
Impaired Vestibulo-Ocular Reflex on Video Head Impulse Test in Superior Canal Dehiscence: “Spontaneous Plugging” or Endolymphatic Flow Dissipation?

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
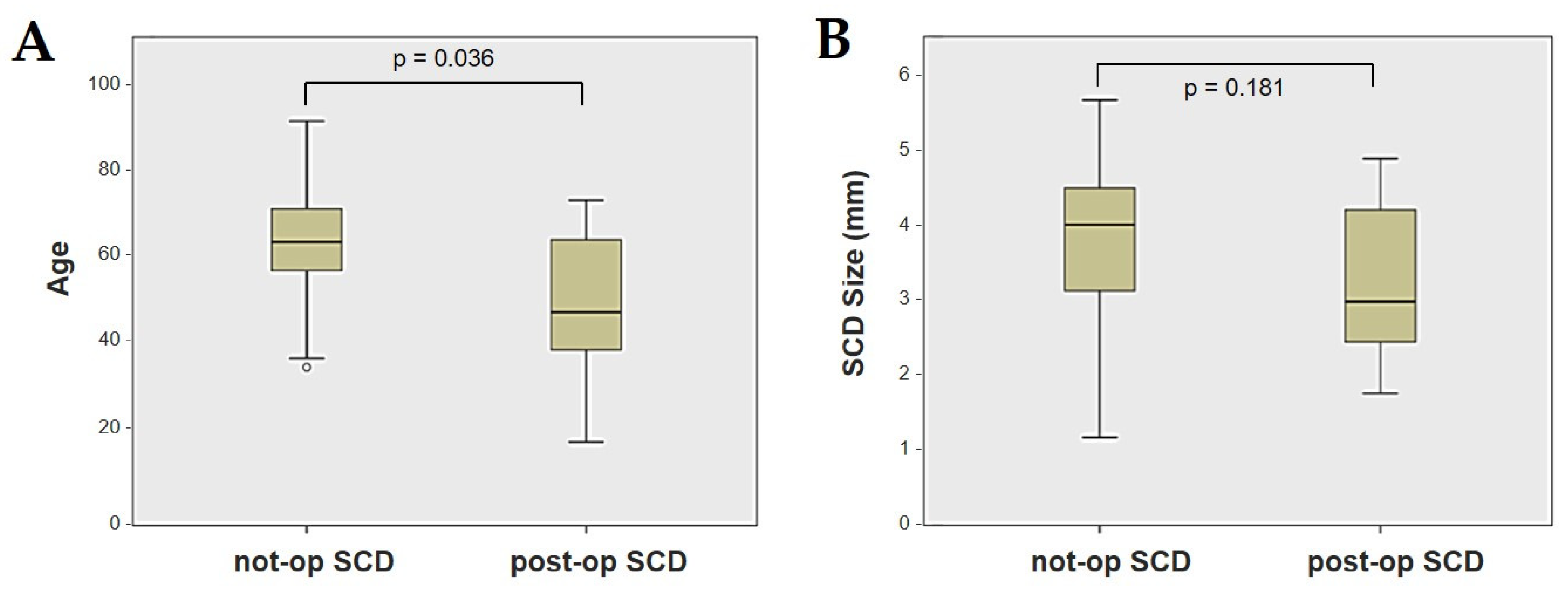
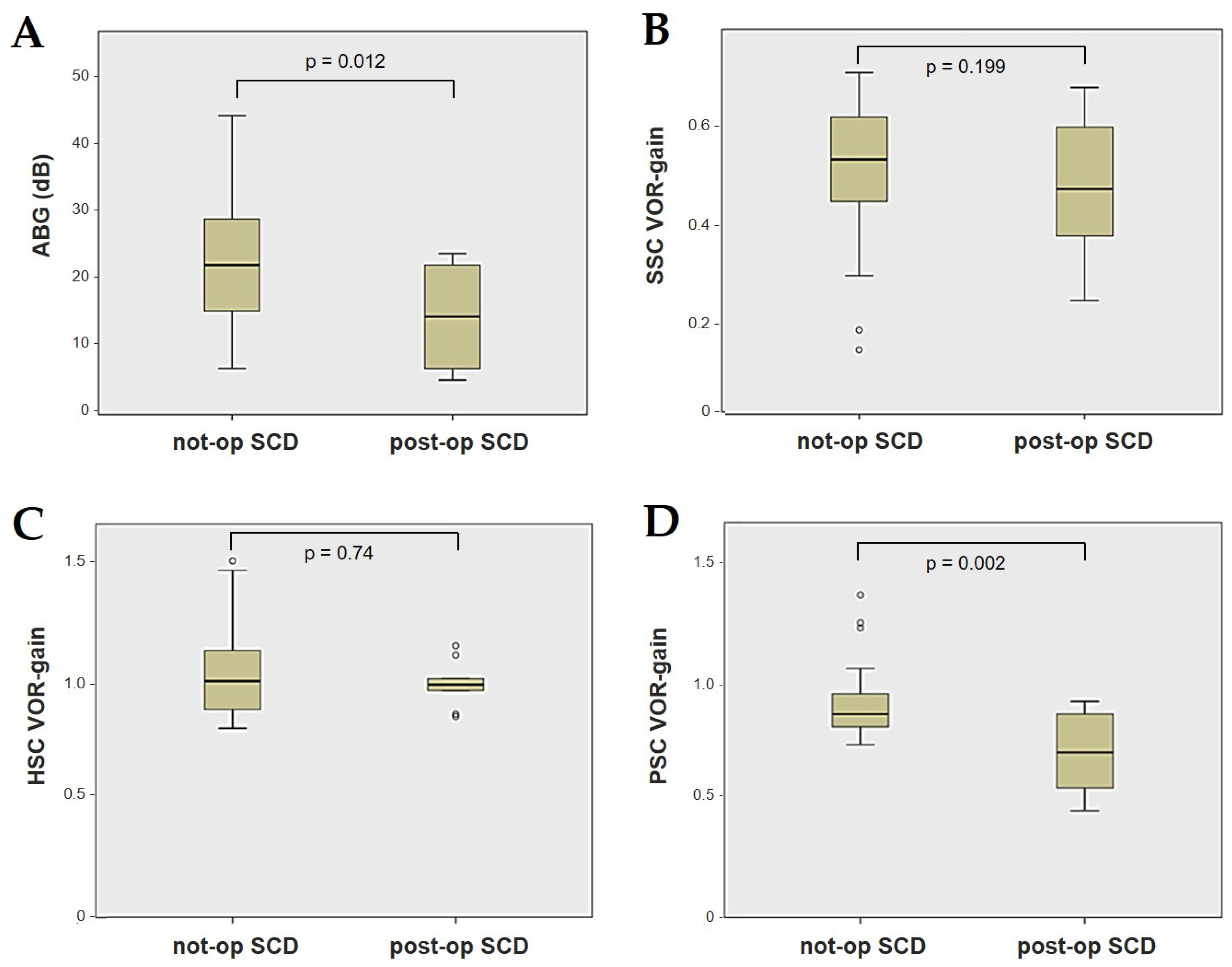
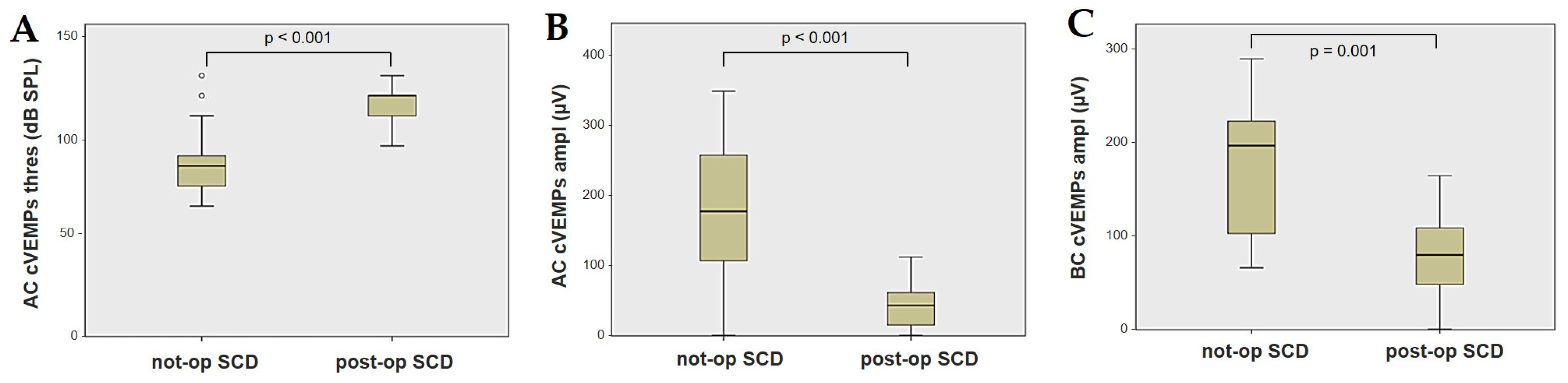
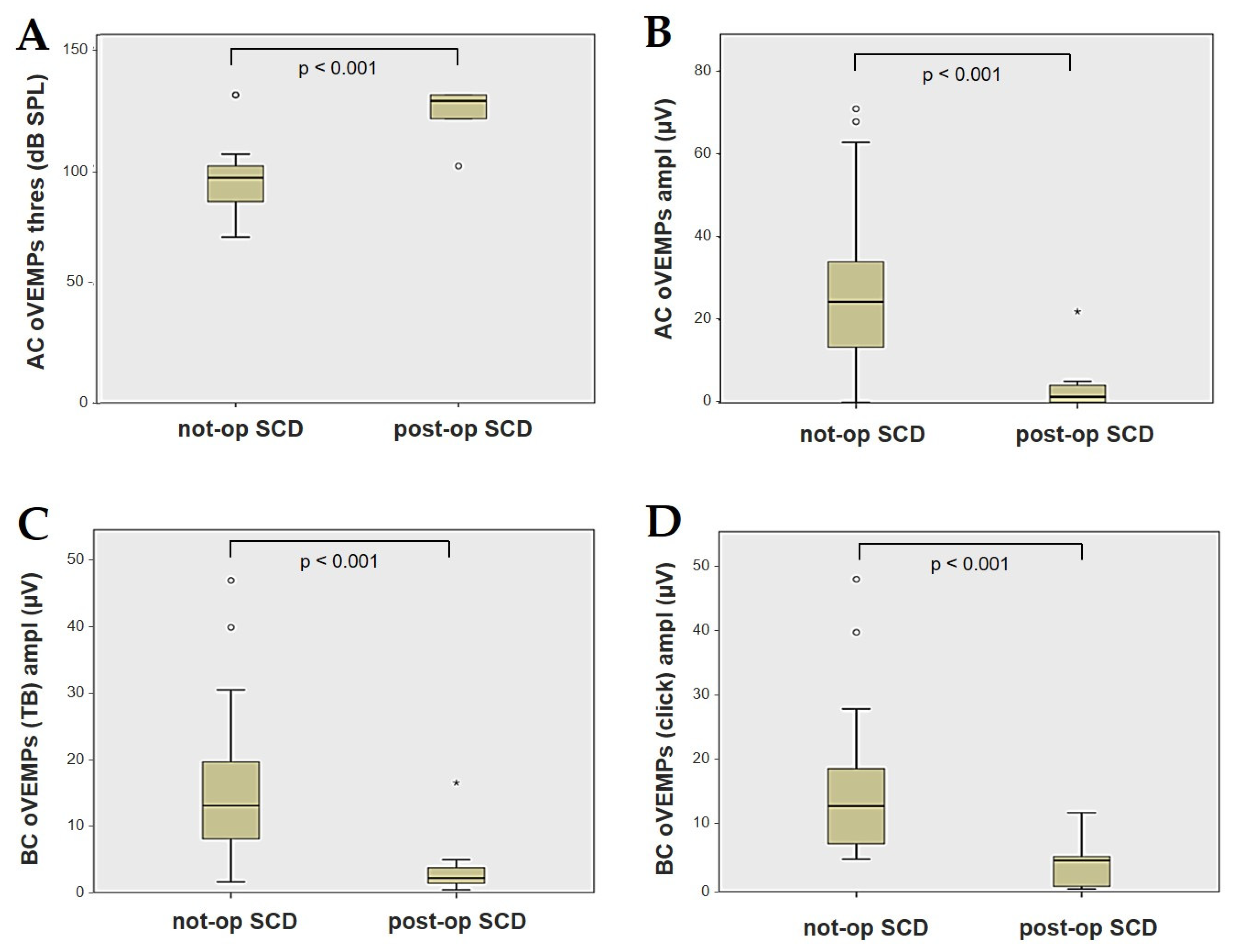
- Ears with SCD exhibiting a VOR gain impairment for the affected SSC were included in the “not-operated SCD” group;
- Ears with SCD that were operated on through a surgical plugging due to disabling symptoms were included in the “post-operative SCD” group. In this case, the instrumental measurements used for the correlation analysis refer to data collected at 6-months after surgery.
