
Assessment of Tissue Adequacy by EBUS in Conjunction with PET Scan and Operator’s Experience
 ,
, {kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Inclusion/Exclusion Criteria
- Diagnosis of advanced NSCLC, stages III or IV;
- Undergone EBUS at the University of Cincinnati Medical Center;
- Presence of EGFR status.
2.2. Pathalogical Diagnosis and Evaluation of Diagnostic Accuracy
2.3. Statistical Data Analysis Methods
3. Results
3.1. Adequacy of Samples Collected
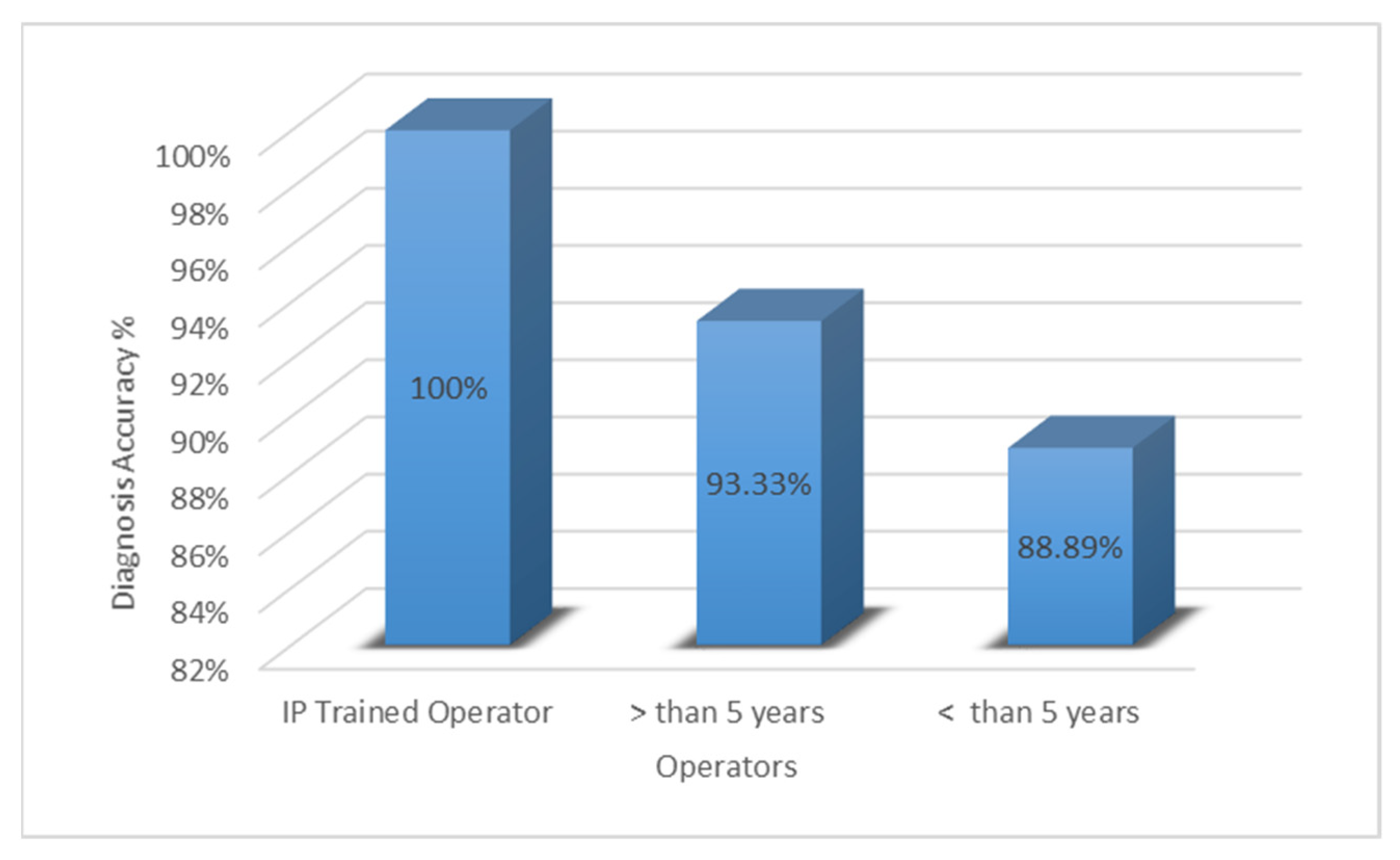
3.2. Effect of Operator Experience
3.3. Diagnostic Accuracy Compared to PET-CT
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ettinger, D.S.; Wood, D.E.; Akerley, W.; Bazhenova, L.A.; Borghaei, H.; Camidge, D.R.; Cheney, R.T.; Chirieac, L.R.; D′Amico, T.A.; Dilling, T.J.; et al. NCCN Guidelines Insights: Non-Small Cell Lung Cancer, Version 4.2016. J. Natl. Compr. Cancer Netw. 2016, 14, 255–264. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eberhardt, W.E.; De Ruysscher, D.; Weder, W.; Le Péchoux, C.; De Leyn, P.; Hoffmann, H.; Westeel, V.; Stahel, R.; Felip, E.; Peters, S. 2nd ESMO Consensus Conference in Lung Cancer: Locally advanced stage III non-small-cell lung cancer. Ann. Oncol. 2015, 26, 1573–1588. [Google Scholar] [CrossRef] [PubMed]
- Sehgal, I.S.; Dhooria, S.; Aggarwal, A.N.; Behera, D.; Agarwal, R. Endosonography Versus Mediastinoscopy in Mediastinal Staging of Lung Cancer: Systematic Review and Meta-Analysis. Ann. Thorac. Surg. 2016, 102, 1747–1755. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karim, N.A.; Schuster, J.; Eldessouki, I.; Gaber, O.; Namad, T.; Wang, J.; Xie, C.; Morris, J.C. Pulmonary sarcomatoid carcinoma: University of Cincinnati experience. Oncotarget 2018, 9, 4102–4108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fischer, B.M.; Lassen, U.; Højgaard, L. PET–CT in Preoperative Staging of Lung Cancer. N. Engl. J. Med. 2011, 364, 980–981. [Google Scholar] [CrossRef]
- Silvestri, G.A.; Gonzalez, A.V.; Jantz, M.A.; Margolis, M.L.; Gould, M.K.; Tanoue, L.T.; Harris, L.J.; Detterbeck, F.C. Methods for staging non-small cell lung cancer: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143, e211S–e250S. [Google Scholar] [CrossRef] [Green Version]
- Madsen, P.H.; Holdgaard, P.C.; Christensen, J.B.; Høilund-Carlsen, P.F. Clinical utility of F-18 FDG PET-CT in the initial evaluation of lung cancer. Eur. J. Pediatr. 2016, 43, 2084–2097. [Google Scholar] [CrossRef]
- Gould, M.K.; Kuschner, W.G.; Rydzak, C.E.; Maclean, C.C.; Demas, A.N.; Shigemitsu, H.; Chan, J.K.; Owens, D.K. Test performance of positron emission tomography and computed tomography for mediastinal staging in patients with non-small-cell lung cancer: A meta-analysis. Ann. Intern. Med. 2003, 139, 879–892. [Google Scholar] [CrossRef]
