
The Effect of Additional Treatment with Empagliflozin or Semaglutide on Endothelial Function and Arterial Stiffness in Subjects with Type 1 Diabetes Mellitus—ENDIS Study

Abstract
:1. Introduction
2. Methods
2.1. Study Design and Subject Selection
2.2. Statistical Analysis
2.3. Study Protocol
2.4. Endothelial Function Assessment
2.5. Brachial Artery Fow-Mediated Dilation (FMD) Assessment
2.6. Forearm Blood Flow (FBF) Reactive Hyperemia Assessment
2.7. Arterial Stiffness Assessment
3. Results
3.1. Participant Disposition, Demographics, and Baseline Characteristics
3.2. Results of Anthropometric Measurements
3.3. Results of Glycemia, Lipid Profile, Renal, and Inflamation-Related Issues
3.4. Brachial Diameter/Flow-Mediated Dilation (Change in Brachial Diameter after Ischemia vs. Baseline)
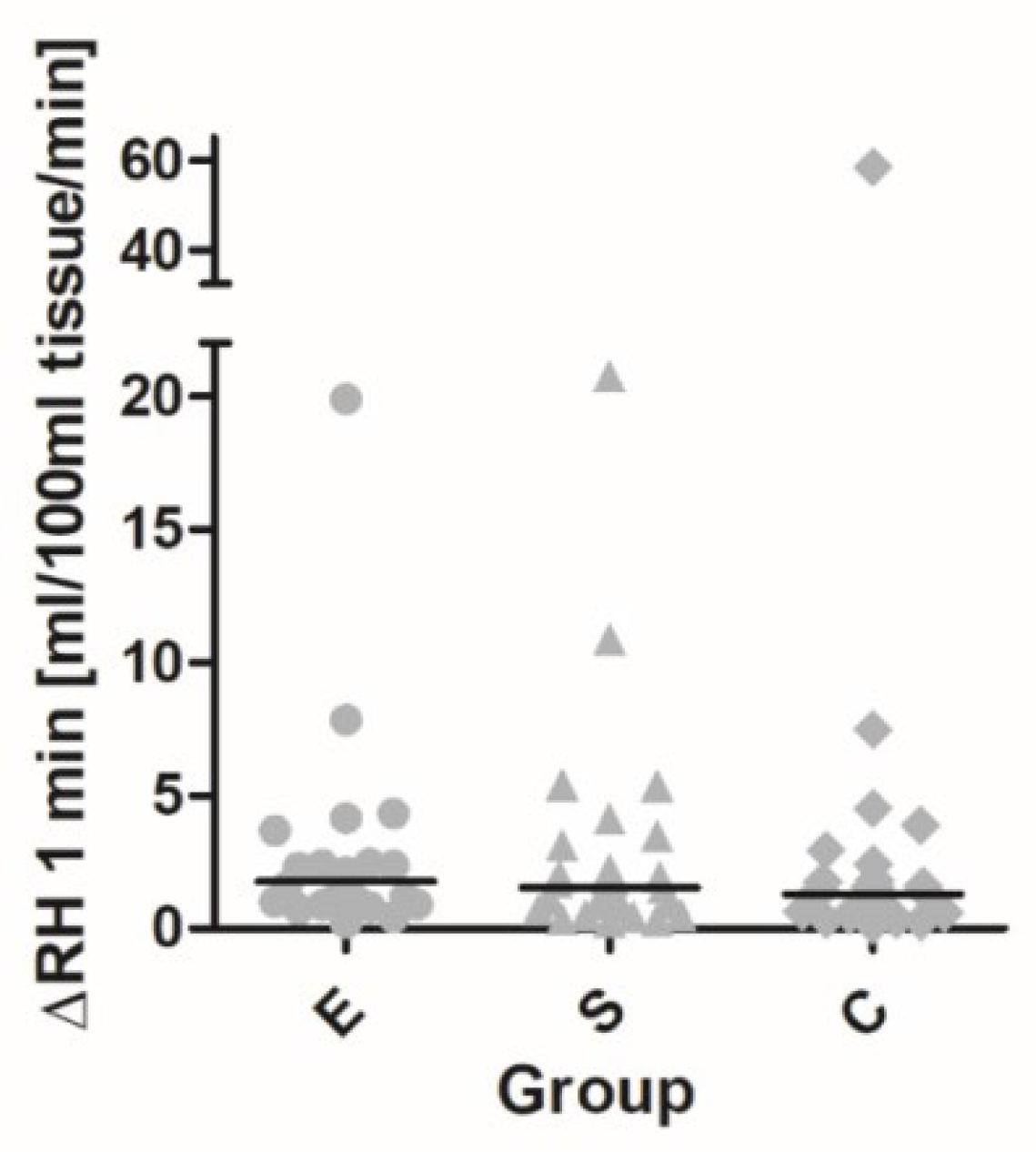
3.5. Forearm Blood Flow/Reactive Hyperemia (Change in Tissue Perfusion after Ischemia vs. Baseline)
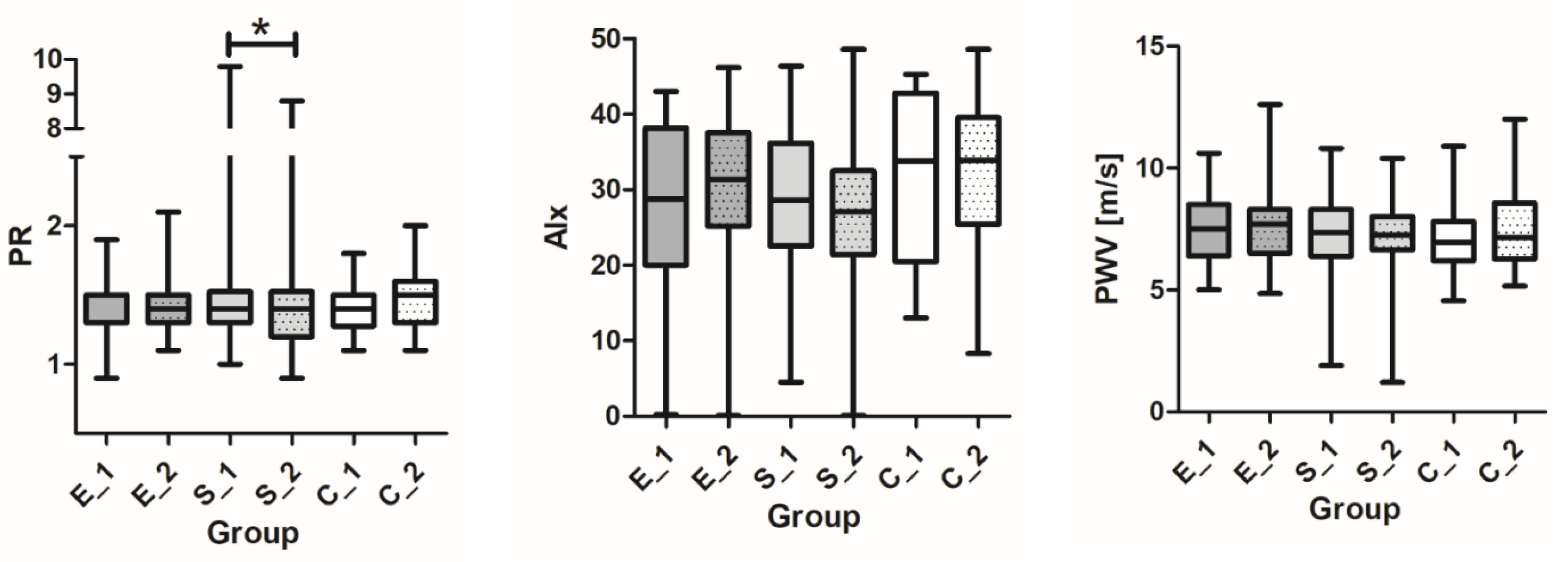
3.6. Arterial Stiffness; PWV, Alx, and PR
3.7. Safety and Tolerability
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zinman, B.; Wanner, C.; Lachin, J. EMPA REG outcome. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stephen, D.W. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 24, 347–357. [Google Scholar]
- Marso, S.; Saniels, G.; Frandsen, K. LEADER: Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 311–322. [Google Scholar] [CrossRef] [Green Version]
- Marso, S.; Bain, S.; Consoli, A. SUSTAIN 6: Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef] [Green Version]
- Davies, M.J.; D’Alessio, D.A. Management of hyperglycaemia in type 2 diabetes. A consensus report by the American Diabetes. Diabetes Ther. 2019, 10, 773–789. [Google Scholar]
- Nathan, D.M. Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications (DCCT/EDIC) Study Research Group. Intensive diabetes treatment and cardiovascular disease in patients with type 1 diabetes. N. Engl. J. Med. 2005, 353, 2643–2653. [Google Scholar]
- Lind, M.; Svensson, A.M.; Kosiborod, M.; Gudbjörnsdottir, S.; Pivodic, A.; Wedel, H.; Dahlqvist, S.; Clements, M.; Rosengren, A. Glycemic control and excess mortality in type 1 diabetes. N. Engl. J. Med. 2014, 371, 1972–1982. [Google Scholar] [CrossRef]
- Schofield, J.; Ho, J. Cardiovascular Risk in Type 1 Diabetes Mellitus. Diabetes Ther. 2019, 3, 773–789. [Google Scholar]
- Deanfield, J. Endothelial Function and Dysfunction Testing and Clinical Relevance. Circulation 2007, 115, 1285–1295. [Google Scholar] [CrossRef]
