
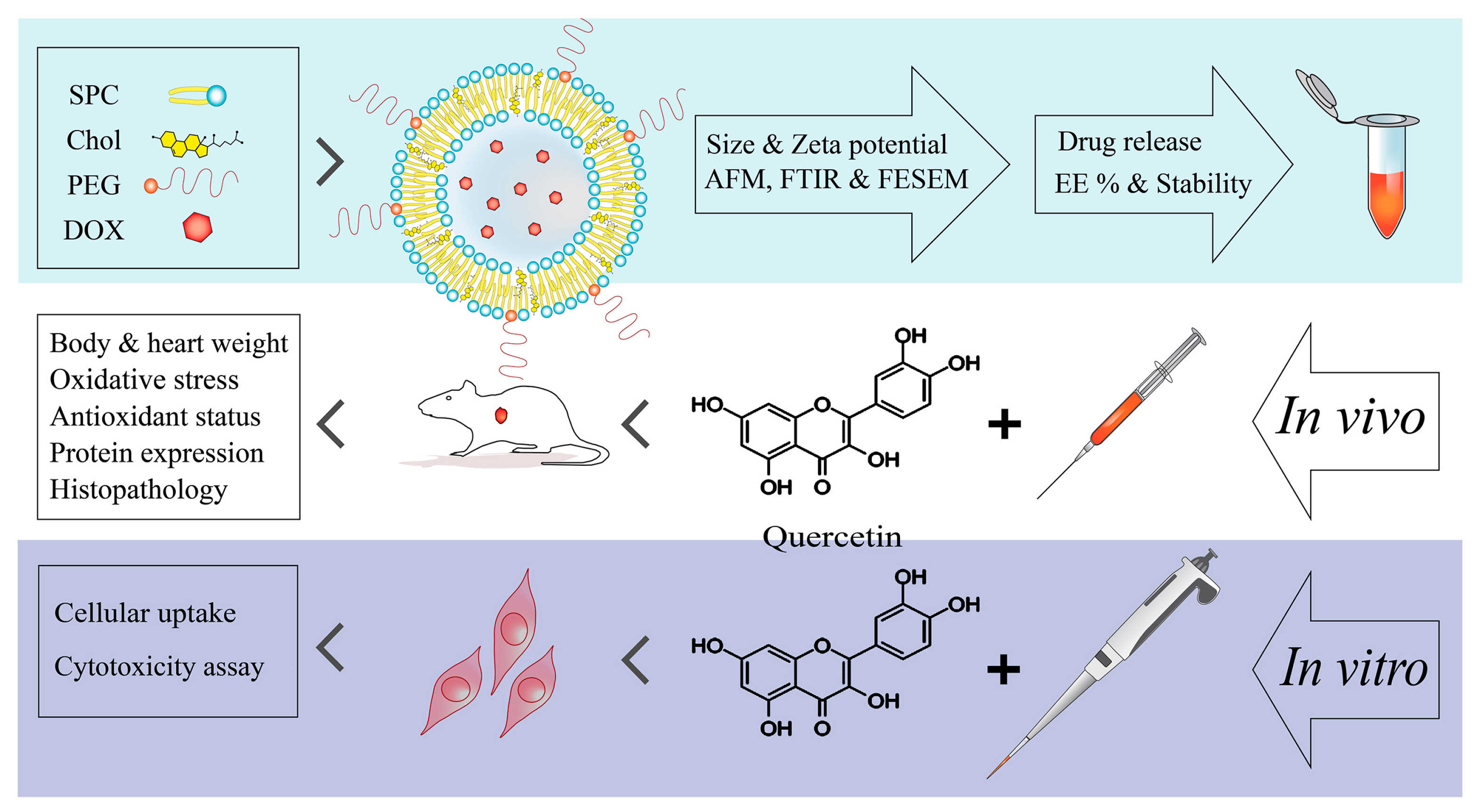
Reduction of Doxorubicin-Induced Cardiotoxicity by Co-Administration of Smart Liposomal Doxorubicin and Free Quercetin: In Vitro and In Vivo Studies
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Design and Synthesis of Nanocarriers
2.3. Characterization and Stability of Nanocarriers
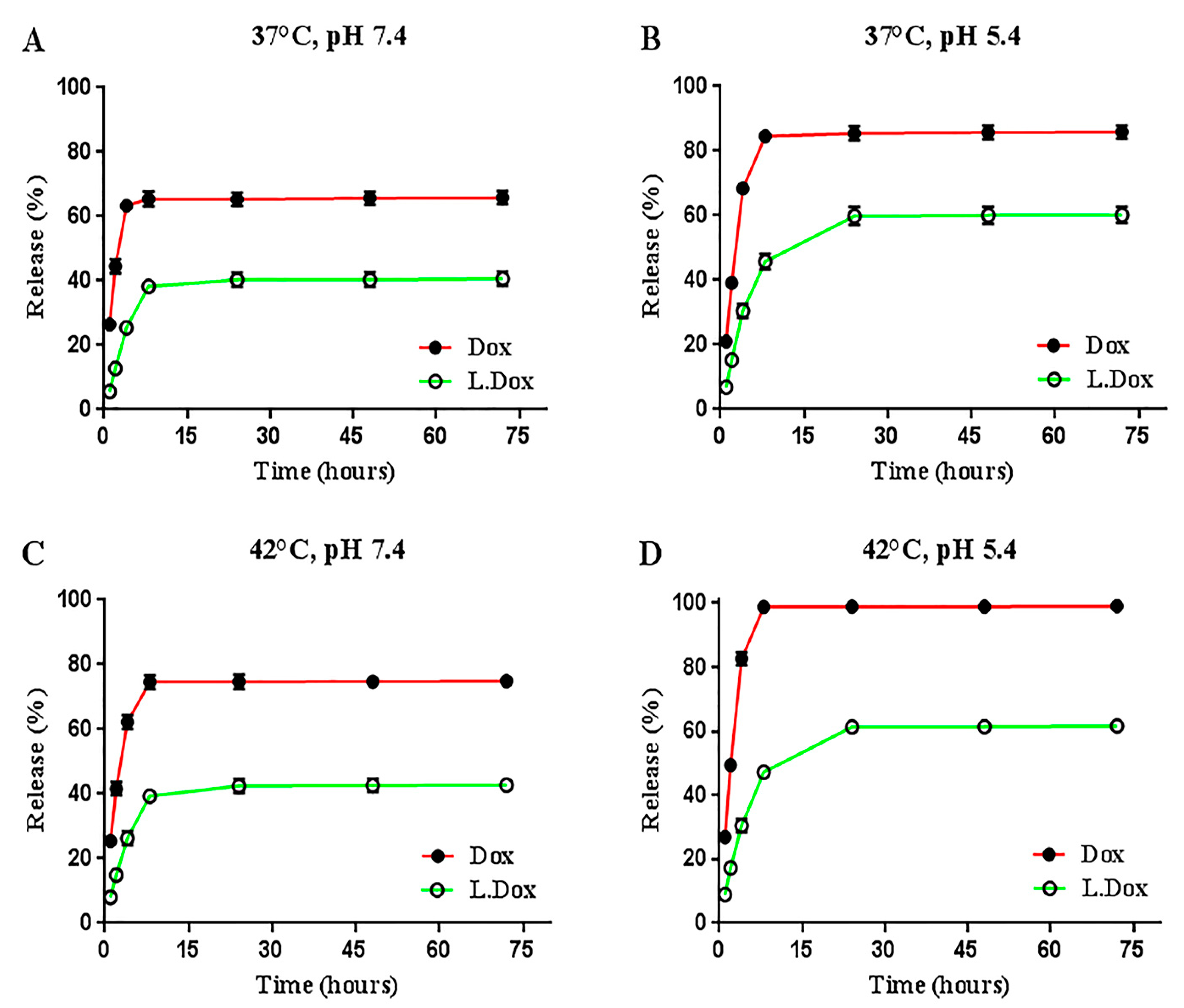
2.4. In Vitro Drug Release
2.5. Animal Groups and Treatment
2.6. Biochemical Assessments
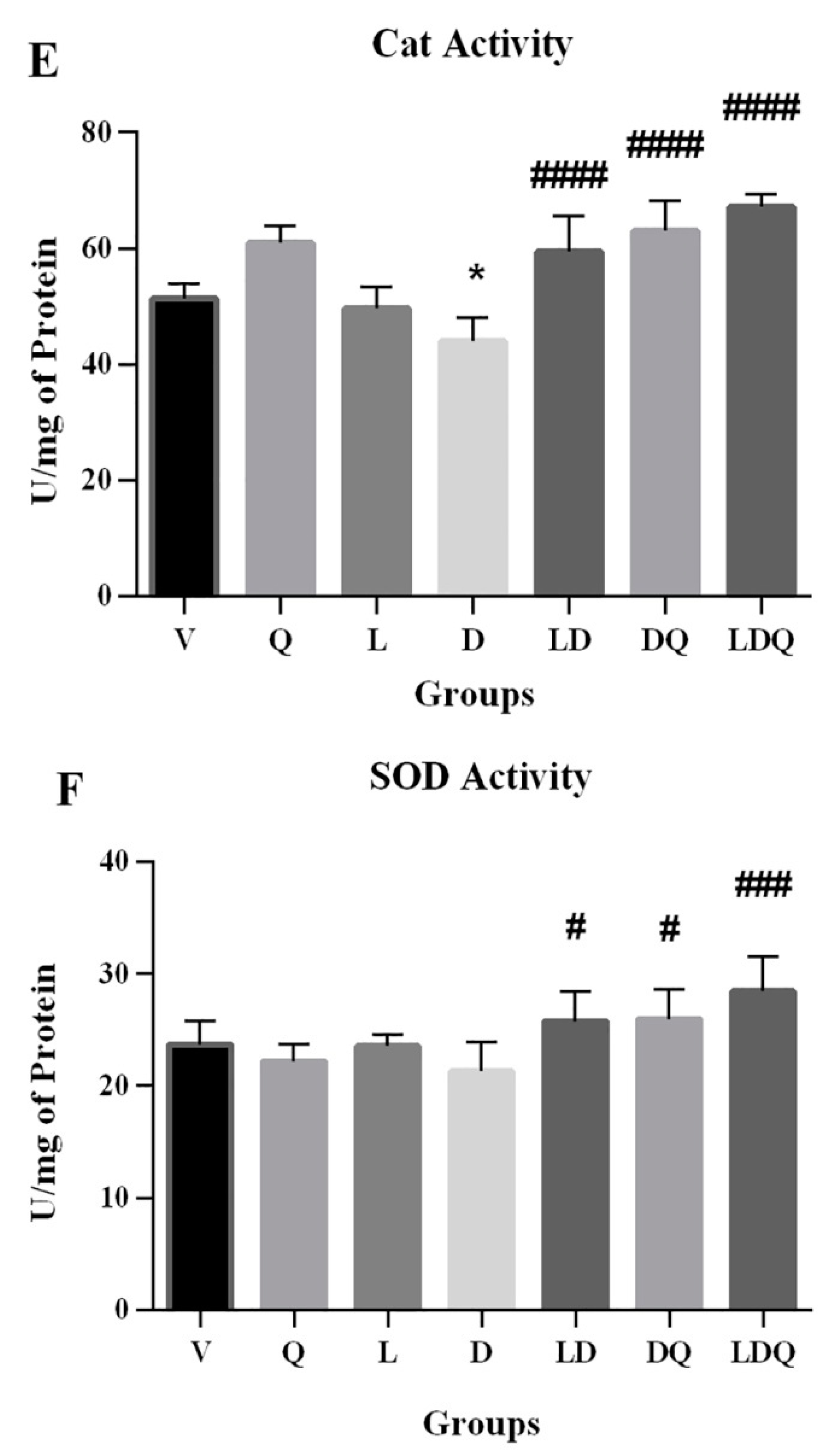
2.7. Analyzing the Activity of Antioxidant Enzymes and the Levels of Oxidative Stress
2.8. Western Blot Analysis
2.9. Histopathological Evaluations
2.10. In Vitro Cellular Uptake
2.11. Cytotoxicity Study
2.12. Statistical Analysis
3. Results and Discussion
3.1. Characteristics and Stability of Nanocarriers
3.2. Evaluation of Drug Release
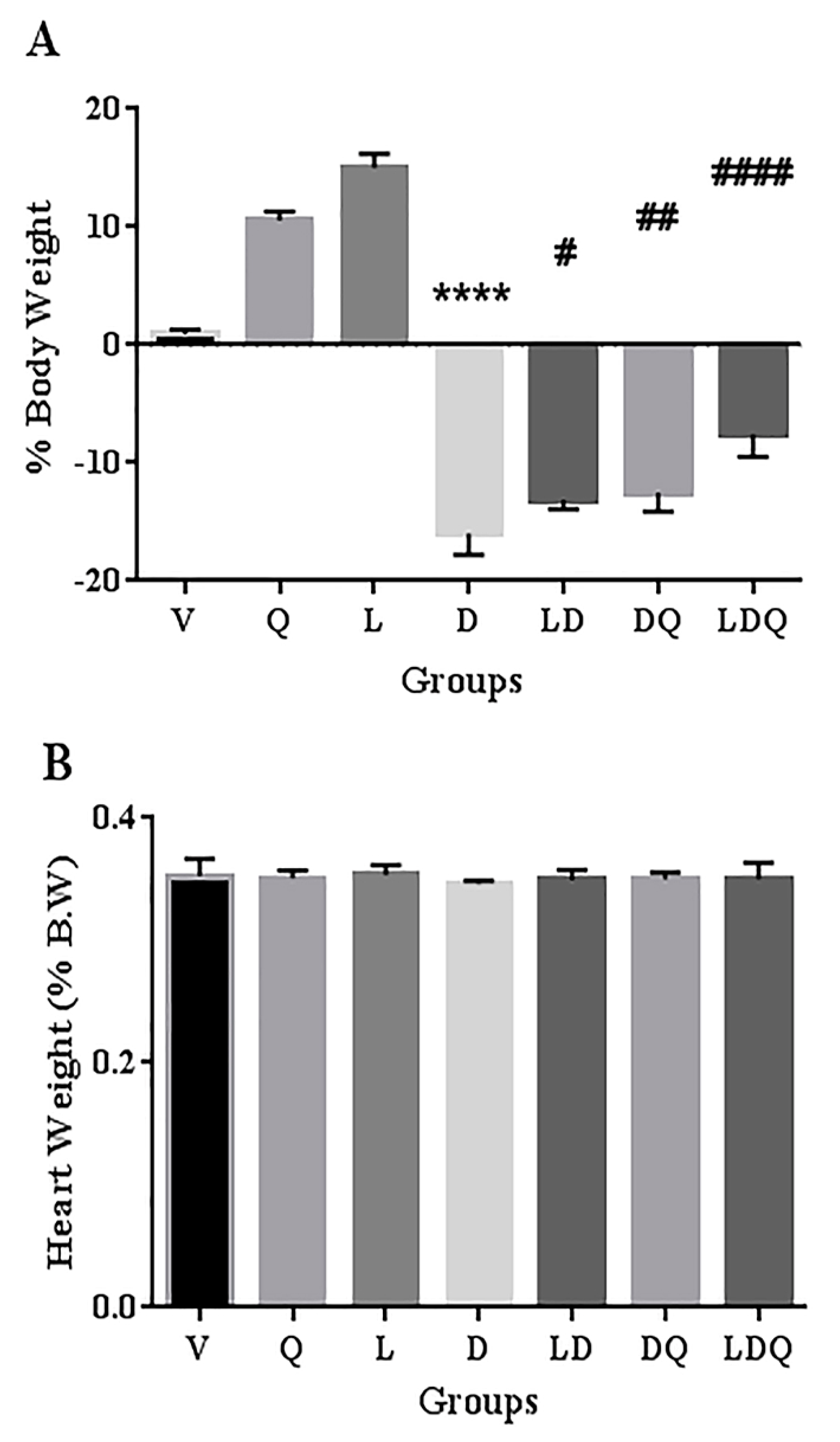
3.3. Animal Studies
3.4. Evaluation of Biochemical, Antioxidant, and Oxidative Stress Status
3.5. Expression of Proteins Involved in Oxidative Stress and Apoptosis
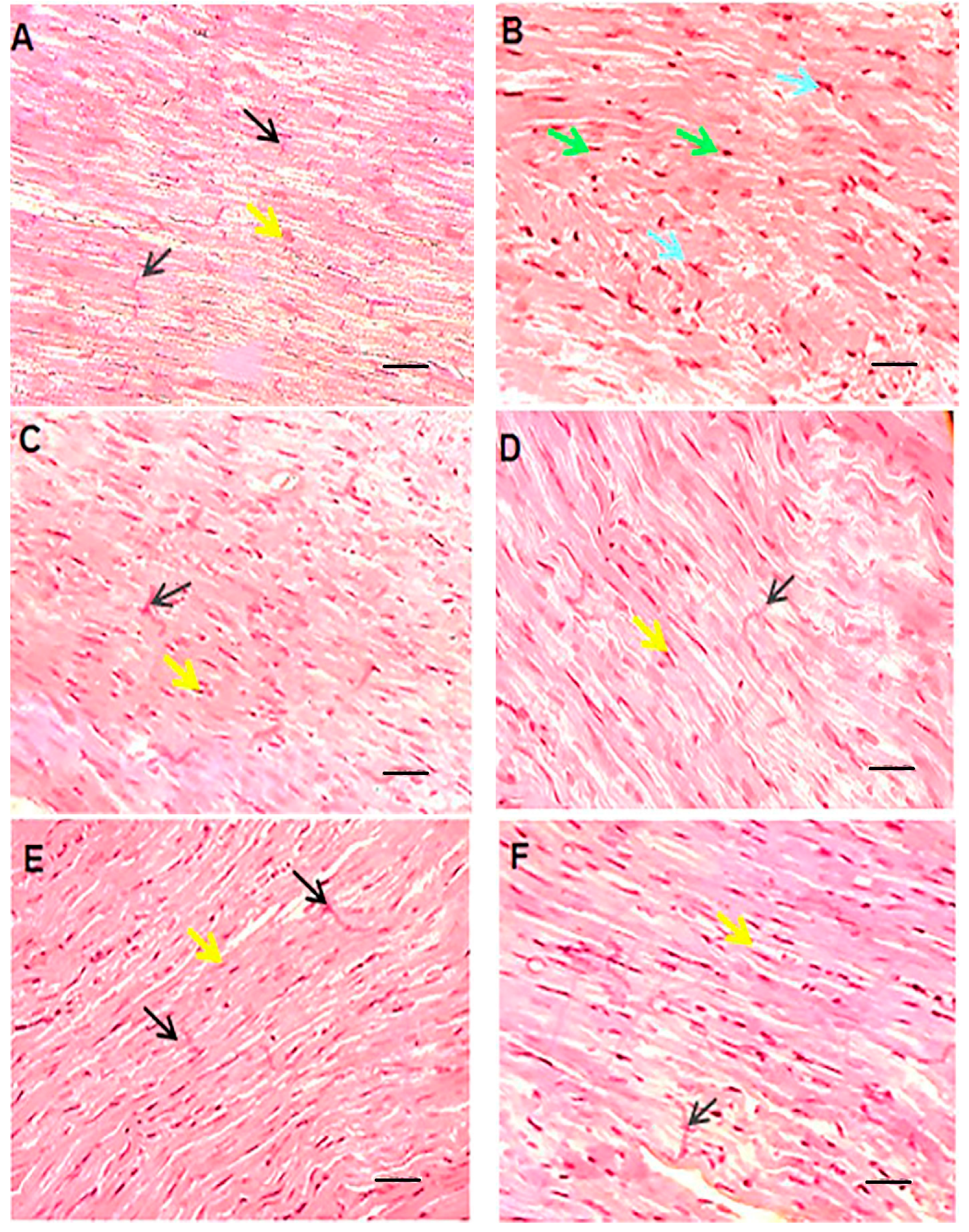
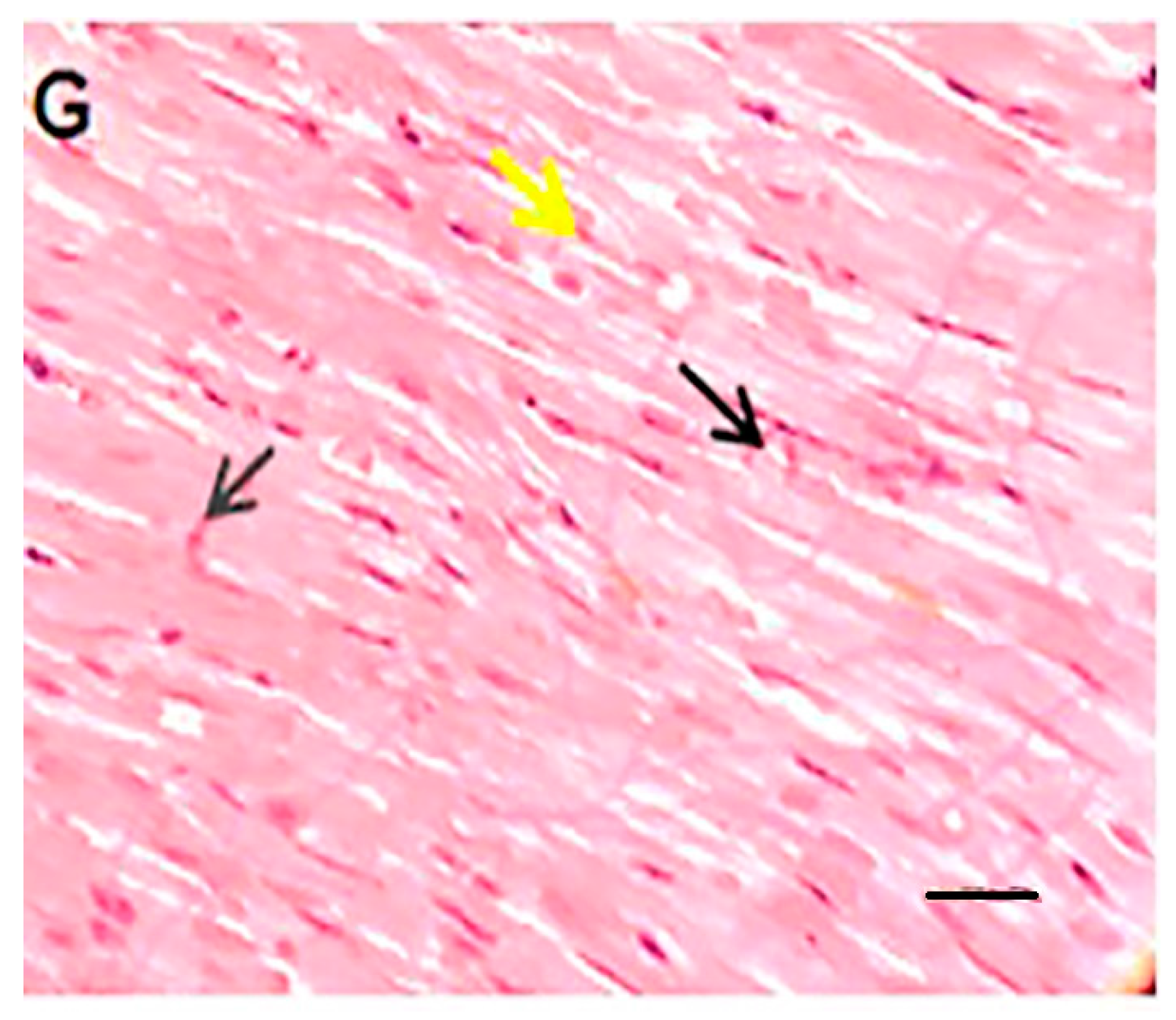
3.6. Histopathological Evaluations
3.7. Cellular Analysis, Uptake, and Cytotoxicity
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global cancer statistics, 2012. CA. Cancer J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [Green Version]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowland, J.H.; Yabroff, K.R.; Alfano, C.M.; Jemal, A.; Kramer, J.L.; Siegel, R.L. Cancer treatment and survivorship statistics, 2019. CA. Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [Green Version]
