

External Ventricular Drains: Development and Evaluation of a Nursing Clinical Practice Guideline

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Development of the “Clinical Practice Guideline for Critical Patients with EVD”
- (1)
- scoping review on nursing care in patients with EVD; indispensable
- (2)
- quality assessment of the studies included in the scoping review using the Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) approach;
- (3)
- development of the guideline following the framework of Pimenta et al. [21].
2.2. Quality Assessment of the “Clinical Practice Guideline for Critical Patients with EVD”
- (4)
- assessment of the methodological rigor of the guideline, with the application of AGREE II for experts on guidelines assessment;
- (5)
- Delphi study to evaluate experts’ opinion on the recommendations of the guideline.
2.2.1. Assessment of the Methodological Rigor of the Guideline
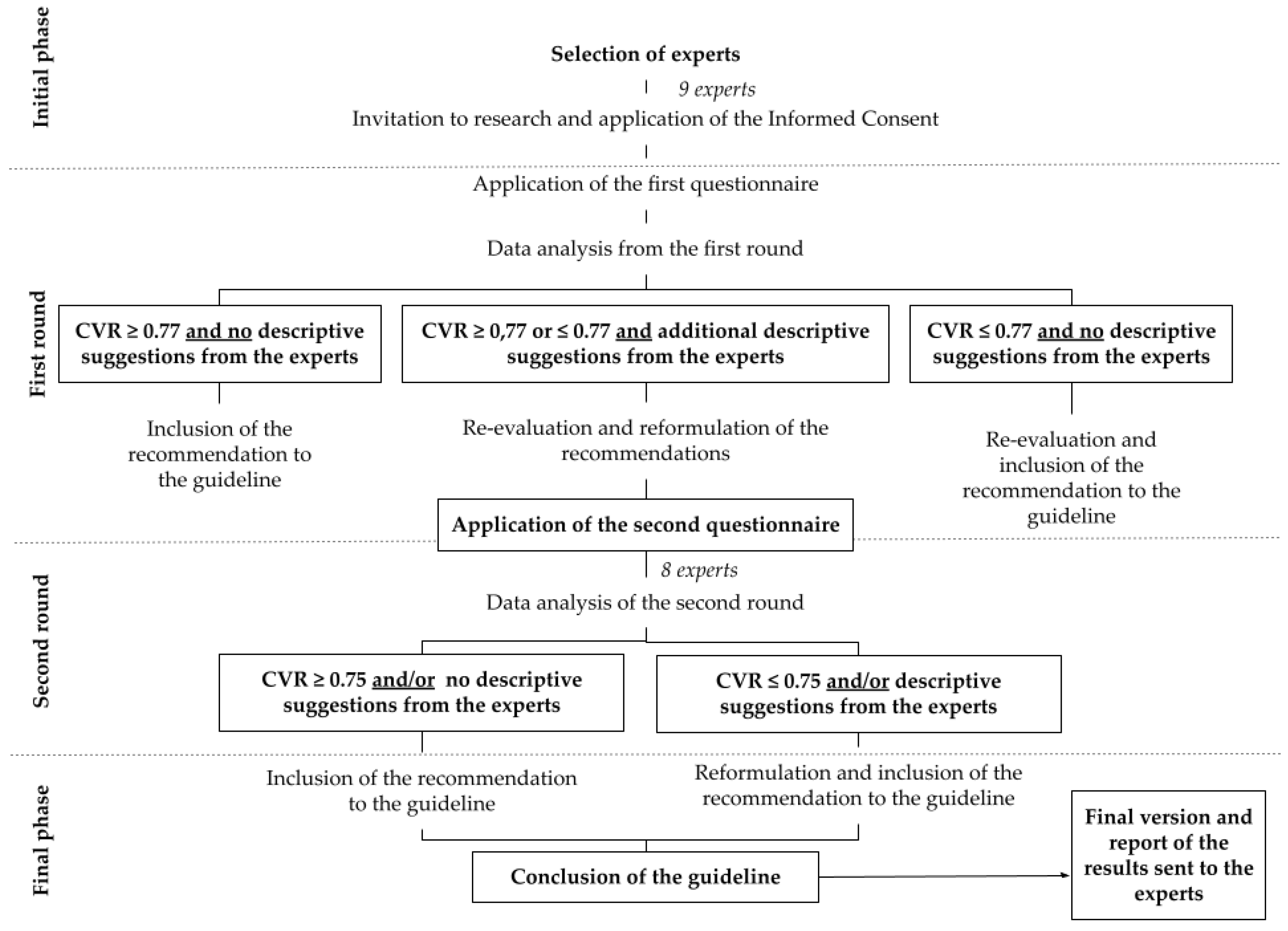
2.2.2. Delphi Study
3. Results
3.1. Development of the Guideline
3.2. Assessment of the Methodological Rigor of the Guideline
3.3. Delphi Study
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chau, C.Y.C.; Craven, C.L.; Rubiano, A.M.; Adams, H.; Tülü, S.; Czosnyka, M.; Servadei, F.; Ercole, A.; Hutchinson, P.J.; Kolias, A.G. The Evolution of the Role of External Ventricular Drainage in Traumatic Brain Injury. J. Clin. Med. 2019, 8, 1422. [Google Scholar] [CrossRef] [Green Version]
- Jamjoom, A.A.B.; Joannides, A.J.; Poon, M.T.-C.; Chari, A.; Zaben, M.; Abdulla, M.A.H.; Roach, J.; Glancz, L.J.; Solth, A.; Duddy, J.; et al. Prospective, multicentre study of external ventricular drainage-related infections in the UK and Ireland. J. Neurol. Neurosurg. Psychiatry 2018, 89, 120–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dossani, R.H.; Patra, D.P.; Terrell, D.L.; Willis, B. Placement of an External Ventricular Drain. N. Engl. J. Med. 2021, 384, e3. [Google Scholar] [CrossRef]
- Arts, S.; van Lindert, E.J.; Aquarius, R.; Bartels, R.H.M.A.; Boogaarts, H.D. Complications of external cerebrospinal fluid drainage in aneurysmal subarachnoid haemorrhage. Acta Neurochir. 2021, 163, 1143–1151. [Google Scholar] [CrossRef] [PubMed]
- Champey, J.; Mourey, C.; Francony, G.; Pavese, P.; Gay, E.; Gergele, L.; Manet, R.; Velly, L.; Bruder, N.; Payen, J.-F. Strategies to reduce external ventricular drain–related infections: A multicenter retrospective study. J. Neurosurg. 2018, 130, 2034–2039. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Whyte, C.; Alhasani, H.; Caplan, R.; Tully, A.P. Impact of an external ventricular drain bundle and limited duration antibiotic prophylaxis on drain-related infections and antibiotic resistance. Clin. Neurol. Neurosurg. 2020, 190, 105641. [Google Scholar] [CrossRef]
