
Splenic Rupture Secondary to Amyloidosis: A Case Report and Review of the Literature

 ,
,  ,
,
Abstract
:1. Introduction
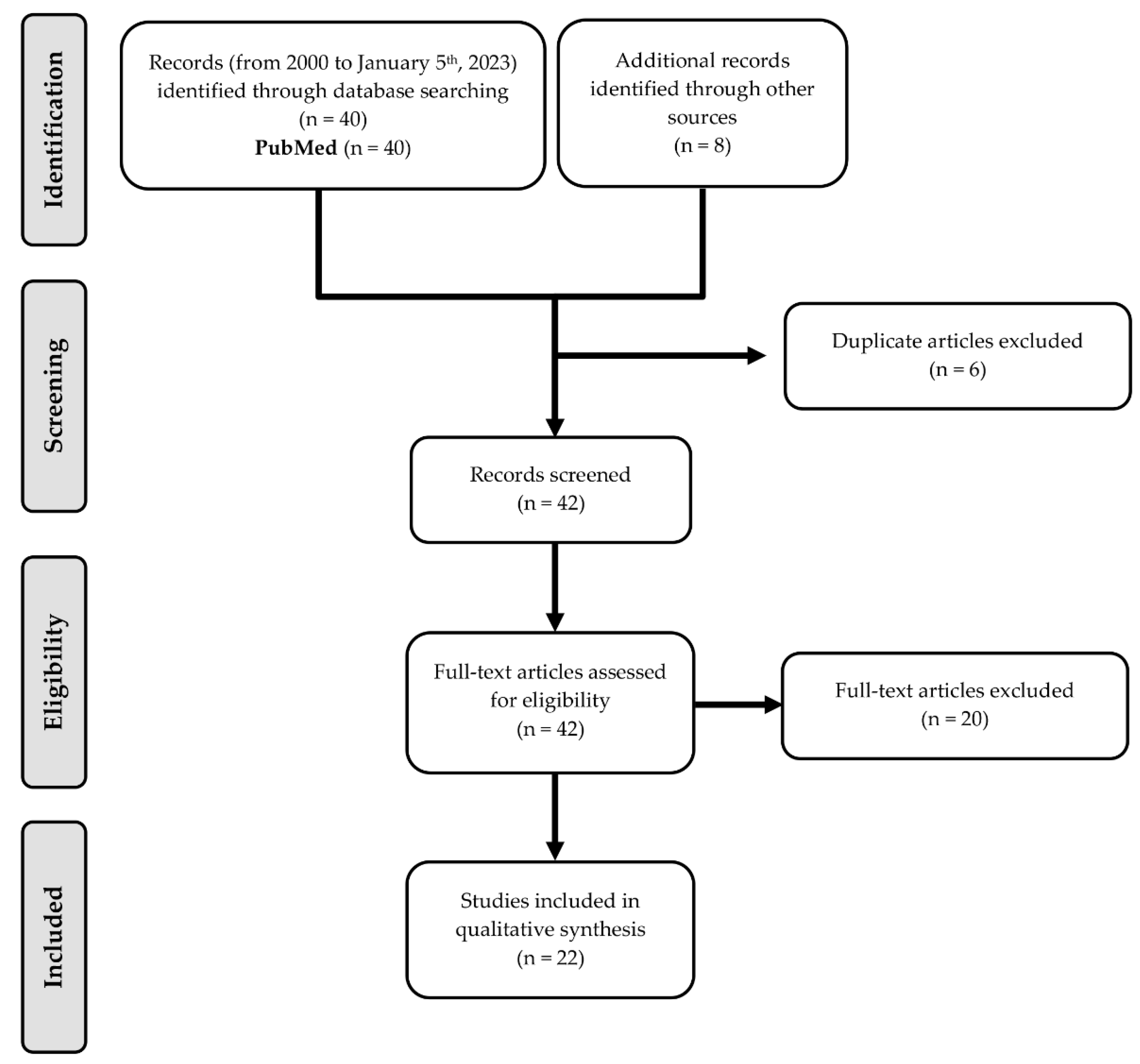
2. Methods
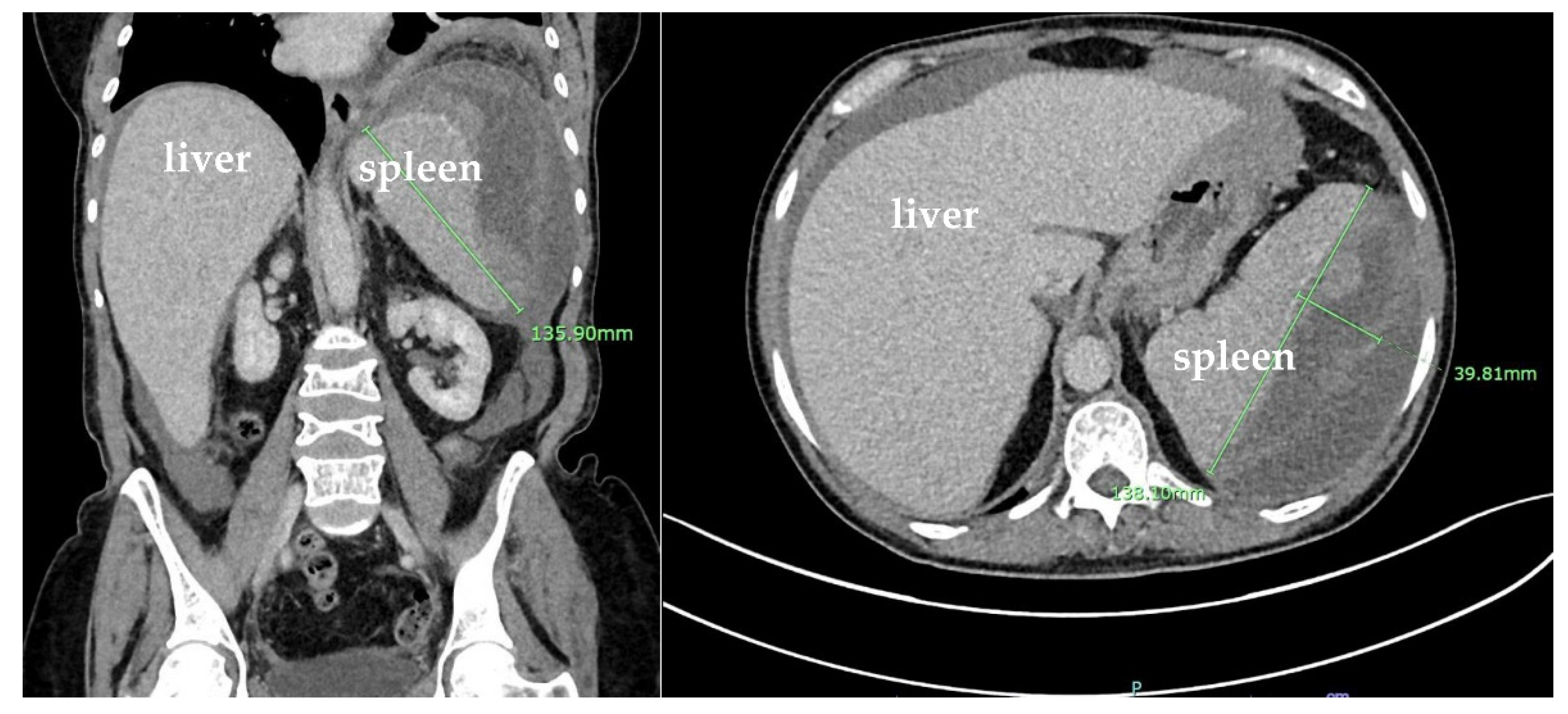
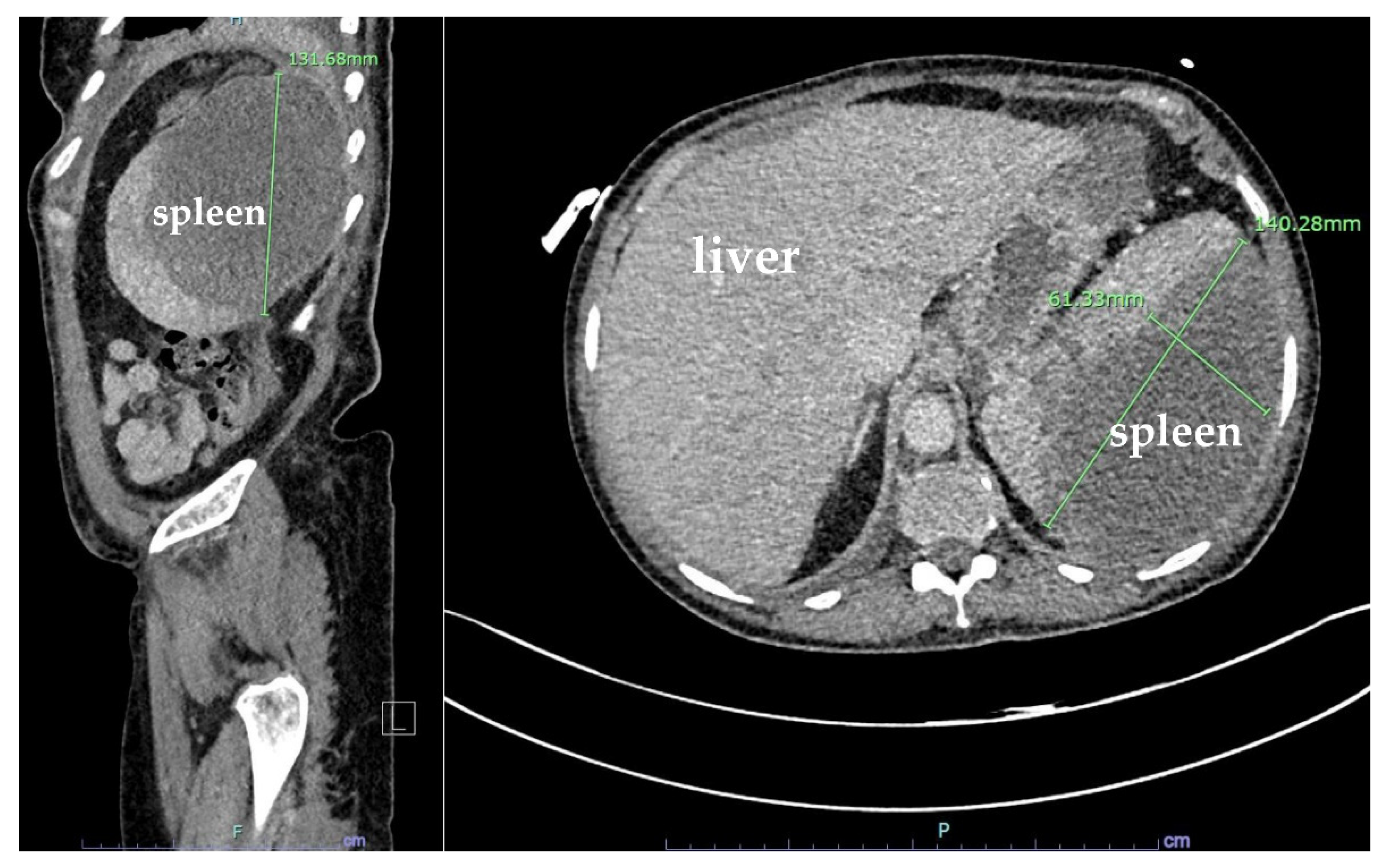
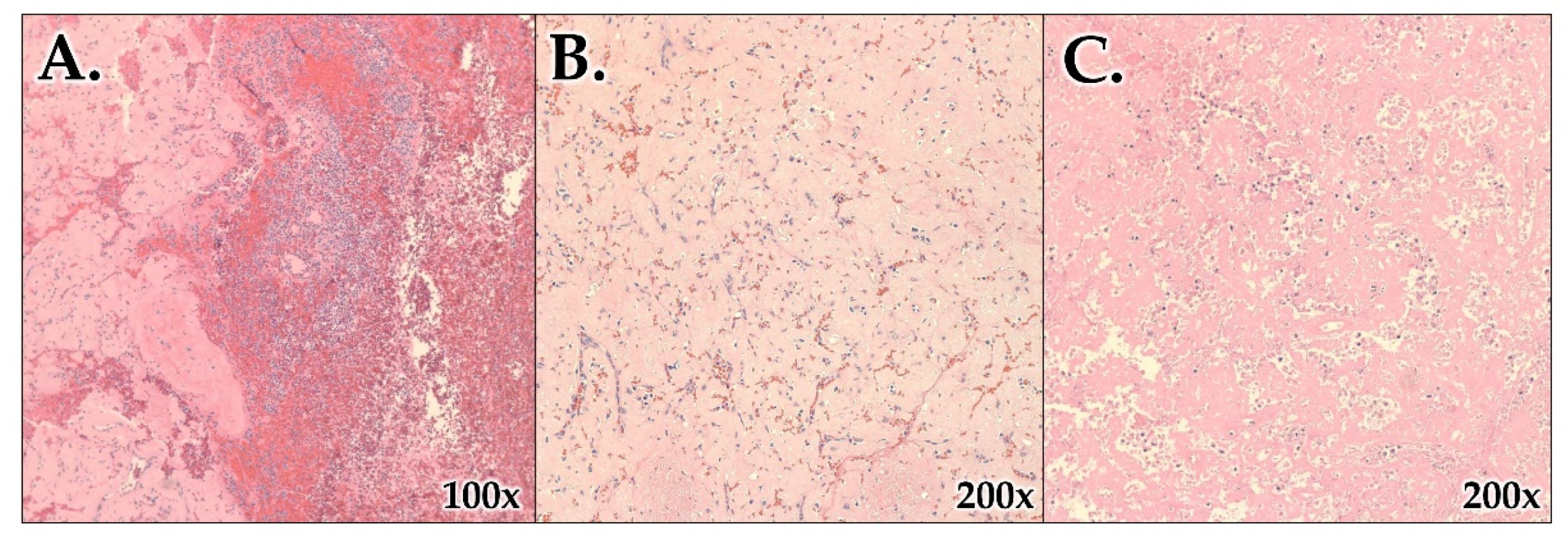
3. Case Presentation
4. Results and Discussion
4.1. Study Designs and Study Population
4.2. AL Amyloidosis as a Risk Factor for Splenic Rupture
4.3. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bellotti, V.; Nuvolone, M.; Giorgetti, S.; Obici, L.; Palladini, G.; Russo, P.; Lavatelli, F.; Perfetti, V.; Merlini, G. The workings of the amyloid diseases. Ann. Med. 2007, 39, 200–207. [Google Scholar] [CrossRef] [PubMed]
- Ke, P.C.; Zhou, R.; Serpell, L.C.; Riek, R.; Knowles, T.P.J.; Lashuel, H.A.; Gazit, E.; Hamley, I.W.; Davis, T.P.; Fändrich, M.; et al. Half a century of amyloids: Past, present and future. Chem. Soc. Rev. 2020, 49, 5473–5509. [Google Scholar] [CrossRef] [PubMed]
- Milani, P.; Merlini, G.; Palladini, G. Light Chain Amyloidosis. Mediterr. J. Hematol. Infect. Dis. 2018, 10, e2018022. [Google Scholar] [CrossRef] [Green Version]
- Bruserud, Ø.; Tvedt, T.H.A.; Ahmed, A.B.; Vintermyr, O.K.; Hervig, T.; Guttormsen, A.B.; Reikvam, H. Spontaneous Splenic Artery Rupture as the First Symptom of Systemic Amyloidosis. Case Rep. Crit. Care 2021, 2021, 6676407. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. J. Clin. Epidemiol. 2009, 62, 1006–1012. [Google Scholar] [CrossRef]
- Quencer, K.B.; Smith, T.A. Review of proximal splenic artery embolization in blunt abdominal trauma. CVIR Endovasc. 2019, 2, 11. [Google Scholar] [CrossRef] [Green Version]
- Lessi, F.; Marson, P.; Colpo, A.; Marino, F.; Branca, A.; Tison, T.; Adami, F. Spontaneous splenic rupture following stem cell mobilization with G-CSF and plerixafor in AL amyloidosis. Transfus. Apher. Sci. 2016, 54, 256–258. [Google Scholar] [CrossRef]
- Buzalewski, J.; Fisher, M.; Rambaran, R.; Lopez, R. Splenic rupture secondary to amyloid light-chain (AL) amyloidosis associated with multiple myeloma. J. Surg. Case Rep. 2019, 2019, rjz021. [Google Scholar] [CrossRef]
- Oran, B.; Wright, D.G.; Seldin, D.C.; McAneny, D.; Skinner, M.; Sanchorawala, V. Spontaneous rupture of the spleen in AL amyloidosis. Am. J. Hematol. 2003, 74, 131–135. [Google Scholar] [CrossRef]