- Mohan, A.; Narayanan, S.; Balasubramanian, G.; Sethuraman, S.; Krishnan, U.M. Dual drug loaded nanoliposomal chemotherapy: A promising strategy for treatment of head and neck squamous cell carcinoma. Eur. J. Pharm. Biopharm. 2016, 99, 73–83. [Google Scholar] [CrossRef]
- Tatlidede, E.; Şehirli, Ö.; Velioğlu-Öğünç, A.; Çetinel, Ş.; Yeğen, B.Ç.; Yarat, A.; Süleymanoğlu, S.; Şener, G. Resveratrol treatment protects against doxorubicin-induced cardiotoxicity by alleviating oxidative damage. Free Radic. Res. 2009, 43, 195–205. [Google Scholar] [CrossRef]
- Aloss, K.; Hamar, P. Recent Preclinical and Clinical Progress in Liposomal Doxorubicin. Pharmaceutics 2023, 15, 893. [Google Scholar] [CrossRef] [PubMed]
- Mitry, M.A.; Edwards, J.G. Doxorubicin induced heart failure: Phenotype and molecular mechanisms. IJC Heart Vasc. 2016, 10, 17–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duarte, J.A.; Gomes, E.R.; De Barros, A.L.B.; Leite, E.A. Co-Encapsulation of Simvastatin and Doxorubicin into pH-Sensitive Liposomes Enhances Antitumoral Activity in Breast Cancer Cell Lines. Pharmaceutics 2023, 15, 369. [Google Scholar] [CrossRef]
- Caron, J.; Nohria, A. Cardiac toxicity from breast cancer treatment: Can we avoid this? Curr. Oncol. Rep 2018, 20, 61. [Google Scholar] [CrossRef]
- Octavia, Y.; Tocchetti, C.G.; Gabrielson, K.L.; Janssens, S.; Crijns, H.J.; Moens, A.L. Doxorubicin-induced cardiomyopathy: From molecular mechanisms to therapeutic strategies. J. Mol. Cell. Cardiol. 2012, 52, 1213–1225. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Q.; Needs, P.W.; Lu, Y.; Kroon, P.A.; Ren, D.; Yang, X. Different antitumor effects of quercetin, quercetin-3′-sulfate and quercetin-3-glucuronide in human breast cancer MCF-7 cells. Food Funct. 2018, 9, 1736–1746. [Google Scholar] [CrossRef] [PubMed]
- Rahmani, F.; Asar, N.; Najafizadeh, P.; Mousavi, S.Z.; Rastegar, T. Cardioprotective effects of quercetin on doxorubicin induced cardiotoxicity in male rats. Med. Sci. J. Islam. Azad Univesity-Tehran Med. Branch 2018, 28, 24–30. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.-M.; Zhang, Z.-Y.; Wang, R.-X. Protective mechanisms of quercetin against myocardial ischemia reperfusion injury. Front. Physiol. 2020, 11, 956. [Google Scholar] [CrossRef] [PubMed]
- Parvanian, S.; Mostafavi, S.M.; Aghashiri, M. Multifunctional nanoparticle developments in cancer diagnosis and treatment. Sens. Biosensing. Res. 2017, 13, 81–87. [Google Scholar] [CrossRef] [Green Version]
- Bulbake, U.; Doppalapudi, S.; Kommineni, N.; Khan, W. Liposomal formulations in clinical use: An updated review. Pharmaceutics 2017, 9, 12. [Google Scholar] [CrossRef]
- Lila, A.S.A.; Ishida, T. Liposomal delivery systems: Design optimization and current applications. Biol. Pharm. Bull. 2017, 40, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Cote, B.; Carlson, L.J.; Rao, D.A.; Alani, A.W. Combinatorial resveratrol and quercetin polymeric micelles mitigate doxorubicin induced cardiotoxicity in vitro and in vivo. J. Control. Release 2015, 213, 128–133. [Google Scholar] [CrossRef] [PubMed]