- Fischer, B.; Lassen, U.; Mortensen, J.; Larsen, S.; Loft, A.; Bertelsen, A.; Ravn, J.; Clementsen, P.; Høgholm, A.; Larsen, K.; et al. Preoperative staging of lung cancer with combined PET-CT. N. Engl. J. Med. 2009, 361, 32–39. [Google Scholar] [CrossRef] [Green Version]
- Karim, N.A.; Eldessouki, I.; Yellu, M.; Namad, T.; Wang, J.; Gaber, O. A Case Study in Advanced Lung Cancer Patients with Vimentin Over Expression. Clin. Lab. 2017, 63, 1575–1579. [Google Scholar] [CrossRef]
- El-Osta, H.; Jani, P.; Mansour, A.; Rascoe, P.; Jafri, S. Endobronchial Ultrasound for Nodal Staging of Patients with Non-Small-Cell Lung Cancer with Radiologically Normal Mediastinum. A Meta-Analysis. Ann. Am. Thorac. Soc. 2018, 15, 864–874. [Google Scholar] [CrossRef] [PubMed]
- Colt, H.G.; Murgu, S.D.; Korst, R.J.; Slatore, C.G.; Unger, M.; Quadrelli, S. Follow-up and surveillance of the patient with lung cancer after curative-intent therapy: Diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013, 143, e437S–e454S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korst, R.J.; Kansler, A.L.; Port, J.L.; Lee, P.C.; Altorki, N.K. Accuracy of surveillance computed tomography in detecting recurrent or new primary lung cancer in patients with completely resected lung cancer. Ann. Thorac. Surg. 2006, 82, 1009–1015, discussion 1015. [Google Scholar] [CrossRef] [PubMed]
- Bury, T.; Corhay, J.L.; Duysinx, B.; Daenen, F.; Ghaye, B.; Barthelemy, N.; Rigo, P.; Bartsch, P. Value of FDG-PET in detecting residual or recurrent nonsmall cell lung cancer. Eur. Respir. J. 1999, 14, 1376–1380. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanzaki, R.; Higashiyama, M.; Maeda, J.; Okami, J.; Hosoki, T.; Hasegawa, Y.; Takami, M.; Kodama, K. Clinical value of F18-fluorodeoxyglucose positron emission tomography-computed tomography in patients with non-small cell lung cancer after potentially curative surgery: Experience with 241 patients. Interact. Cardiovasc. Thorac. Surg. 2010, 10, 1009–1014. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Kim, Y.T.; Kim, S.K.; Kang, K.W.; Goo, J.M.; Kang, C.H.; Kim, J.H. Positron emission tomography-computed tomography for postoperative surveillance in non-small cell lung cancer. Ann. Thorac. Surg. 2011, 92, 1826–1832, discussion 1832. [Google Scholar] [CrossRef] [PubMed]
- Evison, M.; Crosbie, P.A.; Califano, R.; Summers, Y.; Martin, J.; Barber, P.V.; Booton, R. Can EBUS-TBNA provide an accurate diagnosis in patients found to have enlarged or FDG-avid lymph nodes during surveillance of previously treated lung cancer? A retrospective study. J. Bronchol. Interv. Pulmonol. 2015, 22, 114–120. [Google Scholar] [CrossRef]
