
Nano-Formulations for Pulmonary Delivery: Past, Present, and Future Perspectives


Abstract
:1. Introduction
2. Fundamental Research on Inhalable Nano-Formulations Is Comprehensively Conducted
- (i)
- Synthesis methods. There are various synthesis methods available for different inhalable nano-formulations, which can be broadly categorized into top–down and bottom–up methods. Top–down methods refer to the decomposition of larger solid particles into smaller nanoparticles by external forces, such as high-pressure homogenization and wet milling. Bottom–up methods refer to the synthesis of nanoparticles from the molecular level by precipitation, crystallization, and the removal of solvents, such as extrusion, solvent evaporation, and antisolvent methods [4,59,60,61,62].
- (ii)
- Structure elucidation. For synthesized nano-formulations, we need to determine the nanoarchitectonics, including the atomic, molecular, nanoscale, and mesoscale structures. Techniques such as ultraviolet spectrum, infrared spectrum, nuclear magnetic resonance spectroscopy, mass spectrometry, X-ray diffraction, and X-ray photoelectron spectroscopy can be utilized [63].
- (iii)
- Size measurement. The size distribution of nano-formulations is commonly studied by nanoparticle size analyzers. The main tests include PDI, size distribution, and autocorrelation function (ACF) curves, to ensure that the size of the prepared nano-formulations meets the inhalation requirements. After nano-formulations have been prepared into forms suitable for use in inhalation devices such as DPIs, nebulizers, and others, it is equally necessary to study their particle size, PDI, and other properties, to ensure that the sprayed droplets or dry powders meet the size requirements for effective lung deposition [45,64,65].
- (iv)
- Shape identification. The shape of nano-formulations is commonly studied using a Transmission Electron Microscope (TEM), a Scanning Electron Microscope (SEM), and an Atomic Force Microscope (AFM). In addition to the static shape, it is vital to study the shape of sprayed droplets or dry powders after administration to observe the corresponding changes. The shape of xenobiotic particles affects the physiological behavior. For instance, elongated or rod-shaped particles are difficult to be phagocytosed by macrophages, while spherical or elliptical particles have a stronger targeting effect on macrophages [66]. If we can better understand the interplay between the particle shape and the cells, it will help us to develop pulmonary drug delivery systems with greater targetability [67].
- (v)
- Drug-carrying capacity. The large specific surface area or accommodation room of nanoparticles allows for the surface adsorption or physical encapsulation of drug molecules, leading to a better drug-carrying capacity compared to formulations with larger particles [68,69]. The drug-carrying capacity of nano-formulations is commonly analyzed by High-Performance Liquid Chromatography (HPLC) or HPLC tandem methods.
- (vi)
- Release behavior. For the release profile of inhalable nano-formulations in the lungs, they are generally expected to endow a rapid and complete one after deposition in the lungs, thus improving bioavailability [70]. The release behavior of nano-formulations is often studied in vitro by simulating the in vivo environment (like stimulating lung fluid), and release curves are drawn for analysis.
- (vii)
- Aerodynamic properties. It is generally believed that the optimal aerodynamic size range for inhalable particles is 1–3 μm, with which a satisfactory lung deposition can be achieved [64]. From this viewpoint, compared with nano-formulations, micron-sized formulations have superior aerodynamic properties, and thus, current studies seek to enlarge the aerodynamic diameter of the nano-formulations through microencapsulation or bulking techniques, without affecting the excellent bioavailability of the nano-formulations. The Next-Generation Impactor (NGI) is commonly used to study the aerodynamic properties of nano-formulations. Via the NGI, parameters such as fine particle dose (FPD), fine particle fraction (FPF), mass median aerodynamic particle diameter (MMAD), and geometric standard deviation (GSD) can be determined as indicators of aerodynamic performance [71,72].
- (viii)
- Toxicity. The toxicity of nano-formulations mainly stems from two aspects, APIs and nanocarriers. In the area of pharmaceutics, nanocarrier toxicity is emphasized. Smaller nanocarriers are difficult to phagocytose by macrophages and are thus retained in the alveoli, which may produce side effects [73]. In addition, the residual organic solvents and metal ions remaining in the formulations may cause inflammatory and other adverse reactions [74,75]. We need to conduct in vitro and in vivo toxicity testing of the nano-formulations, to assess the safety [72]. Interestingly, it is pointed out that the precise targeting of the nano-formulations can prevent the non-specific interactions between nano-formulations and lung cells and thus alleviate local toxicity [76].
- (ix)
- Pharmacokinetics. By improving the pulmonary deposition rate of nano-formulations as well as active targeting modifications, the pharmacokinetics properties may be enhanced [42]. High-Performance Liquid Chromatography–Mass Spectrometry (HPLC-MS) is commonly used for pharmacokinetic-related studies. Inhalable nano-formulations in the lungs should be concerned with the absorption, distribution, metabolism, and excretion processes [37,70].
- (x)
