
The Early Mobilization of Patients on Extracorporeal Membrane Oxygenation: A Systematic Review

 and
and
Abstract
:1. Introduction
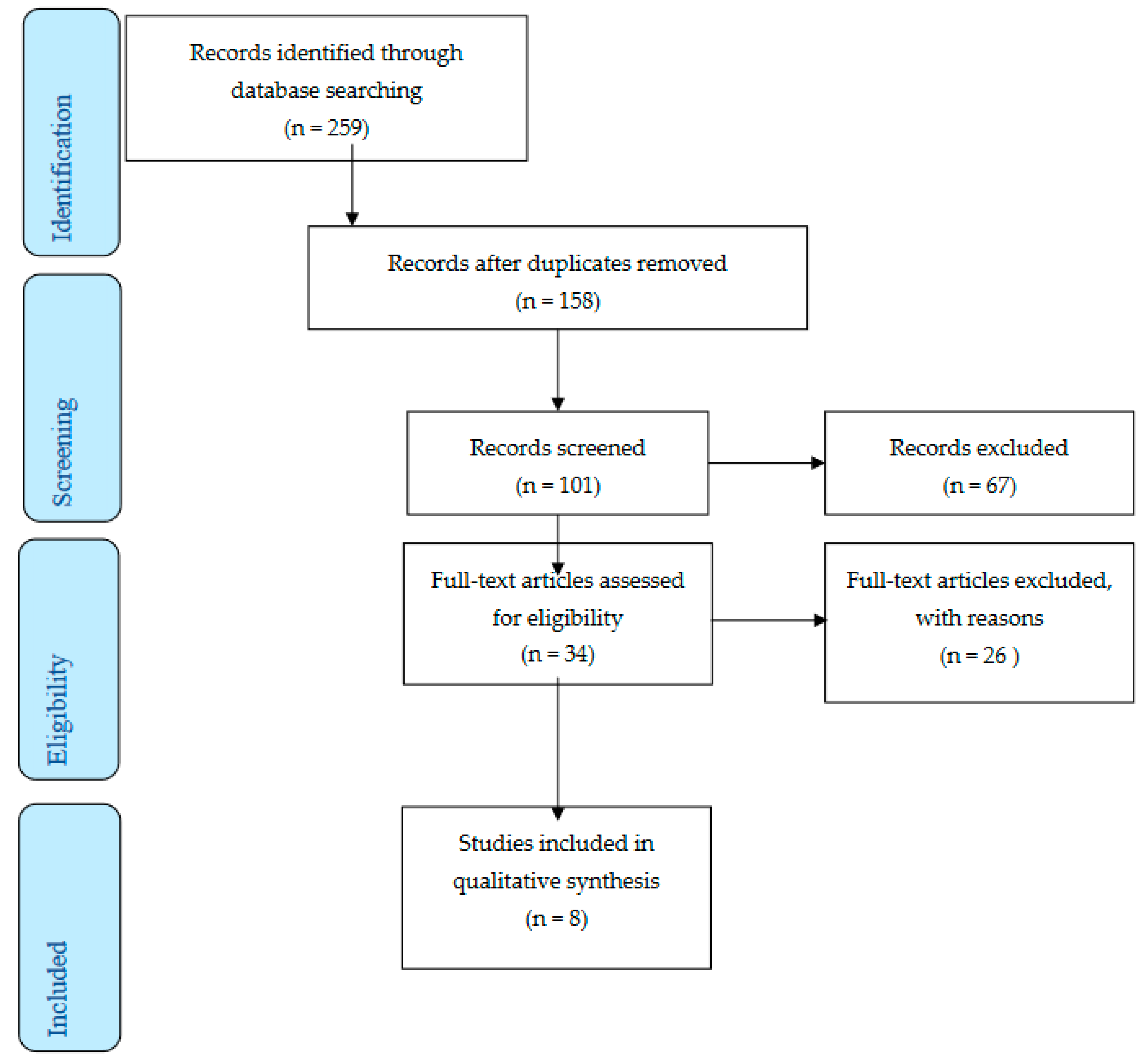
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Abrams, D.; Combes, A.; Brodie, D. Extracorporeal membrane oxygenation in cardiopulmonary disease in adults. J. Am. Coll. Cardiol. 2014, 63, 2769–2778. [Google Scholar] [CrossRef] [PubMed]
- Allen, S.; Holena, D.; McCunn, M.; Kohl, B.; Sarani, B. A review of the fundamental principles and evidence base in the use of extracorporeal membrane oxygenation (ECMO) in critically ill adult patients. J. Intensive Care Med. 2011, 26, 13–26. [Google Scholar] [CrossRef] [PubMed]
- Fan, E.; Dowdy, D.W.; Colantuoni, E.; Mendez-Tellez, P.A.; Sevransky, J.E.; Shanholtz, C.; Himmelfarb, C.R.; Desai, S.V.; Ciesla, N.; Herridge, M.S.; et al. Physical complications in acute lung injury survivors: A two-year longitudinal prospective study. Crit. Care Med. 2014, 42, 849–859. [Google Scholar] [CrossRef] [PubMed]
- Hayes, K.; Holland, A.E.; Pellegrino, V.A.; Leet, A.S.; Fuller, L.M.; Hodgson, C.L. Physical function after extracorporeal membrane oxygenation in patients pre or post heart transplantation—An observational study. Heart Lung 2016, 45, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Todd, E.M.; Biswas Roy, S.; Hashimi, A.S.; Serrone, R.; Panchanathan, R.; Kang, P.; Varsch, K.E.; Steinbock, B.E.; Huang, J.; Omar, A.; et al. Extracorporeal membrane oxygenation as a bridge to lung transplantation: A single-center experience in the present era. J. Thorac. Cardiovasc. Surg. 2017, 154, 1798–1809. [Google Scholar] [CrossRef]
- Weill, D.; Benden, C.; Corris, P.A.; Dark, J.H.; Davis, R.D.; Keshavjee, S.; Lederer, D.J.; Mulligan, M.J.; Patterson, G.A.; Singer, L.G.; et al. A consensus document for the selection of lung transplant candidates: 2014—an update from the Pulmonary Transplantation Council of the International Society for Heart and Lung Transplantation. J. Heart Lung Transplant. Off. Publ. Int. Soc. Heart Transplant. 2015, 34, 1–15. [Google Scholar] [CrossRef]
- Abrams, D.; Brodie, D.; Arcasoy, S.M. Extracorporeal Life Support in Lung Transplantation. Clin. Chest Med. 2017, 38, 655–666. [Google Scholar] [CrossRef]
- Marhong, J.D.; DeBacker, J.; Viau-Lapointe, J.; Munshi, L.; Del Sorbo, L.; Burry, L.; Fan, E.; Mehta, S. Sedation and Mobilization During Venovenous Extracorporeal Membrane Oxygenation for Acute Respiratory Failure: An International Survey. Crit. Care Med. 2017, 45, 1893–1899. [Google Scholar] [CrossRef]
- Wells, C.L.; Forrester, J.; Vogel, J.; Rector, R.; Tabatabai, A.; Herr, D. Safety and Feasibility of Early Physical Therapy for Patients on Extracorporeal Membrane Oxygenator: University of Maryland Medical Center Experience. Crit. Care Med. 2018, 46, 53–59. [Google Scholar] [CrossRef]