- Frenel, J.S.; Carreira, S.; Goodall, J.; Roda, D.; Perez-Lopez, R.; Tunariu, N.; Riisnaes, R.; Miranda, S.; Figueiredo, I.; Nava-Rodrigues, D.; et al. Serial Next-Generation Sequencing of Circulating Cell-Free DNA Evaluating Tumor Clone Response To Molecularly Targeted Drug Administration. Clin. Cancer Res. 2015, 21, 4586–4596. [Google Scholar] [CrossRef] [Green Version]
- Shackelford, R.E.; Whitling, N.A.; McNab, P.; Japa, S.; Coppola, D. KRAS Testing: A Tool for the Implementation of Personalized Medicine. Genes Cancer 2012, 3, 459–466. [Google Scholar] [CrossRef] [Green Version]
- Karim, N.; Bahassi, E.-M.; Gaber, O.; Sadraei, N.H.; Morris, J. P2.03a-027 A Phase I Study of the Non-Receptor Tyrsine Kinase Inhibitor (NKI) Bosutinib in Combination with Pemetrexed in Patients with Advanced Solid Tumors: Topic: Clinical Trials. J. Thorac. Oncol. 2017, 12, S904. [Google Scholar] [CrossRef]
- Zingone, A.; Brown, D.; Bowman, E.D.; Vidal, O.; Sage, J.; Neal, J.; Ryan, B.M. Relationship between anti-depressant use and lung cancer survival. Cancer Treat. Res. Commun. 2017, 10, 33–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bent, T.; Yakar, D.; Kwee, T.C. Clinical and FDG-PET/CT Suspicion of Malignant Disease: Is Biopsy Confirmation Still Necessary? Diagnostics 2021, 11, 559. [Google Scholar] [CrossRef] [PubMed]
- Nakajo, M.; Jinguji, M.; Aoki, M.; Tani, A.; Sato, M.; Yoshiura, T. The clinical value of texture analysis of dual-time-point (18)F-FDG-PET/CT imaging to differentiate between (18)F-FDG-avid benign and malignant pulmonary lesions. Eur. Radiol. 2020, 30, 1759–1769. [Google Scholar] [CrossRef] [PubMed]
- Gould, M.K.; Maclean, C.C.; Kuschner, W.G.; Rydzak, C.E.; Owens, D.K. Accuracy of positron emission tomography for diagnosis of pulmonary nodules and mass lesions: A meta-analysis. JAMA 2001, 285, 914–924. [Google Scholar] [CrossRef]
- Jeong, S.Y.; Lee, K.S.; Shin, K.M.; Bae, Y.A.; Kim, B.T.; Choe, B.K.; Kim, T.S.; Chung, M.J. Efficacy of PET/CT in the characterization of solid or partly solid solitary pulmonary nodules. Lung Cancer 2008, 61, 186–194. [Google Scholar] [CrossRef]
- Sehgal, I.S.; Agarwal, R.; Dhooria, S.; Prasad, K.T.; Aggarwal, A.N. Role of EBUS TBNA in Staging of Lung Cancer: A Clinician′s Perspective. J. Cytol. 2019, 36, 61–64. [Google Scholar] [CrossRef]
- Rosell, R.; Carcereny, E.; Gervais, R.; Vergnenegre, A.; Massuti, B.; Felip, E.; Palmero, R.; Garcia-Gomez, R.; Pallares, C.; Sanchez, J.M.; et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): A multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012, 13, 239–246. [Google Scholar] [CrossRef]