- Lekakis, J.; Abraham, P. Methods for evaluating endothelial function: A position statement from the European Society of Cardiology Working Group on Peripheral Circulation. Eur. J. Cardiovasc. Prev. Rehabil. 2011, 6, 775–789. [Google Scholar] [CrossRef]
- Widlansky, M.E.; Gokce, N. The clinical implications of endothelial dysfunction. J. Am. Coll. Cardiol. 2003, 42, 1149–1160. [Google Scholar] [PubMed] [Green Version]
- Badhwar, S.; Chandar, D. Regional arterial stiffness in central and peripheral arteries is differentially related to endothelial dysfunction assessed by brachial flow-mediated dilation in metabolic syndrome. Diabetes Vasc. Dis. Res. 2018, 2, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Corretti, M.C.; Anderson, T.; Benjamin, E.; Celermajer, D. International Brachial Artery Reactivity Task Force. Guidelines for the ultrasound assessment of endothelial-dependent flow-mediated vasodilation of the brachial artery: A report of the International Brachial Artery Reactivity Task Force. J. Am. Coll. Cardiol. 2002, 39, 257–265. [Google Scholar] [PubMed] [Green Version]
- Higashi, Y. Assessment of endothelial function. History, methodological aspects, and clinical perspectives. Int. Heart J. 2015, 56, 125–134. [Google Scholar]
- Rosenberry, R.; Nelson, M.D. Reactive hyperemia: A review of methods, mechanisms, and considerations. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2020, 318, 605–618. [Google Scholar] [CrossRef]
- Nichols, W.W.; Denardo, S.J. Effects of arterial stiffness, pulse wave velocity, and wave reflections on the central aortic pressure waveform. J. Clin. Hypertens. 2008, 10, 295–303. [Google Scholar] [CrossRef]
- Cé, G.V. Endothelial dysfunction is related to poor glycemic control in adolescents with type 1 diabetes under 5 years of disease: Evidence of metabolic memory. J. Clin. Endocrinol. Metab. 2011, 96, 1493–1499. [Google Scholar] [CrossRef] [Green Version]
- Lespagnol, E.; Dauchet, L.; Pawlak-Chaouch, M. Early Endothelial Dysfunction in Type 1 Diabetes Is Accompanied by an Impairment of Vascular Smooth Muscle Function: A Meta-Analysis. Front. Endocrinol. 2020, 11, 203. [Google Scholar] [CrossRef]
- Hoffman, R.P.; Dye, A.S.; Huang, H.; Bauer, J.A. Effects of Glucose Control and Variability on Endothelial Function and Repair in Adolescents with Type 1 Diabetes. Int. Sch. Res. Not. 2013, 2013, 876547. [Google Scholar] [CrossRef] [Green Version]
- Danne, T.; Nimri, R.; Battelino, T.; Bergenstal, R.M.; Close, K.L.; DeVries, J.H.; Garg, S.; Heinemann, L.; Hirsch, I.; Amiel, S.A.; et al. International Consensus on Use of Continuous Glucose Monitoring. Diabetes Care 2017, 40, 1631–1640. [Google Scholar] [CrossRef] [Green Version]
