

Celecoxib Decreases the Need for Rescue Analgesics after Total Knee Arthroplasty: A Meta-Analysis
 , ,
, ,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population, Interventions, Control, and Outcome Strategy [15]
2.1.1. Inclusion Criteria
- Population: clinical trials included patients undergoing total knee arthroplasty;
- Interventions: patients received celecoxib;
- Control: patients received a placebo;
- Outcome: evaluation of postoperative pain using the Visual Analogue Scale (VAS) at rest, ambulation, and active range of motion, rescue analgesic intake, and adverse effects.
2.1.2. Exclusion Criteria
2.2. Research Question
2.3. Information Search
2.4. Assessment of Bias
2.5. Data Extraction
2.6. Statistical Analysis
3. Results
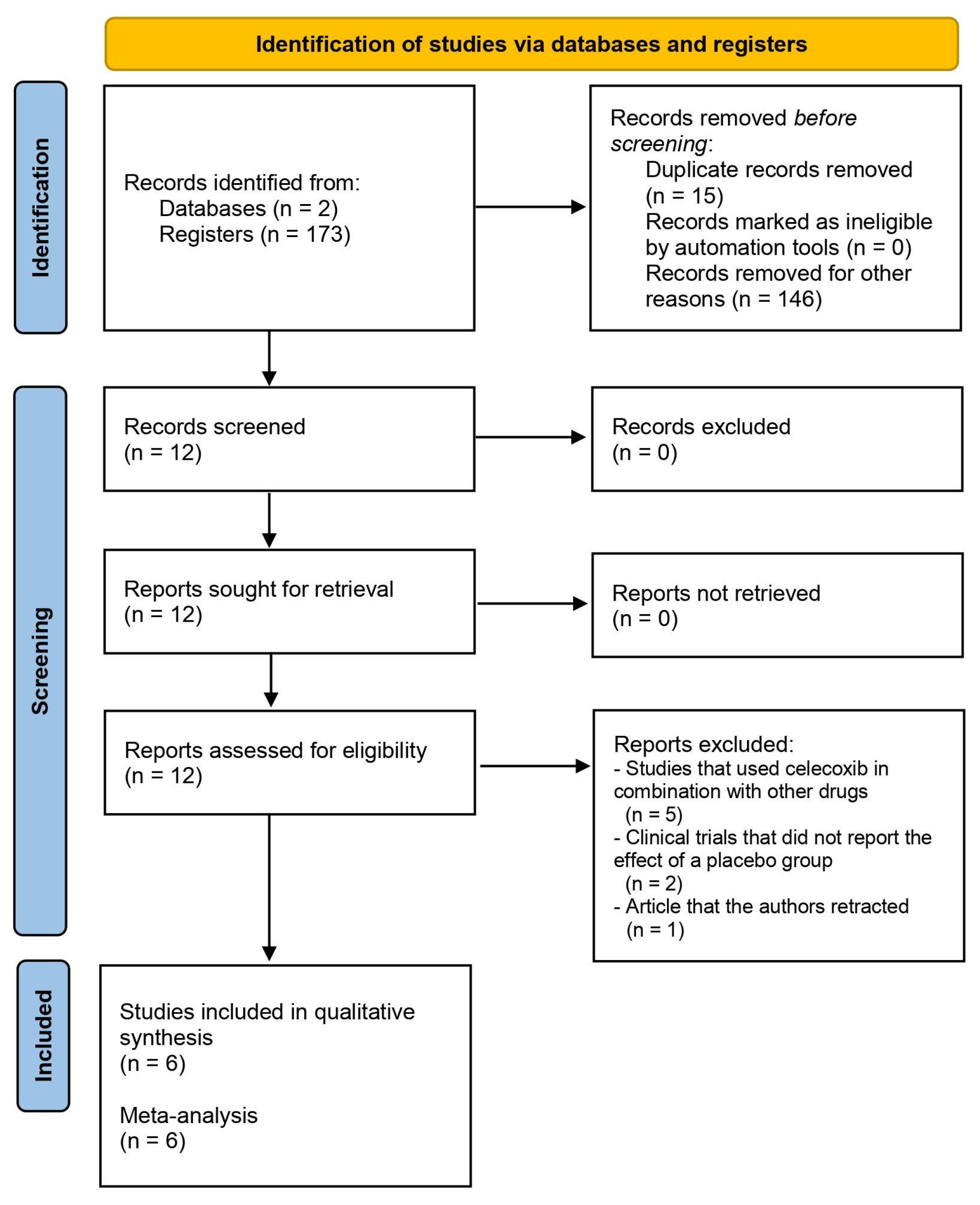
3.1. Information Search
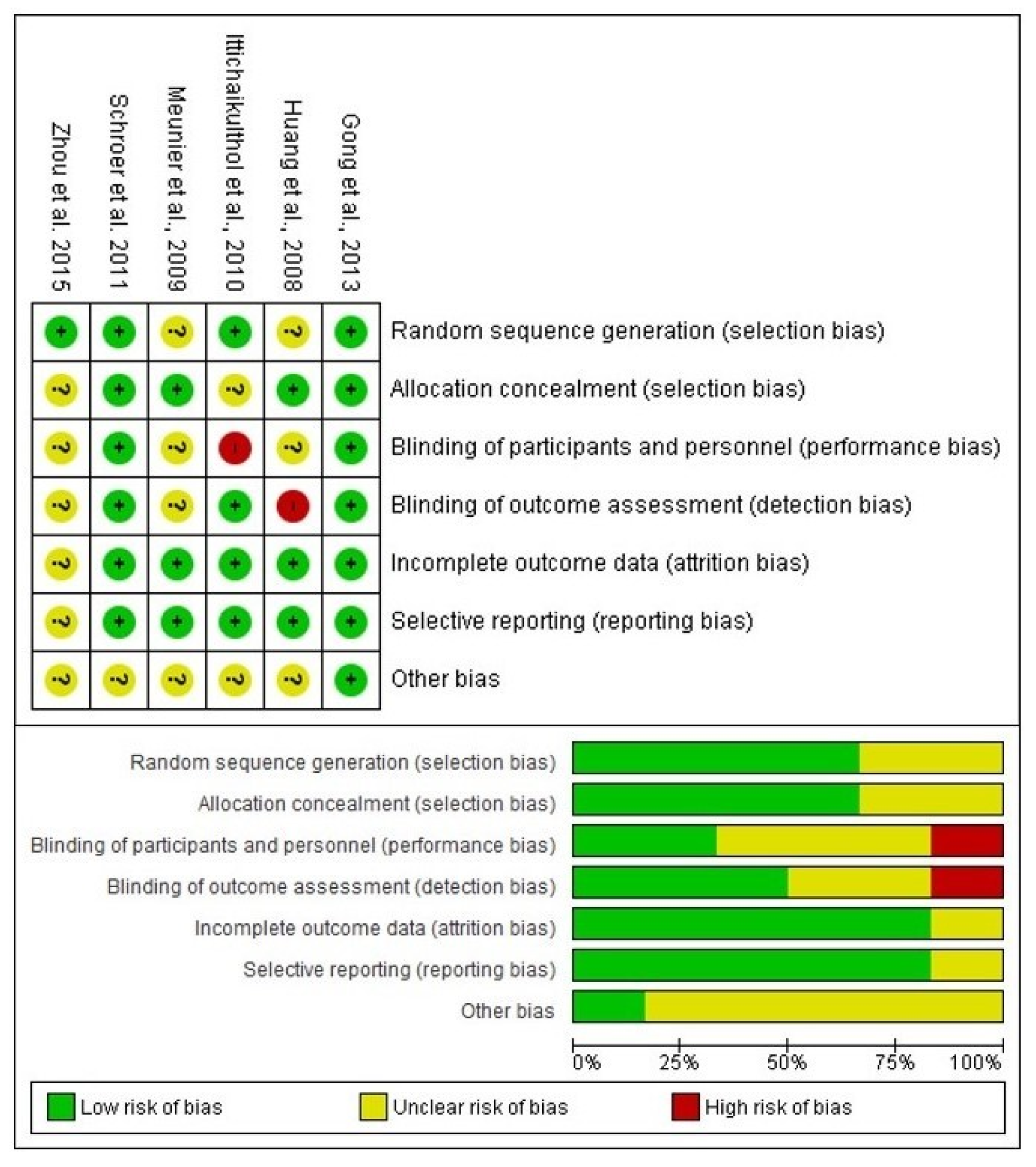
3.2. Bias Assessment
3.3. Qualitative Assessment
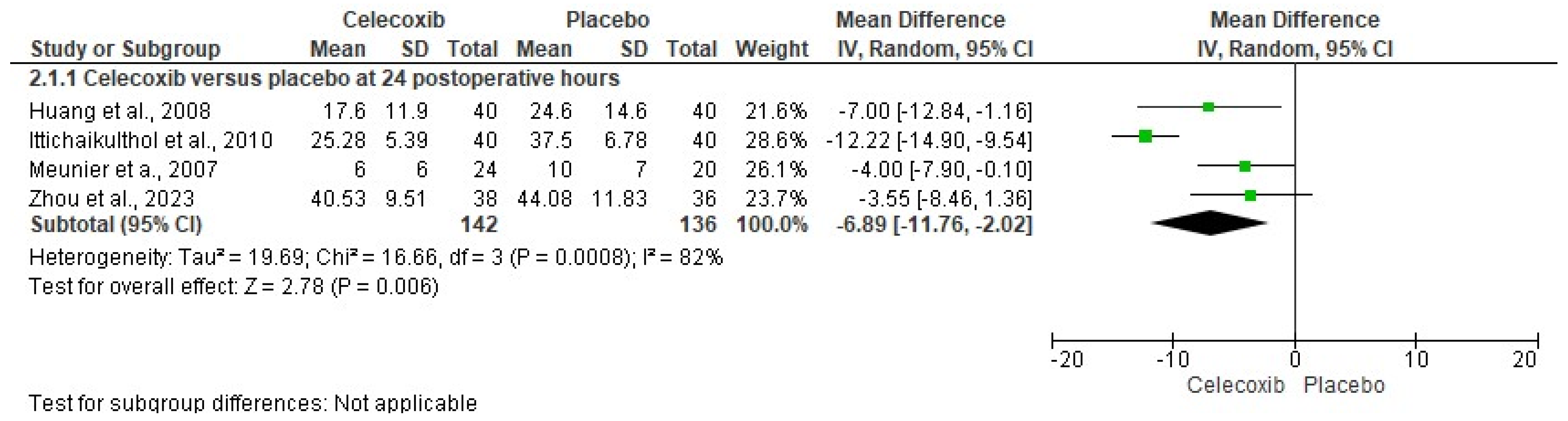
3.4. Quantitative Evaluation
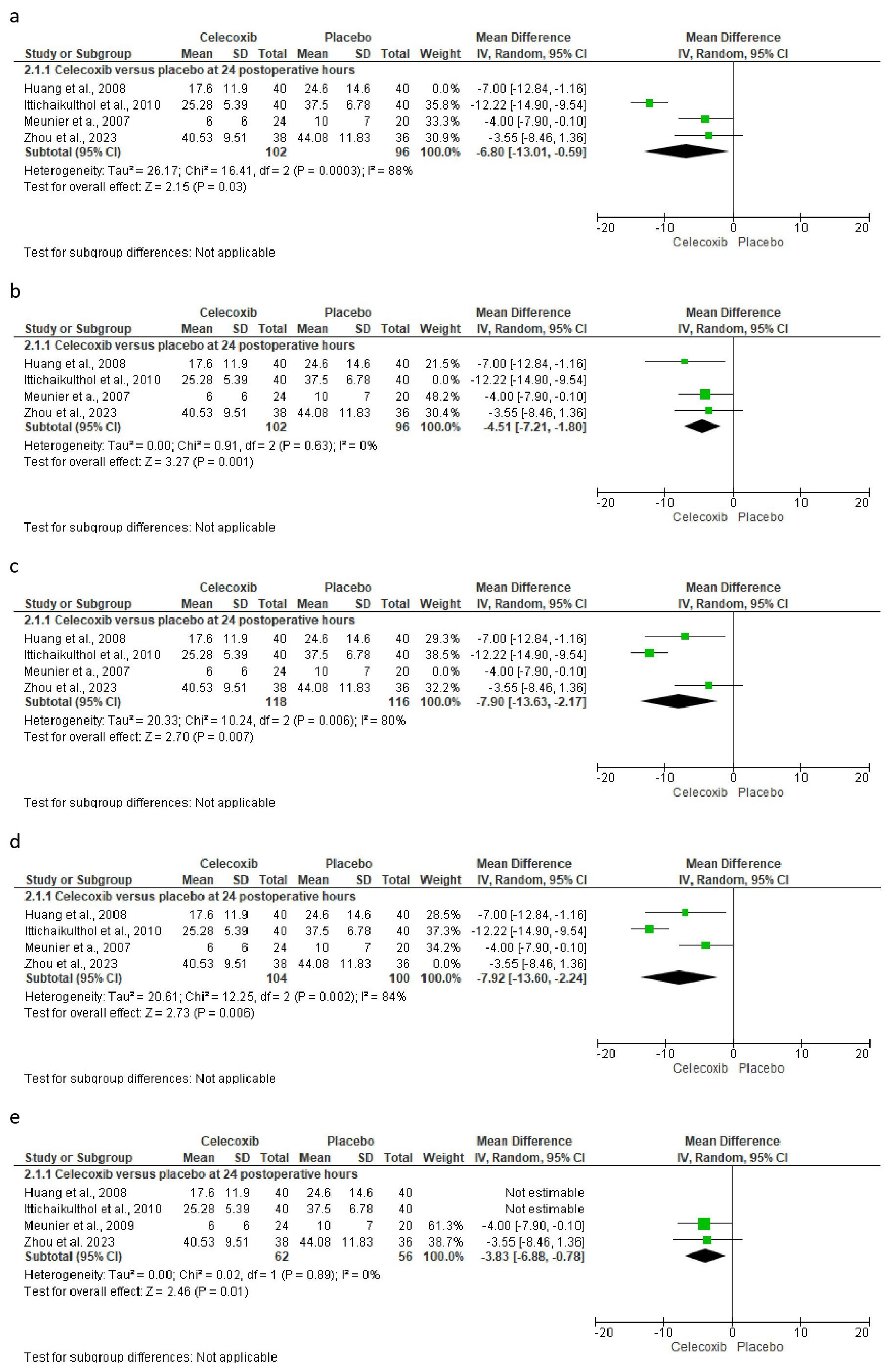
3.5. The Sensitivity Assessment and Publication Bias