- Chung, D.Y.; Olson, D.M.; John, S.; Mohamed, W.; Kumar, M.A.; Thompson, B.B.; Rordorf, G.A. Evidence-Based Management of External Ventricular Drains. Curr. Neurol. Neurosci. Rep. 2019, 19, 94. [Google Scholar] [CrossRef]
- Aten, Q.; Killeffer, J.; Seaver, C.; Reier, L. Causes, Complications, and Costs Associated with External Ventricular Drainage Catheter Obstruction. World Neurosurg. 2020, 134, 501–506. [Google Scholar] [CrossRef]
- Hong, B.; Apedjinou, A.; Heissler, H.E.; Chaib, H.; Lang, J.M.; Al-Afif, S.; Krauss, J.K. Effect of a bundle approach on external ventricular drain-related infection. Acta Neurochir. 2021, 163, 1135–1142. [Google Scholar] [CrossRef]
- Walek, K.W.; Leary, O.P.; Sastry, R.; Asaad, W.F.; Walsh, J.M.; Mermel, L. Decreasing External Ventricular Drain Infection Rates in the Neurocritical Care Unit: 12-Year Longitudinal Experience at a Single Institution. World Neurosurg. 2021, 150, e89–e101. [Google Scholar] [CrossRef]
- Alunpipatthanachai, B.; Thirapattaraphan, P.; Fried, H.; Vavilala, M.S.; Lele, A.V. External Ventricular Drain Management Practices in Thailand: Results of the EPRACT Study. World Neurosurg. 2019, 126, e743–e752. [Google Scholar] [CrossRef] [PubMed]
- Thamjamrassri, T.; Yuwapattanawong, K.; Chanthima, P.; Vavilala, M.S.; Lele, A.V. A Narrative Review of the Published Literature, Hospital Practices, and Policies Related to External Ventricular Drains in the United States: The External Ventricular Drain Publications, Practices, and Policies (EVDPoP) Study. J. Neurosurg. Anesthesiol. 2020, 34, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Hepburn-Smith, M.; Dynkevich, I.; Spektor, M.; Lord, A.; Czeisler, B.; Lewis, A. Establishment of an External Ventricular Drain Best Practice Guideline. J. Neurosci. Nurs. 2016, 48, 54–65. [Google Scholar] [CrossRef] [PubMed]
- Manzo, B.F.; Macedo, K.D.O.; Barbosa, L.M.; Simão, D.A.D.S.; Souza, R.S.; Correa, A.D.R.; Costa, A.C.L. Repercussion of an educational intervention on the knowledge of the nursing team regarding the use of external ventricular drains in pediatrics. REME Rev. Min. Enferm. 2019, 23, e-1189. [Google Scholar] [CrossRef]
- Camacho, E.F.; Boszczowski, I.; Freire, M.P.; Pinto, F.C.G.; Guimaraes, T.; Teixeira, M.J.; Costa, S.F. Impact of an Educational Intervention Implanted in a Neurological Intensive Care Unit on Rates of Infection Related to External Ventricular Drains. PLoS ONE 2013, 8, e50708. [Google Scholar] [CrossRef] [PubMed]