- Pharmacodynamics. The efficacy of nano-formulations can be enhanced by designing and screening the optimal formulation and administration scheme [42]. Pharmacodynamic studies of nano-formulations in pulmonary delivery are conducted in vitro to investigate whether the formulations produce the desired effects on cells (e.g., killing cancer cells, regulating gene expression and production of anti-inflammatory factors, etc.). In vivo, experiments were conducted to investigate whether the formulations could treat animals with lung diseases [28,40,45,49,77].
3. Industrial Translation of Inhalable Nano-Formulations Is Limited
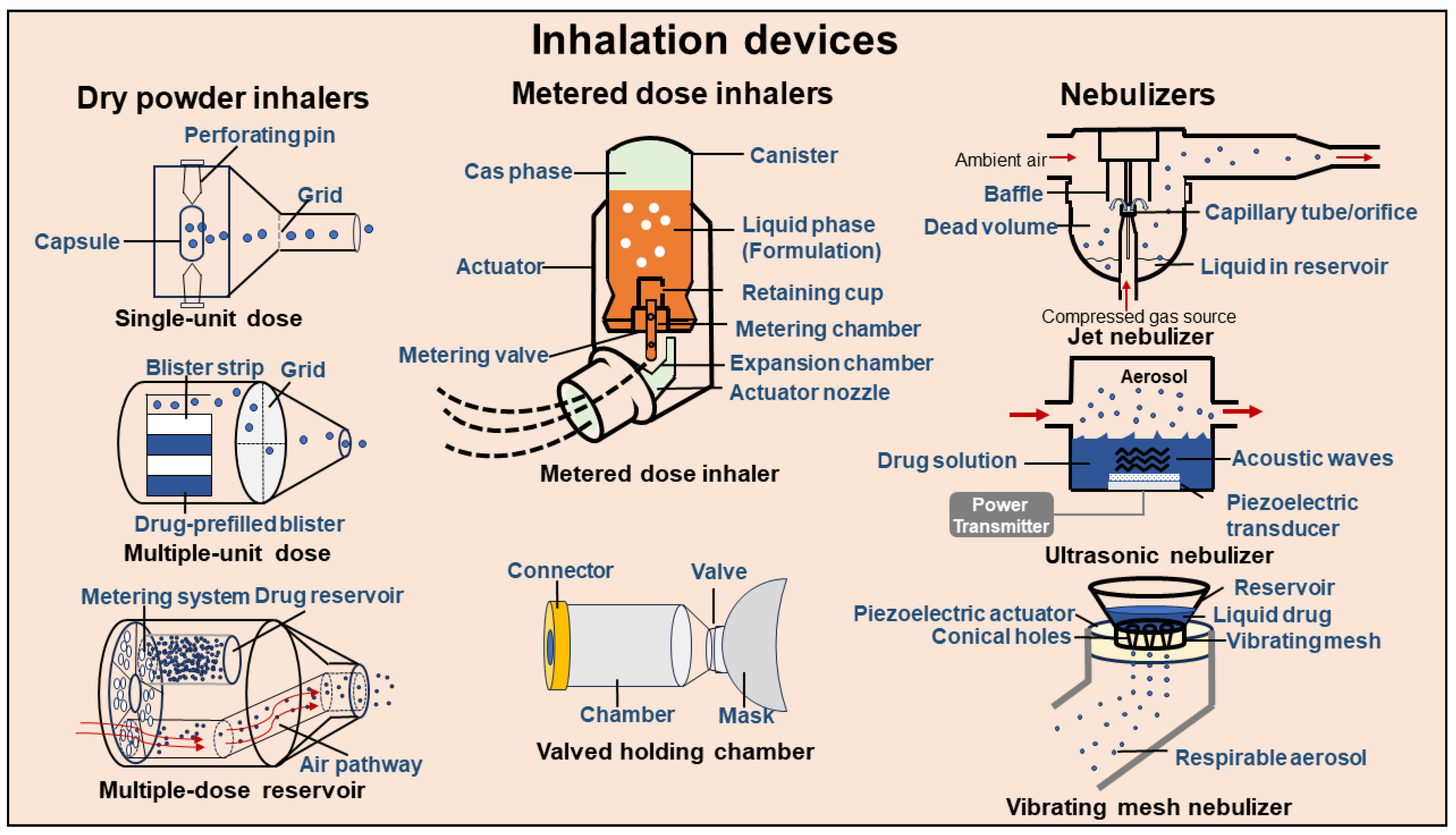
4. Various Inhalation Devices Are Used Clinically
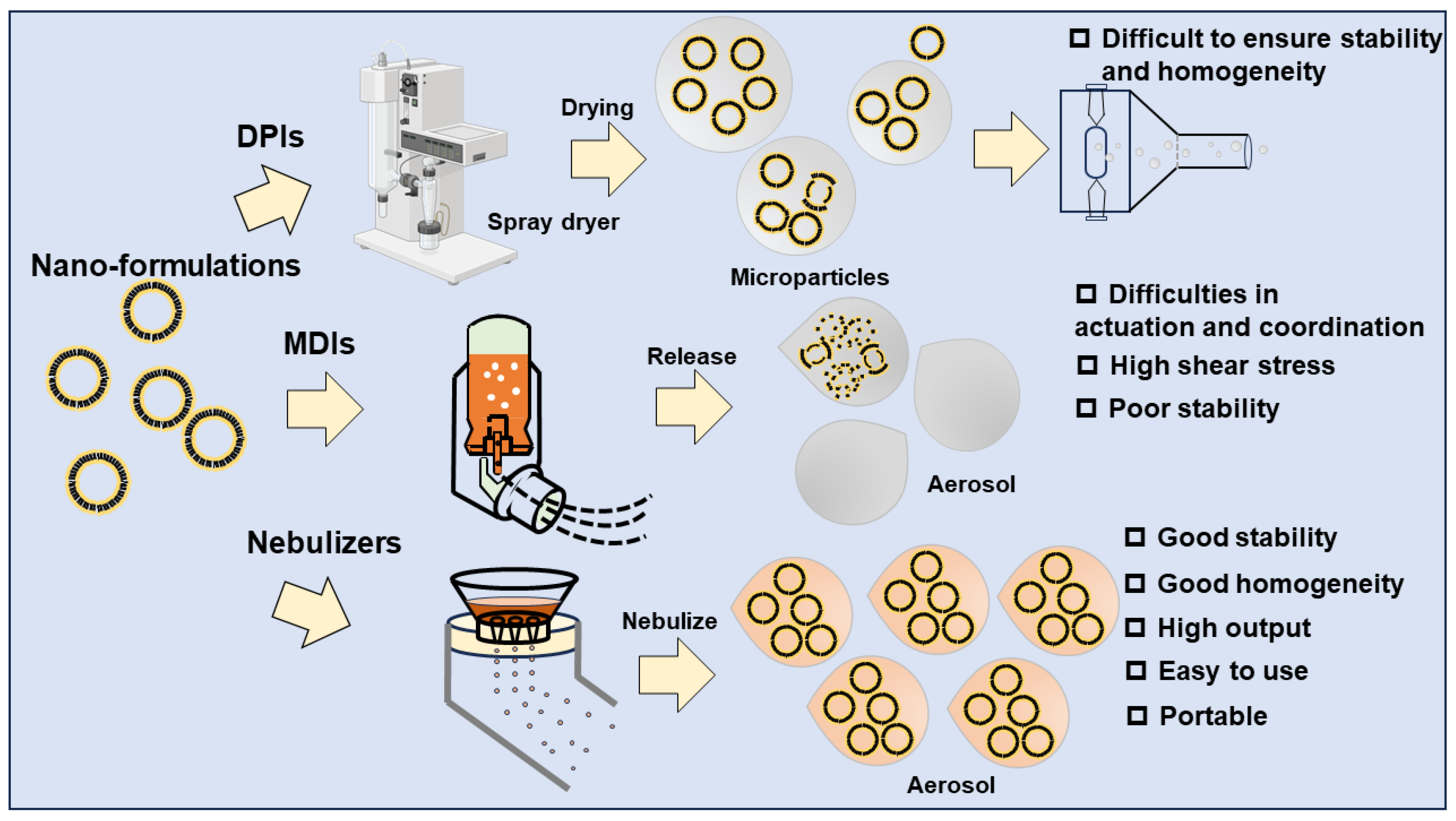
5. Vibrating Mesh Nebulizers Are Suitable for Inhalable Nano-Formulation Delivery
5.1. Status of Research on Using DPIs to Deliver Inhalable Nano-Formulations
5.2. Status of Research on Using MDIs to Deliver Inhalable Nano-Formulations
5.3. Status of Research on Using Nebulizers to Deliver Inhalable Nano-Formulations
5.4. Case Study of ARIKAYCE®
6. The Development of Inhalable Nano-Formulations and Their Nebulizers Is Challenging
7. Conclusions and Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Food and Drug Administration. Guidance for Industry Considering Whether an FDA-Regulated Product Involves the Application of Nanotechnology Contains Nonbinding Recommendations; Food and Drug Administration: Silver Spring, MD, USA, 2014. [Google Scholar]
- Jeevanandam, J.; Chan, Y.S.; Danquah, M.K. Nano-Formulations of Drugs: Recent Developments, Impact and Challenges. Biochimie 2016, 128–129, 99–112. [Google Scholar] [CrossRef] [PubMed]
- Akbarzadeh, A.; Rezaei-Sadabady, R.; Davaran, S.; Joo, S.W.; Zarghami, N.; Hanifehpour, Y.; Samiei, M.; Kouhi, M.; Nejati-Koshki, K. Liposome: Classification, Preparation, and Applications. Nanoscale Res. Lett. 2013, 8, 102. [Google Scholar] [CrossRef] [PubMed]
- Has, C.; Sunthar, P. A Comprehensive Review on Recent Preparation Techniques of Liposomes. J. Liposome Res. 2020, 30, 336–365. [Google Scholar] [CrossRef] [PubMed]
- Jones, M.-C.; Leroux, J.-C. Polymeric Micelles—A New Generation of Colloidal Drug Carriers. Eur. J. Pharm. Biopharm. 1999, 48, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Kwon, G.S. Polymeric Micelles as New Drug Carriers. Adv. Drug Deliv. Rev. 1996, 21, 107–116. [Google Scholar] [CrossRef]
- Singh, Y.; Meher, J.G.; Raval, K.; Khan, F.A.; Chaurasia, M.; Jain, N.K.; Chourasia, M.K. Nanoemulsion: Concepts, Development and Applications in Drug Delivery. J. Control. Release 2017, 252, 28–49. [Google Scholar] [CrossRef]
- Sarker, D. Engineering of Nanoemulsions for Drug Delivery. Curr. Drug Deliv. 2005, 2, 297–310. [Google Scholar] [CrossRef]
- Pardhi, V.P.; Verma, T.; Flora, S.J.S.; Chandasana, H.; Shukla, R. Nanocrystals: An Overview of Fabrication, Characterization and Therapeutic Applications in Drug Delivery. Curr. Pharm. Des. 2018, 24, 5129–5146. [Google Scholar] [CrossRef]
- Shi, J.; Guo, F.; Zheng, A.; Zhang, X.; Sun, J. Progress in the Study of Drug Nanocrystals. Pharmazie 2015, 70, 757–764. [Google Scholar]
- Amreddy, N.; Babu, A.; Muralidharan, R.; Panneerselvam, J.; Srivastava, A.; Ahmed, R.; Mehta, M.; Munshi, A.; Ramesh, R. Recent Advances in Nanoparticle-Based Cancer Drug and Gene Delivery. Adv. Cancer Res. 2018, 137, 115–170. [Google Scholar]
- Singh, R.; Lillard, J.W. Nanoparticle-Based Targeted Drug Delivery. Exp. Mol. Pathol. 2009, 86, 215–223. [Google Scholar] [CrossRef]
- Edis, Z.; Wang, J.; Waqas, M.K.; Ijaz, M.; Ijaz, M. Nanocarriers-Mediated Drug Delivery Systems for Anticancer Agents: An Overview and Perspectives. Int. J. Nanomed. 2021, 16, 1313–1330. [Google Scholar] [CrossRef]
- Pérez-Herrero, E.; Fernández-Medarde, A. Advanced Targeted Therapies in Cancer: Drug Nanocarriers, the Future of Chemotherapy. Eur. J. Pharm. Biopharm. 2015, 93, 52–79. [Google Scholar] [CrossRef]
- Zhou, X.; Hao, Y.; Yuan, L.; Pradhan, S.; Shrestha, K.; Pradhan, O.; Liu, H.; Li, W. Nano-Formulations for Transdermal Drug Delivery: A Review. Chin. Chem. Lett. 2018, 29, 1713–1724. [Google Scholar] [CrossRef]
- Xing, Y.; Lu, P.; Xue, Z.; Liang, C.; Zhang, B.; Kebebe, D.; Liu, H.; Liu, Z. Nano-Strategies for Improving the Bioavailability of Inhaled Pharmaceutical Formulations. Mini-Rev. Med. Chem. 2020, 20, 1258–1271. [Google Scholar] [CrossRef]
- Porche, D.J. Liposomal Doxorubicin (Doxil®). J. Assoc. Nurses AIDS Care 1996, 7, 55–59. [Google Scholar] [CrossRef]
- Caldwell, J.R. Avinza®—24-h Sustained-Release Oral Morphine Therapy. Expert. Opin. Pharmacother. 2004, 5, 469–472. [Google Scholar] [CrossRef]
- Chiechi, L.M. Estrasorb. IDrugs 2004, 7, 860–864. [Google Scholar]
- Mandal, A.; Gote, V.; Pal, D.; Ogundele, A.; Mitra, A.K. Ocular Pharmacokinetics of a Topical Ophthalmic Nanomicellar Solution of Cyclosporine (Cequa®) for Dry Eye Disease. Pharm. Res. 2019, 36, 36. [Google Scholar] [CrossRef]
- Khan, O.; Chaudary, N. The Use of Amikacin Liposome Inhalation Suspension (Arikayce) in the Treatment of Refractory Nontuberculous Mycobacterial Lung Disease in Adults. Drug Des. Devel Ther. 2020, 14, 2287–2294. [Google Scholar] [CrossRef]
- Soriano, J.B.; Abajobir, A.A.; Abate, K.H.; Abera, S.F.; Agrawal, A.; Ahmed, M.B.; Aichour, A.N.; Aichour, I.; Aichour, M.T.E.; Alam, K.; et al. Global, Regional, and National Deaths, Prevalence, Disability-Adjusted Life Years, and Years Lived with Disability for Chronic Obstructive Pulmonary Disease and Asthma, 1990–2015: A Systematic Analysis for the Global Burden of Disease Study 2015. Lancet Respir. Med. 2017, 5, 691–706. [Google Scholar] [CrossRef]
- Forno, E.; Ortega, V.E.; Celedón, J.C. Asthma and Chronic Obstructive Pulmonary Disease. Clin. Chest Med. 2023, 44, 519–530. [Google Scholar] [CrossRef]
- Mims, J.W. Asthma: Definitions and Pathophysiology. Int. Forum Allergy Rhinol. 2015, 5, S2–S6. [Google Scholar] [CrossRef]