- Sauer, C.M.; Yuh, D.D.; Bonde, P. Extracorporeal membrane oxygenation use has increased by 433% in adults in the United States from 2006 to 2011. ASAIO J. (Am. Soc. Artif. Intern. Organs 1992) 2015, 61, 31–36. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Br. Med. J. (Clin. Res. ed.) 2021, 372, n71. [Google Scholar]
- Abrams, D.; Javidfar, J.; Farrand, E.; Mongero, L.B.; Agerstrand, C.L.; Ryan, P.; Zemmel, D.; Galuskin, K.; Morrone, T.M.; Boerem, P.; et al. Early mobilization of patients receiving extracorporeal membrane oxygenation: A retrospective cohort study. Crit. Care 2014, 18, R38. [Google Scholar] [CrossRef] [PubMed]
- Ko, Y.; Cho, Y.H.; Park, Y.H.; Lee, H.; Suh, G.Y.; Yang, J.H.; Park, C.M.; Jeon, K.; Chung, C.R. Feasibility and Safety of Early Physical Therapy and Active Mobilization for Patients on Extracorporeal Membrane Oxygenation. ASAIO J. (Am. Soc. Artif. Intern. Organs 1992) 2015, 61, 564–568. [Google Scholar] [CrossRef] [PubMed]
- Bain, J.C.; Turner, D.A.; Rehder, K.J.; Eisenstein, E.L.; Davis, R.D.; Cheifetz, I.M.; Zaas, D.W. Economic Outcomes of Extracorporeal Membrane Oxygenation With and Without Ambulation as a Bridge to Lung Transplantation. Respir. Care 2016, 61, 1–7. [Google Scholar] [CrossRef]
- Munshi, L.; Kobayashi, T.; DeBacker, J.; Doobay, R.; Telesnicki, T.; Lo, V.; Cote, N.; Cypel, M.; Keshavjee, S.; Ferguson, N.D.; et al. Intensive Care Physiotherapy during Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome. Ann. Am. Thorac. Soc. 2017, 14, 246–253. [Google Scholar] [CrossRef]
- Hayes, K.; Hodgson, C.L.; Pellegrino, V.A.; Snell, G.; Tarrant, B.; Fuller, L.M.; Holland, A.E. Physical Function in Subjects Requiring Extracorporeal Membrane Oxygenation Before or After Lung Transplantation. Respir. Care 2018, 63, 194–202. [Google Scholar] [CrossRef]
- Bonizzoli, M.; Lazzeri, C.; Drago, A.; Tadini Boninsegni, L.; Donati, M.; Di Valvasone, S.; Pesenti, A.; Peris, A. Effects of a physiotherapic program in patients on veno-venous extracorporeal membrane oxygenation: An 8-year single-center experience. Minerva Anestesiol. 2019, 85, 989–994. [Google Scholar] [CrossRef]
- Hayes, K.; Holland, A.E.; Pellegrino, V.A.; Young, M.; Paul, E.; Hodgson, C.L. Early rehabilitation during extracorporeal membrane oxygenation has minimal impact on physiological parameters: A pilot randomised controlled trial. Aust. Crit. Care Off. J. Confed. Aust. Crit. Care Nurses 2021, 34, 217–225. [Google Scholar] [CrossRef]
- Javidfar, J.; Brodie, D.; Wang, D.; Ibrahimiye, A.N.; Yang, J.; Zwischenberger, J.B.; Sonett, J.; Bacchetta, M. Use of bicaval dual-lumen catheter for adult venovenous extracorporeal membrane oxygenation. Ann. Thorac. Surg. 2011, 91, 1763–1769. [Google Scholar] [CrossRef]
