
Cochlear Implantation in Children Affected by Single-Sided Deafness: A Comprehensive Review

Abstract
:1. Introduction
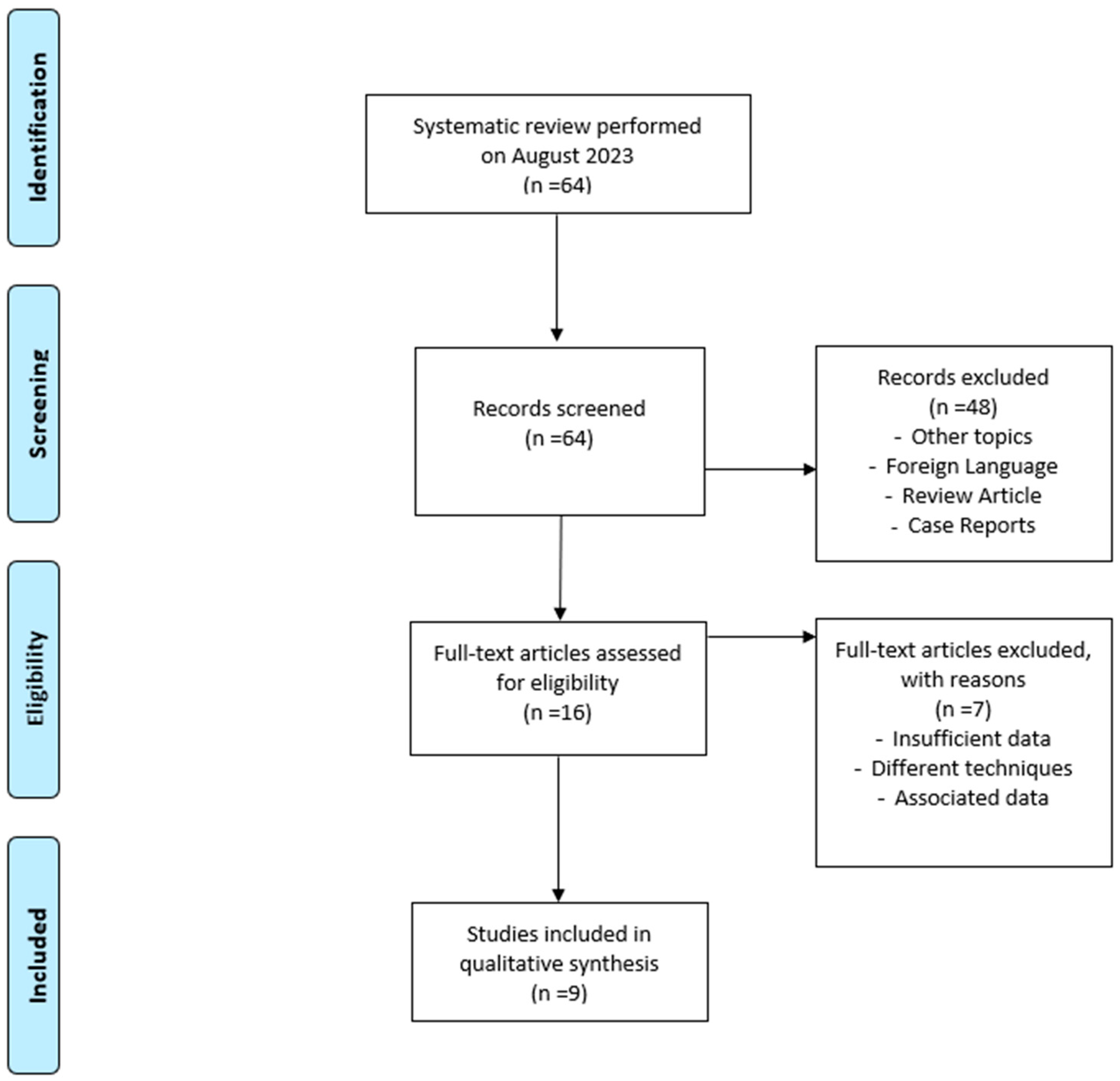
2. Materials and Methods
- Original studies on cohorts > 10 patients (in order to identify studies with an adequate sample size [6]);
- Studies on young subjects, defined as those aged 18 years and under (https://www.who.int/health-topics/ageing#tab=tab_1, accessed on 30 November 2023);
- Studies including patients affected by SSD according to the definition of SSD by the American Audiology Academy.