- Rabe, K.F.; Watz, H. Chronic Obstructive Pulmonary Disease. Lancet 2017, 389, 1931–1940. [Google Scholar] [CrossRef]
- Wu, F.; Deng, Z.S.; Tian, H.S.; Li, H.Q.; Zhou, Y.M. [Progress in Pre-Chronic Obstructive Pulmonary Disease]. Zhonghua Jie He He Hu Xi Za Zhi 2023, 46, 1028–1034. [Google Scholar] [CrossRef]
- Mao, Y.; Yang, D.; He, J.; Krasna, M.J. Epidemiology of Lung Cancer. Surg. Oncol. Clin. N. Am. 2016, 25, 439–445. [Google Scholar] [CrossRef]
- Nasim, F.; Sabath, B.F.; Eapen, G.A. Lung Cancer. Med. Clin. N. Am. 2019, 103, 463–473. [Google Scholar] [CrossRef]
- Bade, B.C.; Dela Cruz, C.S. Lung Cancer 2020: Epidemiology, Etiology, and Prevention. Clin. Chest Med. 2020, 41, 1–24. [Google Scholar] [CrossRef]
- Oliver, A.L. Lung Cancer: Epidemiology and Screening. Surg. Clin. N. Am. 2022, 102, 335–344. [Google Scholar] [CrossRef]
- Abu Rous, F.; Singhi, E.K.; Sridhar, A.; Faisal, M.S.; Desai, A. Lung Cancer Treatment Advances in 2022. Cancer Investig. 2023, 41, 12–24. [Google Scholar] [CrossRef]
- Thanh Le, T.; Andreadakis, Z.; Kumar, A.; Gómez Román, R.; Tollefsen, S.; Saville, M.; Mayhew, S. The COVID-19 Vaccine Development Landscape. Nat. Rev. Drug Discov. 2020, 19, 305–306. [Google Scholar] [CrossRef]
- Shi, Y.; Wang, G.; Cai, X.; Deng, J.; Zheng, L.; Zhu, H.; Zheng, M.; Yang, B.; Chen, Z. An Overview of COVID-19. J. Zhejiang Univ. Sci. B 2020, 21, 343–360. [Google Scholar] [CrossRef]
- Yang, L.; Liu, S.; Liu, J.; Zhang, Z.; Wan, X.; Huang, B.; Chen, Y.; Zhang, Y. COVID-19: Immunopathogenesis and Immunotherapeutics. Signal Transduct. Target. Ther. 2020, 5, 128. [Google Scholar] [CrossRef]
- Ochani, R.; Asad, A.; Yasmin, F.; Shaikh, S.; Khalid, H.; Batra, S.; Sohail, M.R.; Mahmood, S.F.; Ochani, R.; Hussham Arshad, M.; et al. COVID-19 Pandemic: From Origins to Outcomes. A Comprehensive Review of Viral Pathogenesis, Clinical Manifestations, Diagnostic Evaluation, and Management. Infez. Med. 2021, 29, 20–36. [Google Scholar]
- Yuan, Y.; Jiao, B.; Qu, L.; Yang, D.; Liu, R. The Development of COVID-19 Treatment. Front. Immunol. 2023, 14, 1125246. [Google Scholar] [CrossRef]
- Forest, V.; Pourchez, J. Nano-Delivery to the Lung—By Inhalation or Other Routes and Why Nano When Micro Is Largely Sufficient? Adv. Drug Deliv. Rev. 2022, 183, 114173. [Google Scholar] [CrossRef]
- Zhou, Q.T.; Leung, S.S.Y.; Tang, P.; Parumasivam, T.; Loh, Z.H.; Chan, H.-K. Inhaled Formulations and Pulmonary Drug Delivery Systems for Respiratory Infections. Adv. Drug Deliv. Rev. 2015, 85, 83–99. [Google Scholar] [CrossRef]
- Joshi, K.; Chandra, A.; Jain, K.; Talegaonkar, S. Nanocrystalization: An Emerging Technology to Enhance the Bioavailability of Poorly Soluble Drugs. Pharm. Nanotechnol. 2019, 7, 259–278. [Google Scholar] [CrossRef]
- Akhter, S.; Ahmad, J.; Rizwanullah, M.; Rahman, M.; Zaki Ahmad, M.; Rizvi, M.M.A.; Ahmad, F.J.; Amin, S.; Kamal, M.A. Nanotechnology-Based Inhalation Treatments for Lung Cancer: State of the Art. Nanotechnol. Sci. Appl. 2015, 8, 55–66. [Google Scholar] [CrossRef]
- Ngan, C.L.; Asmawi, A.A. Lipid-Based Pulmonary Delivery System: A Review and Future Considerations of Formulation Strategies and Limitations. Drug Deliv. Transl. Res. 2018, 8, 1527–1544. [Google Scholar] [CrossRef]
- Jin, Z.; Gao, Q.; Wu, K.; Ouyang, J.; Guo, W.; Liang, X.-J. Harnessing Inhaled Nanoparticles to Overcome the Pulmonary Barrier for Respiratory Disease Therapy. Adv. Drug Deliv. Rev. 2023, 202, 115111. [Google Scholar] [CrossRef] [PubMed]
- Wijagkanalan, W.; Kawakami, S.; Takenaga, M.; Igarashi, R.; Yamashita, F.; Hashida, M. Efficient Targeting to Alveolar Macrophages by Intratracheal Administration of Mannosylated Liposomes in Rats. J. Control. Release 2008, 125, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Blanco, E.; Shen, H.; Ferrari, M. Principles of Nanoparticle Design for Overcoming Biological Barriers to Drug Delivery. Nat. Biotechnol. 2015, 33, 941–951. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.C.; Pulliam, B.L.; Edwards, D.A. Nanoparticles for Drug Delivery to the Lungs. Trends Biotechnol. 2007, 25, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Mura, S.; Nicolas, J.; Couvreur, P. Stimuli-Responsive Nanocarriers for Drug Delivery. Nat. Mater. 2013, 12, 991–1003. [Google Scholar] [CrossRef]
- Yang, Y.; Liu, X.; Ma, W.; Xu, Q.; Chen, G.; Wang, Y.; Xiao, H.; Li, N.; Liang, X.-J.; Yu, M.; et al. Light-Activatable Liposomes for Repetitive on-Demand Drug Release and Immunopotentiation in Hypoxic Tumor Therapy. Biomaterials 2021, 265, 120456. [Google Scholar] [CrossRef] [PubMed]
- Horejs, C. Nebulized Lipid Nanoparticles. Nat. Rev. Mater. 2021, 6, 1077. [Google Scholar] [CrossRef]
- Zarogoulidis, P.; Chatzaki, E.; Porpodis, K.; Domvri, K.; Hohenforst-Schmidt, W.; Goldberg, E.P.; Karamanos, N.; Zarogoulidis, K. Inhaled Chemotherapy in Lung Cancer: Future Concept of Nanomedicine. Int. J. Nanomed. 2012, 7, 1551–1572. [Google Scholar] [CrossRef]
- Kamaly, N.; Yameen, B.; Wu, J.; Farokhzad, O.C. Degradable Controlled-Release Polymers and Polymeric Nanoparticles: Mechanisms of Controlling Drug Release. Chem. Rev. 2016, 116, 2602–2663. [Google Scholar] [CrossRef]
- Miyata, K.; Christie, R.J.; Kataoka, K. Polymeric Micelles for Nano-Scale Drug Delivery. React. Funct. Polym. 2011, 71, 227–234. [Google Scholar] [CrossRef]
- Videira, M.; Almeida, A.J.; Fabra, À. Preclinical Evaluation of a Pulmonary Delivered Paclitaxel-Loaded Lipid Nanocarrier Antitumor Effect. Nanomedicine 2012, 8, 1208–1215. [Google Scholar] [CrossRef] [PubMed]
- Bobo, D.; Robinson, K.J.; Islam, J.; Thurecht, K.J.; Corrie, S.R. Nanoparticle-Based Medicines: A Review of FDA-Approved Materials and Clinical Trials to Date. Pharm. Res. 2016, 33, 2373–2387. [Google Scholar] [CrossRef] [PubMed]
