005 when the 2003 version was replaced. Standard EN 16244 advanced drafts exist, and a Technical Specification (TS) document is already published. The 2017 version is the latest update of ASHRAE Standard 170.
Table 1 shows the specifications of the standard used in the research.
CFD technology was employed to quantitatively evaluate HVAC system design functioning according to indoor environmental conditions proposed by these three standards using software ANSYS Fluent. A pressure-based coupled steady-state algorithm was employed for multi-species (dry air and water vapor) numerical model. The Reynolds-Averaged Navier–Stokes (RANS) approach was applied to fluid flow govern equations using a standard k-
ε [
39] turbulence model and standard function for fluid flow treatment near wall [
40]. The Boussinesq model was assumed as buoyancy modeling [
41]. Boundary conditions implemented to numerical models differed in each of the three designs proposed as indicated in the Case Study. For these conditions, equations of continuity, momentum, energy, turbulent kinetic energy (
k), turbulence dissipation rate (
ε), and species are expressed in general form in Equation (1), and specification for source term
SΦ and effective diffusion coefficient
ΓΦ for variable
Φ are in
Table 2 [
42]:
where
uj (
j = 1, 2, and 3) are the three components of momentum (
u,
v,
w),
T is mean temperature,
k is turbulent kinetic energy,
ɛ is turbulence dissipation rate,
C is species concentration,
μ is kinematic viscosity,
μt is turbulent viscosity,
P is mean pressure,
xi and
xj are spatial coordinates in the
i and
j direction,
ρ is density,
gi is component
i of the gravitation vector,
β is thermal expansion coefficient,
T0 is operating temperature,
ST is source term for temperature,
SC is the source term for species,
Gk is the generation of turbulent kinetic energy because of the mean velocity gradients,
GB is the generation of turbulent kinetic energy due to buoyancy,
Ui and
Uj are components
i and
j of the mean velocity,
C1ɛ,
C2ɛ, and
C3ɛ are constants of
ɛ-equation,
Cμ is the constant used for calculating
μt,
σ1 is the turbulent Schmidt number,
σt is the energy Prandtl number,
σk is the Prandtl number of
k,
σɛ is the Prandtl number of
ε, and
σC is the species Prandtl number.
2.1. Standard UNE 100713:2015
Standard UNE 100713 was composed by National Technical Committee “CTN 100-Conditioning” and belongs to International Classification of Standards “ICS 91.140.30/Ventilation and Air-Conditioning Systems”. On the one hand, it proposes a series of physiological and hygienic requirements and, on the other, technical requirements. In order to achieve each one, a series of characteristics and requirements specific to each requirement are listed. First, physiological and hygienic requirements proposed by UNE 100713 are thermal comfort, air quality, and sound pressure level. Secondly, there are seven technical and hygienic requirements—OA intakes and exhaust air outlets, air ducts, closing dampers, smoke extraction ducts and fire dampers, components of air conditioning systems, air-conditioning systems in operating rooms, and operation of air-conditioning systems in special cases.
2.2. Pre-Standard EN 16244
The set of standards EN 16244 Ventilation in hospitals have been drafted by CEN-TC 156-WG 18 and is structured by the TS document and initially by five parts: Part 1—General requirements, Part 2—Operating suites, Part 3—Isolation rooms, Part 4—Sterilization room, and Part 5—Treatment room. The TS document creates a framework within which the parts of the standard are structured and developed. TS document defines new terms—critical zone (surgical table and sterile instruments), protected zone (incident area from air diffuser), and periphery area (anesthetist and other equipment and staff circulating zone)—used to define requirements depending on zones.