- Jamiołkowska, M.; Jamiołkowska, I.; Luczynski, W.; Tolwinska, J.; Bossowski, A.; Glowinska Olszewska, B. Impact of Real-Time Continuous Glucose Monitoring Use on Glucose Variability and Endothelial Function in Adolescents with Type 1 Diabetes: New Technology—New Possibility to Decrease Cardiovascular Risk? J. Diabetes Res. 2016, 2016, 4385312. [Google Scholar] [CrossRef] [PubMed]
- Bots, M.L.; Remme, W.J.; Luscher, T.F.; Fox, K.M.; Bertrand, M.; Ferrari, R.; Simoons, M.L.; Grobbee, D.E. ACE inhibition and endothelial function: Main findings of PERFECT, a sub-study of the EUROPA trial. Cardiovasc. Drugs Ther. 2007, 21, 69–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; Gong, D. Meta-analysis of the effects of statin therapy on endothelial function in patients with diabetes mellitus. Atherosclerosis 2012, 223, 78–85. [Google Scholar] [CrossRef] [PubMed]
- Bosch, A.; Ott, C. How does empagliflozin improve arterial stiffness in patients with type 2 diabetes mellitus? Sub analysis of a clinical trial. Cardiovasc. Diabetol. 2019, 18, 44. [Google Scholar] [CrossRef]
- Striepe, K.; Jumar, A. Effects of the selective sodium-glucose cotransporter 2 inhibitor empagliflozin on vascular function and central hemodynamics in patients with type 2 diabetes mellitus. Circulation 2017, 136, 1167–1169. [Google Scholar] [CrossRef]
- Batzias, K.; Antonopoulos, A. Effects of Newer Antidiabetic Drugs on Endothelial Function and Arterial Stiffness: A Systematic Review and Meta-Analysis. J. Diabetes Res. 2018, 2018, 1232583. [Google Scholar] [CrossRef] [Green Version]
- Lunder, M.; Janic, M.; Japelj, M.; Janež, A. Empagliflozin on top of metformin treatment improves arterial function in patients with type 1 diabetes mellitus. Cardiovasc. Diabetol. 2018, 17, 153. [Google Scholar] [CrossRef] [Green Version]
- Pitocco, D.; Zaccardi, F.; Tarzia, P.; Milo, M.; Scavone, G.; Rizzo, P.; Pagliaccia, F.; Nerla, R.; Di Franco, A.; Manto, A.; et al. Metformin improves endothelial function in type 1 diabetic subjects: A pilot, placebo-controlled randomized study. Diabetes Obes. Metab. 2013, 15, 427–431. [Google Scholar] [CrossRef]
- Solini, A.; Giannini, L.; Seghieri, M.; Vitolo, E.; Taddei, S.; Ghiadoni, L.; Bruno, R.M. Dapagliflozin acutely improves endothelial dysfunction, reduces aortic stiffness and renal resistive index in type 2 diabetic patients: A pilot study. Cardiovasc. Diabetol. 2017, 16, 138. [Google Scholar] [CrossRef] [Green Version]