- Studies containing duplicated data from other published work;
- Cohort of patients < 10;
- Studies published in a non-English language;
- Studies not including audio-vestibular diagnoses;
- Studies analyzing only specific subgroups of diagnoses;
- Reviews, letters, and case reports.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kay-Rivest, E.; Irace, A.L.; Golub, J.S.; Svirsky, M.A. Prevalence of Single-Sided Deafness in the United States. Laryngoscope 2022, 132, 1652–1656. [Google Scholar] [CrossRef]
- Lieu, J.E. Permanent unilateral hearing loss (UHL) and childhood development. Curr. Otorhinolaryngol. Rep. 2018, 6, 74–81. [Google Scholar] [CrossRef]
- Caruso, A.; Giannuzzi, A.L.; Sozzi, V.; Sanna, M. Bone anchored hearing implants without skin thinning: The Gruppo Otologico surgical and audiological experience. Eur. Arch. Otorhinolaryngol. 2017, 274, 695–700. [Google Scholar] [CrossRef]
- Lieu, J.E. Speech-language and educational consequences of unilateral hearing loss in children. Arch. Otolaryngol. Head Neck Surg. 2004, 130, 524–530. [Google Scholar] [CrossRef]
- Fischer, C.; Lieu, J. Unilateral hearing loss is associated with a negative effect on language scores in adolescents. Int. J. Pediatr. Otorhinolaryngol. 2014, 78, 1611–1617. [Google Scholar] [CrossRef]
- Hansen, M.R.; Gantz, B.J.; Dunn, C. Outcomes after cochlear implantation for patients with single-sided deafness, including those with recalcitrant Meniere’s disease. Otol. Neurotol. 2013, 34, 1681–1687. [Google Scholar] [CrossRef]
- Buss, E.; Dillon, M.T.; Rooth, M.A.; King, E.R.; Deres, E.J.; Buchman, C.A.; Pillsbury, H.C.; Brown, K.D. Effects of cochlear implantation on binaural hearing in adults with unilateral hearing loss. Trends Hear. 2018, 22, 2331216518771173. [Google Scholar] [CrossRef]
- Peters, J.P.M.; Smit, A.L.; Stegeman, I.; Grolman, W. Review: Bone conduction devices and contralateral routing of sound systems in single-sided deafness. Laryngoscope 2015, 125, 218–226. [Google Scholar] [CrossRef]
- Mertens, G.; De Bodt, M.; Van de Heyning, P. Evaluation of Long-Term Cochlear Implant Use in Subjects with Acquired Unilateral Profound Hearing Loss: Focus on Binaural Auditory Outcomes. Ear Hear. 2017, 38, 117–125. [Google Scholar] [CrossRef]
- Arndt, S.; Aschendorff, A.; Laszig, R.; Beck, R.; Schild, C.; Kroeger, S.; Ihorst, G.; Wesarg, T. Comparison of pseudobinaural hearing to real binaural hearing rehabilitation after cochlear implantation in patients with unilateral deafness and tinnitus. Otol. Neurotol. 2011, 32, 39–47. [Google Scholar] [CrossRef]
- Thomas, J.P.; Neumann, K.; Dazert, S.; Voelter, C. Cochlear Implantation in Children with Congenital Single-Sided Deafness. Otol. Neurotol. 2017, 38, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Ramos Macías, Á.; Borkoski-Barreiro, S.A.; Falcón González, J.C.; de Miguel Martínez, I.; Ramos de Miguel, Á. Single-sided deafness and cochlear implantation in congenital and acquired hearing loss in children. Clin. Otolaryngol. 2019, 44, 138–143. [Google Scholar] [CrossRef]
- Cushing, S.L.; Gordon, K.A.; Sokolov, M.; Papaioannou, V.; Polonenko, M.; Papsin, B.C. Etiology and therapy indication for cochlear implantation in children with single-sided deafness: Retrospective analysis. HNO 2019, 67, 750–759. [Google Scholar] [CrossRef]
- Ganek, H.V.; Cushing, S.L.; Papsin, B.C.; Gordon, K.A. Cochlear Implant Use Remains Consistent Over Time in Children with Single-Sided Deafness. Ear Hear. 2020, 41, 678–685. [Google Scholar] [CrossRef] [PubMed]