- Labarca, G.; Folch, E.; Jantz, M.; Mehta, H.J.; Majid, A.; Fernandez-Bussy, S. Adequacy of Samples Obtained by Endobronchial Ultrasound with Transbronchial Needle Aspiration for Molecular Analysis in Patients with Non-Small Cell Lung Cancer. Systematic Review and Meta-Analysis. Ann. Am. Thorac. Soc. 2018, 15, 1205–1216. [Google Scholar] [CrossRef]
- Sakakibara, R.; Inamura, K.; Tambo, Y.; Ninomiya, H.; Kitazono, S.; Yanagitani, N.; Horiike, A.; Ohyanagi, F.; Matsuura, Y.; Nakao, M.; et al. EBUS-TBNA as a Promising Method for the Evaluation of Tumor PD-L1 Expression in Lung Cancer. Clin. Lung Cancer 2017, 18, 527–534.e521. [Google Scholar] [CrossRef]
- Beamis, J.F.; Becker, H.D.; Cavaliere, S.; Colt, H.; Diaz-Jimenez, J.P.; Dumon, J.F.; Edell, E.; Kovitz, K.L.; Macha, H.N.; Mehta, A.C.; et al. ERS/ATS statement on interventional pulmonology. Eur. Respir. J. 2002, 19, 356. [Google Scholar] [CrossRef]
- Ernst, A.; Silvestri, G.A.; Johnstone, D. Interventional pulmonary procedures: Guidelines from the American College of Chest Physicians. Chest 2003, 123, 1693–1717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hu, Y.; Puri, V.; Crabtree, T.D.; Kreisel, D.; Krupnick, A.S.; Patterson, A.G.; Meyers, B.F. Attaining proficiency with endobronchial ultrasound-guided transbronchial needle aspiration. J. Thorac. Cardiovasc. Surg. 2013, 146, 1387–1392.e1381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stather, D.R.; Chee, A.; MacEachern, P.; Dumoulin, E.; Hergott, C.A.; Gelberg, J.; Folch, E.; Majid, A.; Gonzalez, A.V.; Tremblay, A. Endobronchial ultrasound learning curve in interventional pulmonary fellows. Respirology 2015, 20, 333–339. [Google Scholar] [CrossRef]
- Du Rand, I.A.; Barber, P.V.; Goldring, J.; Lewis, R.A.; Mandal, S.; Munavvar, M.; Rintoul, R.C.; Shah, P.L.; Singh, S.; Slade, M.G.; et al. Summary of the British Thoracic Society guidelines for advanced diagnostic and therapeutic flexible bronchoscopy in adults. Thorax 2011, 66, 1014–1015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Medford, A.R. Learning Curve for EBUS-TBNA: Longer than We May Think. Respiration 2015, 90, 173. [Google Scholar] [CrossRef]
- Wehrmann, T.; Eckardt, A.J.; Riphaus, A. Magnetic resonance cholangiopancreatography (MRCP) for suspected bilio-pancreatic disease: Should the endoscopist take a second look? Z. Gastroenterol. 2013, 51, 204–208. [Google Scholar] [CrossRef]
- Cardoso, A.V.; Neves, I.; Magalhães, A.; Sucena, M.; Barroca, H.; Fernandes, G. The value of rapid on-site evaluation during EBUS-TBNA. Rev. Port. Pneumol. 2015, 21, 253–258. [Google Scholar] [CrossRef]