- Lambadiari, V.; Pavlidis, G.; Kousathana, F.; Varoudi, M.; Vlastos, D.; Maratou, E.; Georgiou, D.; Andreadou, I.; Parissis, J.; Triantafyllidi, H.; et al. Effects of 6-month treatment with the glucagon like peptide-1 analogue liraglutide on arterial stiffness, left ventricular myocardial deformation and oxidative stress in subjects with newly diagnosed type 2 diabetes. Cardiovasc. Diabetol. 2018, 17, 8. [Google Scholar] [CrossRef] [Green Version]
- Delong, C.; Sharma, S. Physiology, Peripheral Vascular Resistance. StatPearls Publishing. 2023. Available online: https://www.ncbi.nlm.nih.gov/books/NBK538308/ (accessed on 22 May 2023).
- Irace, C.; Cutruzzolà, A.; Parise, M.; Fiorentino, R.; Frazzetto, M.; Gnasso, C.; Casciaro, F.; Gnasso, A. Effect of empagliflozin on brachial artery shear stress and endothelial function in subjects with type 2 diabetes: Results from an exploratory study. Diabetes Vasc. Dis. Res. 2020, 17, 1479164119883540. [Google Scholar] [CrossRef] [Green Version]
- Wei, R.; Wang, W.; Pan, Q.; Guo, L. Effects of SGLT-2 Inhibitors on Vascular Endothelial Function and Arterial Stiffness in Subjects with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Endocrinol. 2022, 13, 826604. [Google Scholar] [CrossRef]
- Hong, K.; Park, Y. Effects of short-term exenatide treatment on regional fat distribution, glycated hemoglobin levels, and aortic pulse wave velocity of obese type 2 diabetes mellitus patients. Endocrinol. Metab. 2016, 31, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Maruhashi, T.; Higashi, Y. Pathophysiological Association between Diabetes Mellitus and Endothelial Dysfunction. Antioxidants 2021, 10, 1306. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, M.A.; Flores, S.C. Autoimmune-mediated oxidative stress and endothelial dysfunction: Implications of accelerated vascular injury in type I diabetes. J. Surg. Res. 2009, 155, 173–178. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Baseline Caracteristics | Empagliflozin (n = 30) | Semaglutide (n = 30) | Control (n = 29) | p |
|---|---|---|---|---|
| Age (years) | 48.2 ± 10.7 | 48.5 ± 9.6 | 47.0 ± 12 | 0.697 |
| DM duration(years) | 21.3 ± 10.2 | 21.9 ± 11.2 | 18.8 ± 11.9 | 0.548 |
| Sex male (n/%) | 18/60 | 19/63.3 | 17/58.6 | 0.930 |
| BMI (kg/m2) | 27.7 ± 4.3 | 28.2 ± 4.8 | 26.9 ± 3.0 | 0.783 |
| Weight (kg) | 81.9 ± 14.2 | 84.6 ± 16.4 | 82.6 ± 11.7 | |
| Waist (cm) | 99.9 ± 11.7 | 99.5 ± 14.3 | 98.5 ± 9.9 | |
| Smokers (n/%) | 4/13.3 | 5/16.7 | 5/17.2 | |
| HbA1C (%) | 7.88 ± 0.72 | 7.42 ± 0.80 | 7.04 ± 0.90 | 0.002 * |
| Hypos (%) | 1.9 ± 2.8 | 4.2 ± 4.3 | 3.3 ± 3.1 | |
| Glucose (mmol/L) | 9.02 ± 2.93 | 7.62 ± 2.84 | 7.55 ± 3.04 | |