- Chang, C.F.; Liao, Y.S.; Chen, Y.G.; Ye, R.H. Unexpected amyloidosis, mimicking a splenic cyst. Korean J. Intern. Med. 2018, 33, 231–232. [Google Scholar] [CrossRef]
- Sato, S.; Tamai, Y.; Okada, S.; Kannbe, E.; Takeda, K.; Tanaka, E. Atraumatic Splenic Rupture Due to Ectopic Extramedullary Hematopoiesis after Autologous Stem Cell Transplantation in a Patient with AL Amyloidosis. Intern. Med. 2018, 57, 399–402. [Google Scholar] [CrossRef] [Green Version]
- Li, G.; Han, D.; Wei, S.; Wang, H.; Chen, L. Multiorgan involvement by amyloid light chain amyloidosis. J. Int. Med. Res. 2019, 47, 1778–1786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosch, N.; Renteria, A.S.; Quillen, K.; Brauneis, D.; Santilli, J.; Kim, D.; Sanchorawala, V. Nonoperative Management of Spontaneous Splenic Rupture in a Patient with Light-Chain Amyloidosis: A Case Report. J. Vasc. Interv. Radiol. 2015, 26, 1578–1580. [Google Scholar] [CrossRef] [PubMed]
- Chau, E.M.; Chan, A.C.; Chan, W.K. Spontaneous atraumatic rupture of a normal-sized spleen due to AL amyloid angiopathy. Amyloid 2008, 15, 213–215. [Google Scholar] [CrossRef] [PubMed]
- Choudhuri, S.; Cavet, J. Spontaneous splenic rupture due to isolated splenic peliosis in a case of multiple myeloma. Br. J. Haematol. 2009, 144, 146. [Google Scholar] [CrossRef] [PubMed]
- Magnoli, F.; Freguia, S.; Bernasconi, B.; Campiotti, L.; Oldrini, R.; Facco, C.; Sessa, F.; Uccella, S. Fatal splenic rupture in a previously undiagnosed multiple myeloma: Morphological, immunophenotypical and molecular cytogenetic analyses. Clin. Lymphoma Myeloma Leuk. 2013, 13, e22–e25. [Google Scholar] [CrossRef]
- Perrone, L.; Gervaso, L.; Bosco, E.; Serra, F.; Quaquarini, E. Non-traumatic splenic rupture in amyloidosis as a rare evolution of multiple myeloma. Clin. Pract. 2019, 9, 1146. [Google Scholar] [CrossRef] [Green Version]
- Roh, J.; Huh, J. Splenic rupture in primary amyloidosis with chronic neutrophilic leukemia. Blood Res. 2015, 50, 5. [Google Scholar] [CrossRef] [Green Version]
- Shobeiri, H.; Einakchi, M.; Khajeh, M.; Motie, M.R. Spontaneous rupture of the spleen secondary to amyloidosis. J. Coll. Physicians Surg. Pak. 2013, 23, 427–429. [Google Scholar]
- Báez-García Jde, J.; Martínez-Hernández Magro, P.; Iriarte-Gallego, G.; Báez-Aviña, J.A. Spontaneous rupture of the spleen secondary to amyloidosis. Cir. Cir. 2010, 78, 533–537. [Google Scholar]