2.1. Pure Tone Audiometry and Impedance Audiometry
2.2. VEMPs
2.3. vHIT
2.4. Imaging
2.5. Surgical Plugging
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Minor, L.B.; Solomon, D.; Zinreich, J.S.; Zee, D.S. Sound- and/or pressure-induced vertigo due to bone dehiscence of the superior semicircular canal. Arch. Otolaryngol. Head. Neck Surg. 1998, 124, 249–258. [Google Scholar] [CrossRef]
- Cremer, P.D.; Minor, L.B.; Carey, J.P.; Della Santina, C.C. Eye movements in patients with superior canal dehiscence syndrome align with the abnormal canal. Neurology 2000, 55, 1833–1841. [Google Scholar] [CrossRef] [PubMed]
- Brantberg, K.; Bergenius, J.; Mendel, L.; Witt, H.; Tribukait, A.; Ygge, J. Symptoms, findings and treatment in patients with dehiscence of the superior semicircular canal. Acta Otolaryngol. 2001, 121, 68–75. [Google Scholar] [CrossRef]
- Rosowski, J.J.; Songer, J.E.; Nakajima, H.H.; Brinsko, K.M.; Merchant, S.N. Clinical, experimental, and theoretical investigations of the effect of superior semicircular canal dehiscence on hearing mechanisms. Otol. Neurotol. 2004, 25, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Carey, J.P.; Hirvonen, T.P.; Hullar, T.E.; Minor, L.B. Acoustic responses of vestibular afferents in a model of superior canal dehiscence. Otol. Neurotol. 2004, 25, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Iversen, M.M.; Rabbitt, R.D. Biomechanics of Third Window Syndrome. Front. Neurol. 2020, 11, 891. [Google Scholar] [CrossRef]
- Curthoys, I.S.; Smith, C.M.; Burgess, A.M.; Dlugaiczyk, J. A Review of Neural Data and Modelling to Explain How a Semicircular Canal Dehiscence (SCD) Causes Enhanced VEMPs, Skull Vibration Induced Nystagmus (SVIN), and the Tullio Phenomenon. Audiol. Res. 2023, 13, 418–430. [Google Scholar] [CrossRef]
- Dumas, G.; Curthoys, I.S.; Castellucci, A.; Dumas, L.; Perrin, P.; Schmerber, S. A bone-conducted Tullio phenomenon-A bridge to understand skull vibration induced nystagmus in superior canal dehiscence. Front. Neurol. 2023, 14, 1183040. [Google Scholar] [CrossRef]
- Carey, J.P.; Migliaccio, A.A.; Minor, L.B. Semicircular canal function before and after surgery for superior canal dehiscence. Otol. Neurotol. 2007, 28, 356–364. [Google Scholar] [CrossRef]
- Welgampola, M.S.; Myrie, O.A.; Minor, L.B.; Carey, J.P. Vestibular-evoked myogenic potential thresholds normalize on plugging superior canal dehiscence. Neurology 2008, 70, 464–472. [Google Scholar] [CrossRef]
- Agrawal, S.K.; Parnes, L.S. Transmastoid superior semicircular canal occlusion. Otol. Neurotol. 2008, 29, 363–367. [Google Scholar] [CrossRef] [PubMed]
- Vlastarakos, P.V.; Proikas, K.; Tavoulari, E.; Kikidis, D.; Maragoudakis, P.; Nikolopoulos, T.P. Efficacy assessment and complications of surgical management for superior semicircular canal dehiscence: A meta-analysis of published interventional studies. Eur. Arch. Otorhinolaryngol. 2009, 266, 177–186. [Google Scholar] [CrossRef]
- Fiorino, F.; Barbieri, F.; Pizzini, F.B.; Beltramello, A. A dehiscent superior semicircular canal may be plugged and resurfaced via the transmastoid route. Otol. Neurotol. 2010, 31, 136–139. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.C.; Somers, T.; van Dinther, J.; Vanspauwen, R.; Husseman, J.; Briggs, R. Transmastoid repair of superior semicircular canal dehiscence. J. Neurol. Surg. B Skull Base 2012, 73, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Ward, B.K.; Agrawal, Y.; Nguyen, E.; Della Santina, C.C.; Limb, C.J.; Francis, H.W.; Minor, L.B.; Carey, J.P. Hearing outcomes after surgical plugging of the superior semicircular canal by a middle cranial fossa approach. Otol. Neurotol. 2012, 33, 1386–1391. [Google Scholar] [CrossRef]
- Beyea, J.A.; Agrawal, S.K.; Parnes, L.S. Transmastoid semicircular canal occlusion: A safe and highly effective treatment for benign paroxysmal positional vertigo and superior canal dehiscence. Laryngoscope 2012, 122, 1862–1866. [Google Scholar] [CrossRef]
- Van Haesendonck, G.; Van de Heyning, P.; Van Rompaey, V. Retrospective cohort study on hearing outcome after transmastoid plugging in superior semicircular canal dehiscence syndrome: Our Experience. Clin. Otolaryngol. 2016, 41, 601–606. [Google Scholar] [CrossRef]
- Banakis Hartl, R.M.; Cass, S.P. Effectiveness of Transmastoid Plugging for Semicircular Canal Dehiscence Syndrome. Otolaryngol. Head. Neck Surg. 2018, 158, 534–540. [Google Scholar] [CrossRef]
- Zhang, L.; Creighton, F.X., Jr.; Ward, B.K.; Bowditch, S.; Carey, J.P. A Cohort Study of Hearing Outcomes Between Middle Fossa Craniotomy and Transmastoid Approach for Surgical Repair of Superior Semicircular Canal Dehiscence Syndrome. Otol. Neurotol. 2018, 39, e1160–e1167. [Google Scholar] [CrossRef]
- Allsopp, T.; Kim, A.H.; Robbins, A.M.; Page, J.C.; Dornhoffer, J.L. Quality of life outcomes after transmastoid plugging of superior semicircular canal dehiscence. Am. J. Otolaryngol. 2020, 41, 102287. [Google Scholar] [CrossRef]