- Pápay, Z.E.; Kósa, A.; Böddi, B.; Merchant, Z.; Saleem, I.Y.; Zariwala, M.G.; Klebovich, I.; Somavarapu, S.; Antal, I. Study on the Pulmonary Delivery System of Apigenin-Loaded Albumin Nanocarriers with Antioxidant Activity. J. Aerosol Med. Pulm. Drug Deliv. 2017, 30, 274–288. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-H.; Tsai, C.-Y.; Huang, P.-Y.; Chang, M.-Y.; Cheng, P.-C.; Chou, C.-H.; Chen, D.-H.; Wang, C.-R.; Shiau, A.-L.; Wu, C.-L. Methotrexate Conjugated to Gold Nanoparticles Inhibits Tumor Growth in a Syngeneic Lung Tumor Model. Mol. Pharm. 2007, 4, 713–722. [Google Scholar] [CrossRef] [PubMed]
- Quarta, E.; Degli Esposti, L.; Bettini, R.; Sonvico, F.; Catalucci, D.; Iafisco, M.; De Luca, C.; Trevisi, G.; Colombo, P.; Rossi, A.; et al. Dry Powder Inhalation Technology for Heart Targeting Applied to Calcium Phosphate Nanoparticles Loaded with Active Substances. J. Drug Deliv. Sci. Technol. 2022, 76, 103719. [Google Scholar] [CrossRef]
- Dash, P.; Piras, A.M.; Dash, M. Cell Membrane Coated Nanocarriers—An Efficient Biomimetic Platform for Targeted Therapy. J. Control. Release 2020, 327, 546–570. [Google Scholar] [CrossRef] [PubMed]
- Bunggulawa, E.J.; Wang, W.; Yin, T.; Wang, N.; Durkan, C.; Wang, Y.; Wang, G. Recent Advancements in the Use of Exosomes as Drug Delivery Systems. J. Nanobiotechnology 2018, 16, 81. [Google Scholar] [CrossRef]
- Taratula, O.; Kuzmov, A.; Shah, M.; Garbuzenko, O.B.; Minko, T. Nanostructured Lipid Carriers as Multifunctional Nanomedicine Platform for Pulmonary Co-Delivery of Anticancer Drugs and SiRNA. J. Control. Release 2013, 171, 349–357. [Google Scholar] [CrossRef]
- Shah, S.; Dhawan, V.; Holm, R.; Nagarsenker, M.S.; Perrie, Y. Liposomes: Advancements and Innovation in the Manufacturing Process. Adv. Drug Deliv. Rev. 2020, 154–155, 102–122. [Google Scholar] [CrossRef]
- Sabjan, K.B.; Munawar, S.M.; Rajendiran, D.; Vinoji, S.K.; Kasinathan, K. Nanoemulsion as Oral Drug Delivery—A Review. Curr. Drug Res. Rev. 2020, 12, 4–15. [Google Scholar] [CrossRef]
- Zhang, J.; Wu, L.; Chan, H.-K.; Watanabe, W. Formation, Characterization, and Fate of Inhaled Drug Nanoparticles. Adv. Drug Deliv. Rev. 2011, 63, 441–455. [Google Scholar] [CrossRef] [PubMed]
- Negi, L.M.; Jaggi, M.; Talegaonkar, S. Development of Protocol for Screening the Formulation Components and the Assessment of Common Quality Problems of Nano-Structured Lipid Carriers. Int. J. Pharm. 2014, 461, 403–410. [Google Scholar] [CrossRef]
- Lavorini, F.; Buttini, F.; Usmani, O.S. 100 Years of Drug Delivery to the Lungs. Concepts Princ. Pharmacol. 2019, 260, 143–159. [Google Scholar]
- Wang, W.; Huang, Z.; Li, Y.; Wang, W.; Shi, J.; Fu, F.; Huang, Y.; Pan, X.; Wu, C. Impact of Particle Size and PH on Protein Corona Formation of Solid Lipid Nanoparticles: A Proof-of-Concept Study. Acta Pharm. Sin. B 2021, 11, 1030–1046. [Google Scholar] [CrossRef] [PubMed]
- Champion, J.A.; Mitragotri, S. Shape Induced Inhibition of Phagocytosis of Polymer Particles. Pharm. Res. 2009, 26, 244–249. [Google Scholar] [CrossRef]
- Truong, N.P.; Whittaker, M.R.; Mak, C.W.; Davis, T.P. The Importance of Nanoparticle Shape in Cancer Drug Delivery. Expert Opin. Drug Deliv. 2015, 12, 129–142. [Google Scholar] [CrossRef] [PubMed]
- Bailey, M.M.; Berkland, C.J. Nanoparticle Formulations in Pulmonary Drug Delivery. Med. Res. Rev. 2009, 29, 196–212. [Google Scholar] [CrossRef]
- Loira-Pastoriza, C.; Todoroff, J.; Vanbever, R. Delivery Strategies for Sustained Drug Release in the Lungs. Adv. Drug Deliv. Rev. 2014, 75, 81–91. [Google Scholar] [CrossRef]
- Ibarra-Sánchez, L.Á.; Gámez-Méndez, A.; Martínez-Ruiz, M.; Nájera-Martínez, E.F.; Morales-Flores, B.A.; Melchor-Martínez, E.M.; Sosa-Hernández, J.E.; Parra-Saldívar, R.; Iqbal, H.M.N. Nanostructures for Drug Delivery in Respiratory Diseases Therapeutics: Revision of Current Trends and Its Comparative Analysis. J. Drug Deliv. Sci. Technol. 2022, 70, 103219. [Google Scholar] [CrossRef]
- Harush-Frenkel, O.; Bivas-Benita, M.; Nassar, T.; Springer, C.; Sherman, Y.; Avital, A.; Altschuler, Y.; Borlak, J.; Benita, S. A Safety and Tolerability Study of Differently-Charged Nanoparticles for Local Pulmonary Drug Delivery. Toxicol. Appl. Pharmacol. 2010, 246, 83–90. [Google Scholar] [CrossRef]
- Keil, T.W.M.; Feldmann, D.P.; Costabile, G.; Zhong, Q.; da Rocha, S.; Merkel, O.M. Characterization of Spray Dried Powders with Nucleic Acid-Containing PEI Nanoparticles. Eur. J. Pharm. Biopharm. 2019, 143, 61–69. [Google Scholar] [CrossRef] [PubMed]
- Mansour, H.M.; Rhee, Y.S.; Wu, X. Nanomedicine in Pulmonary Delivery. Int. J. Nanomed. 2009, 4, 299–319. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, S.K.; Panyam, J.; Prabha, S.; Labhasetwar, V. Residual Polyvinyl Alcohol Associated with Poly (d,l-Lactide-Co-Glycolide) Nanoparticles Affects Their Physical Properties and Cellular Uptake. J. Control. Release 2002, 82, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Cho, W.-S.; Duffin, R.; Poland, C.A.; Duschl, A.; Oostingh, G.J.; MacNee, W.; Bradley, M.; Megson, I.L.; Donaldson, K. Differential Pro-Inflammatory Effects of Metal Oxide Nanoparticles and Their Soluble Ions In Vitro and In Vivo; Zinc and Copper Nanoparticles, but Not Their Ions, Recruit Eosinophils to the Lungs. Nanotoxicology 2012, 6, 22–35. [Google Scholar] [CrossRef] [PubMed]
- Kaminskas, L.M.; McLeod, V.M.; Ryan, G.M.; Kelly, B.D.; Haynes, J.M.; Williamson, M.; Thienthong, N.; Owen, D.J.; Porter, C.J.H. Pulmonary Administration of a Doxorubicin-Conjugated Dendrimer Enhances Drug Exposure to Lung Metastases and Improves Cancer Therapy. J. Control. Release 2014, 183, 18–26. [Google Scholar] [CrossRef]
- Couvreur, P. Nanoparticles in Drug Delivery: Past, Present and Future. Adv. Drug Deliv. Rev. 2013, 65, 21–23. [Google Scholar] [CrossRef]