- Fernández de Larrea, C.; Cibeira, M.T.; Rovira, M.; Rosiñol, L.; Esteve, J.; Bladé, J. Spontaneous rupture of the spleen as immediate complication in autologous transplantation for primary systemic amyloidosis. Eur. J. Haematol. 2008, 80, 182–184. [Google Scholar] [CrossRef]
- Skok, P.; Knehtl, M.; Ceranić, D.; Glumbić, I. Splenic rupture in systemic amyloidosis - case presentation and review of the literature. Z. Gastroenterol. 2009, 47, 292–295. [Google Scholar] [CrossRef]
- Dedi, R.; Bhandari, S.; Sagar, P.M.; Turney, J.H. Delayed splenic rupture as a cause of haemoperitoneum in a CAPD patient with amyloidosis. Nephrol. Dial. Transplant. 2001, 16, 2446. [Google Scholar] [CrossRef] [PubMed]
- Chiu, A.; Dasari, S.; Kurtin, P.J.; Theis, J.D.; Vrana, J.A.; Rech, K.L.; Dao, L.N.; Howard, M.T.; Dalland, J.C.; McPhail, E.D. Proteomic Identification and Clinicopathologic Characterization of Splenic Amyloidosis. Am. J. Surg. Pathol. 2023, 47, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Worel, N.; Schulenburg, A.; Mitterbauer, M.; Keil, F.; Rabitsch, W.; Kalhs, P.; Gisslinger, H.; Raderer, M.; Geissler, K.; Höcker, P.; et al. Autologous stem-cell transplantation in progressing amyloidosis is associated with severe transplant-related toxicity. Wien. Klin. Wochenschr. 2006, 118, 49–53. [Google Scholar] [CrossRef] [PubMed]
- Renzulli, P.; Schoepfer, A.; Mueller, E.; Candinas, D. Atraumatic splenic rupture in amyloidosis. Amyloid 2009, 16, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Elvy, A.; Harbach, L.; Bhangu, A. Atraumatic splenic rupture: A 6-year case series. Eur. J. Emerg. Med. 2011, 18, 124–126. [Google Scholar] [CrossRef]
- Platzbecker, U.; Prange-Krex, G.; Bornhäuser, M.; Koch, R.; Soucek, S.; Aikele, P.; Haack, A.; Haag, C.; Schuler, U.; Berndt, A.; et al. Spleen enlargement in healthy donors during G–CSF mobilization of PBPCs. Transfusion 2001, 41, 184–189. [Google Scholar] [CrossRef]
- Chinaka, U.C.; Fultang, J.; Pereca, J.; Ali, A. Atraumatic idiopathic splenic rupture induced by granulocyte-colony stimulating factor (G-CSF) for the treatment of pancytopenia, managed successfully by laparoscopic splenectomy. BMJ Case Rep. 2020, 13, e232411. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Blood Test | Patient Value | Reference Range |
|---|---|---|
| White blood cell (WBC) count | 11.92 × 103/μL | 4.8–10.8 × 103/μL |
| Segmented neutrophils | 55.0% | 42–75% |