- Lee, S.Y.; Bae, Y.J.; Kim, M.; Song, J.J.; Choi, B.Y.; Koo, J.W. Changes in Vestibulo-Ocular Reflex Gain After Surgical Plugging of Superior Semicircular Canal Dehiscence. Front. Neurol. 2020, 11, 694. [Google Scholar] [CrossRef] [PubMed]
- Kontorinis, G.; Gaggini, M. Transmastoid Superior Semicircular Canal Plugging: A Prospective Analysis of Surgical Outcomes. Otol. Neurotol. 2021, 42, 1216–1222. [Google Scholar] [CrossRef] [PubMed]
- de Wolf, M.J.F.; Dawe, N.; Jervis, S.; Kumar, R.; Dalton, C.L.; Lindley, K.; Irving, R. Transmastoid Occlusion Surgery for Superior Semicircular Canal Dehiscence Syndrome Improves Patient-Reported Quality-of-Life Measures and corrects cVEMP Thresholds and Amplitudes. Otol. Neurotol. 2021, 42, 1534–1543. [Google Scholar] [CrossRef] [PubMed]
- Gersdorff, G.; Blaivie, C.; de Foer, B.; Deggouj, N.; Wyckmans, F.; Somers, T. Evaluation of the transmastoid plugging approach for superior semicircular canal dehiscences: A retrospective series of 30 ears. Eur. Arch. Otorhinolaryngol. 2022, 279, 4861–4869. [Google Scholar] [CrossRef] [PubMed]
- Stultiens, J.J.A.; Guinand, N.; Van Rompaey, V.; Pérez Fornos, A.; Kunst, H.P.M.; Kingma, H.; van de Berg, R. The resilience of the inner ear-vestibular and audiometric impact of transmastoid semicircular canal plugging. J. Neurol. 2022, 269, 5229–5238. [Google Scholar] [CrossRef]
- Castellucci, A.; Piras, G.; Del Vecchio, V.; Crocetta, F.M.; Maiolo, V.; Ferri, G.G.; Ghidini, A.; Brandolini, C. The effect of superior canal dehiscence size and location on audiometric measurements, vestibular-evoked myogenic potentials and video-head impulse testing. Eur. Arch. Otorhinolaryngol. 2021, 278, 997–1015. [Google Scholar] [CrossRef]
- Mukherjee, P.; Chiarovano, E.; Cheng, K.; Manzari, L.; McGarvie, L.A.; MacDougall, H.G. Video-head impulse test in superior canal dehiscence. Acta Otolaryngol. 2021, 141, 471–475. [Google Scholar] [CrossRef]
- Tikka, T.; Slim, M.A.M.; Gaggini, M.; Kontorinis, G. Video Head Impulse Test (vHIT) Findings in Patients With Superior Semicircular Canal Dehiscence: A Case-Control Study. J. Int. Adv. Otol. 2021, 17, 103–108. [Google Scholar] [CrossRef]
- Renteria, A.E.; Elblidi, A.; Altamami, N.; Alhabib, S.; Saliba, I. Video Head Impulse Test Demonstrates a Residual Function after Plugging of Dehiscent Superior Semicircular Canal. Otol. Neurotol. 2023, 44, 252–259. [Google Scholar] [CrossRef]
- Halmagyi, G.M.; Chen, L.; MacDougall, H.G.; Weber, K.P.; McGarvie, L.A.; Curthoys, I.S. The video head impulse test. Front. Neurol. 2017, 8, 258. [Google Scholar] [CrossRef]
- Kim, J.S.; Kim, H.J. Inferior vestibular neuritis. J. Neurol. 2012, 259, 1553–1560. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.L.; Kong, J.; Flanagan, S.; Pogson, J.; Croxson, G.; Pohl, D.; Welgampola, M.S. Prevalence of vestibular dysfunction in patients with vestibular schwannoma using video head-impulses and vestibular-evoked potentials. J. Neurol. 2015, 262, 1228–1237. [Google Scholar] [CrossRef] [PubMed]
- Castellucci, A.; Malara, P.; Brandolini, C.; Del Vecchio, V.; Giordano, D.; Ghidini, A.; Ferri, G.G.; Pirodda, A. Isolated horizontal canal hypofunction differentiating a canalith jam from an acute peripheral vestibular loss. Am. J. Otolaryngol. 2019, 40, 319–322. [Google Scholar] [CrossRef] [PubMed]
- Castellucci, A.; Malara, P.; Martellucci, S.; Botti, C.; Delmonte, S.; Quaglieri, S.; Rebecchi, E.; Armato, E.; Ralli, M.; Manfrin, M.L.; et al. Feasibility of Using the Video-Head Impulse Test to Detect the Involved Canal in Benign Paroxysmal Positional Vertigo Presenting With Positional Downbeat Nystagmus. Front. Neurol. 2020, 11, 578588. [Google Scholar] [CrossRef]
- Castellucci, A.; Piras, G.; Del Vecchio, V.; Ferri, G.G.; Ghidini, A.; Brandolini, C. Which Inner Ear Disorders Lie Behind a Selective Posterior Semicircular Canal Hypofunction on Video Head. Impulse Test? Otol. Neurotol. 2021, 42, 573–584. [Google Scholar] [CrossRef]
- Comacchio, F.; Castellucci, A. Posterior semicircular canal ossification following acute vestibular loss mimicking inferior vestibular neuritis: A case report. Front. Neurol. 2022, 13, 1015555. [Google Scholar] [CrossRef]
- Castellucci, A.; Botti, C.; Delmonte, S.; Bettini, M.; Lusetti, F.; Brizzi, P.; Ruberto, R.; Gamberini, L.; Martellucci, S.; Malara, P.; et al. Vestibular assessment in sudden sensorineural hearing loss: Role in the prediction of hearing outcome and in the early detection of vascular and hydropic pathomechanisms. Front. Neurol. 2023, 14, 1127008. [Google Scholar] [CrossRef]
- Castellucci, A.; Brandolini, C.; Del Vecchio, V.; Giordano, D.; Pernice, C.; Bianchin, G.; Maiolo, V.; Ferri, G.G. Temporal Bone Meningocele Associated With Superior Canal Dehiscence. Otol. Neurotol. 2018, 39, e506–e508. [Google Scholar] [CrossRef]
- Constant Ionescu, E.; Idriss, S.; Reynard, P.; Ltaief-Boudrigua, A.; Thai-Van, H. Persistent Positional Vertigo in a Patient with Partial “Auto-Plugged” Superior Semicircular Canal Dehiscence: A Case Study. J. Int. Adv. Otol. 2022, 18, 188–191. [Google Scholar] [CrossRef]
