
Phenazopyridine-Induced Methemoglobinemia in a Jehovah’s Witness Treated with High-Dose Ascorbic Acid Due to Methylene Blue Contradictions: A Case Report and Review of the Literature
Abstract
:1. Introduction
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iolascon, A.; Bianchi, P.; Andolfo, I.; Russo, R.; Barcellini, W.; Fermo, E.; Toldi, G.; Ghirardello, S.; Rees, D.; Van Wijk, R.; et al. Recommendations for diagnosis and treatment of methemoglobinemia. Am. J. Hematol. 2021, 96, 1666–1678. [Google Scholar] [CrossRef] [PubMed]
- Ludlow, J.T.; Wilkerson, R.G.; Nappe, T.M. Methemoglobinemia. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK537317/ (accessed on 17 December 2022).
- Crowley, M.A.; Mollan, T.L.; Abdulmalik, O.Y.; Butler, A.D.; Goodwin, E.F.; Sarkar, A.; Stolle, C.A.; Gow, A.J.; Olson, J.S.; Weiss, M.J. A hemoglobin variant associated with neonatal cyanosis and anemia. N. Engl. J. Med. 2011, 364, 1837. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.M.; Prchal, J.T. Methemoglobinemia and other dyshemoglobinemias. In Williams Hematology, 9e; Kaushansky, K., Lichtman, M.A., Prchal, J.T., Levi, M.M., Press, O.W., Burns, L.J., Caligiuri, M., Eds.; McGraw Hill: New York, NY, USA, 2015; p. 789. [Google Scholar]
- Wright, R.O.; Lewander, W.J.; Woolf, A.D. Methemoglobinemia: Etiology, pharmacology, and clinical management. Ann. Emerg. Med. 1999, 34, 646–656. [Google Scholar] [CrossRef] [PubMed]
- Wilkerson, R.G. Getting the blues at a rock concert: A case of severe methaemoglobinaemia. Emerg. Med. Australas. 2010, 22, 466–469. [Google Scholar] [CrossRef]
- Murphy, T.; Fernandez, M. Acquired methemoglobinemia from phenazopyridine use. Int. J. Emerg. Med. 2018, 11, 45. [Google Scholar] [CrossRef]
- Shahani, L.; Sattovia, S. Acquired methaemoglobinaemia related to phenazopyridine ingestion. BMJ Case Rep. 2012, 2012, 1–2. [Google Scholar] [CrossRef]
- Yu, C.H.; Wang, C.H.; Chang, C.C. Chocolate-colored blood with normal artery oxygen: Methemoglobinemia related to phenazopyridine. Am. J. Med. Sci. 2011, 341, 337. [Google Scholar] [CrossRef]
- Kc, O.; Subedi, A.; Sharma, R.; Dahal, P.H.; Koirala, M. A Case of Severe Hypoxia Caused by Phenazopyridine-Induced Methemoglobinemia: A near Fatal Event from Over-the-Counter Medication Use. Clin. Pract. 2022, 12, 845–851. [Google Scholar] [CrossRef]