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhao, J.; Davis, S.P. An integrative review of multimodal pain management on patient recovery after total hip and knee arthroplasty. Int. J. Nurs. Stud. 2019, 98, 94–106. [Google Scholar] [CrossRef]
- Li, J.W.; Ma, Y.S.; Xiao, L.K. Postoperative Pain Management in Total Knee Arthroplasty. Orthop. Surg. 2019, 11, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Lavand’homme, P.M.; Kehlet, H.; Rawal, N.; Joshi, G.P.; PROSPECT Working Group of the European Society of Regional Anaesthesia and Pain Therapy (ESRA). Pain management after total knee arthroplasty: Procedure Specific Postoperative Pain Management recommendations. Eur. J. Anaesthesiol. 2022, 39, 743–757. [Google Scholar] [CrossRef]
- Corap, Y.; Brix, M.; Brandt, J.R.; Emmeluth, C.; Lindberg-Larsen, M. Knee function, quality of life, pain, and living conditions after distal femoral resection knee arthroplasty for non-tumor indications. BMC Musculoskelet. Disord. 2023, 24, 9. [Google Scholar] [CrossRef]
- Connolly, P.; Coombs, S.; Schwarzkopf, R. Mechanical complications after total knee arthroplasty. Expert. Rev. Med. Devices 2023, 20, 1105–1117. [Google Scholar] [CrossRef]
- Canovas, F.; Dagneaux, L. Quality of life after total knee arthroplasty. Orthop. Traumatol. Surg. Res. 2018, 104, S41–S46. [Google Scholar] [CrossRef] [PubMed]
- Gaffney, C.J.; Pelt, C.E.; Gililland, J.M.; Peters, C.L. Perioperative Pain Management in Hip and Knee Arthroplasty. Orthop. Clin. N. Am. 2017, 48, 407–419. [Google Scholar] [CrossRef]
- Derogatis, M.J.; Sodhi, N.; Anis, H.K.; Ehiorobo, J.O.; Bhave, A.; Mont, M.A. Pain Management Strategies to Reduce Opioid Use Following Total Knee Arthroplasty. Surg. Technol. Int. 2019, 35, 301–310. [Google Scholar] [PubMed]
- Elmallah, R.K.; Chughtai, M.; Khlopas, A.; Newman, J.M.; Stearns, K.L.; Roche, M.; Kelly, M.A.; Harwin, S.F.; Mont, M.A. Pain Control in Total Knee Arthroplasty. J. Knee Surg. 2018, 31, 504–513. [Google Scholar] [CrossRef]
- Soffin, E.M.; Memtsoudis, S.G. Anesthesia and analgesia for total knee arthroplasty. Minerva Anestesiol. 2018, 84, 1406–1412. [Google Scholar] [CrossRef]
- O’Neill, A.; Lirk, P. Multimodal Analgesia. Anesthesiol. Clin. 2022, 40, 455–468. [Google Scholar] [CrossRef]
- Xu, C.P.; Li, X.; Wang, Z.Z.; Song, J.Q.; Yu, B. Efficacy and safety of single-dose local infiltration of analgesia in total knee arthroplasty: A meta-analysis of randomized controlled trials. Knee 2014, 21, 636–646. [Google Scholar] [CrossRef] [PubMed]
- Derry, S.; Moore, R.A. Single dose oral celecoxib for acute postoperative pain in adults. Cochrane Database Syst. Rev. 2013, 2013, CD004233. [Google Scholar] [CrossRef]
- Lefkowith, J.B. Cyclooxygenase-2 specificity and its clinical implications. Am. J. Med. 1999, 106, 43S–50S. [Google Scholar] [CrossRef]
- Leonardo, R. PICO: Model for clinical questions. Evid. Based Med. Pract. 2008, 3, 2. [Google Scholar]
- Higgins, P.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Version 5.1.0 [Updated March 2011]; The Cochrane Collaboration: Oxford, UK, 2011; Available online: http://www.cochrane-handbook.org/ (accessed on 22 September 2023).