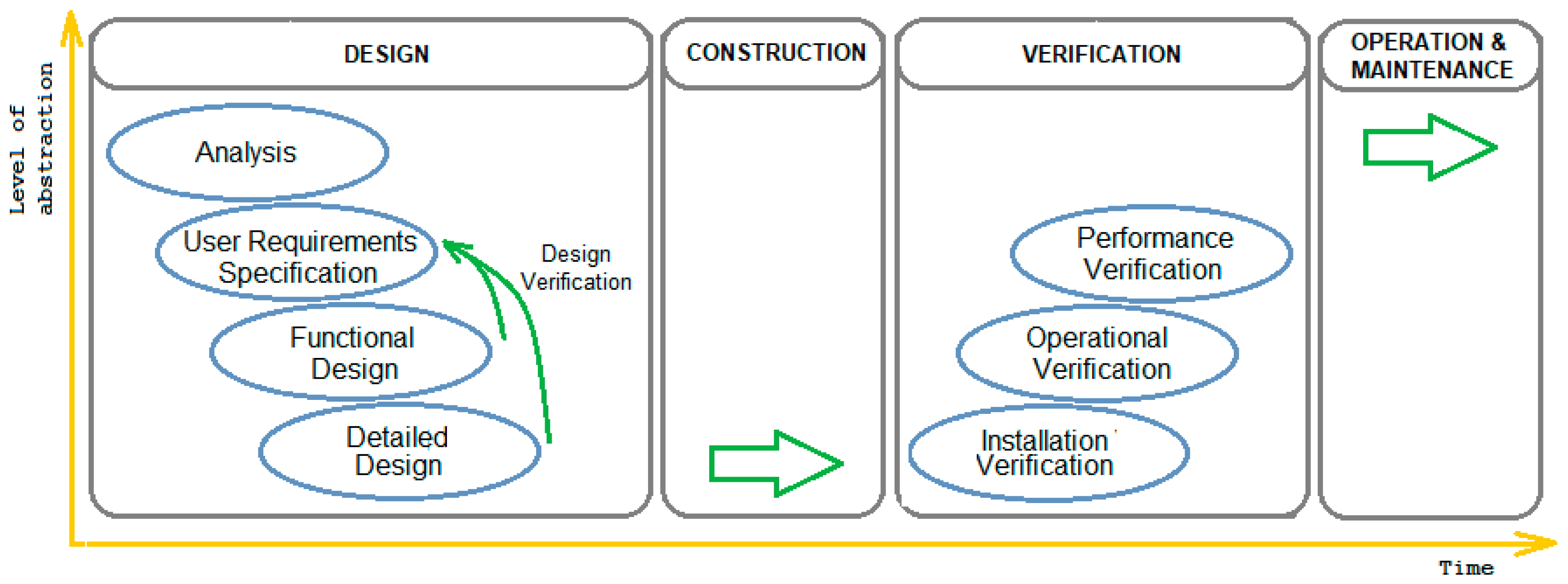
With regard to HVAC systems design, the TS document describes in detail four phases for conditioning installations project in surgical rooms, lists proposed targets of each single phase and appoints who should be in charge. Project phases, specific activities to each one, and how they are distributed along time and the level of abstraction necessary to project development according to “V-Model” project management methodology is schematized in
Figure 1.
Part 1 describes the minimum requirements for ventilation systems in terms of the minimum specifications required by the user, the functional design requirements, and the requirements for the components in the detailed design. Part 2 adapts the technical requirements of each phase defined in Part 1 to operating theatre. In EN 16244-2, the so-called physiological and hygienic requirements are addressed in performance requirements of the ventilation system and the so-called technical and hygienic requirements are addressed as requirements of the system components. Specifically, Part 2 addresses the following hygienic issues related to ventilation systems: (i) air quality, (ii) patient and staff protection from infectious agents, (iii) microorganism growth reduction, and (iv) airflow direction control.
The pre-standard sets out two levels of cleanliness required for an operating room—clean air and ultra-clean air. The air cleanliness level required for an operating room should minimize the chances of contracting an SSI. For each cleaning level, one of two contaminant removal strategies may be used—unidirectional and multidirectional flow ventilation systems. It should be noted that the standard calls them protected area system and air dilution system, respectively. The pre-standard recommends the consideration of factors related to personnel and equipment influence when choosing the ventilation strategy of an HVAC system.
Depending on the required cleanliness level and the chosen ventilation strategy, a number of hygienic and technical requirements are defined. These may vary, depending on whether the operating room is functioning or at rest. When an operating theatre is in operation, requirements are just hygienic and set an upper limit for microbiological load concentration based on ISO 14698 [
43]. With an operating theatre is on standby, requirements are both hygienic and technical, and refer to microbiological load, particle concentration, segregation test, room recovery test, and operating room-lamp wake recovery test.