- Hamza, A.; Nasrullah, A.; Singh, R.; DiSilvio, B. Phenazopyridine-Induced Methaemoglobinaemia The Aftermath of Dysuria Treatment. Eur. J. Case Rep. Intern. Med. 2022, 9, 003191. [Google Scholar] [CrossRef]
- Shah, P.K.; Kraft, K.H. Perioperative Hypoxia Secondary to Phenazopyridine-induced Methemoglobinemia in an Adolescent Patient Without Renal Insufficiency or Overdose: An Unusual Case. Urology 2019, 130, 142–143. [Google Scholar] [CrossRef]
- Kozik, S.; Kirkham, C.; Sudario, G. Acquired Methemoglobinemia in a Ketamine-induced Ulcerative Cystitis Patient: A Case Report. Clin. Pract. Cases Emerg. Med. 2022, 6, 137–140. [Google Scholar] [CrossRef] [PubMed]
- Chiu, D.; Lubin, B. Oxidative hemoglobin denaturation and RBC destruction: The effect of heme on red cell membranes. Semin. Hematol. 1989, 26, 128. [Google Scholar] [PubMed]
- Abe, K.; Sugita, Y. Properties of cytochrome b5 and methemoglobin reduction in human erythrocytes. Eur. J. Biochem. 1979, 101, 423–428. [Google Scholar] [CrossRef] [PubMed]
- Yubisui, T.; Takeshita, M.; Yoneyama, Y. Reduction of methemoglobin through flavin at the physiological concentration by NADPH-flavin reductase of human erythrocytes. J. Biochem. 1980, 87, 1715. [Google Scholar] [CrossRef] [PubMed]
- Rosen, P.J.; Johnson, C.; McGehee, W.G.; Beutler, E. Failure of methylene blue treatment in toxic methemoglobinemia. Association with glucose-6-phosphate dehydrogenase deficiency. Ann. Intern. Med. 1971, 75, 83. [Google Scholar] [CrossRef]
- Rehman, A.; Shehadeh, M.; Khirfan, D.; Jones, A. Severe acute haemolytic anaemia associated with severe methaemoglobinaemia in a G6PD-deficient man. BMJ Case Rep. 2018, 2018, bcr-2017. [Google Scholar] [CrossRef] [PubMed]
- Cheah, C.Y.; Lew, T.E.; Seymour, J.F.; Burbury, K. Rasburicase causing severe oxidative hemolysis and methemoglobinemia in a patient with previously unrecognized glucose-6-phosphate dehydrogenase deficiency. Acta Haematol. 2013, 130, 254–259. [Google Scholar] [CrossRef]
- El Hamzaoui, H.; Chajai, I.; El Ouazzani, M.C.; Benhalima, A.; El Arfaoui, M.; Alilou, M. Acute dapsone poisoning with methemoglobinemia: A case report. Pan Afr. Med. J. 2022, 43, 20. [Google Scholar] [CrossRef]
- Kabir, H.; Lakshmanan, R.; Gopinath, S.; Bhonagiri, D. Dapsone-induced methemoglobinemia-A case report. Clin. Case Rep. 2021, 9, e04054. [Google Scholar] [CrossRef]
- Reeves, D.J.; Saum, L.M.; Birhiray, R.I.V. ascorbic acid for treatment of apparent rasburicase-induced methemoglobinemia in a patient with acute kidney injury and assumed glucose-6-phosphate dehydrogenase deficiency. Am. J. Health Syst. Pharm. 2016, 73, e238–e242. [Google Scholar] [CrossRef]
- Sahu, K.K.; Dhibar, D.P.; Gautam, A.; Kumar, Y.; Varma, S.C. Role of ascorbic acid in the treatment of methemoglobinemia. Turk. J. Emerg. Med. 2016, 16, 119–120. [Google Scholar] [CrossRef] [PubMed]
- De Crem, N.; Verleden, G.M.; Godinas, L.; Vos, R. Once in a blue moon: Primaquine-induced methemoglobinemia—A case report. Respir. Med. Case Rep. 2022, 38, 101675. [Google Scholar] [CrossRef]
- Topal, H.; Topal, Y. Toxic methemoglobinemia treated with ascorbic Acid: Case report. Iran. Red. Crescent. Med. J. 2013, 15, e12718. [Google Scholar] [CrossRef] [PubMed]
- Powell, T.G.; Choi, E.; Vuppala, S.; Hayek, H. Lava Lamp-Induced Methemoglobinemia in Dementia: A Case Report. Cureus 2022, 14, e29441. [Google Scholar] [CrossRef] [PubMed]
- Asif, A.; Preetham, C.; Mahajyoti, C.; Nibedita, M. Clofazimine-induced methemoglobinemia: A rare incidence. J. Fam. Med. Prim. Care 2018, 7, 1573–1575. [Google Scholar] [CrossRef]
- Kilicli, E.; Aksel, G.; Akbuga Ozel, B.; Kavalci, C.; Suveren Artuk, D. Cost of Beauty; Prilocaine Induced Methemoglobinemia. Turk. J. Emerg. Med. 2016, 14, 185–187. [Google Scholar] [CrossRef]
- Park, S.Y.; Lee, K.W.; Kang, T.S. High-dose vitamin C management in dapsone-induced methemoglobinemia. Am. J. Emerg. Med. 2014, 32, 684.e1. [Google Scholar] [CrossRef]
- Singh, P.; Rakesh, K.; Agarwal, R.; Tripathi, P.P.; Dhooria, S.; Sehgal, I.S.; Prasad, K.T.; Hans, R.; Sharma, R.; Sharma, N.; et al. Therapeutic whole blood exchange in the management of methaemoglobinemia: Case series and systematic review of literature. Transfus. Med. 2020, 30, 231. [Google Scholar] [CrossRef]
- Cho, Y.; Park, S.W.; Han, S.-K.; bin Kim, H.; Yeom, S.R. A Case of Methemoglobinemia Successfully Treated with Hyperbaric Oxygenation Monotherapy. J. Emerg. Med. 2017, 53, 685. [Google Scholar] [CrossRef]


{kind=link}
| Author | Cause of Methemoglobinemia | Initial Methemoglobinemia Percentage | Ascorbic Acid Dosing and Treatment | Why Methylene Blue Was Not Utilized |
|---|---|---|---|---|
| Hamzaoui et al. [21] | Dapsone | 13.70% | 1 g of oral ascorbic acid every 12 h for 2 days and a loading dose of 50 g of activated charcoal orally, followed by 25 g every 6 h orally | It was not available |