- Abo Elfadl, S.; Shendi, M.; Reda, A.; Abdelhaleem, A. Resveratrol pre-and post-treatment in doxorubicin-induced cardiac injury in relation to endogenous stem cell activation. J. Med. Histol. 2017, 1, 19–29. [Google Scholar] [CrossRef]
- Pouna, P.; Bonoron-Adèle, S.; Gouverneur, G.; Tariosse, L.; Besse, P.; Robert, J. Development of the model of rat isolated perfused heart for the evaluation of anthracycline cardiotoxicity and its circumvention. Br. J. Pharmacol. 1996, 117, 1593–1599. [Google Scholar] [CrossRef] [Green Version]
- Robert, J. Preclinical assessment of anthracycline cardiotoxicity in laboratory animals: Predictiveness and pitfalls. Cell Biol. Toxicol. 2007, 23, 27–37. [Google Scholar] [CrossRef]
- Zakaria, N.; Khalil, S.R.; Awad, A.; Khairy, G.M. Quercetin reverses altered energy metabolism in the heart of rats receiving adriamycin chemotherapy. Cardiovasc. Toxicol. 2018, 18, 109–119. [Google Scholar] [CrossRef]
- İkizler, M.; Erkasap, N.; Dernek, S.; Kural, T.; Kaygisiz, Z. Dietary polyphenol quercetin protects rat hearts during reperfusion: Enhanced antioxidant capacity with chronic treatment. Anadolu Kardiyol. Derg. 2007, 7, 404–410. [Google Scholar] [PubMed]
- Bin-Jaliah, I. Quercetin inhibits chronic stress-induced myocardial infarction in rats. Int. J. Morphol. 2017, 35, 1363–1369. [Google Scholar] [CrossRef] [Green Version]
- Li, M.; Jiang, Y.; Jing, W.; Sun, B.; Miao, C.; Ren, L. Quercetin provides greater cardioprotective effect than its glycoside derivative rutin on isoproterenol-induced cardiac fibrosis in the rat. Can. J. Physiol. Pharmacol. 2013, 91, 951–959. [Google Scholar] [CrossRef]