- Rauch, A.K.; Arndt, S.; Aschendorff, A.; Beck, R.; Speck, I.; Ketterer, M.C.; Jakob, T.F.; Hassepass, F. Long-term results of cochlear implantation in children with congenital single-sided deafness. Eur. Arch. Otorhinolaryngol. 2021, 278, 3245–3255. [Google Scholar] [CrossRef]
- Brown, K.D.; Dillon, M.T.; Park, L.R. Benefits of Cochlear Implantation in Childhood Unilateral Hearing Loss (CUHL Trial). Laryngoscope 2022, 132 (Suppl. S6), S1–S18. [Google Scholar] [CrossRef]
- Gordon, K.A.; Alemu, R.; Papsin, B.C.; Negandhi, J.; Cushing, S.L. Effects of Age at Implantation on Outcomes of Cochlear Implantation in Children with Short Durations of Single-Sided Deafness. Otol. Neurotol. 2023, 44, 233–240. [Google Scholar] [CrossRef]
- Yaar-Soffer, Y.; Kaplan-Neeman, R.; Greenbom, T.; Habiballah, S.; Shapira, Y.; Henkin, Y. A cortical biomarker of audibility and processing efficacy in children with single-sided deafness using a cochlear implant. Sci. Rep. 2023, 13, 3533. [Google Scholar] [CrossRef]
- Park, L.R.; Gagnon, E.B.; Dillon, M.T. Factors that influence outcomes and device use for pediatric cochlear implant recipients with unilateral hearing loss. Front. Hum. Neurosci. 2023, 17, 1141065. [Google Scholar] [CrossRef]
- Gatehouse, S.; Noble, W. The speech, spatial and qualities of hearing scale (SSQ). Int. J. Audiol. 2004, 43, 85–99. [Google Scholar] [CrossRef]
- Cox, R.M.; Alexander, G.C. The International Outcome Inventory for Hearing Aids (IOI-HA): Psychometric properties of the English version. Int. J. Audiol. 2002, 41, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Arras, T.; Boudewyns, A.; Swinnen, F.; Zarowski, A.; Philips, B.; Desloovere, C.; Wouters, J.; van Wieringen, A. Longitudinal auditory data of children with prelingual single-sided deafness managed with early cochlear implantation. Sci. Rep. 2022, 12, 9376. [Google Scholar] [CrossRef]
- Benchetrit, L.; Ronner, E.A.; Anne, S.; Cohen, M.S. Cochlear Implantation in Children with Single-Sided Deafness: A Systematic Review and Meta-analysis. JAMA Otolaryngol. Head Neck Surg. 2021, 147, 58–69. [Google Scholar] [CrossRef] [PubMed]
- Vashishth, A.; Fulcheri, A.; Prasad, S.C.; Dandinarasaiah, M.; Caruso, A.; Sanna, M. Cochlear Implantation in Chronic Otitis Media with Cholesteatoma and Open Cavities: Long-term Surgical Outcomes. Otol. Neurotol. 2018, 39, 45–53. [Google Scholar] [CrossRef]
- Kinney, H.C.; Brody, B.A.; Kloman, A.S.; Gilles, F.H. Sequence of central nervous system myelination in human infancy. II. Patterns of myelination in autopsied infants. J. Neuropathol. Exp. Neurol. 1988, 47, 217–234. [Google Scholar] [CrossRef] [PubMed]
- Arndt, S.; Prosse, S.; Laszig, R.; Wesarg, T.; Aschendorff, A.; Hassepass, F. Cochlear implantation in children with single-sided deafness: Does aetiology and duration of deafness matter? Audiol. Neurootol. 2015, 20 (Suppl. S1), 21–30. [Google Scholar] [CrossRef]
- Rahne, T.; Plontke, S.K. Functional Result After Cochlear Implantation in Children and Adults with Single-sided Deafness. Otol. Neurotol. 2016, 37, e332–e340. [Google Scholar] [CrossRef]
- Sullivan, C.B.; Al-Qurayshi, Z.; Zhu, V.; Liu, A.; Dunn, C.; Gantz, B.J.; Hansen, M.R. Long-term audiologic outcomes after cochlear implantation for single-sided deafness. Laryngoscope 2020, 130, 1805–1811. [Google Scholar] [CrossRef]
- Probst, R. Kochleaimplantation bei einseitiger Taubheit? Cochlear implantation for unilateral deafness? HNO 2008, 56, 886–888. (In German) [Google Scholar] [CrossRef]