| Absolute neutrophil count | 7.33 × 103/μL | 1.8–7.2 × 103/μL |
| Red blood cell (RBC) count | 3.66 × 106/μL | 3.93–5.22 × 106/μL |
| Hemoglobin | 11.7 g/dL | 12.0–16.0 g/dL |
| Hematocrit | 34.4% | 37.0–47.0% |
| MCV | 94.0 fL | 79.0–92.2 fL |
| MCH | 32.0 pg | 25.6–32.2 pg |
| MCHC | 34.0 g/dL | 32.0–36.0 g/dL |
| Platelet count | 323 × 103/uL | 150–450 × 103/uL |
| SARS-CoV-2 | NOT DETECTED | NOT DETECTED |
| HgbA1C | 6.5% | 4.2–5.6% |
| C-Reactive Protein | 14.7 mg/L | 0.0–3.0 mg/L |
| Blood smear | Large platelets seen | - |
| Author (Year) | Country | Design/ Participants | Main Findings | Strengths/Weaknesses | Comments |
|---|---|---|---|---|---|
| Bruserud et al., 2021 [4] | Norway | Case report, 67-year-old male | Early recognition of hemorrhagic shock and prompt action restored intravascular volume and SpO2 and were lifesaving | Weaknesses: 1 patient was still in hospital receiving treatment when this was written | NSR 2/2 AL amyloidosis patient received 3 courses of chemo with no change in serum lambda levels, treated with daratumumab (which stabilized lambda levels), exploratory laparotomy, and splenectomy |
| Chiu et al., 2022 [24] | USA | Retrospective cohort, 69 patients with spleen amyloidosis from 2008–2020 | Atraumatic splenic rupture was the most common reason for splenectomy in AL cases | Strength: larger sample size, good generalizability since data came from multiple hospitals, had original copies of all data | Only 2 patients had a prior amyloid Dx. Found AL-lambda had diffuse pattern of amyloid deposition with extensive architectural effacement and was more frequently associated with splenic rupture |
| Lessi et al., 2015 [7] | Italy | Case report, 50-year-old woman | Physicians should monitor for NSR when peripheral stem cell mobilization with G-CSF or both G-CSF and plerixafor is performed in patients with AL amyloidosis due to risk of splenomegaly | Weakness: 1 patient | Previously healthy patient, Dx with cardiac AL amyloidosis, underwent peripheral stem cell mobilization and G-CSF; US showed NSR, patient underwent splenectomy and recovered |
| Buzalewski et al., 2019 [8] | USA | Case report, 68-year-old male | Most common cause of atraumatic splenic rupture is hematologic processes; amyloidosis is rare | Weakness: 1 patient, multiple comorbidities, multiple prior treatments, multiple hematologic diagnoses | CT on admission showed splenomegaly and splenic hematoma, treated with exploratory laparotomy and splenectomy; multiple post op complications; Dx with AL amyloidosis and MM |