| TIR > 70% (n/%) | 10/33.3 | 19/63.3 | 17/58.6 | |
| TIR (%) | 61.7 ± 17.1 | 70.6 ± 14.7 | 69.7 ± 17.4 | |
| CV ≤ 36% (n/%) | 22/76.7 | 29/55.2 | 19/67.9 | |
| CV (%) | 33.8 ± 5.7 | 35.3 ± 6.1 | 33.9 ± 5.5 | |
| MDI basal–bolus (n) | 13 | 17 | 17 | |
| CSII without loop (n) | 3 | 4 | 3 | |
| CSII loop (n) | 4 | 2 | 2 | |
| CSII Hybride (n) | 10 | 7 | 7 | |
| Hypertension (n/%) | 15/50 | 15/50 | 12/41.4 | |
| RR sist (mmHg) | 132.5 ± 15.7 | 134.7 ± 16.4 | 130.5 ± 13.6 | 0.875 |
| RR diast (mmHg) | 76.5 ± 7.4 | 78.4 ± 15.5 | 75.7 ± 7.5 | 0.979 |
| Heart rate (/min) | 66.4 ± 10.5 | 68.3 ± 9.9 | 68.6 ± 12.6 | |
| Hyperlipidemia (n/%) | 22/73.3 | 22/73.3 | 19/65.5 | |
| LDL (mmol/L) | 2.61 ± 0.86 | 2.66 ± 0.71 | 2.62 ± 0.78 | 0.948 |
| HDL (mmol/L) | 1.56 ± 0.36 | 1.53 ± 0.38 | 1.51 ± 0.39 | 0.830 |
| Triglycerides (mmol/L) | 1.07 ± 0.51 | 1.23 ± 0.75 | 1.11 ± 0.56 | 0.900 |
| eGFRcys (mL/min/1.73) | 86.1 ± 9.2 | 85.8 ± 8.3 | 86.5 ± 7.8 | 0.872 |
| ACR (g/mol) | 3.35 ± 11.2 | 2.41 ± 2.92 | 2.35 ± 5.54 | |
| All MVC (n/%) | 14/46.7 | 19/63.3 | 9/31 | 0.046 * |
| NPDR (n/%) | 8/26.6 | 11/36.6 | 5/16.6 | |
| D. neuropathy (n/%) | 3/10 | 3/10 | 3/10 | |
| MAU (n/%) | 6/20 | 10/33.3 | 5/17.2 | |
| CM (n/%) | 17/43.3 | 13/43.3 | 9/31 | 0.139 |
| ACE inh/ARB (n) | 14 | 9 | 7 | |
| Statin (n) | 13 | 9 | 6 | |
| hs CRP (mmol/L) | 2.32 ± 2.1 | 5.5 ± 8.2 | 2.5 ± 3.1 | |
| UA (μmol/L) | 252 ± 72 | 245 ± 62 | 252 ± 61 |
| Variables | Empagliflozin (n = 30) | Semaglutide (n = 30) | Control (n = 29) | p ** |
|---|---|---|---|---|
| Mean ± SD Median (Min, Max) | Mean ± SD Median (Min, Max) | Mean ± SD Median (Min, Max) | ||
| ∆BMI (kg/m2) | −0.88 ± 1.07 −0.85 (−3.5, 0.8) p = 0.000 * | −1.42 ± 4.8 −1.5 (−3.8, 0.69) p = 0.000 | 0.04 ± 0.98 −0.30 (2.4, 1.9) p = 0.782 | 0.000 ** |
| ∆Weight (kg) | −2.49 ± 2.69 −2.8 (−10.0, 1.0) p = 0.000 * | −4.3 ± 2.98 −4.2 (−11.7, 1.0) p = 0.000 * | −0.10 ± 2.16 −1.0 (−3.7, 4.0) p = 0.791 | 0.000 ** |
| ∆Waist (cm) | −4.0 ± 5.5 3.5 (−19, 9) p = 0.000 * | −4.4 ± 5.2 −3.5 (−24, 2) p = 0.000 * | −0–97 ± 5.4 0.0 (−14, 12) p = 0.395 | 0.016 ** |
| ∆HbA1C (%) | −0.24 ± 0.59 −0.1 (−1.8, 0.9) p = 0.052 | −0.29 ± 0.61 −0.39 (−2.0, 0.9) p = 0.016 * | 0.12 ± 0.44 0.1 (−1.1, 1.1) p = 0.091 | 0.00 ** |
| ∆TIR (%) | 4.2 ± 11.9 6.0 (−25, 28) p = 0.393 | 0.7 ± 13.7 0.5 (−53, 20) p = 0.247 | −1.35 ± 8.8 −2.5 (−15, 19) p = 0.230 | 0.027 ** |
| ∆CV (%) | −0.91 ± 5.0 −1.5 (−13.0, 10.3) p = 0.221 | −1.28 ± 4.8 −1.2 (−12, 11.4) p = 0.143 | 1.06 ± 4.3 0.7 (−6.4, 16.2) p = 0.223 | 0.103 |
| ∆hypo (%) | −0.71 ± 2.3 0.0 (−9, 2.5) p = 0.176 | 0.22 ± 4.4 0.0 (−4.6, 6.3) p = 0.858 | −0.48 ± 2.3 0.0 (−6.9, 4.0) p = 0.443 | 0.180 |