- Lee, C.K.; Cha, J.M.; Kim, W.J. Endoscopist Fatigue May Contribute to a Decline in the Effectiveness of Screening Colonoscopy. J. Clin. Gastroenterol. 2015, 49, e51–e56. [Google Scholar] [CrossRef] [Green Version]
- Jiang, M.; Sewitch, M.J.; Barkun, A.N.; Joseph, L.; Hilsden, R.J. Endoscopist specialty is associated with colonoscopy quality. BMC Gastroenterol. 2013, 13, 78. [Google Scholar] [CrossRef] [Green Version]
- Yasufuku, K.; Pierre, A.; Darling, G.; de Perrot, M.; Waddell, T.; Johnston, M.; da Cunha Santos, G.; Geddie, W.; Boerner, S.; Le, L.W.; et al. A prospective controlled trial of endobronchial ultrasound-guided transbronchial needle aspiration compared with mediastinoscopy for mediastinal lymph node staging of lung cancer. J. Thorac. Cardiovasc. Surg. 2011, 142, 1393–1400.e1391. [Google Scholar] [CrossRef]
- Yasufuku, K.; Nakajima, T.; Motoori, K.; Sekine, Y.; Shibuya, K.; Hiroshima, K.; Fujisawa, T. Comparison of endobronchial ultrasound, positron emission tomography, and CT for lymph node staging of lung cancer. Chest 2006, 130, 710–718. [Google Scholar] [CrossRef] [PubMed]
- Kandemir, Z.; Sentürk, A.; Ozdemir, E.; Yildirim, N.; Hasanoğlu, H.C.; Keskin, M.; Türkölmez, S. The evaluation of hypermetabolic mediastinal-hilar lymph nodes determined by PET/CT in pulmonary and extrapulmonary malignancies: Correlation with EBUS-TBNA. Turk. J. Med. Sci. 2015, 45, 1234–1242. [Google Scholar] [CrossRef] [PubMed]
- Haranguş, A.; Berindan-Neagoe, I.; Toma, L.; Şimon, I.; Pop, O.; Şimon, M. EBUS in optimizing non-small cell lung cancer diagnosis and treatment. Med. Pharm. Rep. 2021, 94, 176–184. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karim, N.A.; Ullah, A.; Pulliam, S.; Mostafa, A.; Aragaki, A.; Eubanks, A.; Mahajan, A.; Shehata, M.; Benzaquen, S. Assessment of Tissue Adequacy by EBUS in Conjunction with PET Scan and Operator’s Experience. Clin. Pract. 2022, 12, 942-949. https://doi.org/10.3390/clinpract12060099
Karim NA, Ullah A, Pulliam S, Mostafa A, Aragaki A, Eubanks A, Mahajan A, Shehata M, Benzaquen S. Assessment of Tissue Adequacy by EBUS in Conjunction with PET Scan and Operator’s Experience. Clinics and Practice. 2022; 12(6):942-949. https://doi.org/10.3390/clinpract12060099
Chicago/Turabian StyleKarim, Nagla Abdel, Asad Ullah, Steven Pulliam, Ahmed Mostafa, Alejandro Aragaki, Audrey Eubanks, Amit Mahajan, Mahmoud Shehata, and Sadia Benzaquen. 2022. "Assessment of Tissue Adequacy by EBUS in Conjunction with PET Scan and Operator’s Experience" Clinics and Practice 12, no. 6: 942-949. https://doi.org/10.3390/clinpract12060099