- Jones, A.; Steel, D. Evaluating the quality of medical evidence in real-world contexts. J. Eval. Clin. Pract. 2018, 24, 950–956. [Google Scholar] [CrossRef]
- Atkins, D.; Eccles, M.; Flottorp, S.; Guyatt, G.H.; Henry, D.; Hill, S.; Liberati, A.; O’Connell, D.; Oxman, A.D.; Phillips, B.; et al. Systems for grading the quality of evidence and the strength of recommendations I: Critical appraisal of existing approaches The GRADE Working Group. BMC Health Serv. Res. 2004, 4, 38. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J.; GRADE Working Group. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef]
- Franco-de la Torre, L.; Gómez-Sánchez, E.; Aragon-Martinez, O.H.; Hernández-Gómez, A.; Franco-González, D.L.; Guzmán-Flores, J.M.; Alonso-Castro, A.J.; Granados-Soto, V.; Isiordia-Espinoza, M.A. Analgesic Efficacy and Safety of Tapentadol Immediate Release in Bunionectomy: A Meta-Analysis. Pharmaceuticals 2023, 16, 1287. [Google Scholar] [CrossRef]
- Whitley, E.; Ball, J. Statistics review 3: Hypothesis testing and P values. Crit. Care 2002, 6, 222–225. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef]
- Franco-de la Torre, L.; Gómez-Sánchez, E.; Serafín-Higuera, N.A.; Alonso-Castro, Á.J.; López-Verdín, S.; Molina-Frechero, N.; Granados-Soto, V.; Isiordia-Espinoza, M.A. Dexamethasone Increases the Anesthetic Success in Patients with Symptomatic Irreversible Pulpitis: A Meta-Analysis. Pharmaceuticals 2022, 15, 878. [Google Scholar] [CrossRef] [PubMed]
- Gong, L.; Dong, J.Y.; Li, Z.R. Effects of combined application of muscle relaxants and celecoxib administration after total knee arthroplasty (TKA) on early recovery: A randomized, double-blind, controlled study. J. Arthroplast. 2013, 28, 1301–1305. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.M.; Wang, C.M.; Wang, C.T.; Lin, W.P.; Horng, L.C.; Jiang, C.C. Perioperative celecoxib administration for pain management after total knee arthroplasty—A randomized, controlled study. BMC Musculoskelet. Disord. 2008, 9, 77. [Google Scholar] [CrossRef] [PubMed]
- Ittichaikulthol, W.; Prachanpanich, N.; Kositchaiwat, C.; Intapan, T. The post-operative analgesic efficacy of celecoxib compared with placebo and parecoxib after total hip or knee arthroplasty. J. Med. Assoc. Thai. 2010, 93, 937–942. [Google Scholar] [PubMed]
- Meunier, A.; Lisander, B.; Good, L. Effects of celecoxib on blood loss, pain, and recovery of function after total knee replacement: A randomized placebo-controlled trial. Acta Orthop. 2007, 78, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Schroer, W.C.; Diesfeld, P.J.; LeMarr, A.R.; Reedy, M.E. Benefits of prolonged postoperative cyclooxygenase-2 inhibitor administration on total knee arthroplasty recovery: A double-blind, placebo-controlled study. J. Arthroplast. 2011, 26 (Suppl. S6), 2–7. [Google Scholar] [CrossRef]
- Zhou, Y.; Liu, X.; Ding, C.; Xiang, B.; Yan, L. Positive Preemptive Analgesia Effectiveness of Pregabalin Combined with Celecoxib in Total Knee Arthroplasty: A Prospective Controlled Randomized Study. Pain Res. Manag. 2023, 2023, 7088004. [Google Scholar] [CrossRef]
- Mammoto, T.; Fujie, K.; Taguchi, N.; Ma, E.; Shimizu, T.; Hashimoto, K. Short-Term Effects of Early Postoperative Celecoxib Administration for Pain, Sleep Quality, and Range of Motion After Total Knee Arthroplasty: A Randomized Controlled Trial. J. Arthroplast. 2021, 36, 526–531. [Google Scholar] [CrossRef]
- Mammoto, T.; Fujie, K.; Mamizuka, N.; Taguchi, N.; Hirano, A.; Yamazaki, M.; Ueno, S.; Ma, E.; Hashimoto, K. Effects of postoperative administration of celecoxib on pain management in patients after total knee arthroplasty: Study protocol for an open-label randomized controlled trial. Trials 2016, 17, 45. [Google Scholar] [CrossRef]
- Xu, X.; Sang, W.; Liu, Y.; Zhu, L.; Lu, H.; Ma, J. Effect of Celecoxib on Surgical Site Inflammation after Total Knee Arthroplasty: A Randomized Controlled Study. Med. Princ. Pract. 2018, 27, 481–488. [Google Scholar] [CrossRef] [PubMed]
- Lubis, A.M.T.; Rawung, R.B.V.; Tantri, A.R. Preemptive Analgesia in Total Knee Arthroplasty: Comparing the Effects of Single Dose Combining Celecoxib with Pregabalin and Repetition Dose Combining Celecoxib with Pregabalin: Double-Blind Controlled Clinical Trial. Pain Res. Treat. 2018, 2018, 3807217. [Google Scholar] [CrossRef] [PubMed]