2.3. ASHRAE Standard 170-2017
Design criteria for environmental control of comfort, asepsis, and odor are proposed in ANSI/ASHRAE/ASHE Standard 170-2017
Ventilation of Health Care Facilities [
37]. The book “HVAC Design Manual for Hospitals and Clinics” [
18] is the basis of the standard. The standard describes general design criteria, and then they are specified according to application—hospital spaces, outpatient spaces, and nursing home spaces. Recommended values for the design parameters of operating theatre air conditioning (physiological and hygienic requirements) are given in hospital spaces. Furthermore, construction criteria for the arrangement of diffusers and extractions in the room, known as technical requirements, are defined. For this work, we used those referred to hospital spaces.
2.4. Quantitative Requirements of the Standards
A comparison between each key parameter value in operating room conditioning according to the Spanish standard, the ASHRAE Standard, and the European pre-standard are shown in
Table 3.
Technical and hygienic prerequisites that are listed and described in UNE 100713 used as requirements for ventilation system components in the new EN 16244 are ducts, end filters, air supply terminal devices, air exhaust devices, local recirculation fans, acoustic attenuators and doors, and air leakage. In addition, new ones have been introduced—overflow openings, heating systems for cold spaces and ceilings, doors and their slits, and lighting and service equipment—which are related to detailed design of a facility.
4. Discussion
The recommended temperature range is 18–24 °C as a whole. Certain surgeries require lower temperature (deep and organ surgery) or higher temperature (pediatric surgery) [
33]. Research has revealed the influence of clothing and activity level on thermal comfort so that nurses and anesthetists will be comfortable at 23–24 °C, surgeons at 18–19 °C, and patients at 24.5–25.5 °C [
5]. A temperature higher than 23 °C is hardly bearable for surgeons [
44]; nevertheless, the risk of hypothermia exists for patient below 21 °C [
45]. Electromedical equipment and surgical lights have a direct influence on indoor temperature distribution causing asymmetry and/or stratification of air temperatures [
5].
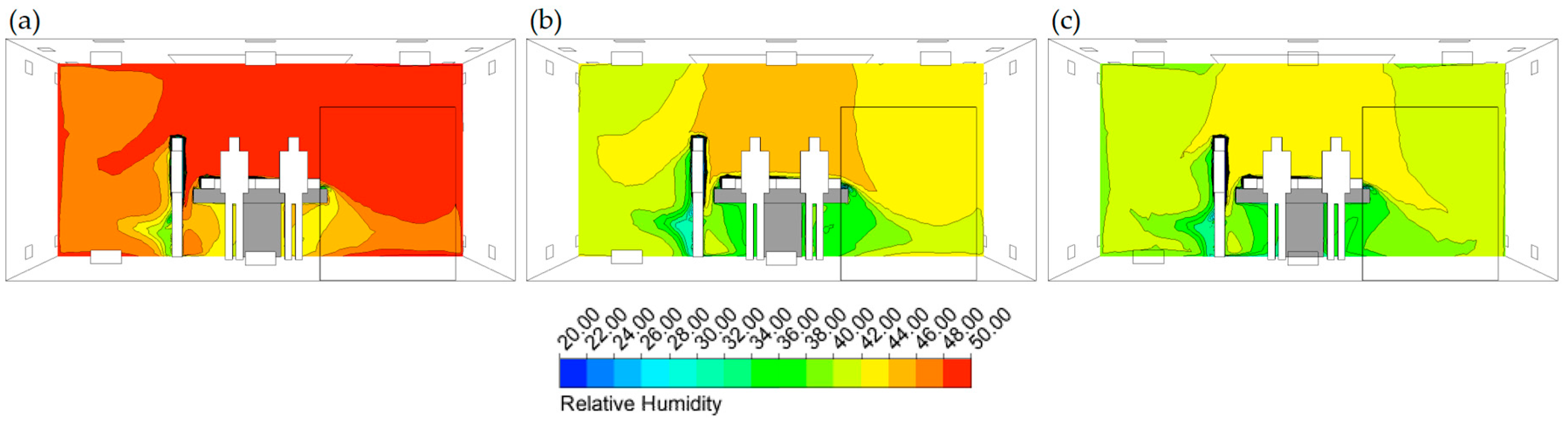
Values proposed for RH by the standards are different, but the maximum value of 60% is shared. The widest range is covered by ASHRAE Standard (20%–60%), while the narrowest is for UNE 100713 (45%–55%). Not limiting RH value favors the proliferation of bacteria for extreme values in both senses [
18], favors blood coagulation, while a dry environment makes staff uncomfortable and sweating is favored when RH is high. The humidification process in air conditioning is critical and must be backed up by an adequate maintenance plan [
46]. The standards allow regulation of values within defined ranges for thermal comfort (temperature and RH), so they can be modified if necessary, for medical requirements.