| Oran et al., 2003 [9] | USA | Case report on 4 patients
| G-CSF may play a role in the development of AL amyloidosis, factor X deficiency may contribute; splenectomy is safe in these patients. There is little rationale for splenic salvage | Weakness: small sample size, short cases may not provide all necessary details | Splenic rupture was manifestation of disease in 1 case, 3 cases had splenic rupture during or after HDM/SCT, 2 had factor X deficiency, all 4 had splenectomy that was uncomplicated |
| Chang et al., 2017 [10] | Taiwan | Case report, 87-year-old male | Most cases of splenic amyloidosis are global, but it was local in this case. Clinicians should be aware that splenic amyloidosis can lead to hyposplenism with infection and increased risk of NSR | Weakness: 1 patient | Dx with splenic cyst, failed 1st line therapy. Microscopic eval of abscess showed light chains. Dx isolated splenic AL amyloidosis |
| Sato et al., 2018 [11] | Japan | Case report, 50-year-old male | Special attention is required for amyloidosis patients undergoing auto-SCT even when GCSF is not administered. Atraumatic splenic rupture is rare but is associated with high mortality rate. Amyloid proteins in spleen cause capsule to become fragile | Weakness: 1 patient | Dx MM complicated AL amyloidosis. Splenic rupture complicated during autologous stem cell transplantation (SCT) in absence of GCSF administration, which has previously been linked to amyloidosis splenic rupture. Patient underwent emergent open splenectomy |
| Li et al., 2019 [12] | China | Case report, 45-year-old male | Dx of this disease took 12 months, suggesting a challenge to Dx. Congo red stain is the gold standard. There are many ways to detect and treat AL amyloidosis. Chemo requires close monitoring | Weakness: 1 patient, and many test results were performed at a prior hospital and the original images or results could not be obtained in those cases | Dx with NSR and hemorrhagic shock, patient had multiorgan involvement and was treated with RPCD regimen. Stable disease state but gradual drug tolerance and insufficient therapeutic response |
| Bosch et al., 2015 [13] | USA | Case report, 44-year-old female | Splenic artery embolization can be a successful management strategy for the treatment of NSR in AL amyloidosis | Weakness: 1 patient, and cannot say for sure that the spleen would have ruptured without the embolization | The patient was treated with induction therapy with bortezomib, and dexamethasone followed by HDM/SCT, admitted 7 days later. CT showed perisplenic bleeding. Splenic artery angiography showed no active extravasation. Underwent distal splenic artery embolization and no further hemodynamic instability |
| Worel et al., 2006 [25] | Austria | Controlled clinical trial, 6 patients between 43 and 59 years old, previously Dx with AL amyloidosis, previously treated with rhG-CSF alone or treated with cyclophosphamide and rhG-CSF | Treatment of select patients with AL amyloidosis with high-dose melphalan and stem-cell support results in reversal of amyloid-related disease and improved survival | Weakness: risk for confounding, and researcher’s conclusion is too generalized | Of all the patients, 1 patient died from sepsis after stem-cell mobilization, 5 had high-dose melphalan and had severe toxicity, 1 died from GI perf, 1 had hyperfibrinolysis and spontaneous splenic rupture, 1 had severe bleeding, 3 needed hemodialysis, and 1 had a renal transplant |
| Chau et al., 2008 [14] | Japan | Case report, 74-year-old female | Splenomegaly not needed for NSR. Emergency laparoscopic splenectomy is necessary | Weakness: 1 patient, extensive comorbidities | Dx with AL amyloidosis on peritoneal dialysis, patient underwent laparoscopy, which showed NSR with normal-size spleen |
| Choudhuri et al., 2008 [15] | UK | Case report, 59-year-old male | Splenic peliosis is an extremely rare manifestation of MM, urgent operative intervention is required | Weakness: 1 patient, very short case report, and other necessary information may be missing | Dx with MM which was asymptomatic; 6 years later, patient experienced renal impairment, and then, had NSR, emergency splenectomy. Patient had splenic peliosis |
| Magnoli et al., 2013 [16] | Italy | Case report, 49-year-old woman | Very aggressive behavior of MM is related to peculiar molecular features with cell cycle progression and microenvironment interactions | Weakness: 1 patient | NSR on CT. Splenectomy complicated by consumption coagulopathy. Patient died from DIC and multiple organ dysfunction syndrome. Performed path exam of spleen and found MM |
| Perrone et al., 2019 [17] | Italy | Case report, 64-year-old male | AL amyloidosis can evolve from MM. Survival improvement in treatment of MM due to new therapies increases probability of developing amyloidosis. Clinicians should control patients for amyloid-induced organ damage | Weakness: 1 patient, several comorbidities, several treatments provided from Dx to death, possible confounding, and bias | Dx of IgG lambda MM, stem cell transplant, NSR 2/2 amyloidosis, treated with exploratory laparotomy and splenectomy |
| Renzulli et al., 2009 [26] | Switzerland | Review, 15 women and 16 men with mean age of 53 with atraumatic splenic rupture; 25 had AL amyloidosis, 4 had secondary amyloidosis, 2 had unspecified amyloidosis | NSR in amyloidosis has a high 30-day mortality rate and occurs mostly in those with undiagnosed amyloidosis. Identified splenomegaly, coagulation abnormalities, and autologous stem cell transplant as predisposing factors | Strength: review of multiple sources, good generalizability of findings Weakness: small sample size | Of 31 patients with NSR in amyloidosis, 79% had NSR as initial manifestation, 8% were affected with MM. Splenic rupture 30-day mortality rate = 26% |
| Roh and Huh 2015 [18] | Korea | Case report, 53-year-old male | Identified amyloidosis with deposition of pink/amorphous material microscopically and apple-green birefringence via Congo red stain | Weakness: 1 patient, very short case report | Dx MM, CT showed nontraumatic splenic rupture |
| Elvy et al., 2011 [27] | UK | Retrospective cohort, 7 patients from the same hospital over 6 years | CT facilitates Dx. Early total splenectomy is needed. High index of suspicion should be maintained by ER physicians | Weakness: same hospital so low generalizability, and small sample size | All patients required splenectomy; 1 had amyloidosis |
| Shobeiri et al., 2013 [19] | Iran | Case report, 61-year-old male | In patients with abdominal pain and hypotension, NSR should be suspected in those without trauma or infection Hx | Weakness: 1 patient | Ultrasound showed NSR; performed laparotomy and found hemoperitoneum 2/2 NSR. Path examination of spleen showed AL amyloidosis |
| Garcia et al., 2010 [20] | Mexico | Case report, 46-year-old male | In patients with abdominal pain and hypotension, NSR should be suspected in those without trauma or infection Hx | Weakness: 1 patient | Performed laparotomy and found hemoperitoneum 2/2 NSR. Performed splenectomy, and path report showed AL amyloidosis |
| Fernandez de Larrea et al., 2008 [21] | Spain | Case report, 51-year-old woman | Only a few cases of splenic rupture from stem cells have been reported. NSR is a medical emergency that needs rapid Dx, especially in those with factor X deficiency or undergoing G-CSF | Weakness: 1 patient | Found AL amyloidosis on renal biopsy. Patient had NSR 24 h after infusion of peripheral blood stem cells and died from multiorgan failure |
| Dedi et al., 2001 [23] | UK | Case report, 59-year-old woman | Splenic rupture should be considered in the Dx of hemoperitoneum complicating peritoneal dialysis, especially in those with amyloidosis. Injury may precede clinical presentation | Weakness: 1 patient, stated that the bleed “appeared” to be from minor trauma, but that cannot be known | Patient on dialysis for end-stage renal failure 2/2 AL amyloidosis; had a minor fall downstairs and admitted 4 days later. Died from numerous complications 6 weeks later. Found amyloidosis in spleen and subcapsular splenic bleed |
| Skok et al., 2009 [22] | Slovenia | Case report, 52-year-old male | Splenomegaly is a risk factor for splenic rupture in patients with AL amyloidosis | Weakness: 1 patient | Patient previously treated for undefined hepatic disease and anemia, confirmed posthumously to be AL amyloidosis. Died from NSR |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bahmad, H.F.; Gogola, S.; Burton, L.; Alloush, F.; Cusnir, M.; Schwartz, M.; Howard, L.; Sriganeshan, V. Splenic Rupture Secondary to Amyloidosis: A Case Report and Review of the Literature. Hematol. Rep. 2023, 15, 370-383. https://doi.org/10.3390/hematolrep15020038
Bahmad HF, Gogola S, Burton L, Alloush F, Cusnir M, Schwartz M, Howard L, Sriganeshan V. Splenic Rupture Secondary to Amyloidosis: A Case Report and Review of the Literature. Hematology Reports. 2023; 15(2):370-383. https://doi.org/10.3390/hematolrep15020038
Chicago/Turabian StyleBahmad, Hisham F., Samantha Gogola, Lorena Burton, Ferial Alloush, Mike Cusnir, Michael Schwartz, Lydia Howard, and Vathany Sriganeshan. 2023. "Splenic Rupture Secondary to Amyloidosis: A Case Report and Review of the Literature" Hematology Reports 15, no. 2: 370-383. https://doi.org/10.3390/hematolrep15020038