- Liu, H.; Zhang, L.; Lu, S. Evaluation of antioxidant and immunity activities of quercetin in isoproterenol-treated rats. Molecules 2012, 17, 4281–4291. [Google Scholar] [CrossRef] [Green Version]
- Bradford, M.M. A rapid and sensitive method for the quantitation of microgram quantities of protein utilizing the principle of protein-dye binding. Anal. Biochem. 1976, 72, 248–254. [Google Scholar] [CrossRef] [PubMed]
- Mozafari, M.R.; Reed, C.J.; Rostron, C. Prospects of anionic nanolipoplexes in nanotherapy: Transmission electron microscopy and light scattering studies. Micron 2007, 38, 787–795. [Google Scholar] [CrossRef] [PubMed]
- Mozafari, M.R.; Reed, C.; Rostron, C. Cytotoxicity evaluation of anionic nanoliposomes and nanolipoplexes prepared by the heating method without employing volatile solvents and detergents. Die Pharm.-Int. J. Pharm. Sci. 2007, 62, 205–209. [Google Scholar]
- Haghiralsadat, F.; Amoabediny, G.; Sheikhha, M.H.; Zandieh-doulabi, B.; Naderinezhad, S.; Helder, M.N.; Forouzanfar, T. New liposomal doxorubicin nanoformulation for osteosarcoma: Drug release kinetic study based on thermo and pH sensitivity. Chem. Biol. Drug Des. 2017, 90, 368–379. [Google Scholar] [CrossRef]
- Tefas, L.R.; Sylvester, B.; Tomuta, I.; Sesarman, A.; Licarete, E.; Banciu, M.; Porfire, A. Development of antiproliferative long-circulating liposomes co-encapsulating doxorubicin and curcumin, through the use of a quality-by-design approach. Drug Des. Devel. 2017, 11, 1605. [Google Scholar] [CrossRef] [Green Version]