| ∆TDI (IU) | −5.1 ± 10.0 −2.7 (−31, 13) p = 0.009 * | −8.5 ± 9.3 −6.0 (−32, 7) p = 0.000 * | −1.1 ± 7.5 0.0 (−32, 10) p = 0.747 | 0.001 ** |
| ∆RR syst (mmHg) | −1.7 ± 19 −4.0 (−31, 55) p = 0.271 | −3.7 ± 18 −3 (−42, 29) p = 0.410 | 5.4 ± 16 8 (−20, 53) p = 0.138 | 0.105 |
| ∆RR diast (mmHg) | −1.8 ± 7.5 −2.5 (−22, 15) p = 0.174 | −3.0 ± 14 −1.0 (−43, 28) p = 0.381 | 2.8 ± 7.8 3.0 (−12, 16) p = 0.067 | 0.066 |
| ∆heart rate (/min) | 1.5 ± 9.0 −1.0 (−15, 24) p = 0.681 | 1.7 ± 6.6 2.5 (−12, 12) p = 0.115 | −0.6 ± 7.7 0.0 (−21, 12) p = 1.0 | 0.512 |
| ∆LDL (mmol/L) | 0.03 ± 0.75 0.00 (−2.8, 1.4) p = 0.393 | −0.30 ± 0.68 −0.5 (−1.2, 1.9) p = 0.017 * | −0.15 ± 0.51 −0.1 (−1.6, 0.9) p = 0.129 | 0.003 ** |
| ∆HDL (mmol/L) | 0.003 ± 0.26 0.0 (−0.9, 0.6) p = 0.741 | −0.05 ± 0.25 0.0 (−0.5, 0.6) p = 0.186 | 0.02 ± 0.25 0.0 (−0.5, 0.6) p = 0.723 | 0.439 |
| ∆Tg (mmol/L) | −0.01 ± 0.39 0.0 (−1.1, 0.9) p = 0.978 | −0.12 ± 0.44 −0.1 (−1.4, 0.7) p = 0.178 | 0.09 ± 0.53 0.0 (−0.8, 2.1) p = 0.556 | 0.346 |
| ∆eGFR (cystatine) | −1.67 ± 5.0 0.0 (−20, 8) p = 0.075 | 0.83 ± 4.2 0.0 (−13, 13) p = 0.202 | −0.62 ± 2.3 0.0 (−9, 3) p = 0.234 | 0.075 |
| ∆cystatine (mg/L) | 0.04 ± 0.08 0.03 ± (0.15, 0.35) p = 0.003 * | −0.003 ± 0.08 0.0 (−0.1, 0.25) p = 0.547 | −0.26 ± 1.48 0.08 (−8, 0.1) p = 0.516 | 0.025 ** |
| ∆ACR (mg/L) | −1.08 ± 5.0 0.0 (−27, 1.2) p = 0.467 | −0.26 ± 2.56 −0.49 (−7.8, 8.3) p = 0.124 | −0.62 ± 3.0 0.0 (−15.8, 2.1) p = 0.273 | 0.639 |
| ∆hsCRP (mmol/L) | 1.69 ± 7.4 0.15 (−3.5, 40) p = 0.234 | −0.64 ± 6.4 −0.25 (−10.6, 21) p = 0.024 * | 0.73 ± 4.6 0.1 (−10.6, 21) p = 0.247 | 0.019 ** |
| ∆UA (μmol/L) | −22 ± 43 −22 (−112, 58) p = 0.014 * | 0.47 ±45 0.5 (−100, 111) p = 0.880 | 0.55 ± 32 5.0 (−84, 75) p = 0.634 | 0.065 |
| 0.02 ± 0.25 | ||||
| ∆βOHB | 0.0 (−0.5, 0.9) | |||
| (mmol/L) | p = 0.938 | |||
| ∆Ht | 0.468 ± 2.4 | −0.017 ± 0.07 | −0.001 ± 0.025 | 0.005 ** |
| p = 0.008 * | p = 0.225 | p = 0.538 |
| Variable | E–C p | S–C p | E–S p |
|---|---|---|---|
| ∆BMI (kg/m2) | 0.006 * | 0.000 * | 0.075 |
| ∆Weight (kg) | 0.006 * | 0.000 * | 0.020 * |
| ∆Waist (cm) | 0.016 * | 0.010 * | 0.857 |
| ∆HbA1C (%) | 0.015 * | 0.003 * | 0.547 |
| ∆TIR (%) | 0.007 * | 0.124 | 0.252 |
| ∆TDI (IU) | 0.022 * | 0.000 * | 0.114 |
| ∆LDL (mmol/L) | 0.192 | 0.044 * | 0.001 * |
| ∆cystatine (mg/L) | 0.009 * | 0.057 | 0.491 |
| ∆hsCRP (mmol/L) ∆Ht | 0.996 0.012 * | 0.015 * 0.596 | 0.015 * 0.002 * |
| Variables | Empagliflozin (n = 30) | Semaglutide (n = 30) | Control (n = 29) | p |
|---|---|---|---|---|
