

Segmental Rectum Resection for Deep Endometriosis and Excision Similarly Improve Sexual Function and Pain


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study
2.2. Outcome
2.3. Surgery
2.4. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sampson, J.A. Perforating hemorrhagic (chocolate) cysts of the ovary. Their importance and especially their relation to pelvic adenomas of the endometrial type. Arch. Surg. 1921, 3, 245–323. [Google Scholar] [CrossRef] [Green Version]
- Koninckx, P.R.; Ussia, A.; Porpora, M.G.; Malzoni, M.; Adamyan, L.; Wattiez, A. Surgical management of endometriosis-associated pain. Minerva Obstet. Gynecol. 2021, 73, 588–605. [Google Scholar] [CrossRef] [PubMed]
- Fairbanks, F.; Abdo, C.H.; Baracat, E.C.; Podgaec, S. Endometriosis doubles the risk of sexual dysfunction: A cross-sectional study in a large amount of patients. Gynecol. Endocrinol. 2017, 33, 544–547. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Xu, X.; Lin, L.; Xu, K.; Xu, M.; Ye, J.; Shen, X. Sexual function in patients with endometriosis: A prospective case–control study in China. J. Int. Med. Res. 2021, 49, 030006052110043. [Google Scholar] [CrossRef] [PubMed]
- Bernays, V.; Schwartz, A.K.; Geraedts, K.; Rauchfuss, M.; Wolfler, M.M.; Haeberlin, F.; von Orelli, S.; Eberhard, M.; Imthurn, B.; Fink, D.; et al. Qualitative and quantitative aspects of sex life in the context of endometriosis: A multicentre case control study. Reprod. Biomed. Online 2020, 40, 296–304. [Google Scholar] [CrossRef]
- Fritzer, N.; Haas, D.; Oppelt, P.; Renner, S.; Hornung, D.; Wolfler, M.; Ulrich, U.; Fischerlehner, G.; Sillem, M.; Hudelist, G. More than just bad sex: Sexual dysfunction and distress in patients with endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 169, 392–396. [Google Scholar] [CrossRef]
- Jia, S.Z.; Leng, J.H.; Sun, P.R.; Lang, J.H. Prevalence and associated factors of female sexual dysfunction in women with endometriosis. Obstet. Gynecol. 2013, 121, 601–606. [Google Scholar] [CrossRef]
- Perez-Lopez, F.R.; Ornat, L.; Perez-Roncero, G.R.; Lopez-Baena, M.T.; Sanchez-Prieto, M.; Chedraui, P. The effect of endometriosis on sexual function as assessed with the Female Sexual Function Index: Systematic review and meta-analysis. Gynecol. Endocrinol. 2020, 36, 1015–1023. [Google Scholar] [CrossRef]
- Di Donato, N.; Montanari, G.; Benfenati, A.; Monti, G.; Bertoldo, V.; Mauloni, M.; Seracchioli, R. Do women with endometriosis have to worry about sex? Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 179, 69–74. [Google Scholar] [CrossRef]
- Pluchino, N.; Wenger, J.M.; Petignat, P.; Tal, R.; Bolmont, M.; Taylor, H.S.; Bianchi-Demicheli, F. Sexual function in endometriosis patients and their partners: Effect of the disease and consequences of treatment. Hum. Reprod. Update 2016, 22, 762–774. [Google Scholar] [CrossRef] [Green Version]
- Rossi, V.; Tripodi, F.; Simonelli, C.; Galizia, R.; Nimbi, F.M. Endometriosis-associated pain: A review of quality of life, sexual health and couple relationship. Minerva Obstet. Gynecol. 2021, 73, 536–552. [Google Scholar] [CrossRef] [PubMed]