- Wang, D.; Zhou, X.; Liu, X.; Sidor, B.; Lynch, J.; Zwischenberger, J.B. Wang-Zwische double lumen cannula-toward a percutaneous and ambulatory paracorporeal artificial lung. ASAIO J. (Am. Soc. Artif. Intern. Organs 1992) 2008, 54, 606–611. [Google Scholar] [CrossRef]
- Shafii, A.E.; McCurry, K.R. Subclavian insertion of the bicaval dual lumen cannula for venovenous extracorporeal membrane oxygenation. Ann. Thorac. Surg. 2012, 94, 663–665. [Google Scholar] [CrossRef] [PubMed]
- Javidfar, J.; Brodie, D.; Costa, J.; Miller, J.; Jurrado, J.; LaVelle, M.; Newmark, A.; Takayama, H.; Sonett, J.R.; Bacchetta, M. Subclavian artery cannulation for venoarterial extracorporeal membrane oxygenation. ASAIO J. (Am. Soc. Artif. Intern. Organs 1992) 2012, 58, 494–498. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors/Year | Country | Type | N | Intervention | Results |
|---|---|---|---|---|---|
| Abrams et al. [12]/2014 | USA | Retrospective cohort study | 35 | Group 1: patients on ECMO as a bridge to transplant (N = 19) Group 2: patients on ECMO as a bridge to recovery (Ν = 16) |
|
| Ko et al. [13]/2015 | South Korea | Retrospective single-center study | 8 | One group on ECMO |
|
| Bain et al. [14]/2016 | USA | Single-center retrospective cohort study | 9 | Group 1: exercise training (Ν = 5) Group 2: usual care (Ν = 4) |
|
| Wells et al. [9]/2017 | USA | Retrospective cohort study | 254 | Group 1: exercise training group (Ν = 167) Group 2: usual care (Ν = 87) |
|
| Munshi et al. [15]/2017 | Canada | Retrospective cohort study | 107 | Group 1: exercise training (N = 50) Group 2: usual care (N = 11) |
|
| Hayes et al. [16]/2018 | Australia | Retrospective single-center study | 42 | Group 1: patients on ECMO (N = 17) Group 2: patients without ECMO (N = 25) |
|
| Bonizzoli et al. [17]/2019 | Italy | Retrospective observational study | 101 | Group 1: physiotherapy within the 1st week from ECMO (N = 33) Group 2: physiotherapy after the 1st week from ECMO (N = 68) |
|
| Hayes et al. [18]/2021 | Australia | A multicenter randomized controlled study | 15 | Group 1: cardiac rehabilitation moderate intense (N = 7) Group 2: usual care (N = 8) |
|
| Authors/Year | Diagnosis | Group | Results |
|---|---|---|---|
| Abrams et al. [12]/2014 | Refractory respiratory or cardiac failure | Bridge to recovery N = 19 | ECMO blood flow rate pre-PT (LPM, mean ± SD): 3.00 ± 0.99 ECMO blood flow rate during PT (LPM, mean ± SD): 2.92 ± 1.09 ECMO sweep gas flow rate pre-PT (LPM, mean ± SD): 2.39 ± 1.77 ECMO sweep gas flow rate during PT (LPM, mean ± SD): 2.35 ± 1.78 Dose of norepinephrine (mcg/min, median, IQR): 1.3 (0.5 to 2) Dose of vasopressin (units/min): 0.04 Maximum distance ambulated (ft, median, IQR): 170 (55 to 525) |
| Bridge to transplant Ν = 16 | ECMO blood flow rate pre-PT (LPM, mean ± SD): 2.99 ± 0.81 ECMO blood flow rate during PT (LPM, mean ± SD): 3.02 ± 0.82 ECMO sweep gas flow rate pre-PT (LPM, mean ± SD): 3.45 ± 1.71 ECMO sweep gas flow rate during PT (LPM, mean ± SD): 3.46 ± 1.71 Dose of norepinephrine (mcg/min, median, IQR): 3.5 (1.3 to 5) Dose of vasopressin (units/min): 0.04 Maximum distance ambulated (ft, median, IQR): 195 (60 to 398) | ||
| Ko et al. [13]/2015 | Unknown | Bridge to transplantation Ν = 8 | Blood flow before PT: 2.93 ± 0.93 During PT: 3.02 ± 0.90 Sweep gas flow before PT: 4.89 ± 1.78 During PT: 4.90 ± 1.78 |
| Bain et al. [14]/2016 | Unknown | Bridge to transplantation Non-rehabilitation group N = 4 | Pre-transplant: $52,124 ($23,824–69,929) Post-transplant ICU: $143,407 ($112,199–168,993) Post-ICU through discharge: $143,407 ($112,199–168,993) Total hospital: $273,291 ($237,299–374,175) Total: $300,307 ($274,262–394,913) Pre-transplant ICU stay: 12 (4–41) Pre-transplant mechanical ventilation duration: 1 (1–5) Post-transplant mechanical ventilation duration: 29.5 (22–54) Post-transplant ICU stay: 45 (34–56) Post-ICU to discharge stay: 34 (11–63) Total hospital stay: 94 (51–151) ECMO support: 1.5 (1–9) |
| Bridge to transplantation Rehabilitation group N = 5 | Pre-transplant: $98,460 ($38,589–122,111) Post-transplant ICU: $43,929 ($23,611–64,126) Post-ICU through discharge: $15,544 ($11,499–43,870) Total hospital: $209,590 ($166,767–264,536) Total: $244,508 ($219,972–268,914) Pre-transplant ICU stay: 20 (17–30) Pre-transplant mechanical ventilation duration: 12 (5–15) Post-transplant mechanical ventilation duration: 2 (1–5) Post-transplant ICU stay: 8 (6–22) Post-ICU to discharge stay: 11 (7–25) Total hospital stay: 50 (31–63) ECMO support: 9 (5–14) | ||
| Wells et al. [9]/2017 | Unknown | Bridge to transplantation Total N = 254 | Discharge outcomes, N (%) Home: 34 (13.38) Rehabilitation facility: 96 (37.79) Skilled nursing: 10 (2.82) Acute care facility: 5 (1.96) |
| Bridge to transplantation Physical therapy group N = 167 | Discharge outcomes, N (%) Home: 26 (15.56) Rehabilitation facility: 75 (44.91) Skilled nursing: 4 (2.39) Acute care facility: 4 (2.39) | ||
| Munshi et al. [15]/2017 | ARDS | N = 61 | Days on ECMO: 12 (9–19) Duration of mechanical ventilation: 21 (18–34) ICU mortality: 18 (30) In hospital mortality: 18 (30) Complications on ECMO Barotrauma: 4 (7) Limb ischemia: 1 (2) Intracerebral hemorrhage: 1 (2) Heparin induced thrombocytopenia: 4 (7) Air embolism: 1 (2) |
| Hayes et al. [16]/2018 | Cystic fibrosis/bronchiectasis, COPD, asthma, and obliterative bronchiolitis, Pulmonary hypertension, Pulmonary fibrosis, Re-transplant | ΕCMO Ν = 42 | Physical function IMS ICU at discharge: 6 (5–7) IMS at hospital discharge: 10 (9–10) 6MWD at hospital discharge, m: 285 ± 112 6MWD at 3 months, m: 541 ± 133 Discharge destination, N (%) Home: 12 (85.7) In-patient rehabilitation: 2 (14.3) |
| Non-ECMO N = 28 | Physical function IMS ICU at discharge: 7 (6–8) IMS at hospital discharge: 10 (10–10) 6MWD at hospital discharge, m: 384 ± 93 6MWD at 3 months, m: 584 ± 67 Discharge destination, N (%) Home: 28 (100)) In-patient rehabilitation: 0 (0) | ||
| Bonizzoli et al. [17]/2019 | ARDS | Within the first week mobilization N = 33 | ECMO (days) (median, IQR): 7 (2.5–13.5) MV (days) (median, IQR): 11 (5–17.75) LOS (days) (median, IQR): 12 (7.25–21) In-ICU mortality: 12 |
| After the first week N = 68 | ECMO (days) (median, IQR): 11 (8.75–22) MV (days) (median, IQR): 23 (13.75–33.25) LOS (days) (median, IQR): 25 (18.75–36.25) In-ICU mortality:14 | ||
| Hayes et al. [18]/2021 | ARDS, pots lung or heart transplantation primary graft failure, cardiac arrest, cardiac failure- infraction and pulmonary hypertension after lung transplantation | Mobilization group N = 7 | Hospital outcomes In-hospital mortality: 3 (42.9) ECMO duration (days): 8.1 ± 4.9 ECMO duration for survivors: 10.5 ± 5.5 Ventilation (days): 6.2 ± 2.5 Ventilation for survivors: 7.3 ± 2.8 LOS in the ICU (days): 12.9 (7.2 ± 16.7) LOS in the ICU for survivors: 16.7 (14.6 ± 21.6) LOS in the hospital for survivors: 41.9 (34.3 ± 56.4) Mobility milestones Time to first SOOB (days): 12.6 ± 6.6 Time to first stand (days): 5.5 ± 4.5 Time to first walk (days): 16.1 (11.5 ± 21.0) Discharge destination of survivors Home: 4 (100) Inpatient rehabilitation: 0 (0) Transfer to the local acute hospital: 0 (0) |
| Usual care group Ν = 8 | Hospital outcomes In-hospital mortality: 1 (12.5) ECMO duration (days): 10.9 ± 5.5 ECMO duration for survivors: 11.5 ± 5.7 Ventilation (days): 9.2 ± 3.8 Ventilation for survivors: 9.4 ± 4.1 LOS in the ICU (days): 21.4 (15.5 ± 38.5) LOS in the ICU for survivors: 22.2 (16.2 ± 38.5) LOS in the hospital for survivors: 34.4 (29.3 ± 87.2) Mobility milestones Time to first SOOB (days): 12.5 ± 7.7 Time to first stand (days): 20.8 ± 12.3 Time to first walk (days): 21.9 (16.5±52.4) Discharge destination of survivors Home: 3 (43) Inpatient rehabilitation: 3 (43) Transfer to the local acute hospital: 1 (14) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chatziefstratiou, A.A.; Fotos, N.V.; Giakoumidakis, K.; Brokalaki, H. The Early Mobilization of Patients on Extracorporeal Membrane Oxygenation: A Systematic Review. Nurs. Rep. 2023, 13, 751-764. https://doi.org/10.3390/nursrep13020066
Chatziefstratiou AA, Fotos NV, Giakoumidakis K, Brokalaki H. The Early Mobilization of Patients on Extracorporeal Membrane Oxygenation: A Systematic Review. Nursing Reports. 2023; 13(2):751-764. https://doi.org/10.3390/nursrep13020066
Chicago/Turabian StyleChatziefstratiou, Anastasia A., Nikolaos V. Fotos, Konstantinos Giakoumidakis, and Hero Brokalaki. 2023. "The Early Mobilization of Patients on Extracorporeal Membrane Oxygenation: A Systematic Review" Nursing Reports 13, no. 2: 751-764. https://doi.org/10.3390/nursrep13020066