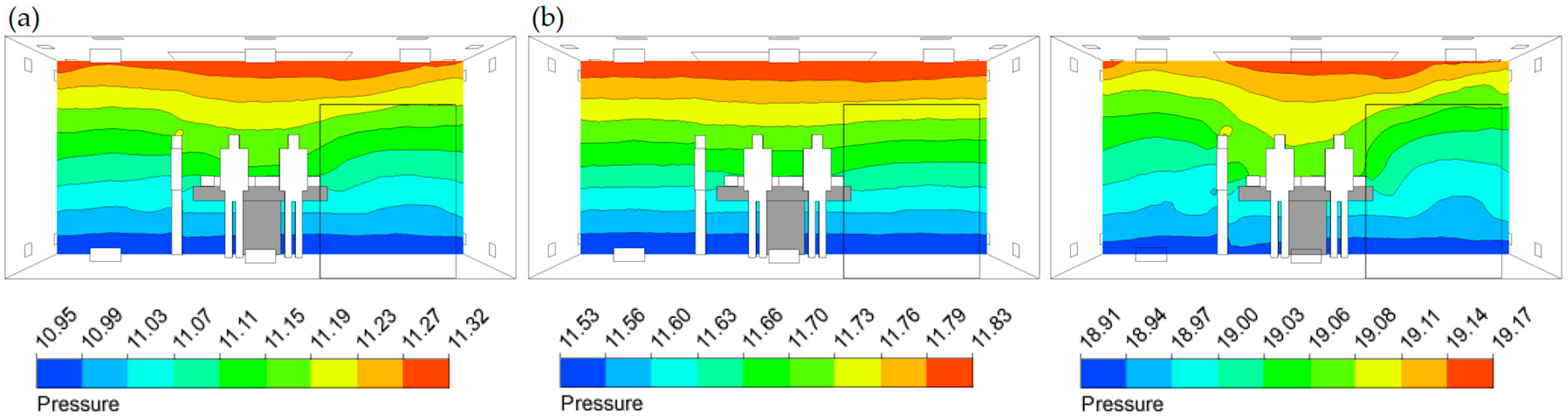
It has been proven that overpressure of the room is reached by mechanical means extracting an air flow lower than the driven one [
47]. This parameter favors protection of the room against cross-contamination since it induces circulation of air from the clean zone to less clean corridors and adjoining rooms inside the surgical block. Overpressure in the room prevents potentially contagious bioparticles entering, complementing the filters’ work. Recommended minimum pressurization value is positive for maintaining operating rooms as protected areas. At this point, it is worth wondering whether a value of 2.5 Pa established by ASHRAE Standard and 5 Pa in EN 16244-2 is adequate to favor and maintain this air circulation among rooms or, on the contrary, this value is insufficient. A great deal of rigor is required from operating theatre medical staff to achieve and maintain pressurization in the room. Avoiding entrance and exit of personnel and materials during surgery is recommended [
8] since the doors opening during surgery entails the complete loss of ventilation system effectiveness [
48] and an increase in air residence time [
49].