- Barbara, G.; Facchin, F.; Buggio, L.; Somigliana, E.; Berlanda, N.; Kustermann, A.; Vercellini, P. What Is Known and Unknown About the Association Between Endometriosis and Sexual Functioning: A Systematic Review of the Literature. Reprod. Sci. 2017, 24, 1933719117707054. [Google Scholar] [CrossRef] [PubMed]
- Tripoli, T.M.; Sato, H.; Sartori, M.G.; de Araujo, F.F.; Girao, M.J.; Schor, E. Evaluation of quality of life and sexual satisfaction in women suffering from chronic pelvic pain with or without endometriosis. J. Sex. Med. 2011, 8, 497–503. [Google Scholar] [CrossRef]
- Shi, C.; Xu, H.; Zhang, T.; Gao, Y. Endometriosis decreases female sexual function and increases pain severity: A meta-analysis. Arch. Gynecol. Obstet. 2023, 307, 195–204. [Google Scholar] [CrossRef]
- Mabrouk, M.; Montanari, G.; Guerrini, M.; Villa, G.; Solfrini, S.; Vicenzi, C.; Mignemi, G.; Zannoni, L.; Frasca, C.; Di Donato, N.; et al. Does laparoscopic management of deep infiltrating endometriosis improve quality of life? A prospective study. Health Qual. Life Outcomes 2011, 9, 98. [Google Scholar] [CrossRef] [Green Version]
- Bray-Beraldo, F.; Pellino, G.; Ribeiro, M.A.F., Jr.; Pereira, A.M.G.; Lopes, R.G.C.; Mabrouk, M.; Di Saverio, S. Evaluation of Bowel Function After Surgical Treatment for Intestinal Endometriosis: A Prospective Study. Dis. Colon Rectum 2021, 64, 1267–1275. [Google Scholar] [CrossRef]
- Di Donato, N.; Montanari, G.; Benfenati, A.; Monti, G.; Leonardi, D.; Bertoldo, V.; Facchini, C.; Raimondo, D.; Villa, G.; Seracchioli, R. Sexual function in women undergoing surgery for deep infiltrating endometriosis: A comparison with healthy women. J. Fam. Plan. Reprod. Health Care 2015, 41, 278–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riiskjaer, M.; Greisen, S.; Glavind-Kristensen, M.; Kesmodel, U.S.; Forman, A.; Seyer-Hansen, M. Pelvic organ function before and after laparoscopic bowel resection for rectosigmoid endometriosis: A prospective, observational study. BJOG 2016, 123, 1360–1367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrero, S.; Abbamonte, L.H.; Giordano, M.; Ragni, N.; Remorgida, V. Deep dyspareunia and sex life after laparoscopic excision of endometriosis. Hum. Reprod. 2007, 22, 1142–1148. [Google Scholar] [CrossRef] [Green Version]
- Ferrero, S.; Abbamonte, L.H.; Parisi, M.; Ragni, N.; Remorgida, V. Dyspareunia and quality of sex life after laparoscopic excision of endometriosis and postoperative administration of triptorelin. Fertil. Steril. 2007, 87, 227–229. [Google Scholar] [CrossRef]
- Martínez-Zamora, M.-A.; Coloma, J.L.; Gracia, M.; Rius, M.; Castelo-Branco, C.; Carmona, F. Long-term Follow-up of Sexual Quality of Life after Laparoscopic Surgery in Patients with Deep Infiltrating Endometriosis. J. Minim. Invasive Gynecol. 2021, 28, 1912–1919. [Google Scholar] [CrossRef] [PubMed]
- Lukic, A.; Di Properzio, M.; De Carlo, S.; Nobili, F.; Schimberni, M.; Bianchi, P.; Prestigiacomo, C.; Moscarini, M.; Caserta, D. Quality of sex life in endometriosis patients with deep dyspareunia before and after laparoscopic treatment. Arch Gynecol. Obstet. 2016, 293, 583–590. [Google Scholar] [CrossRef]
- Malekmaleki, S.; Shahali, S.; Moini, A. Sexual self-efficacy and sexual quality of life before and after laparoscopic surgery in women with endometriosis lesions: A cross-sectional study. Int. J. Reprod. Biomed. 2022, 20, 469–476. [Google Scholar] [CrossRef] [PubMed]
- Halici, B.N.A.; Aktoz, F.; Kabakci, M.; Kiran, G.; Ozcan, P. Analysis of preoperative and postoperative quality of life, sexual function, and sleep in patients with endometriosis: A prospective cohort study. Arch. Gynecol. Obstet. 2022, 307, 113–120. [Google Scholar] [CrossRef] [PubMed]
- Dior, U.P.; Reddington, C.; Cheng, C.; Levin, G.; Healey, M. Sexual Function of Women With Deep Endometriosis Before and After Surgery: A Prospective Study. J. Sex. Med. 2022, 19, 280–289. [Google Scholar] [CrossRef] [PubMed]
- Harvey, M.A.; Chih, H.J.; Geoffrion, R.; Amir, B.; Bhide, A.; Miotla, P.; Rosier, P.; Offiah, I.; Pal, M.; Alas, A.N. International Urogynecology Consultation Chapter 1 Committee 5: Relationship of pelvic organ prolapse to associated pelvic floor dysfunction symptoms: Lower urinary tract, bowel, sexual dysfunction and abdominopelvic pain. Int. Urogynecol. J. 2021, 32, 2575–2594. [Google Scholar] [CrossRef]
- Guan, Y.; Yu, G.; Wang, G.; Bai, Z. The negative effect of urologic chronic pelvic pain syndrome on female sexual function: A systematic review and meta-analysis. Int. Urogynecol. J. 2019, 30, 1807–1816. [Google Scholar] [CrossRef]
- Tam, T.; Levine, E.M. Female Sexual Dysfunction in Women with Pelvic Pain. Semin. Reprod. Med. 2018, 36, 152–158. [Google Scholar] [CrossRef]
- Dhingra, C.; Kellogg-Spadt, S.; McKinney, T.B.; Whitmore, K.E. Urogynecological causes of pain and the effect of pain on sexual function in women. Female Pelvic Med. Reconstr. Surg. 2012, 18, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Wahl, K.J.; Imtiaz, S.; Lisonek, M.; Joseph, K.S.; Smith, K.B.; Yong, P.J.; Cox, S.M. Dyspareunia in Their Own Words: A Qualitative Description of Endometriosis-Associated Sexual Pain. Sex. Med. 2021, 9, 100274. [Google Scholar] [CrossRef]
- Paulo Leonardo-Pinto, J.; Laguna Benetti-Pinto, C.; Angerame Yela, D. When Solving Dyspareunia Is Not Enough to Restore Sexual Function in Women With Deep Infiltrating Endometriosis Treated With Dienogest. J. Sex Marital. Ther. 2019, 45, 44–49. [Google Scholar] [CrossRef]
- Shum, L.K.; Bedaiwy, M.A.; Allaire, C.; Williams, C.; Noga, H.; Albert, A.; Lisonkova, S.; Yong, P.J. Deep Dyspareunia and Sexual Quality of Life in Women With Endometriosis. Sex. Med. 2018, 6, 224–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritzer, N.; Tammaa, A.; Haas, D.; Oppelt, P.; Renner, S.; Hornung, D.; Wolfler, M.; Ulrich, U.; Hudelist, G. When sex is not on fire: A prospective multicentre study evaluating the short-term effects of radical resection of endometriosis on quality of sex life and dyspareunia. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 197, 36–40. [Google Scholar] [CrossRef] [PubMed]
- De Graaff, A.A.; Van Lankveld, J.; Smits, L.J.; Van Beek, J.J.; Dunselman, G.A. Dyspareunia and depressive symptoms are associated with impaired sexual functioning in women with endometriosis, whereas sexual functioning in their male partners is not affected. Hum. Reprod. 2016, 31, 2577–2586. [Google Scholar] [CrossRef] [Green Version]
- Fritzer, N.; Tammaa, A.; Salzer, H.; Hudelist, G. Dyspareunia and quality of sex life after surgical excision of endometriosis: A systematic review. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 173, 1–6. [Google Scholar] [CrossRef]
- Vercellini, P.; Somigliana, E.; Buggio, L.; Barbara, G.; Frattaruolo, M.P.; Fedele, L. “I Can’t Get No Satisfaction”: Deep dyspareunia and sexual functioning in women with rectovaginal endometriosis. Fertil. Steril. 2012, 98, 1503–1511.e1. [Google Scholar] [CrossRef]
- Ferrero, S.; Esposito, F.; Abbamonte, L.H.; Anserini, P.; Remorgida, V.; Ragni, N. Quality of sex life in women with endometriosis and deep dyspareunia. Fertil. Steril. 2005, 83, 573–579. [Google Scholar] [CrossRef] [PubMed]
- Cozzolino, M.; Magro-Malosso, E.R.; Tofani, L.; Coccia, M.E. Evaluation of sexual function in women with deep infiltrating endometriosis. Sex. Reprod. Healthc. 2018, 16, 6–9. [Google Scholar] [CrossRef]
- Evangelista, A.; Dantas, T.; Zendron, C.; Soares, T.; Vaz, G.; Oliveira, M.A. Sexual function in patients with deep infiltrating endometriosis. J. Sex. Med. 2014, 11, 140–145. [Google Scholar] [CrossRef]
- Yong, P.J. Deep dyspareunia: A narrative review of impact on sexual function and quality of life. Minerva Obstet. Gynecol. 2022, 74, 222–233. [Google Scholar] [CrossRef]
- Wattiez, A.; Puga, M.; Albornoz, J.; Faller, E. Surgical strategy in endometriosis. Best Pract. Res. Clin. Obstet. Gynaecol. 2013, 27, 381–392. [Google Scholar] [CrossRef] [PubMed]
- Donnez, O.; Donnez, J. Deep endometriosis: The place of laparoscopic shaving. Best Pract. Res. Clin. Obs. Gynaecol. 2021, 71, 100–113. [Google Scholar] [CrossRef]
- Koninckx, P.R.; Ussia, A.; Adamian, L.; Alsuwaidi, S.; Amro, B.; Gharbi, H.; Tahlak, M.; Wattiez, A. Conservative Surgery of Deep Bowel Endometriosis. In Clinical Management of Bowel Endometriosis; Ferrero, S., Ceccaroni, M., Eds.; Springer Nature: Cham, Swizerland, 2020; pp. 119–134. [Google Scholar]
- Kondo, W.; Ribeiro, R.; Zomer, M.T.; Hayashi, R.; Ferreira, L.R.; Martin, R.L. Double Discoid Resection in Deep Intestinal Endometriosis. J. Minim. Invasive. Gynecol 2015, 22, S140. [Google Scholar] [CrossRef] [PubMed]
- Kamergorodsky, G.; Lemos, N.; Rodrigues, F.C.; Asanuma, F.Y.; D’Amora, P.; Schor, E.; Girao, M.J. Evaluation of pre- and post-operative symptoms in patients submitted to linear stapler nodulectomy due to anterior rectal wall endometriosis. Surg. Endosc. 2015, 29, 2389–2393. [Google Scholar] [CrossRef] [PubMed]
- Afors, K.; Centini, G.; Fernandes, R.; Murtada, R.; Zupi, E.; Akladios, C.; Wattiez, A. Segmental and Discoid Resection are Preferential to Bowel Shaving for Medium-Term Symptomatic Relief in Patients With Bowel Endometriosis. J. Minim. Invasive Gynecol. 2016, 23, 1123–1129. [Google Scholar] [CrossRef]
- Ribeiro, P.A.; Rodrigues, F.C.; Kehdi, I.P.; Rossini, L.; Abdalla, H.S.; Donadio, N.; Aoki, T. Laparoscopic resection of intestinal endometriosis: A 5-year experience. J. Minim. Invasive Gynecol. 2006, 13, 442–446. [Google Scholar] [CrossRef]
- Koninckx, P.R.; Ussia, A.; Alsuwaidi, S.; Amro, B.; Keckstein, J.; Adamyan, L.; Donnez, J.; Dan, M.C.; Wattiez, A. Reconsidering evidence-based management of endometriosis. Facts Views Vis. ObGyn 2022, 14, 225–233. [Google Scholar] [CrossRef]
- Roman, H.; Merlot, B.; Forestier, D.; Noailles, M.; Magne, E.; Carteret, T.; Tuech, J.T.; Martin, D.C. Nonvisualized palpable bowel endometriotic satellites. Hum. Reprod. 2021, 36, 656–665. [Google Scholar] [CrossRef]
- Roman, H.; Hennetier, C.; Darwish, B.; Badescu, A.; Csanyi, M.; Aziz, M.; Tuech, J.J.; Abo, C. Bowel occult microscopic endometriosis in resection margins in deep colorectal endometriosis specimens has no impact on short-term postoperative outcomes. Fertil. Steril. 2016, 105, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Koninckx, P.R.; Fernandes, R.; Ussia, A.; Schindler, L.; Wattiez, A.; Al-Suwaidi, S.; Amro, B.; Al-Maamari, B.; Hakim, Z.; Tahlak, M. Pathogenesis based Diagnosis and Treatment of endometriosis. Front. Endocrinol. 2021, 12, 745548. [Google Scholar] [CrossRef]
- Koninckx, P.R.; Ussia, A.; Adamyan, L.; Wattiez, A.; Donnez, J. Deep endometriosis: Definition, diagnosis, and treatment. Fertil. Steril. 2012, 98, 564–571. [Google Scholar] [CrossRef] [PubMed]
- Dávalos, M.L.R.; De Cicco, C.; D’hoore, A.; De Decker, B.; Koninckx, P.R. Outcome after rectum or sigmoid resection: A review for gynecologists. J. Minim. Invasive Gynecol. 2007, 14, 33–38. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Martínez, D.; Rodríguez-Infante, A.; Otero-Díez, J.L.; Baldonedo-Cernuda, R.F.; Mosteiro-Díaz, M.P.; García-Flórez, L.J. Is my life going to change?—A review of quality of life after rectal resection. J. Gastrointest. Oncol. 2020, 11, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Hendren, S.K.; O’Connor, B.I.; Liu, M.; Asano, T.; Cohen, Z.; Swallow, C.J.; Macrae, H.M.; Gryfe, R.; McLeod, R.S. Prevalence of male and female sexual dysfunction is high following surgery for rectal cancer. Ann. Surg. 2005, 242, 212–223. [Google Scholar] [CrossRef] [PubMed]
- Keane, C.; Wells, C.; O’Grady, G.; Bissett, I.P. Defining low anterior resection syndrome: A systematic review of the literature. Colorectal. Dis. 2017, 19, 713–722. [Google Scholar] [CrossRef]
- Miacci, F.L.C.; Guetter, C.R.; Moreira, P.H.; Sartor, M.C.; Savio, M.C.; Baldin Júnior, A.; Nóbrega, N.L. Síndrome da ressecção anterior do reto: Fatores preditivos. Rev. do Colégio Bras. de Cir. 2019, 46, e20192361. [Google Scholar] [CrossRef] [Green Version]
- Possover, M. Pathophysiologic explanation for bladder retention in patients after laparoscopic surgery for deeply infiltrating rectovaginal and/or parametric endometriosis. Fertil. Steril. 2014, 101, 754–758. [Google Scholar] [CrossRef]
- De Cicco, C.; Corona, R.; Schonman, R.; Mailova, K.; Ussia, A.; Koninckx, P.R. Bowel resection for deep endometriosis: A systematic review. BJOG 2011, 118, 285–291. [Google Scholar] [CrossRef]
- Scheepers, W.F.W.; Maas, J.W.M.; van de Kar, M.M.A. Bowel function and quality of life following surgery for deep endometriosis. J. Psychosom. Obstet. Gynaecol. 2021, 43, 334–339. [Google Scholar] [CrossRef]
- Bassi, M.A.; Andres, M.P.; Bassi, C.M.; Neto, J.S.; Kho, R.M.; Abrao, M.S. Postoperative Bowel Symptoms Improve over Time after Rectosigmoidectomy for Endometriosis. J. Minim. Invasive Gynecol. 2020, 27, 1316–1323. [Google Scholar] [CrossRef]
- Spagnolo, E.; Zannoni, L.; Raimondo, D.; Ferrini, G.; Mabrouk, M.; Benfenati, A.; Villa, G.; Bertoldo, V.; Seracchioli, R. Urodynamic evaluation and anorectal manometry pre- and post-operative bowel shaving surgical procedure for posterior deep infiltrating endometriosis: A pilot study. J. Minim. Invasive Gynecol. 2014, 21, 1080–1085. [Google Scholar] [CrossRef]
- Ballester, M.; Chereau, E.; Dubernard, G.; Coutant, C.; Bazot, M.; Daraï, E. Urinary dysfunction after colorectal resection for endometriosis: Results of a prospective randomized trial comparing laparoscopy to open surgery. Am. J. Obstet. Gynecol. 2011, 204, 303.e1–303.e6. [Google Scholar] [CrossRef] [PubMed]
- Kavallaris, A.; Mebes, I.; Evagyelinos, D.; Dafopoulos, A.; Beyer, D.A. Follow-up of dysfunctional bladder and rectum after surgery of a deep infiltrating rectovaginal endometriosis. Arch. Gynecol. Obstet. 2011, 283, 1021–1026. [Google Scholar] [CrossRef] [PubMed]
- Lermann, J.; Topal, N.; Renner, S.P.; Beckmann, M.W.; Burghaus, S.; Adler, W.; Heindl, F. Comparison of preoperative and postoperative sexual function in patients with deeply infiltrating endometriosis with and without bowel resection. Eur. J. Obstet. Gynecol. Reprod. Biol. 2019, 239, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Van den Broeck, U.; Meuleman, C.; Tomassetti, C.; D’Hoore, A.; Wolthuis, A.; Van Cleynenbreugel, B.; Vergote, I.; Enzlin, P.; D’Hooghe, T. Effect of laparoscopic surgery for moderate and severe endometriosis on depression, relationship satisfaction and sexual functioning: Comparison of patients with and without bowel resection. Hum. Reprod. 2013, 28, 2389–2397. [Google Scholar] [CrossRef] [Green Version]
- Meston, C.M.; Freihart, B.K.; Handy, A.B.; Kilimnik, C.D.; Rosen, R.C. Scoring and Interpretation of the FSFI: What can be Learned From 20 Years of use? J. Sex. Med. 2020, 17, 17–25. [Google Scholar] [CrossRef]
- Rosen, R.; Brown, C.; Heiman, J.; Leiblum, S.; Meston, C.; Shabsigh, R.; Ferguson, D.; D’Agostino, R., Jr. The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J. Sex Marital Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef]
- Pacagnella Rde, C.; Martinez, E.Z.; Vieira, E.M. Construct validity of a Portuguese version of the Female Sexual Function Index. Cad. Saude Publica 2009, 25, 2333–2344. [Google Scholar] [CrossRef] [Green Version]
- Mengarda, C.V.; Passos, E.P.; Picon, P.; Costa, A.F.; Picon, P.D. Validation of Brazilian Portuguese version of quality of life questionnaire for women with endometriosis (Endometriosis Health Profile Questionnaire—EHP-30). Rev. Bras. Ginecol. Obstet. 2008, 30, 384–392. [Google Scholar] [CrossRef] [Green Version]
- Ribeiro, M.C.; Nakamura, M.U.; Scanavino Mde, T.; Torloni, M.R.; Mattar, R. Female sexual function and gestational diabetes. J. Sex. Med. 2012, 9, 786–792. [Google Scholar] [CrossRef]
- Neijenhuijs, K.I.; Hooghiemstra, N.; Holtmaat, K.; Aaronson, N.K.; Groenvold, M.; Holzner, B.; Terwee, C.B.; Cuijpers, P.; Verdonck-De Leeuw, I.M. The Female Sexual Function Index (FSFI)—A Systematic Review of Measurement Properties. J. Sex. Med. 2019, 16, 640–660. [Google Scholar] [CrossRef]
- Abrao, M.S.; Petraglia, F.; Falcone, T.; Keckstein, J.; Osuga, Y.; Chapron, C. Deep endometriosis infiltrating the recto-sigmoid: Critical factors to consider before management. Hum. Reprod. Update 2015, 21, 329–339. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdalla-Ribeiro, H.; Maekawa, M.M.; Lima, R.F.; de Nicola, A.L.A.; Rodrigues, F.C.M.; Ribeiro, P.A. Intestinal endometriotic nodules with a length greater than 2.25 cm and affecting more than 27% of the circumference are more likely to undergo segmental resection, rather than linear nodulectomy. PLoS ONE 2021, 16, e0247654. [Google Scholar] [CrossRef] [PubMed]
- Tomasi, M.C.; Ribeiro, P.A.A.; Farah, D.; Vidoto Cervantes, G.; Nicola, A.L.; Abdalla-Ribeiro, H.S. Symptoms and Surgical Technique of Bladder Endometriosis: A Systematic Review. J. Minim. Invasive Gynecol. 2022, 29, 1294–1302. [Google Scholar] [CrossRef]
- Quintairos, R.A.; Brito, L.G.O.; Farah, D.; Ribeiro, H.; Ribeiro, P. Conservative versus Radical Surgery for Women with Deep Infiltrating Endometriosis: Systematic Review and Meta-analysis of Bowel Function. J. Minim. Invasive Gynecol. 2022, 29, 1231–1240. [Google Scholar] [CrossRef]
- English, J.; Sajid, M.S.; Lo, J.; Hudelist, G.; Baig, M.K.; Miles, W.A. Limited segmental rectal resection in the treatment of deeply infiltrating rectal endometriosis: 10 years’ experience from a tertiary referral unit. Gastroenterol. Rep. 2014, 2, 288–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- SAS. SAS User’s Guide. In Statistics, Version 5; SAS Institute, Inc.: Cary, NC, USA, 1985. [Google Scholar]
- Farland, L.V.; Correia, K.F.; Wise, L.A.; Williams, P.L.; Ginsburg, E.S.; Missmer, S.A. P-values and reproductive health: What can clinical researchers learn from the American Statistical Association? Hum. Reprod. 2016, 31, 2406–2410. [Google Scholar] [CrossRef] [Green Version]
- Wasserstein, R.L.; Lazar, N.A. The ASA Statement on p-Values: Context, Process, and Purpose. Am. Stat. 2016, 70, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Koninckx, P.R.; Ussia, A.; Keckstein, J.; Malzoni, M.; Adamyan, L.; Wattiez, A. Review on endometriosis surgery. Gynecol. Pelvic Med. 2021, 4, 38. [Google Scholar] [CrossRef]
- Ianieri, M.M.; Raimondo, D.; Rosati, A.; Cocchi, L.; Trozzi, R.; Maletta, M.; Raffone, A.; Campolo, F.; Beneduce, G.; Mollo, A.; et al. Impact of nerve-sparing posterolateral parametrial excision for deep infiltrating endometriosis on postoperative bowel, urinary, and sexual function. Int. J. Gynaecol. Obstet. 2022, 159, 152–159. [Google Scholar] [CrossRef]
- Parish, S.J.; Cottler-Casanova, S.; Clayton, A.H.; McCabe, M.P.; Coleman, E.; Reed, G.M. The Evolution of the Female Sexual Disorder/Dysfunction Definitions, Nomenclature, and Classifications: A Review of DSM, ICSM, ISSWSH, and ICD. Sex. Med. Rev. 2021, 9, 36–56. [Google Scholar] [CrossRef] [PubMed]
- Calabrò, R.S.; Cacciola, A.; Bruschetta, D.; Milardi, D.; Quattrini, F.; Sciarrone, F.; Rosa, G.; Bramanti, P.; Anastasi, G. Neuroanatomy and function of human sexual behavior: A neglected or unknown issue? Brain Behav. 2019, 9, e01389. [Google Scholar] [CrossRef]
- Rossi, V.; Galizia, R.; Tripodi, F.; Simonelli, C.; Porpora, M.G.; Nimbi, F.M. Endometriosis and Sexual Functioning: How Much Do Cognitive and Psycho-Emotional Factors Matter? Int. J. Environ. Res. Public Health 2022, 19, 5319. [Google Scholar] [CrossRef] [PubMed]
- Netzl, J.; Gusy, B.; Voigt, B.; Sehouli, J.; Mechsner, S. Chronic Pelvic Pain in Endometriosis: Cross-Sectional Associations with Mental Disorders, Sexual Dysfunctions and Childhood Maltreatment. J. Clin. Med. 2022, 11, 3714. [Google Scholar] [CrossRef] [PubMed]
- As-Sanie, S.; Till, S.R.; Schrepf, A.D.; Griffith, K.C.; Tsodikov, A.; Missmer, S.A.; Clauw, D.J.; Brummett, C.M. Incidence and predictors of persistent pelvic pain following hysterectomy in women with chronic pelvic pain. Am. J. Obstet. Gynecol. 2021, 225, 568.e1–568.e11. [Google Scholar] [CrossRef]
- Abbott, J.; Hawe, J.; Hunter, D.; Holmes, M.; Finn, P.; Garry, R. Laparoscopic excision of endometriosis: A randomized, placebo-controlled trial. Fertil. Steril. 2004, 82, 878–884. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Linear Nodulectomy n = 23 | Segmental Resection n = 33 | p Value | |
|---|---|---|---|
| Age | 28.9 ± 6.2 | 37.4 ± 5.6 | NS |
| Height (cm) | 162.2 ± 5.5 | 163.0 ± 7.0 | NS |
| Weight (kg) | 74.3 ± 12.4 | 71.8 ± 13.8 | NS |
| Para (deliveries) | 1.4 ± 1.5 | 1.0 ± 1.2 | NS |
| Deep endo volume (mL) | 1.3 ± 1.3 | 6.2 ± 6.9 | 0.0006 |
| Duration of surgery (min) | 186 ± 50 | 204 ± 61 | NS |
| Length of resection (cm) | 1.4 ± 1.3 | 9.7 ± 3.6 | <0.0001 |
| Pain score | 19.5 ± 7.9 | 18.1 ± 8.1 | NS |
| Linear Resection | Segmental Resection | |||||
|---|---|---|---|---|---|---|
| Before | After | p Value | Before | After | p Value | |
| Desire | 3.1 + 1.1 | 3.8 + 1.6 | 0.045 | 2.9 + 1.0 | 3.7 + 1.2 | 0.004 |
| Arousal | 3.0 + 1.1 | 3.8 + 1.6 | 0.004 | 3.1 + 1.0 | 3.9 + 1.4 | 0.004 |
| Lubrification | 3.8 + 1.3 | 4.7 + 1.7 | 0.022 | 4.1 + 1.4 | 4.5 + 1.6 | NS |
| Orgasm | 3.5 + 1.3 | 4.3 + 1.6 | 0.034 | 3.8 + 1.5 | 4.5 + 1.5 | 0.021 |
| Satisfaction | 3.8 + 1.3 | 4.5 + 1.5 | NS | 3.8 + 1.3 | 4.3 + 1.7 | NS |
| Pain | 2.6 + 1.6 | 4.6 + 1.7 | 0.001 | 2.9 + 1.6 | 4.6 + 1.5 | <0.001 |
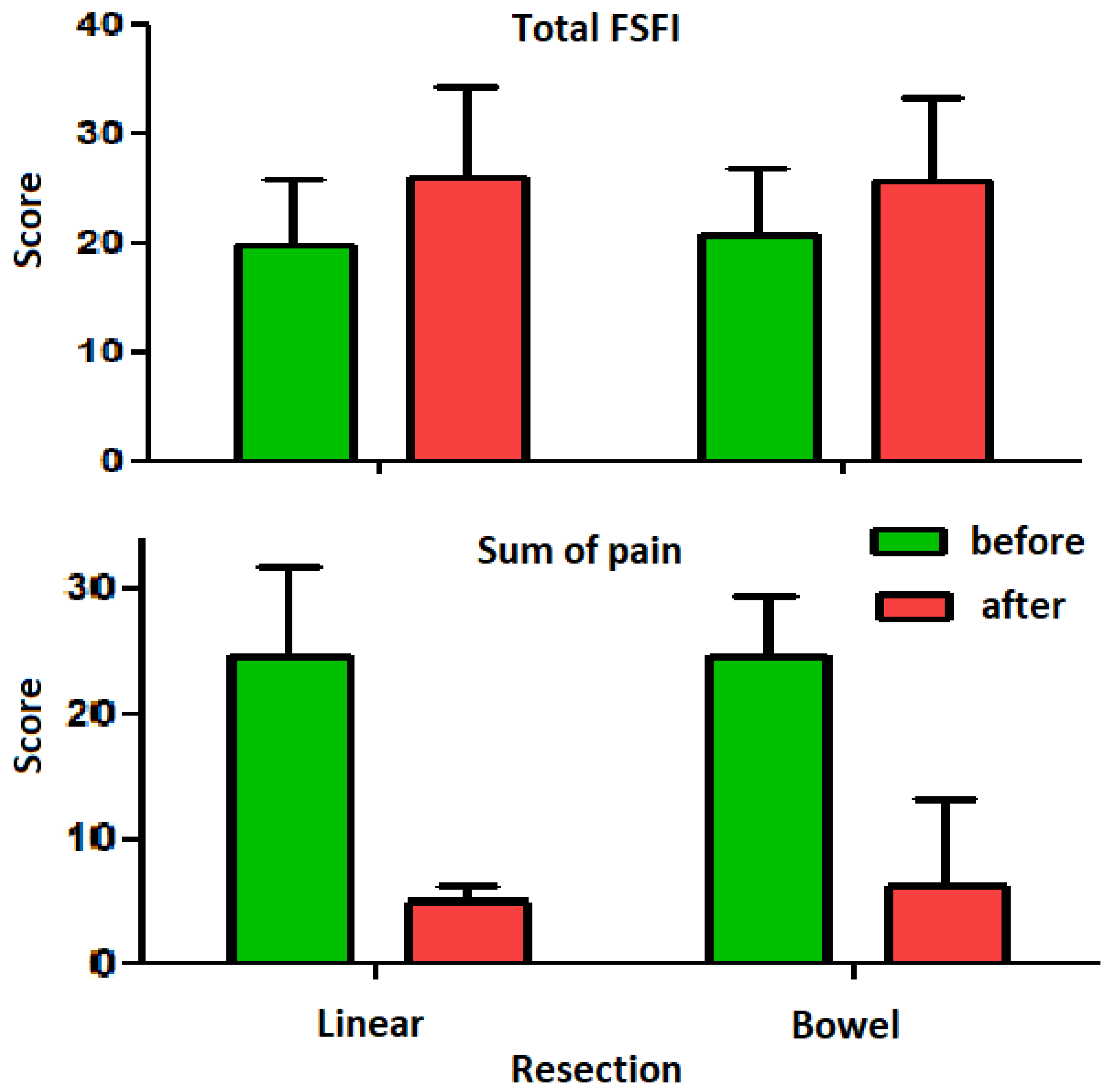
| Tota FSFI | 19.8 + 6.0 | 25.9 + 8.4 | <0.001 | 20.8 + 5.9 | 25.6 + 7.7 | <0.001 |
| EHP-30 | 64.6 + 28.1 | 34.8 + 33.8 | 0.003 | 57.6 + 31.2 | 35.3 + 32.5 | <0.001 |
| Dysmenorrhoea | 9.2 + 1.1 | 1.3 + 2.4 | <0.001 | 8.5 + 2.5 | 6.9 + 3.4 | <0.001 |
| Dyspareunea | 7.0 + 2.9 | 2.0 + 2.8 | <0.001 | 7.1 + 3.3 | 4.9 + 3.8 | <0.001 |
| Dyschesia | 5.2 + 3.4 | 1.4 + 2.8 | 0.005 | 5.3 + 4.0 | 3.5 + 4.5 | 0.001 |
| Dysuria | 1.6 + 2.7 | 0.3 + 0.7 | 0.021 | 1.7 ± 3.5 | 1.4 + 3.1 | 0.017 |
| CPP | 6.5 + 3.6 | 1.3 + 2.4 | <0.001 | 6.9 ± 3.7 | 4.8 + 3.9 | <0.001 |
| The sum of all pain | 24.5 + 7.2 | 4.9 + 1.3 | <0.001 | 24.5 ± 7.2 | 6.2 + 6.9 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asencio, F.d.A.; Fins, R.J.P.; Mitie, C.K.; Ussia, A.; Wattiez, A.; Ribeiro, H.S.; Ribeiro, P.A.; Koninckx, P.R. Segmental Rectum Resection for Deep Endometriosis and Excision Similarly Improve Sexual Function and Pain. Clin. Pract. 2023, 13, 780-790. https://doi.org/10.3390/clinpract13040071
Asencio FdA, Fins RJP, Mitie CK, Ussia A, Wattiez A, Ribeiro HS, Ribeiro PA, Koninckx PR. Segmental Rectum Resection for Deep Endometriosis and Excision Similarly Improve Sexual Function and Pain. Clinics and Practice. 2023; 13(4):780-790. https://doi.org/10.3390/clinpract13040071
Chicago/Turabian StyleAsencio, Fernanda de Almeida, Raphael Jose Palhares Fins, Carolina Kami Mitie, Anastasia Ussia, Arnauld Wattiez, Helizabet Salomao Ribeiro, Paulo Ayrosa Ribeiro, and Philippe Robert Koninckx. 2023. "Segmental Rectum Resection for Deep Endometriosis and Excision Similarly Improve Sexual Function and Pain" Clinics and Practice 13, no. 4: 780-790. https://doi.org/10.3390/clinpract13040071