- Bilton, D.; Fajac, I.; Pressler, T.; Clancy, J.P.; Sands, D.; Minic, P.; Cipolli, M.; Galeva, I.; Solé, A.; Quittner, A.L.; et al. Long-Term Amikacin Liposome Inhalation Suspension in Cystic Fibrosis Patients with Chronic P. Aeruginosa Infection. J. Cyst. Fibros. 2021, 20, 1010–1017. [Google Scholar] [CrossRef]
- Winthrop, K.L.; Flume, P.A.; Thomson, R.; Mange, K.C.; Yuen, D.W.; Ciesielska, M.; Morimoto, K.; Ruoss, S.J.; Codecasa, L.R.; Yim, J.-J.; et al. Amikacin Liposome Inhalation Suspension for Mycobacterium Avium Complex Lung Disease: A 12-Month Open-Label Extension Clinical Trial. Ann. Am. Thorac. Soc. 2021, 18, 1147–1157. [Google Scholar] [CrossRef]
- Dorkin, H.L.; Staab, D.; Operschall, E.; Alder, J.; Criollo, M. Ciprofloxacin DPI: A Randomised, Placebo-Controlled, Phase IIb Efficacy and Safety Study on Cystic Fibrosis. BMJ Open Respir. Res. 2015, 2, e000100. [Google Scholar] [CrossRef]
- Li, M.; Zhou, H.; Yang, C.; Wu, Y.; Zhou, X.; Liu, H.; Wang, Y. Bacterial Outer Membrane Vesicles as a Platform for Biomedical Applications: An Update. J. Control. Release 2020, 323, 253–268. [Google Scholar] [CrossRef]
- Balanag, V.M.; Yunus, F.; Yang, P.-C.; Jorup, C. Efficacy and Safety of Budesonide/Formoterol Compared with Salbutamol in the Treatment of Acute Asthma. Pulm. Pharmacol. Ther. 2006, 19, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Ball, D.J.; Hirst, P.H.; Newman, S.P.; Sonet, B.; Streel, B.; Vanderbist, F. Deposition and Pharmacokinetics of Budesonide from the Miat Monodose Inhaler, a Simple Dry Powder Device. Int. J. Pharm. 2002, 245, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Alton, E.W.F.W.; Armstrong, D.K.; Ashby, D.; Bayfield, K.J.; Bilton, D.; Bloomfield, E.V.; Boyd, A.C.; Brand, J.; Buchan, R.; Calcedo, R.; et al. Repeated Nebulisation of Non-Viral CFTR Gene Therapy in Patients with Cystic Fibrosis: A Randomised, Double-Blind, Placebo-Controlled, Phase 2b Trial. Lancet Respir. Med. 2015, 3, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Miah, K.M.; Hyde, S.C.; Gill, D.R. Emerging Gene Therapies for Cystic Fibrosis. Expert. Rev. Respir. Med. 2019, 13, 709–725. [Google Scholar] [CrossRef] [PubMed]
- Matschiner, G.; Fitzgerald, M.F.; Moebius, U.; Hohlbaum, A.M.; Gille, H.; Jensen, K.; Kirchfeld, K.; Rattenstetter, B.; Laforge, A.; Bel Aiba, R.S.; et al. Elarekibep (PRS-060/AZD1402), a New Class of Inhaled Anticalin Medicine Targeting IL-4Ra for Type 2 Endotype Asthma. J. Allergy Clin. Immunol. 2023, 151, 966–975. [Google Scholar] [CrossRef] [PubMed]
- Haughney, J.; Price, D.; Barnes, N.C.; Virchow, J.C.; Roche, N.; Chrystyn, H. Choosing Inhaler Devices for People with Asthma: Current Knowledge and Outstanding Research Needs. Respir. Med. 2010, 104, 1237–1245. [Google Scholar] [CrossRef] [PubMed]
- Virchow, J.C.; Crompton, G.K.; Dal Negro, R.; Pedersen, S.; Magnan, A.; Seidenberg, J.; Barnes, P.J. Importance of Inhaler Devices in the Management of Airway Disease. Respir. Med. 2008, 102, 10–19. [Google Scholar] [CrossRef]
- Bivolaru, S.; Constantin, A.; Vlase, C.M.; Gutu, C. COPD Patients’ Behaviour When Involved in the Choice of Inhaler Device. Healthcare 2023, 11, 1606. [Google Scholar] [CrossRef]
- Zhou, Q.T.; Tang, P.; Leung, S.S.Y.; Chan, J.G.Y.; Chan, H.-K. Emerging Inhalation Aerosol Devices and Strategies: Where Are We Headed? Adv. Drug Deliv. Rev. 2014, 75, 3–17. [Google Scholar] [CrossRef]
- Saha, T.; Quiñones-Mateu, M.E.; Das, S.C. Inhaled Therapy for COVID-19: Considerations of Drugs, Formulations and Devices. Int. J. Pharm. 2022, 624, 122042. [Google Scholar] [CrossRef]
- Ahookhosh, K.; Saidi, M.; Mohammadpourfard, M.; Aminfar, H.; Hamishehkar, H.; Farnoud, A.; Schmid, O. Flow Structure and Particle Deposition Analyses for Optimization of a Pressurized Metered Dose Inhaler (PMDI) in a Model of Tracheobronchial Airway. Eur. J. Pharm. Sci. 2021, 164, 105911. [Google Scholar] [CrossRef] [PubMed]
- Hejduk, A.; Urbańska, A.; Osiński, A.; Łukaszewicz, P.; Domański, M.; Sosnowski, T.R. Technical Challenges in Obtaining an Optimized Powder/DPI Combination for Inhalation Delivery of a Bi-Component Generic Drug. J. Drug Deliv. Sci. Technol. 2018, 44, 406–414. [Google Scholar] [CrossRef]
- Thalberg, K.; Ahmadi, R.; Stuckel, J.; Elfman, P.; Svensson, M. The Match between Adhesive Mixture Powder Formulations for Inhalation and the Inhaler Device. Eur. J. Pharm. Sci. 2023, 186, 106457. [Google Scholar] [CrossRef] [PubMed]
- Shahin, H.I.; Chablani, L. A Comprehensive Overview of Dry Powder Inhalers for Pulmonary Drug Delivery: Challenges, Advances, Optimization Techniques, and Applications. J. Drug Deliv. Sci. Technol. 2023, 84, 104553. [Google Scholar] [CrossRef]
- Smyth, H.D.C. The Influence of Formulation Variables on the Performance of Alternative Propellant-Driven Metered Dose Inhalers. Adv. Drug Deliv. Rev. 2003, 55, 807–828. [Google Scholar] [CrossRef] [PubMed]
- Csonka, P.; Lehtimäki, L. Valved Holding Chamber Drug Delivery Is Dependent on Breathing Pattern and Device Design. ERJ Open Res. 2019, 5, 00158–02018. [Google Scholar] [CrossRef] [PubMed]
- Hatley, R.H.M.; von Hollen, D.; Sandell, D.; Slator, L. In Vitro Characterization of the OptiChamber Diamond Valved Holding Chamber. J. Aerosol Med. Pulm. Drug Deliv. 2014, 27, S-24–S-36. [Google Scholar] [CrossRef]
- Xu, Z.; Hsu, W.; von Hollen, D.; Viswanath, A.; Nikander, K.; Dalby, R. Methodology for the In Vitro Evaluation of the Delivery Efficiency from Valved Holding Chambers with Facemasks. J. Aerosol Med. Pulm. Drug Deliv. 2014, 27, S-44–S-54. [Google Scholar] [CrossRef]
- Hickey, A.J. Emerging Trends in Inhaled Drug Delivery. Adv. Drug Deliv. Rev. 2020, 157, 63–70. [Google Scholar] [CrossRef]