| Kabir et al. [22] | Dapsone | 17.70% | 10 g of IV ascorbic acid every 6 h for 4 days, and was then switched to oral vitamin C | Unknown glucose-6-phosphate dehydrogenase status |
| Reeves et al. [23] | Rasburicase-induced | 14.50% | 5 g of IV ascorbic acid every 6 h for 3 days | Glucose-6-phosphate dehydrogenase deficiency |
| Sahu et al. [24] | Dapsone | 18.30% | 1 g of IV ascorbic acid every 12 h for 7 days | It was not available |
| De Crem et al. [25] | Primaquine | 33.70% | 1 g of IV ascorbic acid 4 times daily for 7 days | Patient was taking trazodone |
| Topal et al. [26] | Pilocarpine | 24.50% | 3 g of IV ascorbic acid over the course of 24 h | It was not available |
| Powell et al. [27] | Lava lamp poisoning | Over 30% | 5 g of IV ascorbic acid over the course of 24 h | Patient was taking trazodone and duloxetine |
| Asif et al. [28] | Clofazimine | 26.70% | 0.5 g of oral ascorbic acid every 6 h (2000 mg/day) and 600 mg of oral N-acetylcysteine 600 mg every 8 h | It was not available |
| Kilicli et al. [29] | Prilocaine | 14.10% | 3 g of IV ascorbic acid over the course of 24 h | It was not available |
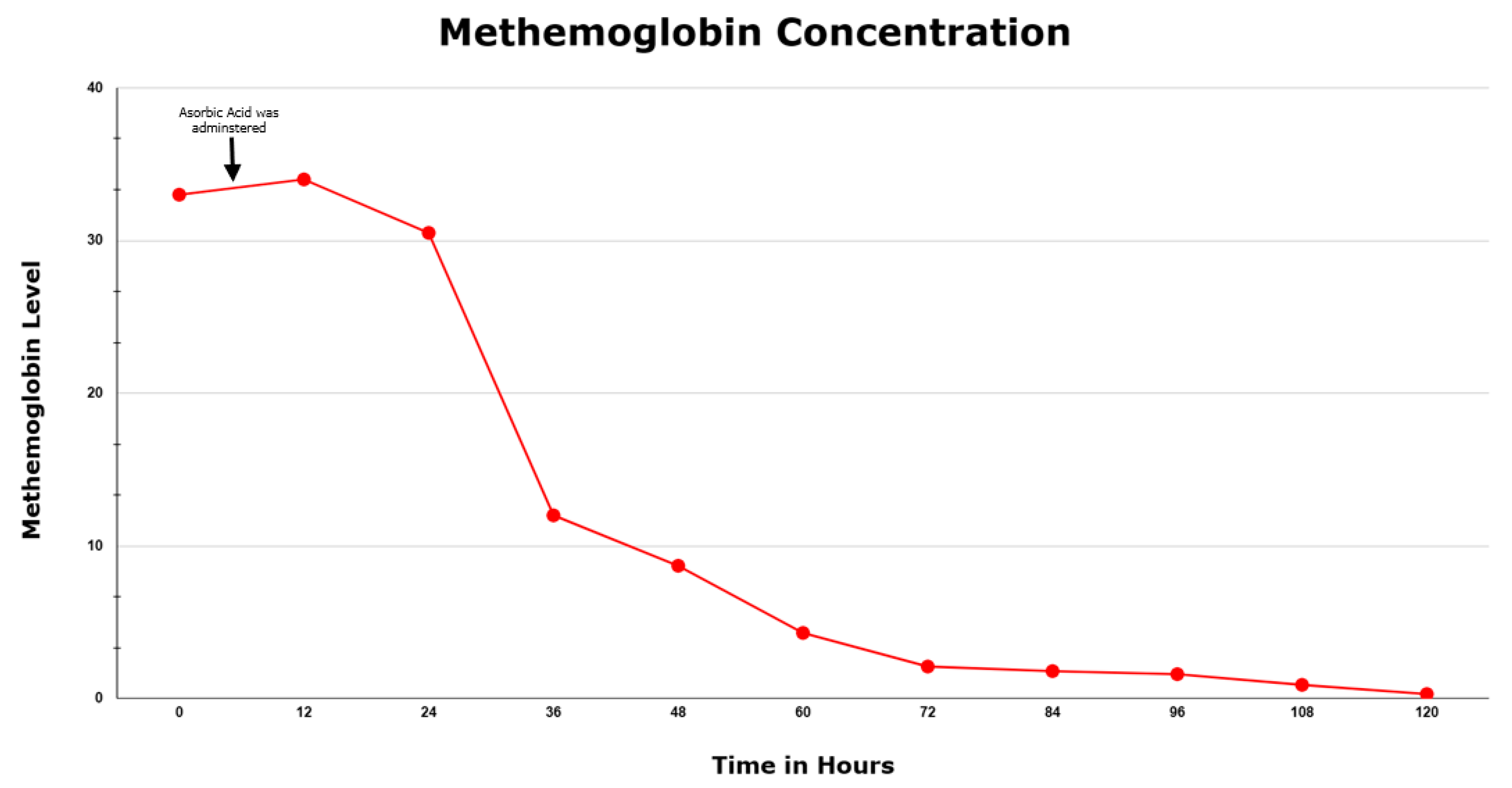
| Menakuru et al. | Phenazopyridine | 33.0% | 5 g of IV ascorbic acid every 12 h for 2.5 days | Patient was taking citalopram |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Menakuru, S.R.; Dhillon, V.S.; Atta, M.; Mann, K.; Salih, A. Phenazopyridine-Induced Methemoglobinemia in a Jehovah’s Witness Treated with High-Dose Ascorbic Acid Due to Methylene Blue Contradictions: A Case Report and Review of the Literature. Hematol. Rep. 2023, 15, 325-330. https://doi.org/10.3390/hematolrep15020034
Menakuru SR, Dhillon VS, Atta M, Mann K, Salih A. Phenazopyridine-Induced Methemoglobinemia in a Jehovah’s Witness Treated with High-Dose Ascorbic Acid Due to Methylene Blue Contradictions: A Case Report and Review of the Literature. Hematology Reports. 2023; 15(2):325-330. https://doi.org/10.3390/hematolrep15020034
Chicago/Turabian StyleMenakuru, Sasmith R., Vijaypal S. Dhillon, Mona Atta, Keeret Mann, and Ahmed Salih. 2023. "Phenazopyridine-Induced Methemoglobinemia in a Jehovah’s Witness Treated with High-Dose Ascorbic Acid Due to Methylene Blue Contradictions: A Case Report and Review of the Literature" Hematology Reports 15, no. 2: 325-330. https://doi.org/10.3390/hematolrep15020034