- Park, T.; Amatya, R.; Min, K.A.; Shin, M.C. Liposomal Iron Oxide Nanoparticles Loaded with Doxorubicin for Combined Chemo-Photothermal Cancer Therapy. Pharmaceutics 2023, 15, 292. [Google Scholar] [CrossRef]
- Al-Rubaie, M.S.; Abdullah, T.S. Multi Lamellar Vesicles (Mlvs) Liposomes Preparation byThin Film Hydration Technique. Eng. Technol. J. 2014, 32, 550–560. [Google Scholar]
- dos Santos Ferreira, D.; Faria, S.D.; de Araújo Lopes, S.C.; Teixeira, C.S.; Malachias, A.; Magalhães-Paniago, R.; de Souza Filho, J.D.; Oliveira, B.L.d.J.P.; Guimarães, A.R.; Caravan, P. Development of a bone-targeted pH-sensitive liposomal formulation containing doxorubicin: Physicochemical characterization, cytotoxicity, and biodistribution evaluation in a mouse model of bone metastasis. Int. J. Nanomed. 2016, 11, 3737. [Google Scholar]
- Biabanikhankahdani, R.; Alitheen, N.B.M.; Ho, K.L.; Tan, W.S. pH-responsive virus-like nanoparticles with enhanced tumour-targeting ligands for cancer drug delivery. Sci. Rep. 2016, 6, 37891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, Q.; Ding, H.; Zhou, J.; Zhao, X.; Zhang, J.; Yang, C.; Li, K.; Qiao, M.; Hu, H.; Ding, P. Novel glycyrrhetinic acid conjugated pH-sensitive liposomes for the delivery of doxorubicin and its antitumor activities. RSC Adv. 2016, 6, 17782–17791. [Google Scholar] [CrossRef]
- Shaker, R.A.; Abboud, S.H.; Assad, H.C.; Hadi, N. Enoxaparin attenuates doxorubicin induced cardiotoxicity in rats via interfering with oxidative stress, inflammation and apoptosis. BMC Pharm. Toxicol. 