- Sharma, A.; Glick, H.; Campbell, J.; Torres, J.; Dorman, M.; Zeitler, D.M. Cortical Plasticity and Reorganization in Pediatric Single-sided Deafness Pre- and Postcochlear Implantation: A Case Study. Otol. Neurotol. 2016, 37, e26–e34. [Google Scholar] [CrossRef]
- Deep, N.L.; Gordon, S.A.; Shapiro, W.H.; Waltzman, S.B.; Roland, J.T., Jr.; Friedmann, D.R. Cochlear Implantation in Children with Single-Sided Deafness. Laryngoscope 2021, 131, E271–E277. [Google Scholar] [CrossRef] [PubMed]
- Holt, R.F.; Beer, J.; Kronenberger, W.G.; Pisoni, D.B.; Lalonde, K. Contribution of family environment to pediatric cochlear implant users’ speech and language outcomes: Some preliminary findings. J. Speech Lang Hear Res. 2012, 55, 848–864. [Google Scholar] [CrossRef] [PubMed]
- Watson, V.; Verschuur, C.; Lathlean, J. Exploring the experiences of teenagers with cochlear implants. Cochlear Implants Int. 2016, 17, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Ward, K.M.; Coughran, A.J.; Lee, M.; Fitzgerald, M.B.; Cheng, A.G.; Chang, K.W.; Ahmad, I.N. Prevalence of Cochlear Nerve Deficiency and Hearing Device Use in Children with Single-Sided Deafness. Otolaryngol. Head Neck Surg. 2023, 169, 390–396. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Authors | Ref. | Year | Country | # | Sex | Age | Study |
|---|---|---|---|---|---|---|---|
| Thomas et al. | [11] | 2017 | Germany | 21 | M: 8, F: 13 | 9 m.–11 y. | R |
| Ramos Marcias et al. | [12] | 2018 | Spain | 23 | M: 11, F: 12 | 11 m.–11 y. | O |
| Cushing et al. | [13] | 2019 | Canada | 37 | - | - | R |
| Ganek et al. | [14] | 2019 | Canada | 23 | M: 13, F: 10 | 1–15 y. | R |
| Rauch et al. | [15] | 2020 | Germany | 11 | - | 1–13 y. | R |
| Brown et al. | [16] | 2022 | USA | 20 | M: 12, F: 8 | 3–12 y. | P |
| Gordon et al. | [17] | 2023 | Canada | 57 | - | 1–15 y. | P |
| Yaar-Soffer et al. | [18] | 2023 | Israel | 22 | M: 16, F: 6 | 1–8 y. | R |
| Park et al. | [19] | 2023 | USA | 97 | M: 47, F: 50 | 6 m.–17 y. | P |
| Summary | - | 2017–2023 | - | 311 | F:M = 1:1.1 | 6 m.–17 y. | - |
| Authors | Pre-Verbal | Post Verbal | PTA Normal Ear | PTA Deaf Ear | Deprivation (Range) | Use of Hearing Aid Pre-CI (#) |
|---|---|---|---|---|---|---|
| Thomas et al. [11] | 21 | 0 | - | - | 6 y | - |
| Ramos Marcias et al. [12] | 4 | 19 | - | - | 1 y 3 m | - |
| Cushing et al. [13] | - | - | 20 | 100 | <4 y | - |
| Ganek et al. [14] | 13 | 10 | <25 | >90 | 2 y | - |
| Rauch et al. [15] | 9 | 2 | <20 | >90 | From 1 y to 13 y | - |
| Brown et al. [16] | 11 | 9 | 10 | 108 | 3 y 3 m | 6 |
| Gordon et al. [17] | 40 | 17 | <25 | - | 1 y 9 m | - |
| Yaar-Soffer et al. [18] | 20 | 2 | <20 | >80 | - | - |
| Park et al. [19] | 53 | 44 | - | - | From 2 m to 14 y | - |
| Summary | 171 | 103 | <25 | >80 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santopietro, G.; Fancello, V.; Fancello, G.; Bianchini, C.; Pelucchi, S.; Ciorba, A. Cochlear Implantation in Children Affected by Single-Sided Deafness: A Comprehensive Review. Audiol. Res. 2024, 14, 77-85. https://doi.org/10.3390/audiolres14010007
Santopietro G, Fancello V, Fancello G, Bianchini C, Pelucchi S, Ciorba A. Cochlear Implantation in Children Affected by Single-Sided Deafness: A Comprehensive Review. Audiology Research. 2024; 14(1):77-85. https://doi.org/10.3390/audiolres14010007
Chicago/Turabian StyleSantopietro, Giuseppe, Virginia Fancello, Giuseppe Fancello, Chiara Bianchini, Stefano Pelucchi, and Andrea Ciorba. 2024. "Cochlear Implantation in Children Affected by Single-Sided Deafness: A Comprehensive Review" Audiology Research 14, no. 1: 77-85. https://doi.org/10.3390/audiolres14010007