- Zhuang, Q.; Tao, L.; Lin, J.; Jin, J.; Qian, W.; Bian, Y.; Li, Y.; Dong, Y.; Peng, H.; Li, Y.; et al. Postoperative intravenous parecoxib sodium followed by oral celecoxib post total knee arthroplasty in osteoarthritis patients (PIPFORCE): A multicentre, double-blind, randomised, placebo-controlled trial. BMJ Open 2020, 10, e030501. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Xie, L.; Liu, H.; Hu, Y. Transdermal buprenorphine patch versus oral celecoxib for pain management after total knee arthroplasty: An open- label, randomized controlled trial. Orthop. Traumatol. Surg. Res. 2020, 106, 915–919. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Wang, F. Preoperative celecoxib analgesia is more efficient and equally tolerated compared to postoperative celecoxib analgesia in knee osteoarthritis patients undergoing total knee arthroplasty: A randomized, controlled study. Medicine 2018, 97, e13663. [Google Scholar] [CrossRef] [PubMed]
- Reuben, S.S.; Buvenandran, A.; Katz, B.; Kroin, J.S. A prospective randomized trial on the role of perioperative celecoxib administration for total knee arthroplasty: Improving clinical outcomes. Anesth. Analg. 2008, 106, 1258–1264. [Google Scholar] [CrossRef] [PubMed]
- Pandey, C.K.; Priye, S.; Singh, S.; Singh, U.; Singh, R.B.; Singh, P.K. Preemptive use of gabapentin significantly decreases postoperative pain and rescue analgesic requirements in laparoscopic cholecystectomy. Can. J. Anaesth. 2004, 51, 358–363. [Google Scholar] [CrossRef]
- Garcia, J.B.; Barbosa-Neto, J.O.; Vasconcelos, J.W.; Ferro, L.S.; Silva, R.C. Analgesic efficacy of the intra-articular administration of high doses of morphine in patients undergoing total knee arthroplasty. Rev Bras Anestesiol. 2010, 60, 1–12. [Google Scholar] [CrossRef]
- Kiefhaber, T.R.; Vyrva, O. Will the Use of Intraoperative Liposomal Bupivacaine During Thumb Carpometacarpal Arthroplasty Decrease Postoperative Use of Opioids? A Prospective Randomized Study. J. Hand Surg. Am. 2022, 47, 586.e1–586.e8. [Google Scholar] [CrossRef]
- Han, S.S.; Do, S.H.; Kim, T.H.; Choi, W.J.; Yun, J.S.; Ryu, J.H. Stepwise tapering of remifentanil at the end of surgery decreased postoperative pain and the need of rescue analgesics after thyroidectomy. BMC Anesthesiol. 2015, 15, 46. [Google Scholar] [CrossRef]
- Yu, L.; Yang, Y.; Wu, H.; Yu, Y.; Wang, Y.; Yan, S.; Li, N.; Li, H.; Chen, C.; Zhang, Z. Pupillary monitoring decreases remifentanil consumption during laparoscopic uterine surgery and improves postoperative recovery. Minerva Anestesiol. 2023, 89, 859–866. [Google Scholar] [CrossRef]
- Bilir, S.; Yurtlu, B.S.; Hancı, V.; Okyay, R.D.; Erdoğan-Kayhan, G.; Ayoğlu, H.P.; Özkoçak-Turan, I. Effects of peroperative intravenous paracetamol and lornoxicam for lumbar disc surgery on postoperative pain and opioid consumption: A randomized, prospective, placebo-controlled study. Agri 2016, 28, 98–105. [Google Scholar] [CrossRef]
- Stepan, J.G.; Sacks, H.A.; Verret, C.I.; Wessel, L.E.; Kumar, K.; Fufa, D.T. Standardized Perioperative Patient Education Decreases Opioid Use after Hand Surgery: A Randomized Controlled Trial. Plast. Reconstr. Surg. 2021, 147, 409–418. [Google Scholar] [CrossRef]
- Gormley, J.; Gouveia, K.; Sakha, S.; Stewart, V.; Emmanuel, U.; Shehata, M.; Tushinski, D.; Shanthanna, H.; Madden, K. Reduction of opioid use after orthopedic surgery: A scoping review. Can. J. Surg. 2022, 65, E695–E715. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Deng, H.; Chen, X.; Lin, Y.; Xie, X.; Bo, Z. The efficacy and safety of selective COX-2 inhibitors for postoperative pain management in patients after total knee/hip arthroplasty: A meta-analysis. J. Orthop. Surg. Res. 2020, 15, 39. [Google Scholar] [CrossRef] [PubMed]
- Hong, C.; Xie, H.Y.; Ge, W.K.; Yu, M.; Lin, S.N.; Liu, C.J. The efficacy of parecoxib in improving pain after total knee or total hip arthroplasty: Systematic review and meta-analysis. Medicine 2022, 101, e30748. [Google Scholar] [CrossRef]
- Geng, X.; Zhou, S.; Zhang, X.; Liu, X.; Cheng, X.; Jiang, L.; Zhang, D. The Efficacy and Safety of Celecoxib for Pain Management After Total Knee Arthroplasty: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Surg. 2022, 9, 791513. [Google Scholar] [CrossRef] [PubMed]