2018, 19, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qureshi, W.A.; Zhao, R.; Wang, H.; Ji, T.; Ding, Y.; Ihsan, A.; Mujeeb, A.; Nie, G.; Zhao, Y. Co-delivery of doxorubicin and quercetin via mPEG–PLGA copolymer assembly for synergistic anti-tumor efficacy and reducing cardio-toxicity. Sci. Bull. 2016, 61, 1689–1698. [Google Scholar] [CrossRef] [Green Version]
- Paliwal, S.R.; Paliwal, R.; Pal, H.C.; Saxena, A.K.; Sharma, P.R.; Gupta, P.N.; Agrawal, G.P.; Vyas, S.P. Estrogen-anchored pH-sensitive liposomes as nanomodule designed for site-specific delivery of doxorubicin in breast cancer therapy. Mol. Pharm. 2012, 9, 176–186. [Google Scholar] [CrossRef]
- Matouk, A.I.; Taye, A.; Heeba, G.H.; El-Moselhy, M.A. Quercetin augments the protective effect of losartan against chronic doxorubicin cardiotoxicity in rats. Environ. Toxicol. Pharmacol. 2013, 36, 443–450. [Google Scholar] [CrossRef]
- Nazmi, A.S.; Ahmad, S.J.; Pillai, K.K.; Akhtar, M.; Ahmad, A.; Najmi, A.K. Protective effects of Bombyx mori, quercetin and benazepril against doxorubicin induced cardiotoxicity and nephrotoxicity. J. Saudi Chem. Soc. 2016, 20, S573–S578. [Google Scholar] [CrossRef] [Green Version]
- Iwata, K.; Matsuno, K.; Yabe-Nishimura, C. Reactive Oxygen Species Derived from the NOX1 Isoform of NADPH Oxidase Exacerbate Doxorubicin-Induced Cardiotoxicity by Promoting Cardiac Remodeling. Free Radic. Biol. Med. 2016, 100, S144. [Google Scholar] [CrossRef]
- Tsutsui, H.; Ide, T.; Kinugawa, S. Mitochondrial oxidative stress, DNA damage, and heart failure. Antioxid. Redox Signal. 2006, 8, 1737–1744. [Google Scholar] [CrossRef]