Ultra-clean air must be supplied to high-performance operating rooms to prevent entrance of microorganisms or other pathogens from the outside environment. EN 16244-2 adds a new filtration stage by means of a pre-filter (M5) installed on top of stages already recommended in UNE 100713 standard: F7 (ε = 80%–90%), F9 (ε > 95%), and H13 (ε = 99.95%). This will improve the filter stages’ performance by lengthening their useful life. This recommendation strongly disagrees with the ASHRAE Standard, which proposes two lower-efficiency filter stages. The first filtering level will be through MERV 7 filter and the second one will be through MERV 14 filter. Both filter levels match a G4 filter (ε < 90%) and F8 (ε = 90%–95%) according to ISO 16890-1 [
50]. They agree to place the high-efficiency filter in a drive terminal unit. None of the standards contemplates ultraviolet germicidal irradiation, being an effective germicidal method [
33].
ACH is performed to decrease the microbiological load generated within the operating room. ACH allows for the dilution of anesthetic gases and surgical smoke concentration inside the room, therefore, a much higher number of ACH will be performed compared to other types of rooms. Infection risk increases with bioparticles concentration due to its increased viability as a pathogen [
51]. Anesthetic gas concentration increases can be caused by a leak in equipment or due to bad practical execution, and the surgical smoke increase is derived from electrosurgery, laser, or ultrasound use [
52]. The recommended minimum value of ACH is very similar in UNE 100713 and ASHRAE Standard 170, however, this parameter is not specified in EN 16244-2. On the one hand, increasing the amount of fresh air impelled improves dilution effectiveness [
53] but, on the other hand, it does not guarantee an SSI rate decrease and, nevertheless, operating costs are always raised [
54]. Infection hazard is reduced by controlling air movement pattern [
52,
55] which leads to an equipment expenditure and operating costs reduction. OA discharge into a room through the HVAC system also contributes to lowering the concentration of medical gases and surgical smoke generated during surgery. UNE 100713 sets a minimum OA flow value in volumetric flow units. Nonetheless, EN 16244-2 prescribes it according to the number of people in the room. The number of people attending surgery is variable, which will cause the value of this parameter to change. This requirement is therefore not easy to implement since an automatic control system that regulates OA flow according to the occupation of the room is necessary. ASHRAE Standard 170 states that four over 20 ACH shall be performed by OA. Air recirculated to the room should pass through filtration stages to ensure its charge of particles.
The room recovery time concept is not contemplated by ASHRAE Standard although it is included in Spanish and European standards. However, the reference standard used to define a room recovery test is different: UNE 100713 applies another Spanish standard (UNE 171340: 2012 [
56]) and pre-standard EN 16244-2 reference ISO 14644-3. It should be noted that UNE 171340 is specifically aimed at hospital wards, while ISO 14644-3 is for controlled environment rooms in general. The Center for Disease Control proposes an equation to determine room recovery time based on initial concentration, room volume, airflow, and ACH [
8].
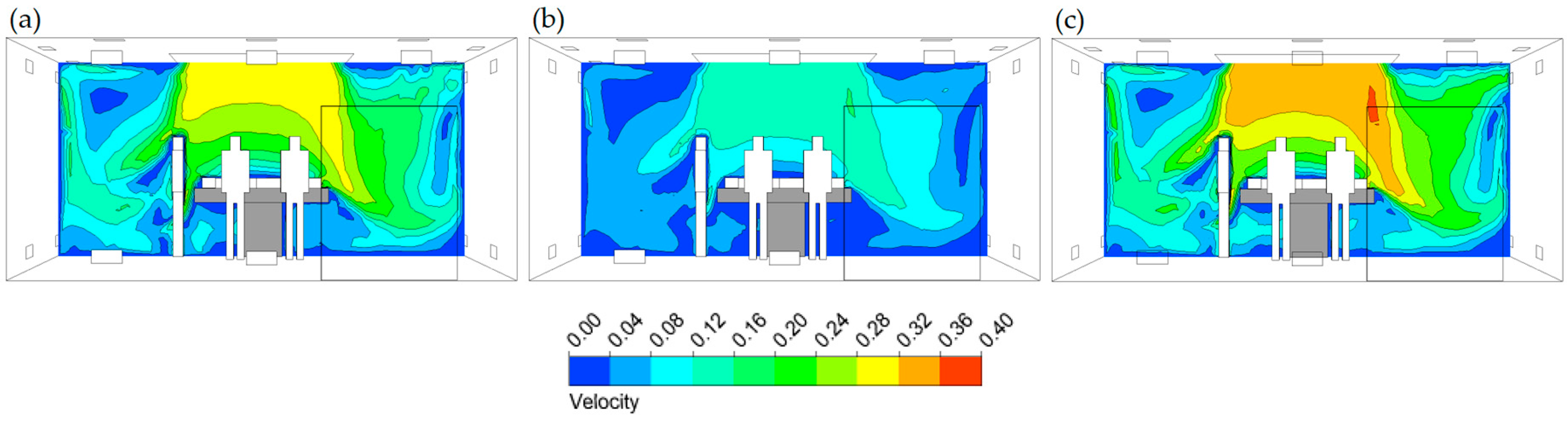