- Stiller, C.O.; Hjemdahl, P. Lessons from 20 years with COX-2 inhibitors: Importance of dose-response considerations and fair play in comparative trials. J. Intern. Med. 2022, 292, 557–574. [Google Scholar] [CrossRef]
- Coskun Benlidayi, I. Are non-steroidal anti-inflammatory drugs safe and effective in patients with acute gout? A Cochrane review summary with commentary. Int. J. Rheum. Dis. 2023, 26, 1178–1182. [Google Scholar] [CrossRef]
- Oms Arias, M.; Morral Parente, R.M. Are COX-2 inhibitors indicated for patients at risk? Aten. Primaria 2002, 29, 230–232. [Google Scholar] [CrossRef]
- LaForge, J.M.; Urso, K.; Day, J.M.; Bourgeois, C.W.; Ross, M.M.; Ahmadzadeh, S.; Shekoohi, S.; Cornett, E.M.; Kaye, A.M.; Kaye, A.D. Non-steroidal Anti-inflammatory Drugs: Clinical Implications, Renal Impairment Risks, and AKI. Adv. Ther. 2023, 40, 2082–2096. [Google Scholar] [CrossRef]
- Giercksky, K.E.; Haglund, U.; Rask-Madsen, J. Selective inhibitors of COX-2 are they safe for the stomach? Scand. J. Gastroenterol. 2000, 35, 1121–1124. [Google Scholar] [CrossRef]
- Vase, L. Can insights from placebo and nocebo mechanisms studies improve the randomized controlled trial? Scand. J. Pain 2020, 20, 451–467. [Google Scholar] [CrossRef]
- Diener, H.C.; Schorn, C.F.; Bingel, U.; Dodick, D.W. The importance of placebo in headache research. Cephalalgia Int. J. Headache 2008, 28, 1003–1011. [Google Scholar] [CrossRef]
- Dobrilla, G.; Scarpignato, C. Placebo and placebo effect: Their impact on the evaluation of drug response in patients. Dig. Dis. 1994, 12, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Vase, L.; Riley, J.L., III; Price, D.D. A comparison of placebo effects in clinical analgesic trials versus studies of placebo analgesia. Pain 2002, 99, 443–452. [Google Scholar] [CrossRef] [PubMed]
- Urrútia, G.; Bonfill, X. Declaración PRISMA: Una propuesta para mejorar la publicación de revisiones sistemáticas y metaanálisis [PRISMA declaration: A proposal to improve the publication of systematic reviews and meta-analyses]. Med. Clin. 2010, 135, 507–511. [Google Scholar] [CrossRef] [PubMed]
- Dawson, B.; Trapp, R.G. Bioestadística Médica, 4th ed.; Editorial El Manual Moderno: Guanajuato, Mexico, 2005. [Google Scholar]
- Argimon-Pallás, J.M.; Jiménez-Villa, J. Métodos de Investigación Clínica y Epidemiológica, 5th ed.; Elsevier: Barcelona, Spain, 2019. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID Study and Study Design | Treatments (n) | Details of Patients, Surgical Procedure, and Evaluation | Authors’ Conclusion |
|---|---|---|---|
| Gong et al., 2013 [24]. Randomized, double-blind, placebo-controlled, and parallel-group clinical trial. | Group A: Celecoxib 300 mg twice daily orally and eperisone hydrochloride 50 mg thrice daily orally for 14 days (n = 50). Group B: Celecoxib 300 mg twice daily orally and placebo thrice daily (n = 48). Group C: Placebo (n = 49). | Patients with degenerative arthritis in the knee joint with grade III muscle strength and between 50 and 75 years of age who required total knee arthroplasty were included. The surgery was performed under general anesthesia, was controlled with a tourniquet, and used in all cases a CR prosthesis (Gemini, MK-II. Link). A thromboprophylaxis protocol of rivaroxaban 10 mg per day was used. Morphine (patient-controlled analgesia) was used during the hospital stay. Antibiotic prophylaxis with vancomycin or cefotaxime was used. Pain intensity at rest (VAS score), ambulation (VAS score), active range of motion, postoperative morphine intake, and adverse effects were evaluated. | The celecoxib–eperisone combination had better analgesic efficacy compared to celecoxib alone and the placebo. |
| Huang et al., 2008 [25]. Randomized, observer-blind, and parallel-group clinical study. | Group A: Single 400 mg dose of celecoxib 1 h before surgery and 200 mg of celecoxib every 12 h for five days, along with patient-controlled analgesic morphine (n = 40). Group B: Patient-controlled analgesic morphine alone (n = 40). | Patients with osteoarthritis and those over sixty years of age were included. Spinal anesthesia was used. No description of the surgical procedure was provided. Morphine rescue analgesia was utilized. The VAS pain scores, active range of motion, total opioid intake, and adverse effects were evaluated. | Celecoxib was better in all efficacy indicators compared to the control group. |
| Ittichaikulthol et al., 2010 [26]. Randomized, single-blind, placebo-controlled, and parallel-group clinical assay. | Group A: Celecoxib 400 mg orally (n = 40). Group B: Parecoxib 40 mg IV (n = 40). Group C: Placebo orally (n = 40). | ASA-1 and -2 patients, aged 18 to 75 years, for elective knee surgery were included. For general anesthesia, intravenous thiopental 3–5 mg/kg and fentanyl 2 mcg/kg were used and maintained with sevoflurane and 66% nitrous oxide in oxygen. No description of the surgical procedure was provided. Morphine rescue analgesia was employed. Pain scores, morphine intake, sedation scores, and adverse effects were evaluated. | Parecoxib had a better analgesic effect than celecoxib and the placebo. |
| Meunier et al., 2007 [27]. Randomized, double-blind, placebo-controlled, and parallel-group clinical trial. | Group A: Celecoxib 200 mg (n = 24). Group B: Placebo (n = 20). Both treatments were given orally 1 h preoperatively and then twice daily for 3 weeks. | Patients from age 50 to 80 years, ASA-1 and -2, and capacity to give informed consent. Prophylactic treatment with 2 g intravenous cloxacillin was used. Subarachnoid spinal anesthesia with isobaric bupivacaine was used. Sedation with midazolam was used only if necessary. The procedures were performed by three surgeons. Pain VAS scores, active range of motion, and ketobemidone intake were assessed. | Similar clinical efficacy was observed between celecoxib and the placebo. |
| Schroer et al., 2011 [28]. Randomized, double-blind, placebo-controlled, and parallel-group clinical assay. | Group A: Celecoxib 200 mg orally twice daily for six weeks (n = 53). Group B: Placebo orally (n = 54) | Spinal anesthesia was used. The surgical procedures were conducted by the same surgeon with a minisubvastus technique. Morphine (patient-controlled analgesia) was used during hospital stay. Narcotic intake, knee flexion, Knee Society Score, Oxford Knee Score, and Short-Form 12 scores were evaluated. | Celecoxib induced better postoperative pain relief and faster recovery than the placebo. |
| Zhou et al., 2023 [29]. Randomized, double-blind, placebo-controlled, and parallel-group clinical study. | Group A: Celecoxib 200 mg and placebo 150 mg (n = 38). Group B: Pregabalin 150 mg and placebo 200 mg (n = 38). Group C: Celecoxib 200 mg and pregabalin 150 mg (n = 37). Group D: Placebo 200 mg and placebo 150 mg (n = 36). The treatments were given orally 2 h before surgery. | Patients who received elective, initial, and single total knee arthroplasty treatment were included. ASA-4 patients were excluded. General anesthesia before surgery was used, and a peripheral infiltration (0.5% ropivacaine, 10 mg/mL triamcinolone acetonide acetate, 0.1% epinephrine hydrochloride) was given to all patients after surgery. No description of the surgical procedure was provided. Pain scores at rest and with movement, opioid intake, hs-CRP level, maximal knee flexion range of motion, time to first analgesia after surgery, and adverse effects were evaluated. | The drug combination had a better analgesic effect and decreased the intake of analgesics after surgery. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gómez-Sánchez, E.; Hernández-Gómez, A.; Guzmán-Flores, J.M.; Alonso-Castro, A.J.; Serafín-Higuera, N.A.; Balderas-Peña, L.M.-A.; Franco-de la Torre, L.; Isiordia-Espinoza, M.A. Celecoxib Decreases the Need for Rescue Analgesics after Total Knee Arthroplasty: A Meta-Analysis. Clin. Pract. 2024, 14, 461-472. https://doi.org/10.3390/clinpract14020035
Gómez-Sánchez E, Hernández-Gómez A, Guzmán-Flores JM, Alonso-Castro AJ, Serafín-Higuera NA, Balderas-Peña LM-A, Franco-de la Torre L, Isiordia-Espinoza MA. Celecoxib Decreases the Need for Rescue Analgesics after Total Knee Arthroplasty: A Meta-Analysis. Clinics and Practice. 2024; 14(2):461-472. https://doi.org/10.3390/clinpract14020035
Chicago/Turabian StyleGómez-Sánchez, Eduardo, Adriana Hernández-Gómez, Juan Manuel Guzmán-Flores, Angel Josabad Alonso-Castro, Nicolás Addiel Serafín-Higuera, Luz Ma.-Adriana Balderas-Peña, Lorenzo Franco-de la Torre, and Mario Alberto Isiordia-Espinoza. 2024. "Celecoxib Decreases the Need for Rescue Analgesics after Total Knee Arthroplasty: A Meta-Analysis" Clinics and Practice 14, no. 2: 461-472. https://doi.org/10.3390/clinpract14020035