- Ma, J.; Wang, Y.; Zheng, D.; Wei, M.; Xu, H.; Peng, T. Rac1 signalling mediates doxorubicin-induced cardiotoxicity through both reactive oxygen species-dependent and-independent pathways. Cardiovasc. Res. 2013, 97, 77–87. [Google Scholar] [CrossRef] [Green Version]
- Henninger, C.; Fritz, G. Statins in anthracycline-induced cardiotoxicity: Rac and Rho, and the heartbreakers. Cell Death Dis. 2018, 8, e2564. [Google Scholar] [CrossRef] [Green Version]
- Dong, Q.; Chen, L.; Lu, Q.; Sharma, S.; Li, L.; Morimoto, S.; Wang, G. Quercetin attenuates doxorubicin cardiotoxicity by modulating B mi-1 expression. Br. J. Pharmacol. 2014, 171, 4440–4454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, K.G.; Cole, L.K.; Xiang, B.; Chen, K.; Ma, X.; Myal, Y.; Hatch, G.M.; Tong, Q.; Dolinsky, V.W. Sirtuin-3 (SIRT3) protein attenuates doxorubicin-induced oxidative stress and improves mitochondrial respiration in H9c2 cardiomyocytes. J. Biol. Chem. 2015, 290, 10981–10993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, Q.; Zhu, B.; Zhai, Q.; Yu, B. Sirt3 attenuates doxorubicin-induced cardiac hypertrophy and mitochondrial dysfunction via suppression of Bnip3. Am. J. Transl. Res. 2017, 9, 3360. [Google Scholar] [PubMed]
- Saad, S.Y.; Najjar, T.A.; Alashari, M. Cardiotoxicity of doxorubicin/paclitaxel combination in rats: Effect of sequence and timing of administration. J. Biochem. Mol. Toxicol. 2004, 18, 78–86. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Lu, X.; Liu, Q.; Dai, Y.; Zhu, X.; Wen, Y.; Xu, J.; Lu, Y.; Zhao, D.; Chen, X. Palmitoyl ascorbate and doxorubicin co-encapsulated liposome for synergistic anticancer therapy. Eur. J. