

Development and Psychometric Evaluation of a Japanese Version of Newly Graduated Nurses’ Difficulties with End-of-Life Care for Cancer Patients (NDEC Scale)


Abstract
:1. Introduction
2. Materials and Methods
2.1. Phase 1: Selecting Items
2.2. Phase 2: Examining the Content Validity of the Items of the NDEC Scale and Refining Expressions
2.3. Phase 3: Testing Reliability and Validity
2.3.1. Participants and Procedure
2.3.2. Survey Items
2.3.3. Data Analysis
2.3.4. Ethical Approval
3. Results
3.1. Responses
3.2. The NDEC Scale’s Reliability and Validity
3.2.1. Reliability of the NDEC Scale
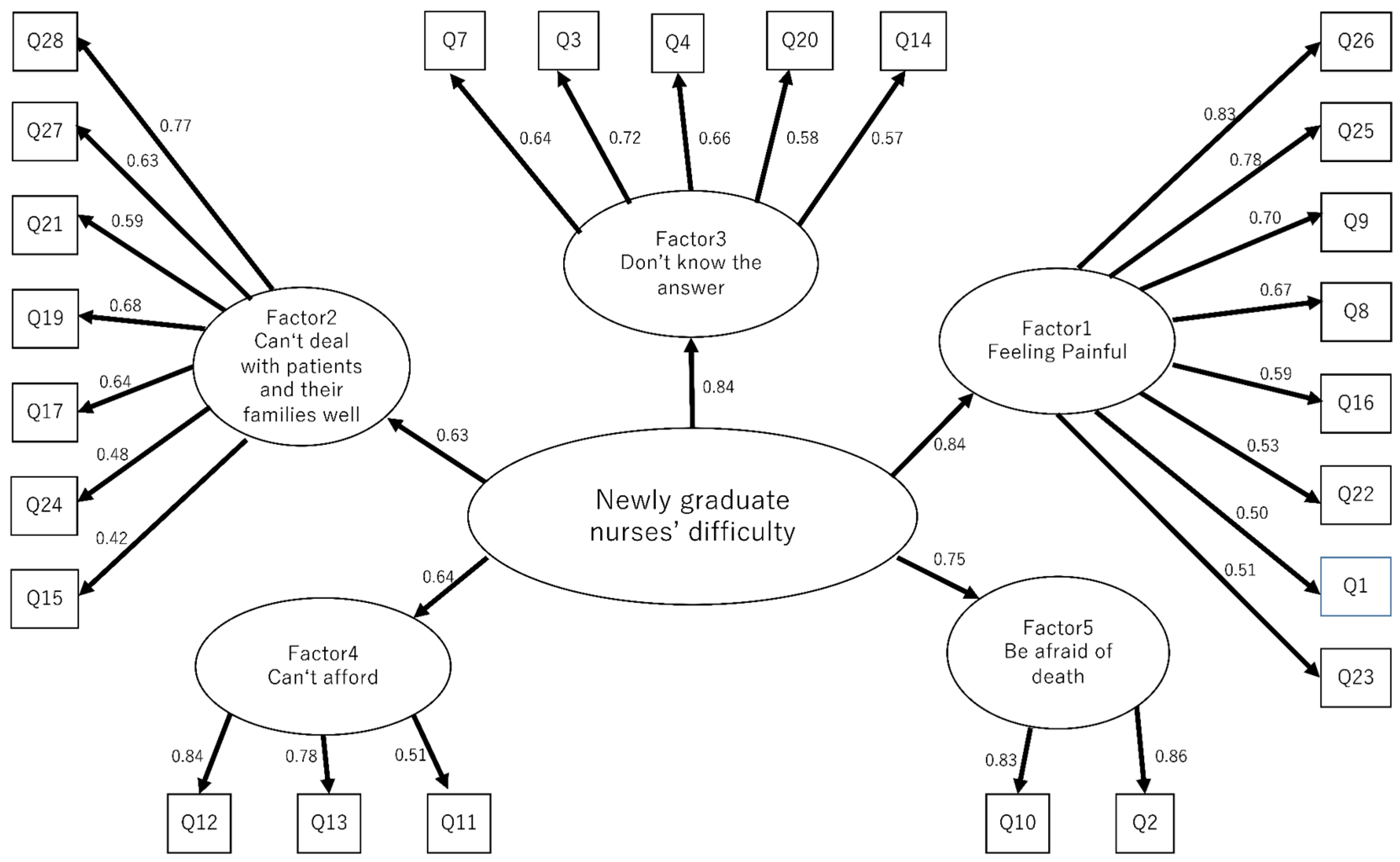
3.2.2. Validity of the NDEC Scale
4. Discussion
4.1. The Difficulties of NGNs in EoL Care
4.2. Reliability and Validity of the NDEC Scale
4.3. Availability of the NDEC Scale
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pereira, S.M.; Fonseca, A.M.; Carvalho, A.S. Burnout in palliative care: A systematic review. Nurs. Ethics 2011, 18, 317–326. [Google Scholar] [CrossRef] [PubMed]
- Sasahara, T.; Miyashita, M.; Kawa, M.; Kazuma, K. Difficulties encountered by nurses in the care of terminally ill cancer patients in general hospitals in Japan. Palliat. Med. 2003, 17, 520–526. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.Y.S.; Li, W.H.C.; Ho, L.L.K.; Ho, L.L.K.; Cheung, A.T.; Chung, J.O.K. Newly graduate nurse perception and experience of clinical handover. Nurs. Educ. Today 2021, 97, 104693. [Google Scholar] [CrossRef] [PubMed]
- Han, K.; Kim, Y.H.; Lee, H.Y. Novice nurse’s sleep disturbance trajectories within the first 2years of work and actual turnover: A prospective longitudinal study. Int. J. Nurs. Stud. 2020, 112, 103575. [Google Scholar] [CrossRef]