| FMD Measurements | Mean ± SD Median (Min, Max) p | Mean ± SD Median (Min, Max) p | Mean ± SD Median (Min, Max) p | |
| FMD1 (mm) | 0.20 ± 0.11 0.21 (0.00, 0.4) p = 0.000 * | 0.23 ± 0.11 0.23 (0.00, 0.5) p = 0.000 * | 0.27 ± 0.09 0.26 (0.00, 0.40) p = 0.000 * | 0.024 ** |
| % FMD1 (%) | 5.39 ± 3.01 5.21 (0.00, 10.4) | 5.81 ± 3.14 5.45 (0.00, 13.5) | 7.15 ± 2.48 7.54 (0.00, 10.7) | |
| FMD2 (mm) | 0.41 ± 0.22 0.45 (0.22, 1.06) p = 0.000 * | 0.44 ± 0.18 0.40 (0.0, 0.7) p = 0.000 * | 0.28 ± 0.13 0.30 (0.00, 0.56) p = 0.000 * | 0.001 ** |
| % FMD2 (%) | 10.6 ± 5.7 11.6 (0.00, 23.6) | 11.1 ± 4.9 11.7 (0.3, 19) | 7.2 ± 3.2 7.7 (0.00, 13) | |
| FMD2 − FMD1 (mm) | 0.209 ± 0.18 | 0.211 ± 0.14 | 0.008 ± 0.11 | |
| 0.233 (−0.1, 0.9) | 0.217 (0.0, 0.5) | 0.00 (−0.3, 0.2) | 0.000 ** | |
| %FMD2/%FMD1 | 2.0 ± 1.3 | 1.9 ± 1.3 | 1.0 ± 0.5 | |
| 1.7 (0.0, 5.4) | 1.7 (0.0, 5.0) | 0.9 (0.0, 2.6) | 0.000 ** | |
| p = 0.000 * | p = 0.000 * | p = 0.427 | ||
| FBF measurements | Median (Min, Max) p | Median (Min, Max) p | Median (Min, Max) p | |
| Baseline FBF1 | 2.87 (1.3,6.3) | 3.58 (1.33, 9.0) | 3.2 (1.44, 7.5) | 0.418 |
| RH 1 (1 min interval) Ml/100 mL/min/% | 1.96 (0.04, 7.7) =66% | 2.08 (0.15, 6.79) =68% | 2.29 (0.04, 6.42) =60% | 0.684 |
| RH 1 (3 min interval) Ml/100 mL/min/% | 0.45 (−0.25, 2.82) =14% | 0.54 (−1.0, 3.9) =17% | 0.62 (−2.0, 4.0) =22% | 0.685 |
| Baseline FBF2 | 3.47 (0.7, 5.9) | 3.25 (0.5, 5.2) | 2.82 (0.5, 5.2) | 0.327 |
| RH 2 (1 min interval) Ml/100 mL/min | 2.55 (0.01, 9.78) =97% p = 0.074 | 3.14 (0.73, 13.0) =78% p = 0.701 | 2.79 (0.33, 7.86) =103% p = 0.990 | 0.912 |
| RH 2 (3 min interval) Ml/100 mL/min/% | 1.11 (−0.58, 9.9) =35% p = 0.101 | 1.08 (−0.62, 13.0) =31% p = 0.564 | 0.85 (−0.90, 6.1) =31% p = 0.675 | 0.973 |
| RH2/RH1 1 min | 1.77 (0.21, 19.8) | 1.55 (0.26, 20.7) | 1.2 (0.14, 58.4) | 0.552 |
| RH2/RH1 3 min | 1.68 (−52, 35) | 0.72 (−2.4, 24.8) | 0.71 (−13, 8.0) | 0.445 |
| Arterial stiffness | Mean ± SD Median (Min, Max) p | Mean ± SD Median (Min, Max) p | Mean ± SD Median (Min, Max) p | |
| ∆ PWV (m/s) | 0.04 ± 0.82 0.0 (−2.0–2.0) p = 0.923 | −0.29 ± 1.43 0.0 (−7.3–1.1) p = 0.483 | 0.27 ± 0.82 0.2 (−0.8–3.4) p = 0.109 | 0.250 |
| ∆ Alx 75 (%) | 2.55 ± 8.7 2.0 (−12, 28) p = 0.149 | −1.42 ± 8.0 −0.5 (−19, 18) p = 0.248 | 1.56 ± 7.8 0.00 (−9.6, 27) p = 0.501 | 0.209 |
| ∆ PR (mmHg/Lmin) | −0.01 ± 0.17 0.0 (−0.4–0.4) p = 0.754 | −0.07 ± 0.23 0.0 (−1.0–0.3) p = 0.046 * | 0.06 ± 0.06 0.37 (0.2–0.5) p = 0.060 | 0.025 ** |
| Variable | E–C p | S–C p | E–S p |
|---|---|---|---|
| FMD 1 | 0.035 * | 0.088 | 1.0 |
| %FMD1 | 0.015 * | 0.029 * | 0.810 |