- Sieg, E.P.; Schlauderaff, A.C.; Payne, R.A.; Glantz, M.J.; Simon, S.D. Impact of an External Ventricular Drain Placement and Handling Protocol on Infection Rates: A Meta-Analysis and Single Institution Experience. World Neurosurg. 2018, 115, e53–e58. [Google Scholar] [CrossRef]
- Hall, M.A.L.-V.; Hopmans, T.E.M.; Van Der Sprenkel, J.W.B.; Blok, H.E.M.; Van Der Mark, W.A.M.A.; Hanlo, P.W.; Bonten, M.J.M. A bundle approach to reduce the incidence of external ventricular and lumbar drain-related infections. J. Neurosurg. 2010, 112, 345–353. [Google Scholar] [CrossRef]
- Catapano, J.S.; Rubel, N.C.; Veljanoski, D.; Farber, S.H.; Whiting, A.C.; Morgan, C.; Brigeman, S.; Lawton, M.T.; Zabramski, J.M. Standardized Ventriculostomy Protocol without an Occlusive Dressing: Results of an Observational Study in Patients with Aneurysmal Subarachnoid Hemorrhage. World Neurosurg. 2019, 131, e433–e440. [Google Scholar] [CrossRef]
- Flint, A.C.; Toossi, S.; Chan, S.L.; Rao, V.A.; Sheridan, W. A Simple Infection Control Protocol Durably Reduces External Ventricular Drain Infections to Near-Zero Levels. World Neurosurg. 2017, 99, 518–523. [Google Scholar] [CrossRef]
- Camargo, F.C.; Iwamoto, H.H.; Galvão, C.M.; Pereira, G.D.A.; Andrade, R.B.; Masso, G.C. Competences and Barriers for the Evidence-Based Practice in Nursing: An integrative review. Rev. Bras. Enferm. 2018, 71, 2030–2038. [Google Scholar] [CrossRef]
- Pimenta, C.A.M.; Pastana, I.C.A.S.S.; Sichieri, K.; Solha, R.K.T.; Souza, W. Guia Para Construção de Protocolos Assistenciais de Enfermagem; COREN/SP: São Paulo, Brazil, 2017. Available online: https://portal.coren-sp.gov.br/sites/default/files/Protocolo-web.pdf (accessed on 7 July 2021).
- Gomes, A.T.D.L.; Alves, K.Y.A.; Bezerril, M.D.S.; Rodrigues, C.C.F.M.; Júnior, M.A.F.; Santos, V.E.P. Validação de protocolos gráficos para avaliação da segurança do paciente politraumatizado. Acta Paul. Enferm. 2018, 31, 504–517. [Google Scholar] [CrossRef] [Green Version]
- Sakamoto, V.T.M.; Vieira, T.W.; Viegas, K.; Blatt, C.R.; Caregnato, R.C.A. Nursing assistance in patient care with external ventricular drain: A scoping review. Rev. Bras. Enferm. 2021, 74, e20190796. [Google Scholar] [CrossRef] [PubMed]
- AGREE Next Steps Consortium. The AGREE II Instrument. Hamilton: AGREE Next Steps Consortium. 2017. Available online: https://www.agreetrust.org/wp-content/uploads/2017/12/AGREE-II-Users-Manual-and-23-item-Instrument-2009-Update-2017.pdf (accessed on 7 July 2021).
- Jünger, S.; Payne, S.A.; Brine, J.; Radbruch, L.; Brearley, S.G. Guidance on conducting and Reporting Delphi Studies in pal-liative care> recommendations based on a methodological systematic review. Palliat. Med. 2017, 31, 684–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayre, C.; Scally, A.J. Critical Values for Lawshe’s Content Validity Ratio. Meas. Eval. Couns. Dev. 2014, 47, 79–86. [Google Scholar] [CrossRef] [Green Version]
- Hill, M.; Baker, G.; Carter, D.; Henman, L.J.; Marshall, K.; Mohn, K.; Moody, E. A Multidisciplinary Approach to End External Ventricular Drain Infections in the Neurocritical Care Unit. J. Neurosci. Nurs. 2012, 44, 188–193. [Google Scholar] [CrossRef]
- Humphrey, E. Caring for neurosurgical patients with external ventricular drains. Nurs. Times 2018, 114, 52–56. [Google Scholar]
- Woodward, S.; Addison, C.; Shah, S.; Brennan, F.; MacLeod, A.; Clements, M. Benchmarking best practice for external ventricular drainage. Br. J. Nurs. 2002, 11, 47–53. [Google Scholar] [CrossRef]
- Muralidharan, R. External ventricular drains: Management and complications. Surg. Neurol. Int. 2015, 6, 271–274. [Google Scholar] [CrossRef]
- Omar, A.S.; Elshawarby, A.; Singh, R. Early monitoring of ventriculostomy-related infections with procalcitonin in patients with ventricular drains. Int. J. Clin. Monit. Comput. 2015, 29, 759–765. [Google Scholar] [CrossRef]
- Griesdale, D.E.G.; McEwen, J.; Kurth, T.; Chittock, D.R. External Ventricular Drains and Mortality in Patients with Severe Traumatic Brain Injury. Can. J. Neurol. Sci. J. Can. Des Sci. Neurol. 2010, 37, 43–48. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.H.; Mann, K.S. Prolonged therapeutic external ventricular drainage: A prospective study. Neurosurgery 1988, 23, 436–438. [Google Scholar] [CrossRef] [PubMed]
- Chaikittisilpa, N.; Lele, A.V.; Lyons, V.H.; Nair, B.G.; Newman, S.-F.; Blissitt, P.A.; Vavilala, M.S. Risks of Routinely Clamping External Ventricular Drains for Intrahospital Transport in Neurocritically Ill Cerebrovascular Patients. Neurocrit. Care 2017, 26, 196–204. [Google Scholar] [CrossRef]
- Young, B.; Moyer, M.; Pino, W.; Kung, D.; Zager, E.; Kumar, M.A. Safety and Feasibility of Early Mobilization in Patients with Subarachnoid Hemorrhage and External Ventricular Drain. Neurocrit. Care 2019, 31, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Kumble, S.; Zink, E.K.; Burch, M.; Deluzio, S.; Stevens, R.D.; Bahouth, M.N. Physiological Effects of Early Incremental Mobilization of a Patient with Acute Intracerebral and Intraventricular Hemorrhage Requiring Dual External Ventricular Drainage. Neurocrit. Care 2017, 27, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Shah, S.; Kraft, J.; Ankam, N.; Bu, P.; Stout, K.; Melnyk, S.; Rincon, F.; Athar, M.K. Early Ambulation in Patients With External Ventricular Drains. J. Intensiv. Care Med. 2018, 33, 370–374. [Google Scholar] [CrossRef]
- Stout, D.E.; Cortes, M.X.; Aiyagari, V.; Olson, D.M. Management of External Ventricular Drains During Intrahospital Transport for Radiographic Imaging. J. Radiol. Nurs. 2019, 38, 92–97. [Google Scholar] [CrossRef]
- Barros, L.N.; Uchoa, R.B.; Mejia, J.A.C.; Nunes, R.R.; Barros, D.A.S.N.; Filho, F.R. Anesthetic protocol for right ventricular dysfunction management in heart transplantation: Systematic review, development and validation. BMC Anesthesiol. 2021, 21, 1–9. [Google Scholar] [CrossRef]
- Brasil, R.F.G.; Da Silva, M.J.; Moura, E.R.F. Avaliação da qualidade de protocolo clínico para atendimento em planejamento familiar de pessoas vivendo com HIV/aids. Rev. Esc. Enferm. Da USP 2018, 52, e03335. [Google Scholar] [CrossRef] [Green Version]
- Sousa, D.M.D.N.; Chagas, A.C.M.A.; Vasconcelos, C.; Stein, A.T.; Oriá, M.O.B. Development of a clinical protocol for detection of cervical cancer precursor lesions. Rev. Lat.-Am. Enferm. 2018, 26, e2999. [Google Scholar] [CrossRef] [Green Version]
- Bergman, L.; Pettersson, M.E.; Chaboyer, W.; Carlström, E.D.; Ringdal, M.L. Safety Hazards During Intrahospital Transport. Crit. Care Med. 2017, 45, e1043–e1049. [Google Scholar] [CrossRef]
- Tu, H. Intrafacility Transportation of Patients with Acute Brain Injury. J. Neurosci. Nurs. 2014, 46, E12–E16. [Google Scholar] [CrossRef] [PubMed]
- Capion, T.; Lilja-Cyron, A.; Juhler, M.; Mathiesen, T.I.; Wetterslev, J. Prompt closure versus gradual weaning of external ventricular drainage for hydrocephalus in adult patients with aneurysmal subarachnoid haemorrhage: A systematic review. BMJ Open 2020, 10, e040722. [Google Scholar] [CrossRef] [PubMed]
- Capion, T.; Lilja-Cyron, A.; Bartek, J.; Forsse, A.; Logallo, N.; Juhler, M.; Mathiesen, T. Discontinuation of External Ventricular Drainage in Patients with Hydrocephalus Following Aneurysmal Subarachnoid Hemorrhage—A Scandinavian Multi-institutional Survey. Acta Neurochir. 2020, 162, 1363–1370. [Google Scholar] [CrossRef] [PubMed]
- Jabbarli, R.; Pierscianek, D.; Rölz, R.; Reinhard, M.; Oppong, M.D.; Scheiwe, C.; Dammann, P.; Kaier, K.; Wrede, K.H.; Shah, M.; et al. Gradual External Ventricular Drainage Weaning Reduces the Risk of Shunt Dependency After Aneurysmal Subarachnoid Hemorrhage: A Pooled Analysis. Oper. Neurosurg. 2018, 15, 498–504. [Google Scholar] [CrossRef]
- Caregnato, R.C.A.; Roloff, A.; Sakamoto, V.T.M. Assistência de Enfermagem ao Paciente Neurológico; Moriá: Porto Alegre, Brazil, 2019. [Google Scholar]
- Moyer, M.; Young, B.; Wilensky, E.M.; Borst, J.; Pino, W.; Hart, M.; Lobreglio, J.; Zaleski, D.; Leonor, I.; Kung, D.; et al. Implementation of an Early Mobility Pathway in Neurointensive Care Unit Patients with External Ventricular Devices. J. Neurosci. Nurs. 2017, 49, 102–107. [Google Scholar] [CrossRef]


{kind=link}
| CVR * | |
| Round 1 | Round 2 | |
| ||
| 0.77 | NA |
| 0.55 | NA |
| 1.00 | NA |
| 0.55 | NA |
| 1.00 | NA |
| 1.00 | NA |
| 1.00 | NA |
| 1.00 | NA |
| ||
| 0.55 | 1.00 |
| 0.11 | 0.75 |
| 0.55 | 0.50 |
| 0.11 | 0.75 |
| 0.33 | 1.00 |
| 0.55 | 1.00 |
| 0.55 | 0.50 |
| 0.33 | 1.00 |
| 0.33 | 0.75 |
| 0.11 | 0.75 |
| 1.00 | 1.00 |
| 1.00 | 1.00 |
| 0.25 | 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vieira, T.W.; Sakamoto, V.T.M.; Araujo, B.R.; Pai, D.D.; Blatt, C.R.; Caregnato, R.C.A. External Ventricular Drains: Development and Evaluation of a Nursing Clinical Practice Guideline. Nurs. Rep. 2022, 12, 933-944. https://doi.org/10.3390/nursrep12040090
Vieira TW, Sakamoto VTM, Araujo BR, Pai DD, Blatt CR, Caregnato RCA. External Ventricular Drains: Development and Evaluation of a Nursing Clinical Practice Guideline. Nursing Reports. 2022; 12(4):933-944. https://doi.org/10.3390/nursrep12040090
Chicago/Turabian StyleVieira, Tainara Wink, Victória Tiyoko Moraes Sakamoto, Bárbara Rodrigues Araujo, Daiane Dal Pai, Carine Raquel Blatt, and Rita Catalina Aquino Caregnato. 2022. "External Ventricular Drains: Development and Evaluation of a Nursing Clinical Practice Guideline" Nursing Reports 12, no. 4: 933-944. https://doi.org/10.3390/nursrep12040090