- Epstein, M.; Soderstrom, M.; Jirwe, M.; Tucker, P.; Dahlgren, A. Sleep and fatigue in newly graduated nurses-Experiences and strategies for handing shiftwork. J. Clin. Nurs. 2019, 29, 184–194. [Google Scholar] [CrossRef]
- Della Ratta, C. Challenging graduate nurses’ transition: Care of the deteriorating patient. J. Clin. Nurs. 2016, 25, 3036–3048. [Google Scholar] [CrossRef]
- Zheng, R.S.; Lee, S.F.; Bloomer, M.J. How new graduate nurses experience patient death: A systematic review and qualitative meta-synthesis. Int. J. Nurs. Stud. 2016, 53, 320–330. [Google Scholar] [CrossRef]
- Croxon, L.; Deravin, L.; Anderson, J. Dealing with end-of-life New graduated nurse experiences. J. Clin. Nurs. 2018, 27, 337–344. [Google Scholar] [CrossRef]
- Hopkinson, J.B.; Hallett, C.E.; Luker, K.A. Caring for dying people in hospital. J. Adv. Nurs. 2003, 44, 525–533. [Google Scholar] [CrossRef]
- Higashiguchi, T.; Ikegaki, J.; Sobue, K.; Tamura, Y.; Nakajima, N.; Futamura, A.; Miyashita, M.; Mori, N.; Inui, A.; Ohata, K.; et al. Guidelines for parenteral fluid management for terminal cancer patients. Jpn. J. Clin. Oncol. 2016, 46, 986–992. [Google Scholar] [CrossRef] [Green Version]
- Ministry of Health, Labor, and Welfare. Statistics and Information Department. Vital Statistics. 2020. Available online: https://www.e-stat.go.jp/en/stat-search/files?page=1&layout=dataist&toukei=00450011&kikan=00450&tstat=000001028897&cycle=7&year=20200&tclass1=000001053058&tclass2=000001053061&tclass3=000001053063&tclass4val=0 (accessed on 15 March 2022).