- Myrdal, P.B.; Sheth, P.; Stein, S.W. Advances in Metered Dose Inhaler Technology: Formulation Development. AAPS PharmSciTech 2014, 15, 434–455. [Google Scholar] [CrossRef]
- Frijlink, H.W.; De Boer, A.H. Dry Powder Inhalers for Pulmonary Drug Delivery. Expert Opin. Drug Deliv. 2004, 1, 67–86. [Google Scholar] [CrossRef] [PubMed]
- Ashurst, I.; Malton, A.; Prime, D.; Sumby, B. Latest Advances in the Development of Dry Powder Inhalers. Pharm. Sci. Technol. Today 2000, 3, 246–256. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Ma, Y.; Zhang, L.; Zhu, J.; Jin, F. The Development of a Novel Dry Powder Inhaler. Int. J. Pharm. 2012, 431, 45–52. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.R.; Finlay, W.H. Nebulizers for Drug Delivery to the Lungs. Expert Opin. Drug Deliv. 2015, 12, 889–900. [Google Scholar] [CrossRef] [PubMed]
- Ari, A. Jet, Ultrasonic, and Mesh Nebulizers: An Evaluation of Nebulizers for Better Clinical Outcomes. Eurasian J. Pulmonol. 2014, 16, 1–7. [Google Scholar] [CrossRef]
- Rubin, B.K.; Williams, R.W. Emerging Aerosol Drug Delivery Strategies: From Bench to Clinic. Adv. Drug Deliv. Rev. 2014, 75, 141–148. [Google Scholar] [CrossRef] [PubMed]
- Smithmaitrie, P.; Tangudomkit, K. Multiphysics Finite Element Modeling and Validation of Transient Aerosol Generation in an Ultrasonic Nebulizer Drug Delivery Device. J. Aerosol Sci. 2018, 126, 110–121. [Google Scholar] [CrossRef]
- Yeo, L.Y.; Friend, J.R.; McIntosh, M.P.; Meeusen, E.N.; Morton, D.A. Ultrasonic Nebulization Platforms for Pulmonary Drug Delivery. Expert Opin. Drug Deliv. 2010, 7, 663–679. [Google Scholar] [CrossRef]
- Huang, Y.-Y.; Wang, C.-H. Pulmonary Delivery of Insulin by Liposomal Carriers. J. Control. Release 2006, 113, 9–14. [Google Scholar] [CrossRef]
- Sanchis, J.; Corrigan, C.; Levy, M.L.; Viejo, J.L. Inhaler Devices—From Theory to Practice. Respir. Med. 2013, 107, 495–502. [Google Scholar] [CrossRef]
- de Pablo, E.; Fernández-García, R.; Ballesteros, M.P.; Torrado, J.J.; Serrano, D.R. Nebulised Antibiotherapy: Conventional versus Nanotechnology-Based Approaches, Is Targeting at a Nano Scale a Difficult Subject? Ann. Transl. Med. 2017, 5, 448. [Google Scholar] [CrossRef] [PubMed]
- Fossat, P.; Ichchou, M.; Bareille, O. Analytical Model of the Dynamic Behavior of a Vibrating Mesh Nebulizer for Optimal Atomization Efficiency. Sens. Actuators A Phys. 2022, 343, 113646. [Google Scholar] [CrossRef]
- Pitance, L.; Vecellio, L.; Leal, T.; Reychler, G.; Reychler, H.; Liistro, G. Delivery Efficacy of a Vibrating Mesh Nebulizer and a Jet Nebulizer under Different Configurations. J. Aerosol Med. Pulm. Drug Deliv. 2010, 23, 389–396. [Google Scholar] [CrossRef] [PubMed]
- Zhang, G.; David, A.; Wiedmann, T.S. Performance of the Vibrating Membrane Aerosol Generation Device: Aeroneb Micropump Nebulizer TM. J. Aerosol Med. 2007, 20, 408–416. [Google Scholar] [CrossRef] [PubMed]
- Beck-Broichsitter, M.; Knuedeler, M.-C.; Oesterheld, N.; Seeger, W.; Schmehl, T. Boosting the Aerodynamic Properties of Vibrating-Mesh Nebulized Polymeric Nanosuspensions. Int. J. Pharm. 2014, 459, 23–29. [Google Scholar] [CrossRef]
- Dailey, L.A.; Schmehl, T.; Gessler, T.; Wittmar, M.; Grimminger, F.; Seeger, W.; Kissel, T. Nebulization of Biodegradable Nanoparticles: Impact of Nebulizer Technology and Nanoparticle Characteristics on Aerosol Features. J. Control. Release 2003, 86, 131–144. [Google Scholar] [CrossRef]
- Beck-Broichsitter, M.; Kleimann, P.; Gessler, T.; Seeger, W.; Kissel, T.; Schmehl, T. Nebulization Performance of Biodegradable Sildenafil-Loaded Nanoparticles Using the Aeroneb® Pro: Formulation Aspects and Nanoparticle Stability to Nebulization. Int. J. Pharm. 2012, 422, 398–408. [Google Scholar] [CrossRef]
- Chan, H.W.; Chow, S.; Zhang, X.; Zhao, Y.; Tong, H.H.Y.; Chow, S.F. Inhalable Nanoparticle-Based Dry Powder Formulations for Respiratory Diseases: Challenges and Strategies for Translational Research. AAPS PharmSciTech 2023, 24, 98. [Google Scholar] [CrossRef]
- Khatib, I.; Khanal, D.; Ruan, J.; Cipolla, D.; Dayton, F.; Blanchard, J.D.; Chan, H.-K. Ciprofloxacin Nanocrystals Liposomal Powders for Controlled Drug Release via Inhalation. Int. J. Pharm. 2019, 566, 641–651. [Google Scholar] [CrossRef]
- Li, Z.; Perkins, W.; Cipolla, D. Robustness of Aerosol Delivery of Amikacin Liposome Inhalation Suspension Using the EFlow® Technology. Eur. J. Pharm. Biopharm. 2021, 166, 10–18. [Google Scholar] [CrossRef]
- Vass, P.; Démuth, B.; Hirsch, E.; Nagy, B.; Andersen, S.K.; Vigh, T.; Verreck, G.; Csontos, I.; Nagy, Z.K.; Marosi, G. Drying Technology Strategies for Colon-Targeted Oral Delivery of Biopharmaceuticals. J. Control. Release 2019, 296, 162–178. [Google Scholar] [CrossRef] [PubMed]
- Liao, Q.; Yip, L.; Chow, M.Y.T.; Chow, S.F.; Chan, H.-K.; Kwok, P.C.L.; Lam, J.K.W. Porous and Highly Dispersible Voriconazole Dry Powders Produced by Spray Freeze Drying for Pulmonary Delivery with Efficient Lung Deposition. Int. J. Pharm. 2019, 560, 144–154. [Google Scholar] [CrossRef] [PubMed]
- Ingvarsson, P.T.; Yang, M.; Nielsen, H.M.; Rantanen, J.; Foged, C. Stabilization of Liposomes during Drying. Expert Opin. Drug Deliv. 2011, 8, 375–388. [Google Scholar] [CrossRef] [PubMed]
- Zaibudeen, A.W.; Bandyopadhyay, R. Combined Effects of Nanoparticle Size, and Nanoparticle and Surfactant Concentrations on the Evaporative Kinetics, Dried Morphologies, and Plasmonic Property of Gold Colloidal Dispersion Droplets. Nanotechnology 2023, 34, 295601. [Google Scholar] [CrossRef] [PubMed]
- Wan, K.Y.; Weng, J.; Wong, S.N.; Kwok, P.C.L.; Chow, S.F.; Chow, A.H.L. Converting Nanosuspension into Inhalable and Redispersible Nanoparticles by Combined In-Situ Thermal Gelation and Spray Drying. Eur. J. Pharm. Biopharm. 2020, 149, 238–247. [Google Scholar] [CrossRef]