Surgical field cleaning in high-performance operating theatres is achieved by the piston effect. The piston effect is generated by unidirectional flow diffusers. It is possible to obtain an adequate air movement pattern by driving ultra clean air at an adequate velocity, across a given surface and being extracted from the room by strategic locations. Air impulsion velocity in a terminal unit located above the surgical field must be sufficient to maintain unidirectionality when going through a protected zone and to ensure particle dragging by piston effect [
57]. In order to maintain unidirectionality of flow, air must have a certain velocity and turbulence lower than 5% [
18]. Too high velocity will cause airflow swirls re-entering surgical field and/or decreasing bioparticle removal efficacy. Obstacles to maintaining unidirectional airflow are, first, physical elements such as luminaires and personnel present; and, second, the thermal contour of people and equipment. ASHRAE Standard recommends a maximum air supply velocity value of 0.18 m/s, a minimum in UNE 100713 of 0.20 m/s, and in EN 16244-2 0.24 m/s. The values of ASHRAE are based on the work of Memarzadeh and Manning [
4] and Rui et al. [
24] and are much lower than those proposed in the other two standards under study. However, there are research projects [
22] that support the stated in UNE 100713 and EN 16244-2. Forced air exhaust location determines air movement pattern generated. A strategic location of grilles will cause air to trace a certain path towards the outlet, consequently improving dilution rate (cleaning, particle removal, etc.).
It has been proven that medical personnel subjected to a sound pressure level influence their fatigue and, therefore, their performance in medical–surgical practice [
58]. The ASHRAE criterion is the most tolerant while UNE 100713 is the most restrictive. Pre-standard EN 16244-2 specifies a limit of 48 dBA, closer to the AHSRAE limit than to the UNE standard. No other studies have been found on the influence of sound pressure level on acoustic comfort in operating theatres.
Aforementioned standard UNE 171340:2012 [
56] is used to validate and qualify controlled environment rooms in hospitals. It evaluates a series of environmental and facility parameters. Environmental parameters are temperature and RH, microbiology, bioparticles classification, and sound pressure level; facility parameters are differential pressure, absolute filter location, airflows and ACH, airflow direction, and room recovery test. In addition, energetic and environmental saves can be achieved [
59].
Default value ranges for parameters are different in standards applicable to a single country. It reveals the disparity of baseline criteria for defining guidelines and standards and causes designers to face technical indecision to ensure patient and caregiver safety. Adequate value of each parameter is chosen in order to minimize infection risk. The international nature of the standards analyzed allows the results of this work to be applicable to other countries since surgeries demand similar hygienic levels all over the world.
Future works should be aimed at adapting the value of each design parameter to the conditions of each surgery. Multivariable tables and/or abacus can be obtained to define suitable environmental conditions according to the type of surgery. In this way, it will be possible to integrate people’s thermal comfort, maintaining safety and sterility levels during surgery. Analyses using CFD technology will play a crucial role.
5. Conclusions
Design parameters of HVAC installations in high-performance hospital operating theatres were evaluated according to UNE 100713, ASHRAE Standard 170, and pre-standard EN 16244-2. All of them establish a range of values for thermohygrometric conditions.