- Margaret, M.; Beth, M.; Joan, M. The palliative care quiz for nursing: The development of an instrument to measure nurses’ knowledge of palliative care. J. Adv. Nurs. 1996, 23, 126–137. [Google Scholar] [CrossRef]
- Kanno, Y.; Sato, K.; Shimizu, M.; Funamizu, Y.; Andoh, H.; Kishino, M.; Senaga, T.; Takahashi, T.; Miyashita, M. Development and Validity of the Nursing Care Scale and Nurse’s Difficulty Scale in Caring for Dying Patients with Cancer and their Families in General Hospitals in Japan. J. Hosp. Palliat. Nurs. 2019, 21, 174–182. [Google Scholar] [CrossRef] [PubMed]
- Asano, A.; Sakai, S.; Kikunaga, J.; Seki, N.; Koyama, Y. Development and Assessment of the content validity of a scale to measure newly graduated nurses’ difficulty with end-of-life care for cancer patients (NDEC scale). J. Health Sci. Niigata Univ. 2022, 19, 13–20. [Google Scholar]
- Prebble, K.S.; Gerbild, H.; Abrahamsen, C. Content validity and reliability of the Danish version of health care students’ attitudes towards addressing sexual health: A psychometric study. Scand. J. Caring Sci. 2022, 36, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Ushiro, R. Nurse-Physician Collaboration Scale: Development and psychometric testing. J. Adv. Nurs. 2009, 65, 1497–1508. [Google Scholar] [CrossRef]
- Japan Hospital Association. Members List 2020. Available online: http://www.hospital.or.jp/e/ (accessed on 15 March 2022).
- Benner, P. From novice to expert. Am. J. Nurs. 1982, 82, 402–407. [Google Scholar]
- Questant Powered by Macromill. Available online: https://questant.jp/en/ (accessed on 10 March 2022).
- COnsensus-Based Standards for the Selection of Health Measurement Instrument. COSMIN Methodology for Systematic Reviews of Patient-Reported Outcome Measures (PROMs) User Manual. 2018. Available online: https://cosmin.nl/wp-content/uploads/COSMIN-syst-review-for-PROMs-manual_version-1_feb-2018.pdf (accessed on 10 March 2022).
- Rolt, L.; Gillett, K. Employing newly qualified nurses to work in hospices: A qualitative interview study. J. Adv. Nurs. 2020, 76, 1717–1727. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Theisen, J.L.; Sandau, K.E. Competency of New Graduate Nurses: A Review of Their Weaknesses and Strategies for Success. J. Contin. Educ. Nurs. 2013, 44, 406–415. [Google Scholar] [CrossRef]
- Mazanec, P.; Ferrell, B.; Virani, R.; Alayu, F.; Ruel, N.H. Preparing New Graduate RNs to Provide Primary Palliative Care. J. Contin. Educ. Nurs. 2020, 51, 280–286. [Google Scholar] [CrossRef]
- Liang, Z.; Di Nella, J.; Ren, D.X.; Tuite, P.K.; Usher, B.M. Evaluation of a Peer Nurse Coach Quality Improvement Project on New Nurse Hire Attitudes Toward Care for the Dying. J. Hosp. Palliat. Nurs. 2016, 18, 398–404. [Google Scholar] [CrossRef]
- Kim, J.H.; Shin, H.S. Exploring barriers and facilitators for successful transition in new graduate nurses: A mixed methods study. J. Prof. Nurs. 2020, 36, 560–568. [Google Scholar] [CrossRef] [PubMed]
- Tantan, S.; Unver, V.; Hatipoglu, S. An analysis of the factors affecting the transition period to professional roles for newly graduated nurses in Turkey. Int. Nurs. Rev. 2013, 60, 405–412. [Google Scholar] [CrossRef]
- Delaney, C. Walking a fine line: Graduate nurses’ transition experiences during orientation. J. Nurs. Educ. 2003, 42, 437–443. [Google Scholar] [CrossRef] [PubMed]
- American Organization for Nursing Leadership. Guiding Principles. The Newly Licensed Nurse’s Transition into Practice. Available online: https://www.aonl.org/system/files/media/file/2020/12/newly-licensed-nurses-transition-practice.pdf (accessed on 8 July 2022).
- Department of Health Republic of South Africa. Strategic Plan for Nurse Education, Training and Practice 2012/13–2016/17. Available online: https://health-e.org.za/2013/10/06/strategic-plan-nurse-education-training-practice/ (accessed on 8 July 2022).
- Rudman, A.; Gustavsson, J.P. Early-career burnout among new graduate nurses: A prospective observational study of in-tra-individual change trajectories. Int. J. Nurs. Stud. 2011, 48, 292–302. [Google Scholar] [CrossRef]


{kind=link}
| NGNs = 171, GNs = 194 | |||
|---|---|---|---|
| NGNs’ n (%) or Mean ± SD | GNs’ n (%) or Mean ± SD | ||
| Male | 5 (3) | 21 (11) | |
| Female | 166 (97) | 173 (89) | |
| Age (Years) | 23.00 ± 2.32 | 34.08 ± 8.30 | |
| NRS | 7.22 ± 1.46 | 6.54 ± 2.01 | |
| CN or CNS license | None | 41 (21) | |
| Advisors (multiple selection) | 171 (100) | 194 (100) | |
| Individual educator (ex preceptor) | 144 | Same department nurse | 178 |
| Senior nurses other than individual educator | 143 | Same hospital CN or CNS | 112 |
| New graduate nurse in the same hospital | 93 | ||
| Head nurse | 45 | Head nurse | 113 |
| Nursing school classmate | 53 | Nursing school classmate | 27 |
| Family | 37 | Family | 25 |
| No advisor | 0 | No advisor | 0 |
| Others | 0 | Others | 11 |
| Doctor | 5 | ||
| Another hospital CN | 4 | ||
| Another hospital CNS | 1 | ||
| Pharmacist | 1 | ||
| Standard Regression Coefficients | |||||
|---|---|---|---|---|---|
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | |
| Factor1: Feeling Painful α = 0.83 mean ± SD = 4.57 ± 0.98 | |||||
| Q26 I was sad about the care just before the patient died | 0.84 | 0.34 | 0.46 | 0.34 | 0.42 |
| Q25 I felt empty in the care just before the patient died | 0.81 | 0.38 | 0.48 | 0.41 | 0.31 |
| Q9 I couldn’t accept that the patient died | 0.69 | 0.22 | 0.43 | 0.37 | 0.41 |
| Q8 Conflict with having to prepare for bereavement while the patient is still alive | 0.67 | 0.22 | 0.40 | 0.26 | 0.35 |
| Q16 After experiencing patients’ death several times, I felt painful and couldn’t see the surroundings | 0.58 | 0.24 | 0.23 | 0.32 | 0.50 |
| Q22 I thought I shouldn’t ask the patient about death | 0.51 | 0.37 | 0.20 | 0.41 | 0.38 |
| Q1 I’m confused as to whether it’s good or bad to cry when a patient dies | 0.49 | 0.08 | 0.41 | 0.25 | 0.40 |
| Q23 I hesitated to talk to the patient about the last moment, thinking that it would be depressing | 0.48 | 0.41 | 0.28 | 0.43 | 0.28 |
| Factor2: Can’t deal with patients and their families well α = 0.78 mean ± SD = 5.30 ± 0.81 | |||||
| Q28 I felt that I was an inconvenience to the patient due to my lack of knowledge and skills | 0.32 | 0.81 | 0.36 | 0.42 | 0.03 |
| Q27 I was just doing what my seniors told me, and I couldn’t predict the medical condition | 0.22 | 0.67 | 0.12 | 0.32 | 0.22 |
| Q21 I couldn’t afford to grasp the patient’s condition because I was busy with work | 0.15 | 0.64 | 0.15 | 0.26 | 0.03 |
| Q19 I regret not being able to support the patient | 0.50 | 0.63 | 0.59 | 0.54 | 0.15 |
| Q17 feel that my ability to assess patients is weak | 0.23 | 0.63 | 0.35 | 0.52 | 0.26 |
| Q24 I was having trouble dealing with a family member who did not express emotions | 0.35 | 0.47 | 0.27 | 0.35 | 0.15 |