- Arpagaus, C.; Collenberg, A.; Rütti, D.; Assadpour, E.; Jafari, S.M. Nano Spray Drying for Encapsulation of Pharmaceuticals. Int. J. Pharm. 2018, 546, 194–214. [Google Scholar] [CrossRef]
- Elmowafy, E.; Osman, R.; Ishak, R.A.H. Polymer-Based Novel Lung Targeted Delivery Systems. Curr. Pharm. Des. 2017, 23, 373–392. [Google Scholar] [CrossRef]
- Ruge, C.A.; Bohr, A.; Beck-Broichsitter, M.; Nicolas, V.; Tsapis, N.; Fattal, E. Disintegration of Nano-Embedded Microparticles after Deposition on Mucus: A Mechanistic Study. Colloids Surf. B Biointerfaces 2016, 139, 219–227. [Google Scholar] [CrossRef]
- Torge, A.; Grützmacher, P.; Mücklich, F.; Schneider, M. The Influence of Mannitol on Morphology and Disintegration of Spray-Dried Nano-Embedded Microparticles. Eur. J. Pharm. Sci. 2017, 104, 171–179. [Google Scholar] [CrossRef]
- Anton, N.; Jakhmola, A.; Vandamme, T.F. Trojan Microparticles for Drug Delivery. Pharmaceutics 2012, 4, 1–25. [Google Scholar] [CrossRef]
- Cheow, W.S.; Ng, M.L.L.; Kho, K.; Hadinoto, K. Spray-Freeze-Drying Production of Thermally Sensitive Polymeric Nanoparticle Aggregates for Inhaled Drug Delivery: Effect of Freeze-Drying Adjuvants. Int. J. Pharm. 2011, 404, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.W.; Lee, H.W.; Chow, S.; Lam, D.C.L.; Chow, S.F. Integrated Continuous Manufacturing of Inhalable Remdesivir Nanoagglomerate Dry Powders: Design, Optimization and Therapeutic Potential for Respiratory Viral Infections. Int. J. Pharm. 2023, 644, 123303. [Google Scholar] [CrossRef] [PubMed]
- Tsapis, N.; Bennett, D.; Jackson, B.; Weitz, D.A.; Edwards, D.A. Trojan Particles: Large Porous Carriers of Nanoparticles for Drug Delivery. Proc. Natl. Acad. Sci. USA 2002, 99, 12001–12005. [Google Scholar] [CrossRef] [PubMed]
- Hoppentocht, M.; Hagedoorn, P.; Frijlink, H.W.; de Boer, A.H. Technological and Practical Challenges of Dry Powder Inhalers and Formulations. Adv. Drug Deliv. Rev. 2014, 75, 18–31. [Google Scholar] [CrossRef] [PubMed]
- Costa, C.; Nobre, B.; Matos, A.S.; Silva, A.S.; Casimiro, T.; Corvo, M.L.; Aguiar-Ricardo, A. Inhalable Hydrophilic Molecule-Loaded Liposomal Dry Powder Formulations Using Supercritical CO2—Assisted Spray-Drying. J. CO2 Util. 2021, 53, 101709. [Google Scholar] [CrossRef]
- Kumar, R.; Mehta, P.; Shankar, K.R.; Rajora, M.A.K.; Mishra, Y.K.; Mostafavi, E.; Kaushik, A. Nanotechnology-Assisted Metered-Dose Inhalers (MDIs) for High-Performance Pulmonary Drug Delivery Applications. Pharm. Res. 2022, 39, 2831–2855. [Google Scholar] [CrossRef] [PubMed]
- Metz, J. Safety Assessment of Excipients (SAFE) for Orally Inhaled Drug Products. ALTEX 2020, 37, 275–286. [Google Scholar] [CrossRef]
- Chiang, P.-C.; Alsup, J.W.; Lai, Y.; Hu, Y.; Heyde, B.R.; Tung, D. Evaluation of Aerosol Delivery of Nanosuspension for Pre-Clinical Pulmonary Drug Delivery. Nanoscale Res. Lett. 2009, 4, 254. [Google Scholar] [CrossRef]
- Wiedmann, T.S.; DeCastro, L.; Wood, R.W. Nebulization of NanoCrystals(TM): Production of a Respirable Solid-in-Liquid-in-Air Colloidal Dispersion. Pharm. Res. 1997, 14, 112–116. [Google Scholar] [CrossRef]
- Patlolla, R.R.; Chougule, M.; Patel, A.R.; Jackson, T.; Tata, P.N.V.; Singh, M. Formulation, Characterization and Pulmonary Deposition of Nebulized Celecoxib Encapsulated Nanostructured Lipid Carriers. J. Control. Release 2010, 144, 233–241. [Google Scholar] [CrossRef]
- Meng, Q.-F.; Tai, W.; Tian, M.; Zhuang, X.; Pan, Y.; Lai, J.; Xu, Y.; Xu, Z.; Li, M.; Zhao, G.; et al. Inhalation Delivery of Dexamethasone with ISEND Nanoparticles Attenuates the COVID-19 Cytokine Storm in Mice and Nonhuman Primates. Sci. Adv. 2023, 9. [Google Scholar] [CrossRef] [PubMed]
- Lokugamage, M.P.; Vanover, D.; Beyersdorf, J.; Hatit, M.Z.C.; Rotolo, L.; Echeverri, E.S.; Peck, H.E.; Ni, H.; Yoon, J.-K.; Kim, Y.; et al. Optimization of Lipid Nanoparticles for the Delivery of Nebulized Therapeutic MRNA to the Lungs. Nat. Biomed. Eng. 2021, 5, 1059–1068. [Google Scholar] [CrossRef]
- Kraft, W.K.; Steiger, B.; Beussink, D.; Quiring, J.N.; Fitzgerald, N.; Greenberg, H.E.; Waldman, S.A. The Pharmacokinetics of Nebulized Nanocrystal Budesonide Suspension in Healthy Volunteers. J. Clin. Pharmacol. 2004, 44, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Bridges, P.A.; Taylor, K.M.G. An Investigation of Some of the Factors Influencing the Jet Nebulisation of Liposomes. Int. J. Pharm. 2000, 204, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Beck-Broichsitter, M.; Kleimann, P.; Schmehl, T.; Betz, T.; Bakowsky, U.; Kissel, T.; Seeger, W. Impact of Lyoprotectants for the Stabilization of Biodegradable Nanoparticles on the Performance of Air-Jet, Ultrasonic, and Vibrating-Mesh Nebulizers. Eur. J. Pharm. Biopharm. 2012, 82, 272–280. [Google Scholar] [CrossRef] [PubMed]
- Elhissi, A.; Faizi, M.; Naji, W.; Gill, H.; Taylor, K. Physical Stability and Aerosol Properties of Liposomes Delivered Using an Air-Jet Nebulizer and a Novel Micropump Device with Large Mesh Apertures. Int. J. Pharm. 2007, 334, 62–70. [Google Scholar] [CrossRef]
- Beck-Broichsitter, M.; Merkel, O.M.; Kissel, T. Controlled Pulmonary Drug and Gene Delivery Using Polymeric Nano-Carriers. J. Control. Release 2012, 161, 214–224. [Google Scholar] [CrossRef]
- Beck-Broichsitter, M.; Knuedeler, M.-C.; Schmehl, T.; Seeger, W. Following the Concentration of Polymeric Nanoparticles During Nebulization. Pharm. Res. 2013, 30, 16–24. [Google Scholar] [CrossRef]
- Beck-Broichsitter, M.; Gauss, J.; Packhaeuser, C.B.; Lahnstein, K.; Schmehl, T.; Seeger, W.; Kissel, T.; Gessler, T. Pulmonary Drug Delivery with Aerosolizable Nanoparticles in an Ex Vivo Lung Model. Int. J. Pharm. 2009, 367, 169–178. [Google Scholar] [CrossRef]