It was found that ASHRAE Standard was the most tolerant in values proposed for room overpressure. Pre-standard maintains the minimum value proposed by UNE standard but does not define a maximum, so in both, the value of this parameter is at designer criteria. ASHRAE Standard recommends a smaller number of filtering stages and less efficiency. The pre-standard adds an additional level of pre-filtering over UNE standard.
It was noticed that the unit used to define OA flow recommended by EN 16244 is of difficult practical implementation, however, UNE and ASHRAE standards establish a more feasible way to define it. Nonetheless, Standard 170 does not contemplate room recovery time concept for study standards, as UNE 100713 and EN 16244-2 do. A minimum drive speed of 0.07 m/s and 0.11 m/s less than UNE and EN 16244-2, respectively, is proposed by ASHRAE. In addition, its maximum value is lower than the minimum proposed in the other two standards. There is a similar discrepancy in the scientific literature regarding this parameter. The most restrictive sound pressure level is for UNE 100713.
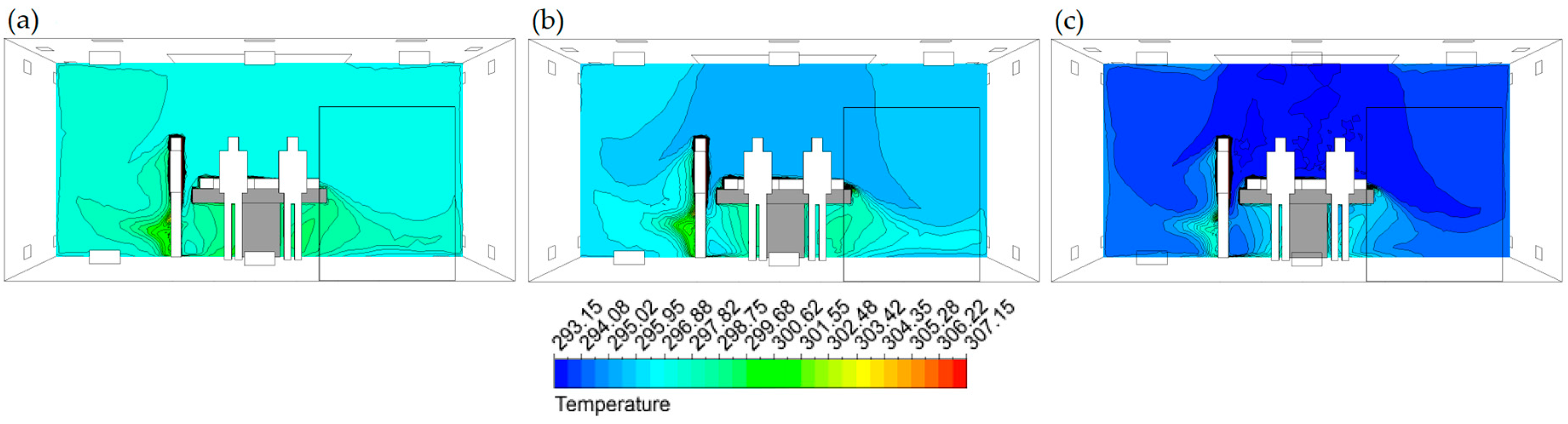
Huge temperature and RH gradients (1.18 K/cm and 3.75%/cm in UNE 100713, 1.37 K/cm and 3.06%/cm in ASHRAE 170, and 1.55 K/cm and 2.75%/cm in EN 16244-2, respectively) highlight the importance of adapting the values of these parameters to the patient’s health status to ensure their safety and taking into account the thermal comfort of medical staff to improve their medical–surgical performance. CFD studies can quantify the pressure gradient due to stratification generated in the room (0.124 Pa/m in UNE 100713, 0.112 Pa/m in ASHRAE 170, and 0.082 Pa/m in EN 16244). They also make it possible to detect areas of haven that constitute microbiological load accumulation areas. In this way, cleaning protocols can be defined to avoid consequences in a preventive way.