| Q15 Difficult to communicate with the family of patients with reduced consciousness | 0.33 | 0.40 | 0.30 | 0.34 | 0.18 |
| Factor3: Don’t know the answer α = 0.75 mean ± SD = 5.65 ± 0.83 | |||||
| Q7 I want to learn to become a nurse who meets the needs of patients and their families | 0.33 | 0.25 | 0.73 | 0.31 | 0.25 |
| Q3 No matter how many times I experience final hours care, I feel uncomfortable | 0.58 | 0.21 | 0.67 | 0.27 | 0.46 |
| Q4 Final hours care is always an unanswered question | 0.39 | 0.23 | 0.66 | 0.21 | 0.27 |
| Q20 I was wondering if this was all right for the care of the patient just before patient died | 0.46 | 0.57 | 0.61 | 0.44 | 0.11 |
| Q14 Difficult to deal with patients who cannot make decisions | 0.43 | 0.44 | 0.47 | 0.43 | 0.25 |
| Factor4: Can’t afford α = 0.72 mean ± SD = 5.31 ± 0.98 | |||||
| Q12 When the patient asked me about my condition, I was very upset | 0.37 | 0.47 | 0.35 | 0.98 | 0.22 |
| Q13 I was worried when the patient asked me about the prognosis | 0.46 | 0.46 | 0.30 | 0.71 | 0.30 |
| Q11 The patient suddenly changed and I was upset | 0.34 | 0.46 | 0.30 | 0.51 | 0.33 |
| Factor5:Being afraid of death α = 0.82 mean ± SD = 5.01 ± 1.38 | |||||
| Q10 There is a vague fear of death | 0.55 | 0.24 | 0.43 | 0.34 | 0.85 |
| Q2 Somewhere there is a fear of facing death | 0.56 | 0.28 | 0.45 | 0.35 | 0.76 |
| Cumulative Contribution ratio: 50%. Cronbach’s α of the entire scale: α = 0.9. | |||||
| α: Cronbach’s coefficient alpha. SD: standard deviation | |||||
| Highlighted areas indicate standard regression coefficients of 0.4 or higher. | |||||
| Factor 1 | Factor 2 | Factor 3 | Factor 4 | Factor 5 | Total | |
|---|---|---|---|---|---|---|
| NRS | 0.34 ** | 0.30 ** | 0.39 ** | 0.25 ** | 0.40 ** | 0.43 ** |
| NGNs (n = 171) | GNs (n = 194) | ||||
|---|---|---|---|---|---|
| Mean | SD | Mean | SD | p-Value | |
| Total | 142.81 | 19.42 | 118.05 | 27.91 | <0.01 * |
| Factor 1 | 4.56 | 1.01 | 3.71 | 1.08 | <0.01 * |
| Factor 2 | 5.30 | 0.82 | 4.18 | 1.07 | <0.01 * |
| Factor 3 | 5.66 | 0.84 | 5.45 | 0.90 | 0.03 * |
| Factor 4 | 5.30 | 1.03 | 4.16 | 1.37 | <0.01 * |
| Factor 5 | 5.01 | 1.41 | 3.50 | 1.47 | <0.01 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Asano, A.; Sakai, S.; Seki, N.; Koyama, Y. Development and Psychometric Evaluation of a Japanese Version of Newly Graduated Nurses’ Difficulties with End-of-Life Care for Cancer Patients (NDEC Scale). Nurs. Rep. 2022, 12, 637-647. https://doi.org/10.3390/nursrep12030063
Asano A, Sakai S, Seki N, Koyama Y. Development and Psychometric Evaluation of a Japanese Version of Newly Graduated Nurses’ Difficulties with End-of-Life Care for Cancer Patients (NDEC Scale). Nursing Reports. 2022; 12(3):637-647. https://doi.org/10.3390/nursrep12030063
Chicago/Turabian StyleAsano, Akitoshi, Sayuri Sakai, Nao Seki, and Yu Koyama. 2022. "Development and Psychometric Evaluation of a Japanese Version of Newly Graduated Nurses’ Difficulties with End-of-Life Care for Cancer Patients (NDEC Scale)" Nursing Reports 12, no. 3: 637-647. https://doi.org/10.3390/nursrep12030063