| FMD 2 | 0.013 * | 0.001 * | 1.0 |
| %FMD2 FMD2-FMD1 | 0.004 * 0.000 * | 0.000 * 0.000 * | 0.461 0.709 |
| %FMD2/%FMD1 | 0.000 * | 0.000 * | 0.745 |
| ∆ PR | 0.119 | 0.007 * | 0.258 |
| β | SE | CI95 L | CI95 U | p | |
|---|---|---|---|---|---|
| Intercept | 0.800 | 0.2627 | 0.285 | 1.314 | 0.002 |
| Smoking | −0.265 | 0.2744 | −0.803 | 0.272 | 0.333 |
| AH | 0.098 | 0.3051 | −0.500 | 0.696 | 0.748 |
| HLP | 0.064 | 0.2630 | −0.451 | 0.580 | 0.807 |
| MVC | −0.001 | 0.2563 | −0.504 | 0.501 | 0.996 |
| CM | 0.558 | 0.3122 | −0.054 | 1.179 | 0.074 |
| Duration | −0.001 | 0.0107 | −0.022 | 0.020 | 0.904 |
| ∆CV | 0.024 | 0.0230 | −0.021 | 0.069 | 0.300 |
| ∆BW | −0.060 | 0.0401 | −0.138 | 0.019 | 0.136 |
| ∆TIRp | 0.008 | 0.0097 | −0.011 | 0.027 | 0.432 |
| ∆HbA1C | 0.410 | 0.1976 | −0.022 | 0.797 | 0.038 * |
| ∆LDL ∆CRP | 0.306 0.009 | 0.1677 0.0172 | −0.022 −0.025 | 0.635 0.043 | 0.068 0.602 |
| ∆UA | 0.001 | 0.0025 | −0.004 | 0.006 | 0.663 |
| Group E | 0.793 | 0.2938 | 0.217 | 1.368 | 0.007 * |
| Group S | 0.820 | 0.3258 | 0.182 | 1.459 | 0.012 * |
| Variable | β | SE | CI95 L | CI95 U | p |
|---|---|---|---|---|---|
| Intercept | 0.200 | 0.1018 | 0.001 | 0.400 | 0.049 |
| Smoking | −0.027 | 0.0556 | −0.136 | 0.082 | 0.627 |
| AH | 0.001 | 0.0485 | −0.094 | 0.096 | 0.980 |
| HLP | 0.080 | 0.0501 | −0.018 | 0.179 | 0.108 |
| Age | −0.004 | 0.0023 | −0.009 | 0.059 | 0.052 |
| ∆RRsyst | 0.003 | 0.0012 | −0.001 | 0.005 | 0.0.13 * |
| ∆LDL | −0.064 | 0.0335 | −0.130 | 0.001 | 0.055 |
| ∆HbA1C | 0.020 | 0.0335 | −0.049 | 0.090 | 0.565 |
| Group E | −0.033 | 0.0492 | −0.129 | 0.063 | 0.502 |
| Group S | −0.114 | 0.0494 | −0.017 | 5.352 | 0.021 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Navodnik, M.P.; Janež, A.; Žuran, I. The Effect of Additional Treatment with Empagliflozin or Semaglutide on Endothelial Function and Arterial Stiffness in Subjects with Type 1 Diabetes Mellitus—ENDIS Study. Pharmaceutics 2023, 15, 1945. https://doi.org/10.3390/pharmaceutics15071945
Navodnik MP, Janež A, Žuran I. The Effect of Additional Treatment with Empagliflozin or Semaglutide on Endothelial Function and Arterial Stiffness in Subjects with Type 1 Diabetes Mellitus—ENDIS Study. Pharmaceutics. 2023; 15(7):1945. https://doi.org/10.3390/pharmaceutics15071945
Chicago/Turabian StyleNavodnik, Maja Preložnik, Andrej Janež, and Ivan Žuran. 2023. "The Effect of Additional Treatment with Empagliflozin or Semaglutide on Endothelial Function and Arterial Stiffness in Subjects with Type 1 Diabetes Mellitus—ENDIS Study" Pharmaceutics 15, no. 7: 1945. https://doi.org/10.3390/pharmaceutics15071945