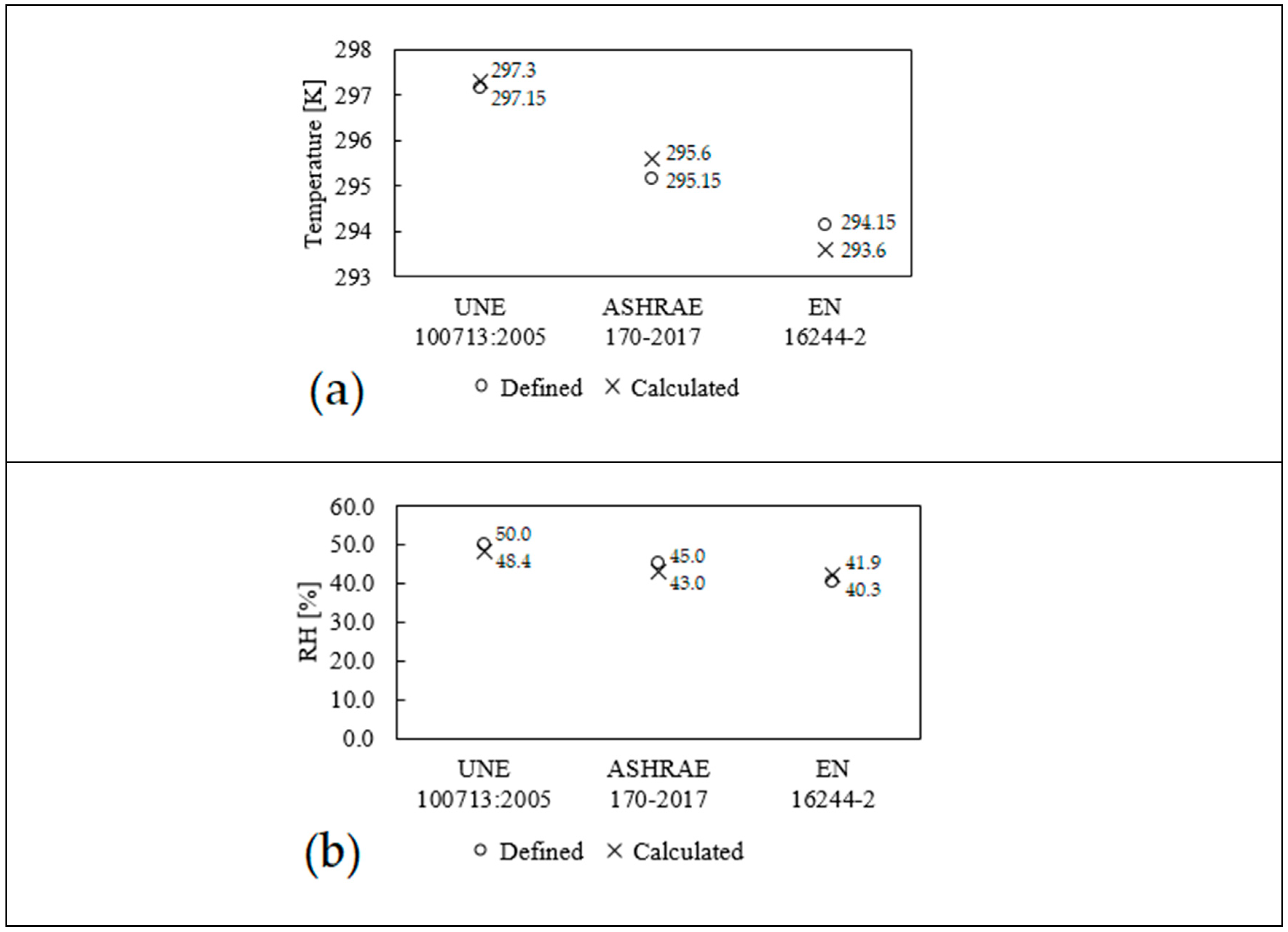
The soundness of the results obtained is related to their appropriateness to characteristics of surgery performed. It was detected that different results are obtained in order to design a room according to the regulation employed. It was proven that CFD technology is an adequate tool to obtain performance evaluations of installations prior to construction. It even allows the inverse process to be established, i.e., desired pressurization, temperature, and RH values are defined, and the value of boundary conditions is calculated as a result.











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}