- Hirvonen, T.P.; Weg, N.; Zinreich, S.J.; Minor, L.B. High-resolution CT findings suggest a developmental abnormality underlying superior canal dehiscence syndrome. Acta Otolaryngol. 2003, 123, 477–481. [Google Scholar] [CrossRef]
- Rajan, G.P.; Leaper, M.R.; Goggin, L.; Atlas, M.D.; Boeddinghaus, R.; Eikelboom, R.K. The effects of superior semicircular canal dehiscence on the labyrinth: Does size matter? Otol. Neurotol. 2008, 29, 972–975. [Google Scholar] [CrossRef] [PubMed]
- Pfammatter, A.; Darrouzet, V.; Gärtner, M.; Somers, T.; Van Dinther, J.; Trabalzini, F.; Ayache, D.; Linder, T. A superior semicircular canal dehiscence syndrome multicenter study: Is there an association between size and symptoms? Otol. Neurotol. 2010, 31, 447–454. [Google Scholar] [CrossRef] [PubMed]
- Saliba, I.; Maniakas, A.; Benamira, L.Z.; Nehme, J.; Benoit, M.; Montreuil-Jacques, V. Superior canal dehiscence syndrome: Clinical manifestations and radiologic correlations. Eur. Arch. Otorhinolaryngol. 2014, 271, 2905–2914. [Google Scholar] [CrossRef] [PubMed]
- Niesten, M.E.; Hamberg, L.M.; Silverman, J.B.; Lou, K.V.; McCall, A.A.; Windsor, A.; Curtin, H.D.; Herrmann, B.S.; Grolman, W.; Nakajima, H.H.; et al. Superior canal dehiscence length and location influences clinical presentation and audiometric and cervical vestibular-evoked myogenic potential testing. Audiol. Neurootol. 2014, 19, 97–105. [Google Scholar] [CrossRef] [PubMed]
- Darr, A.; Thomas, C.; Rainsbury, J.; Banga, R.; Irving, R.; Chavda, S. Relationship Between Clinical Features and the Arc and Length of Dehiscence in SCDS: A Single Center Review of 42 Cases. Otol. Neurotol. 2022, 43, 236–243. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.H.; Patel, V.S.; Yang, I.; Gopen, Q.S. Computed tomography approximated superior semicircular canal dehiscence size and location and their association with clinical presentation. J. Clin. Neurosci. 2023, 112, 30–37. [Google Scholar] [CrossRef]
- Yuen, H.W.; Boeddinghaus, R.; Eikelboom, R.H.; Atlas, M.D. The relationship between the air-bone gap and the size of superior semicircular canal dehiscence. Otolaryngol. Head. Neck Surg. 2009, 141, 689–694. [Google Scholar] [CrossRef]
- Manzari, L.; Burgess, A.M.; McGarvie, L.A.; Curthoys, I.S. Ocular and cervical vestibular evoked myogenic potentials to 500 Hz fz bone-conducted vibration in superior semicircular canal dehiscence. Ear Hear. 2012, 33, 508–520. [Google Scholar] [CrossRef]
- Chien, W.W.; Janky, K.; Minor, L.B.; Carey, J.P. Superior canal dehiscence size: Multivariate assessment of clinical impact. Otol. Neurotol. 2012, 33, 810–815. [Google Scholar] [CrossRef]
- Hunter, J.B.; O’Connell, B.P.; Wang, J.; Chakravorti, S.; Makowiec, K.; Carlson, M.L.; Dawant, B.; McCaslin, D.L.; Noble, J.H.; Wanna, G.B. Correlation of Superior Canal Dehiscence Surface Area With Vestibular Evoked Myogenic Potentials, Audiometric Thresholds, and Dizziness Handicap. Otol. Neurotol. 2016, 37, 1104–1110. [Google Scholar] [CrossRef]
- Maheu, M.; Elblidi, A.; Saliba, I. Investigating Performance of cVEMP and oVEMP in the Identification of Superior Canal Dehiscence in Relation to Dehiscence Location and Size. Audiol. Res. 2021, 11, 452–462. [Google Scholar] [CrossRef] [PubMed]
- Castellucci, A.; Martellucci, S.; Malara, P.; Botti, C.; Del Vecchio, V.; Brandolini, C.; Ferri, G.G.; Ghidini, A.; Armato, E. Possible pathomechanisms accounting for both sound/pressure-induced eye movements and video head impulse test data in superior canal dehiscence. Acta Otolaryngol. 2021, 141, 749–753. [Google Scholar] [CrossRef] [PubMed]
- Ward, B.K.; van de Berg, R.; van Rompaey, V.; Bisdorff, A.; Hullar, T.E.; Welgampola, M.S.; Carey, J.P. Superior semicircular canal dehiscence syndrome: Diagnostic criteria consensus document of the committee for the classification of vestibular disorders of the Bárány Society. J. Vestib. Res. 2021, 31, 131–141. [Google Scholar] [CrossRef]
- Xie, Y.; Sharon, J.D.; Pross, S.E.; Abt, N.B.; Varma, S.; Della Santina, C.C.; Minor, L.B.; Carey, J.P. Surgical Complications from Superior Canal Dehiscence Syndrome Repair: Two Decades of Experience. Otolaryngol. Head. Neck Surg. 2017, 157, 273–280. [Google Scholar] [CrossRef]
- Lin, K.F.; Bojrab, D.I., 2nd; Fritz, C.G.; Vandieren, A.; Babu, S.C. Hearing Outcomes After Surgical Manipulation of the Membranous Labyrinth During Superior Semicircular Canal Dehiscence Plugging or Posterior Semicircular Canal Occlusion. Otol. Neurotol. 2021, 42, 806–814. [Google Scholar] [CrossRef]
- Agrawal, Y.; Migliaccio, A.A.; Minor, L.B.; Carey, J.P. Vestibular hypofunction in the initial postoperative period after surgical treatment of superior semicircular canal dehiscence. Otol. Neurotol. 2009, 30, 502–506. [Google Scholar] [CrossRef] [PubMed]
- Janky, K.L.; Zuniga, M.G.; Carey, J.P.; Schubert, M. Balance dysfunction and recovery after surgery for superior canal dehiscence syndrome. Arch. Otolaryngol. Head. Neck Surg. 2012, 138, 723–730. [Google Scholar] [CrossRef] [PubMed]
- Mantokoudis, G.; Saber Tehrani, A.S.; Wong, A.L.; Agrawal, Y.; Wenzel, A.; Carey, J.P. Adaptation and Compensation of Vestibular Responses Following Superior Canal Dehiscence Surgery. Otol. Neurotol. 2016, 37, 1399–1405. [Google Scholar] [CrossRef]
- Barber, S.R.; Cheng, Y.S.; Owoc, M.; Lin, B.M.; Remenschneider, A.K.; Kozin, E.D.; Lee, D.J. Benign paroxysmal positional vertigo commonly occurs following repair of superior canal dehiscence. Laryngoscope 2016, 126, 2092–2097. [Google Scholar] [CrossRef]
- Hassannia, F.; Douglas-Jones, P.; Rutka, J.A. Gauging the effectiveness of canal occlusion surgery: How I do it. J. Laryngol. Otol. 2019, 133, 1012–1016. [Google Scholar] [CrossRef]
- Rabbitt, R.D.; Boyle, R.; Highstein, S.M. Physiology of the semicircular canals after surgical plugging. Ann. N. Y Acad. Sci. 2001, 942, 274–286. [Google Scholar] [CrossRef]
- Sadeghi, S.G.; Goldberg, J.M.; Minor, L.B.; Cullen, K.E. Effects of canal plugging on the vestibuloocular reflex and vestibular nerve discharge during passive and active head rotations. J. Neurophysiol. 2009, 102, 2693–2703. [Google Scholar] [CrossRef]
- Arts, H.A.; Adams, M.E.; Telian, S.A.; El-Kashlan, H.; Kileny, P.R. Reversible electrocochleographic abnormalities in superior canal dehiscence. Otol. Neurotol. 2009, 30, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Brandolini, C.; Modugno, G.C. Do signs of natural plugging of superior semicircular canal dehiscence exist? Am. J. Otolaryngol. 2012, 33, 268–271. [Google Scholar] [CrossRef] [PubMed]
- Sone, M.; Yoshida, T.; Morimoto, K.; Teranishi, M.; Nakashima, T.; Naganawa, S. Endolymphatic hydrops in superior canal dehiscence and large vestibular aqueduct syndromes. Laryngoscope 2016, 126, 1446–1450. [Google Scholar] [CrossRef] [PubMed]
- Johanis, M.; De Jong, R.; Miao, T.; Hwang, L.; Lum, M.; Kaur, T.; Willis, S.; Arsenault, J.J.; Duong, C.; Yang, I.; et al. Concurrent superior semicircular canal dehiscence and endolymphatic hydrops: A novel case series. Int. J. Surg. Case Rep. 2021, 78, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Ray, A.; Hautefort, C.; Guichard, J.P.; Horion, J.; Herman, P.; Kania, R.; Houdart, E.; Verillaud, B.; Vitaux, H.; Attyé, A.; et al. MRI contribution for the detection of endolymphatic hydrops in patients with superior canal dehiscence syndrome. Eur. Arch. Otorhinolaryngol. 2021, 278, 2229–2238. [Google Scholar] [CrossRef] [PubMed]
- Ionescu, E.C.; Reynard, P.; Damien, M.; Ltaief-Boudrigua, A.; Hermann, R.; Gianoli, G.J.; Thai-Van, H. Why should multiple dehiscences of the otic capsule be considered before surgically treating patients with superior semicircular canal dehiscence? A radiological monocentric review and a case series. Front. Neurol. 2023, 14, 1209567. [Google Scholar] [CrossRef]
- Lee, S.Y.; Lee, Y.; Choi, J.Y.; Bae, Y.J.; Kim, M.; Song, J.J.; Choi, B.Y.; Jeong, W.K.; Koo, J.W. Quantitative three-dimensional image analysis of the superior canal after surgical plugging to treat superior semicircular canal dehiscence. Sci. Rep. 2021, 11, 16112. [Google Scholar] [CrossRef]
- Lookabaugh, S.; Niesten, M.E.; Owoc, M.; Kozin, E.D.; Grolman, W.; Lee, D.J. Audiologic, cVEMP, and Radiologic Progression in Superior Canal Dehiscence Syndrome. Otol. Neurotol. 2016, 37, 1393–1398. [Google Scholar] [CrossRef]
- Patel, N.S.; Hunter, J.B.; O’Connell, B.P.; Bertrand, N.M.; Wanna, G.B.; Carlson, M.L. Risk of progressive hearing loss in untreated superior semicircular canal dehiscence. Laryngoscope 2017, 127, 1181–1186. [Google Scholar] [CrossRef] [PubMed]
- Castellucci, A.; Brandolini, C.; Piras, G.; Del Vecchio, V.; Modugno, G.C.; Ghidini, A.; Pirodda, A. Spontaneous plugging of superior canal: Two possible natural evolutions of an “unstable” dehiscence. J. Vestib. Res. 2018, 28, i-281. [Google Scholar] [CrossRef]
- Verrecchia, L.; Edholm, K.; Pekkari, M. Asymptomatic superior semicircular canal dehiscence. J. Laryngol. Otol. 2022, 136, 87–90. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Ear | Age | Sex | SCD Side | SCD Size (mm) | ABG (dB) | VOR Gain on vHIT | AC cVEMPs | BC cVEMPs | AC oVEMPs | BC oVEMPs | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SSC | HSC | PSC | Thres (dB SPL) | Ampl (µV) | Ampl (µV) | Thres (dB SPL) | Ampl (µV) | TB-Ampl (µV) | Click-Ampl (µV) | ||||||
| 1 | 59 | M | L | 4.6 | 20.00 | 0.47 | 1.04 | 0.73 | 90 | 262.5 | 271.0 | 95 | 6.4 | 9.8 | 16.6 |
| 2 | 36 | M | R | 3.7 | 33.33 | 0.47 | 1.15 | 0.87 | 80 | 237.5 | 201.5 | 80 | 51.4 | 25.8 | 27.0 |
| 3 | 54 | M | L | 2.2 | 23.33 | 0.61 | 1.03 | 0.90 | 85 | 223.0 | 268.0 | 85 | 28.6 | 31.0 | 12.4 |
| 4 | 38 | M | L | 3.8 | 25.00 | 0.56 | 1.13 | 0.79 | 80 | 150.5 | 217.5 | 90 | 49.6 | 47.8 | 48.2 |
| 5 | 40 | M | R | 3.2 | 11.67 | 0.69 | 1.05 | 0.98 | 90 | 281.5 | 224.0 | 80 | 30.0 | 19.2 | 11.8 |
| 6 | 61 | F | L | 4.3 | 28.33 | 0.49 | 1.31 | 0.70 | 65 | 202.0 | 277.0 | 75 | 55.6 | 40.6 | 40.0 |
| 7 | 58 | F | R | 4.9 | 20.00 | 0.50 | 1.06 | 0.82 | 85 | 105.5 | 203.0 | 95 | 7.8 | 5.4 | 16.2 |
| 8 | 68 | F | R | 3.9 | 30.00 | 0.69 | 1.15 | 0.80 | 90 | 204.5 | 132.5 | 90 | 11.4 | 9.6 | 7.0 |
| 9 | 59 | F | R | 3.5 | 23.33 | 0.67 | 1.34 | 1.14 | 95 | 272.5 | 176.0 | 100 | 19.2 | 1.6 | 6.8 |
| 10 | 58 | M | L | 4.9 | 10.00 | 0.67 | 0.88 | 0.79 | 90 | 90.7 | - | 95 | 23.2 | - | - |
| 11 | 66 | F | R | 4.1 | 13.33 | 0.45 | 0.99 | 0.75 | 80 | 151.5 | 94.0 | 90 | 8.2 | 4.6 | 5.0 |
| 12 | 74 | M | L | 4.2 | 28.33 | 0.46 | 0.83 | 0.74 | 85 | 99.0 | 155.0 | 85 | 33.4 | 14.0 | 7.2 |
| 13 | 70 | F | R | 2.7 * | 35.00 | 0.39 | 1.01 | 0.68 | 85 | 169.0 | 295.5 | 95 | 26.8 | 13.4 | 9.2 |
| 14 | 58 | F | L | 2.2 | 6.67 | 0.67 | 1.12 | 0.76 | 110 | 53.5 | 105.0 | 130 | 0.2 | 8.8 | 9.2 |
| 15 | 70 | F | L | 4.4 | 41.67 | 0.51 | 1.15 | 0.79 | 90 | 146.5 | 211.5 | 105 | 6.2 | 7.8 | 15.6 |
| 16 | 40 | F | R | 4.3 | 23.33 | 0.64 | 1.03 | 0.71 | 70 | 186.5 | 184.5 | 75 | 13.4 | 12.8 | 19.0 |
| 17 | 48 | F | R | 1.2 | 31.67 | 0.43 | 0.98 | 0.83 | 70 | 333.0 | - | 75 | 67.8 | - | - |
| 18 | 72 | F | R | 4.9 | 20.00 | 0.52 | 0.85 | 0.73 | 80 | 66.5 | 221.0 | 95 | 16.6 | 3.2 | 5.4 |
| 19 | 77 | M | R | 3.9 | 38.33 | 0.54 | 0.80 | 0.80 | 90 | 151.5 | 93.0 | 100 | 8.4 | 11.2 | 7.4 |
| 20 | 73 | F | L | 3.2 | 28.33 | 0.28 | 0.92 | 0.70 | 90 | 69.5 | 200.0 | 95 | 28.4 | 25.0 | 16.2 |
| 21 | 74 | F | R | 1.5 | 28.33 | 0.60 | 1.15 | 0.72 | 120 | 30.0 | 172.5 | 105 | 7.6 | 13.2 | 14.0 |
| 22 | 44 | M | R | 2.9 | 20.00 | 0.66 | 1.05 | 0.88 | 80 | 295.0 | 248.5 | 75 | 31.8 | 15.8 | 23.2 |
| 23 | 76 | M | L | 2.6 | 25.00 | 0.54 | 1.17 | 1.16 | 130 | 0.5 | 67.5 | 130 | 0.2 | 2.2 | 9.0 |
| 24 | 72 | F | L | 3.8 | 26.67 | 0.54 | 0.90 | 0.79 | 85 | 197.5 | 89.0 | 80 | 57.2 | 22.4 | 18.6 |
| 25 | 59 | M | R | 4.2 | 43.33 | 0.43 | 0.85 | 0.91 | 95 | 168.0 | 81.0 | 100 | 19.2 | 20.0 | 28.2 |
| 26 | 38 | F | R | 5.1 | 25.00 | 0.51 | 1.07 | 0.85 | 70 | 185.0 | 227.5 | 70 | 26.8 | 14.6 | 23.4 |
| 27 | 39 | M | L | 4.1 | 13.33 | 0.42 | 1.01 | 0.83 | 75 | 309.0 | 275.5 | 85 | 20.6 | 8.2 | 6.4 |
| 28 | 75 | M | L | 4.7 | 30.00 | 0.39 | 0.98 | 0.71 | 85 | 143.5 | 81.5 | 85 | 38.2 | 13.4 | 9.4 |
| 29 | 74 | M | L | 3.5 | 19.67 | 0.41 | 0.84 | 0.71 | 70 | 219.0 | - | 95 | 25.5 | - | - |
| 30 | 65 | F | R | 1.5 * | 13.33 | 0.47 | 0.94 | 0.95 | 110 | 146.0 | - | 95 | 70.9 | - | - |
| 31 | 58 | M | L | 4.6 | 15.00 | 0.66 | 0.87 | 0.88 | 70 | 163.0 | - | 85 | 33.1 | - | - |
| 32 | 67 | F | L | 3.4 | 18.33 | 0.39 | 0.82 | 0.73 | 80 | 270.0 | - | 95 | 33.0 | - | - |
| 33 | 69 | F | R | 5.0 | 11.67 | 0.49 | 1.51 | 0.96 | 80 | 312.0 | - | 95 | 22.8 | - | - |
| 34 | 69 | F | L | 4.4 | 11.67 | 0.53 | 1.47 | 0.86 | 80 | 316.0 | - | 95 | 29.6 | - | - |
| 35 | 51 | M | L | 5.8 | 30.00 | 0.13 | 1.14 | 0.78 | 70 | 188.0 | - | 85 | 44.0 | - | - |
| 36 | 60 | M | L | 5.0 | 18.33 | 0.17 | 0.98 | 0.91 | 100 | 76.0 | - | 100 | 41.0 | - | - |
| 37 | 58 | F | R | 5.4 | 20.00 | 0.28 | 0.97 | 0.83 | 75 | 251.0 | - | 95 | 13.0 | - | - |
| 38 | 58 | F | L | 4.1 | 23.33 | 0.43 | 0.81 | 0.76 | 70 | 321.0 | - | 85 | 16.6 | - | - |
| 39 | 72 | F | L | 4.4 | 18.33 | 0.56 | 0.90 | 0.83 | 85 | 257.0 | - | 100 | 14.2 | - | - |
| 40 | 56 | F | R | 4.3 | 30.00 | 0.59 | 1.21 | 0.81 | 65 | 348.0 | - | 75 | 62.8 | - | - |
| 41 | 65 | F | L | 3.0 | 11.67 | 0.31 | 0.81 | 0.78 | 90 | 224.0 | - | 90 | 16.0 | - | - |
| 42 | 74 | M | R | 5.3 | 28.33 | 0.55 | 0.89 | 0.78 | 75 | 130.0 | - | 85 | 48.0 | - | - |
| 43 | 72 | M | R | 3.9 | 16.67 | 0.54 | 0.88 | 1.27 | 100 | 93.0 | - | 100 | 22.7 | - | - |
| 44 | 92 | M | R | 2.1 * | 8.33 | 0.54 | 1.05 | 0.75 | 100 | 104.0 | - | 100 | 15.7 | - | - |
| 45 | 71 | F | L | 3.0 | 16.67 | 0.67 | 0.95 | 0.91 | 95 | 107.0 | - | 95 | 34.0 | - | - |
| 46 | 64 | M | R | 4.8 | 15.00 | 0.68 | 0.87 | 0.89 | 85 | 110.3 | - | 100 | 8.3 | - | - |
| Median | 65 | 4.1 | 21.67 | 0.52 | 1.00 | 0.80 | 85 | 177.0 | 200.8 | 95 | 24.4 | 13.3 | 13.2 | ||
| IQR | 15 | 1.5 | 13.33 | 0.17 | 0.25 | 0.14 | 15 | 151.8 | 130.5 | 15 | 21.7 | 12.5 | 12.7 | ||
| Range | 56 | 4.6 | 63.66 | 0.56 | 0.71 | 0.59 | 65 | 347.5 | 228.0 | 60 | 70.7 | 46.2 | 43.2 | ||
| Ear | Age | Sex | SCD Side | Pre-Operative Auditory Symptoms and Signs | Pre-Operative Vestibular Symptoms and Signs | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Hearing | Hyperacusis | Autophony | Pulsatile Tinnitus | Fullness | Vertigo/Unsteadiness | SVIN Test | vHIT Findings | c/o VEMPs | ||||
| 1 | 19 | M | R | mixed HL | - | yes | yes | - | recurrent vertigo, T, H | up/contra ny | normal | enhanced |
| 2 | 49 | F | L | normal | - | yes | yes | yes | unsteadiness, T, H | up/contra ny | normal | enhanced |
| 3 | 65 | M | R | mixed HL | - | yes | yes | yes | unsteadiness, T, H | ipsi ny | SSC impairment | enhanced |
| 4 | 48 | F | L | CHL | yes | yes | yes | yes | recurrent vertigo | down/ipsi ny | SSC impairment | enhanced |
| 5 | 39 | M | R | CHL | yes | yes | yes | yes | recurrent vertigo, T, H | up/contra ny | SSC impairment | enhanced |
| 6 | 74 | F | Bil | CHL | - | - | - | L | recurrent L BPPV, T, H | L ny | SSC impairment | enhanced |
| 7 | 45 | F | Bil | normal | L | L | Bil | L | unsteadiness, recurrent L BPPV, T, H | down/L ny | normal | enhanced |
| 8 | 54 | M | L | mixed HL | yes | yes | yes | yes | T, H | up/contra ny | normal | enhanced |
| 9 | 68 | M | L | CHL | yes | yes | yes | yes | unsteadiness, T | contra ny | SSC impairment | enhanced |
| 10 | 40 | M | L | normal | yes | yes | yes | yes | H | up/contra ny | SSC impairment | enhanced |
| Ear | Age | Sex | Side of Plug | Post-Operative Auditory Symptoms and Signs | Post-Operative Vestibular Symptoms and Signs | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Transient Hearing Loss | Hyperacusis | Autophony | Pulsatile Tinnitus | Fullness | Transient Vertigo/ Unsteadiness | Transient Spontaneous ny | Transient vHIT Findings | c/o VEMPs | ||||
| 1 | 19 | M | R | slight flat SNHL | - | improved | improved | - | unsteadiness | contra | - | absent |
| 2 | 49 | F | L | slight flat SNHL | - | improved | improved | improved | unsteadiness + BPPV | ipsi then contra | global SC impairment | reduced |
| 3 | 65 | M | R | slight flat SNHL | - | improved | improved | improved | unsteadiness + BPPV | ipsi/down then contra | global SC impairment | absent |
| 4 | 48 | F | L | - | improved | improved | improved | improved | unsteadiness | ipsi then contra | global SC impairment | absent |
| 5 | 39 | M | R | - | improved | improved | improved | improved | unsteadiness | ipsi | - | reduced |
| 6 | 74 | F | L | severe flat SNHL | - | - | - | improved | unsteadiness | ipsi then contra | global SC impairment | reduced |
| 7 | 45 | F | L | - | improved | improved | improved | improved | unsteadiness + BPPV | down/ipsi then contra | global SC impairment | reduced |
| 8 | 54 | M | L | - | improved | improved | improved | improved | unsteadiness + BPPV | up/contra ny | - | reduced |
| 9 | 68 | M | L | severe flat SNHL | improved | improved | improved | improved | unsteadiness | ipsi then contra | global SC impairment | absent |
| 10 | 40 | M | L | - | improved | improved | improved | improved | unsteadiness + BPPV | ipsi | - | reduced |
| Ear | Age | Sex | Side of SCD Surgery | SCD Size (mm) | ABG (dB) | VOR-Gain on vHIT | AC cVEMPs | BC cVEMPs | AC oVEMPs | BC oVEMPs | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| SSC | HSC | PSC | Thres (dB SPL) | Ampl (µV) | Ampl (µV) | Thres (dB SPL) | Ampl (µV) | TB-Ampl (µV) | Click-Ampl (µV) | ||||||
| 1 | 19 | M | R | 1.8 | 5.00 | 0.44 | 1.00 | 0.71 | 130 | 0.5 | - | - | - | - | - |
| 2 | 49 | F | L | 3.0 | 6.67 | 0.36 | 0.96 | 0.58 | 110 | 49.5 | - | - | - | 2.8 | 3.0 |
| 3 | 65 | M | R | 3.1 | 20.00 | 0.58 | 1.11 | 0.42 | 130 | 0.5 | 0.5 | 130 | 0.2 | 0.4 | 0.4 |
| 4 | 48 | F | L | 2.5 * | 11.67 | 0.66 | 0.86 | 0.85 | 120 | 29.0 | 43.5 | 125 | 3.2 | 3.8 | 0.8 |
| 5 | 39 | M | R | 4.0 | 21.67 | 0.47 | 1.01 | 0.80 | 120 | 71.0 | 106.5 | 130 | 0.2 | 0.8 | 5.2 |
| 6 | 74 | F | L | 4.5 | 21.67 | 0.30 | 0.98 | 0.51 | 120 | 15.5 | 61.0 | 130 | 0.2 | 1.4 | 10.8 |
| 7 | 45 | F | L | 1.8 | 10.00 | 0.23 | 1.15 | 0.61 | 110 | 61.5 | 55.5 | 120 | 5.2 | 5.0 | 4.8 |
| 8 | 54 | M | L | 3.0 | 23.33 | 0.65 | 0.99 | 0.69 | 95 | 112.0 | 102.0 | 100 | 22.0 | 16.8 | 12.2 |
| 9 | 68 | M | L | 5.0 | 16.67 | 0.47 | 0.85 | 0.50 | 120 | 47.0 | 168.0 | 130 | 0.2 | 2.2 | 5.4 |
| 10 | 40 | M | L | 4.3 | 6.67 | 0.37 | 0.98 | 0.82 | 115 | 39.5 | 115.5 | 120 | 2.6 | 1.4 | 0.6 |
| Median | 49 | 3.1 | 14.17 | 0.46 | 0.96 | 0.65 | 120 | 43.3 | 81.5 | 128 | 1.4 | 2.2 | 4.8 | ||
| IQR | 26 | 2.0 | 15.00 | 0.25 | 0.10 | 0.30 | 13 | 52.1 | 66.8 | 10 | 4.5 | 3.3 | 7.4 | ||
| Range | 55 | 3.2 | 18.33 | 0.43 | 0.30 | 0.43 | 35 | 111.5 | 167.5 | 30 | 21.8 | 16.4 | 11.8 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castellucci, A.; Malara, P.; Martellucci, S.; Alfarghal, M.; Brandolini, C.; Piras, G.; Armato, E.; Ruberto, R.R.; Brizzi, P.; Presutti, L.; et al. Impaired Vestibulo-Ocular Reflex on Video Head Impulse Test in Superior Canal Dehiscence: “Spontaneous Plugging” or Endolymphatic Flow Dissipation? Audiol. Res. 2023, 13, 802-820. https://doi.org/10.3390/audiolres13050071
Castellucci A, Malara P, Martellucci S, Alfarghal M, Brandolini C, Piras G, Armato E, Ruberto RR, Brizzi P, Presutti L, et al. Impaired Vestibulo-Ocular Reflex on Video Head Impulse Test in Superior Canal Dehiscence: “Spontaneous Plugging” or Endolymphatic Flow Dissipation? Audiology Research. 2023; 13(5):802-820. https://doi.org/10.3390/audiolres13050071
Chicago/Turabian StyleCastellucci, Andrea, Pasquale Malara, Salvatore Martellucci, Mohamad Alfarghal, Cristina Brandolini, Gianluca Piras, Enrico Armato, Rosanna Rita Ruberto, Pasquale Brizzi, Livio Presutti, and et al. 2023. "Impaired Vestibulo-Ocular Reflex on Video Head Impulse Test in Superior Canal Dehiscence: “Spontaneous Plugging” or Endolymphatic Flow Dissipation?" Audiology Research 13, no. 5: 802-820. https://doi.org/10.3390/audiolres13050071