- Neurohr, C.; Kneidinger, N.; Ghiani, A.; Monforte, V.; Knoop, C.; Jaksch, P.; Parmar, J.; Ussetti, P.; Sole, A.; Müller-Quernheim, J.; et al. A Randomized Controlled Trial of Liposomal Cyclosporine A for Inhalation in the Prevention of Bronchiolitis Obliterans Syndrome Following Lung Transplantation. Am. J. Transplant. 2022, 22, 222–229. [Google Scholar] [CrossRef]
- Gaspar, M.M.; Gobbo, O.; Ehrhardt, C. Generation of Liposome Aerosols with the Aeroneb Pro and the AeroProbe Nebulizers. J. Liposome Res. 2010, 20, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Hoy, S.M. Amikacin Liposome Inhalation Suspension in Refractory Mycobacterium Avium Complex Lung Disease: A Profile of Its Use. Clin. Drug Investig. 2021, 41, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Griffith, D.E.; Eagle, G.; Thomson, R.; Aksamit, T.R.; Hasegawa, N.; Morimoto, K.; Addrizzo-Harris, D.J.; O’Donnell, A.E.; Marras, T.K.; Flume, P.A.; et al. Amikacin Liposome Inhalation Suspension for Treatment-Refractory Lung Disease Caused by Mycobacterium Avium Complex (CONVERT). A Prospective, Open-Label, Randomized Study. Am. J. Respir. Crit. Care Med. 2018, 198, 1559–1569. [Google Scholar] [CrossRef] [PubMed]
- Lass, J.S.; Sant, A.; Knoch, M. New Advances in Aerosolised Drug Delivery: Vibrating Membrane Nebuliser Technology. Expert Opin. Drug Deliv. 2006, 3, 693–702. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Zhang, X.; Feng, K.; Zeng, W.; Wu, J.; Sun, D.; Lu, Z.; Feng, H.; Di, L. Nanotechnologies Meeting Natural Sources: Engineered Lipoproteins for Precise Brain Disease Theranostics. Asian J. Pharm. Sci. 2023, 18, 100857. [Google Scholar] [CrossRef]
- Schoni, M.; Kraemer, R. Osmolality Changes in Nebulizer Solutions. Eur. Respir. J. 1989, 2, 887–892. [Google Scholar] [CrossRef]
- Eschenbacher, W.L.; Boushey, H.A.; Sheppard, D. Alteration in Osmolarity of Inhaled Aerosols Cause Bronchoconstriction and Cough, but Absence of a Permeant Anion Causes Cough Alone. Am. Rev. Respir. Dis. 1984, 129, 211–215. [Google Scholar]
- Niven, R.W.; Carvajal, T.M.; Schreier, H. Nebulization of Liposomes. III. The Effects of Operating Conditions and Local Environment. Pharm. Res. 1992, 09, 515–520. [Google Scholar] [CrossRef]
- Ghazanfari, T.; Elhissi, A.M.A.; Ding, Z.; Taylor, K.M.G. The Influence of Fluid Physicochemical Properties on Vibrating-Mesh Nebulization. Int. J. Pharm. 2007, 339, 103–111. [Google Scholar] [CrossRef]
- Mc Callion, O.N.M.; Patel, M.J. Viscosity Effects on Nebulisation of Aqueous Solutions. Int. J. Pharm. 1996, 130, 245–249. [Google Scholar] [CrossRef]
- Weber, A.; Morlin, G.; Cohen, M.; Williams-Warren, J.; Ramsey, B.; Smith, A. Effect of Nebulizer Type and Antibiotic Concentration on Device Performance. Pediatr. Pulmonol. 1997, 23, 249–260. [Google Scholar] [CrossRef]
- Yohan, D.; Chithrani, B.D. Applications of Nanoparticles in Nanomedicine. J. Biomed. Nanotechnol. 2014, 10, 2371–2392. [Google Scholar] [CrossRef] [PubMed]
- Nelson, B.J.; Pané, S. Delivering Drugs with Microrobots. Science 2023, 382, 1120–1122. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Nano-Formulations | API | Implications | Status | Reference/NCT |
|---|---|---|---|---|
| Liposome | Amikacin | Mycobacterium avium complex (MAC) lung disease | Approved by FDA in 2018 | ARIKAYCE® KIT [21] |
| Liposome | Amikacin | CF | Phase III (last update posted in 2020) | NCT01316276 [78] |
| Liposome | Amikacin | NTM lung infection due to MAC | Phase III (last update posted in 2020) | NCT02344004 [79] |
| Liposome | Amikacin | Bronchiectasis | Phase II (last update posted in 2019) | NCT00775138 |
| Liposome | Ciprofloxacin | Cystic fibrosis (CF) | Phase II (last update posted in 2014) | NCT00645788 [80,81] |
| Nano-vesicles/niosomes | Salbutamol Sulphate | Pulmonary disease | Phase I (last update posted in 2017) | NCT03059017 [82,83] |
| Gene product/lipid vector | pGM169/GL67A (Plasmid DNA) | CF | Phase II (last update posted in 2015) | NCT01621867 [84] |
| mRNA-refdLNP (not stated in the literature) | MRT5005 (CFTR mRNA) | CF | Phase I/II (last update posted in 2020, recruiting) | NCT03375047 [85] |
| Inhaled nanoparticle (not stated in the literature) | Remdesivir (GS-5734) and NA-831 (NEUROSIVIR) | COVID-19, SARS, Severe Acute Respiratory Syndrome, etc. | Phase I (last update posted in 2020, recruiting) | NCT04480333 |
| Lipocalin-1 | IL-4Ra antagonist (PRS-060) | Asthma | Phase I (last update posted in 2020) | NCT03574805 [86] |
| Inhalation Devices | Delivery Mechanisms | Advantages | Limitations |
|---|---|---|---|
| DPIs | The drug-containing dry powder enters the airway through the airflow of the patient’s inhalation |
|
|
| MDIs | Propellant provides energy to release drug-containing aerosols |
|
|
| Jet nebulizers | Compressed air nebulizes drug-containing liquids into aerosols |
|
|
| Ultrasonic nebulizers | Nebulize drug-containing liquids into aerosols by generating high-frequency vibrations through a piezoelectric transducer |
|
|
| Vibrating mesh nebulizers | Drug-containing liquids are nebulized into aerosols by passing through ultrasonically vibrating mesh |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peng, S.; Wang, W.; Zhang, R.; Wu, C.; Pan, X.; Huang, Z. Nano-Formulations for Pulmonary Delivery: Past, Present, and Future Perspectives. Pharmaceutics 2024, 16, 161. https://doi.org/10.3390/pharmaceutics16020161
Peng S, Wang W, Zhang R, Wu C, Pan X, Huang Z. Nano-Formulations for Pulmonary Delivery: Past, Present, and Future Perspectives. Pharmaceutics. 2024; 16(2):161. https://doi.org/10.3390/pharmaceutics16020161
Chicago/Turabian StylePeng, Siyuan, Wenhao Wang, Rui Zhang, Chuanbin Wu, Xin Pan, and Zhengwei Huang. 2024. "Nano-Formulations for Pulmonary Delivery: Past, Present, and Future Perspectives" Pharmaceutics 16, no. 2: 161. https://doi.org/10.3390/pharmaceutics16020161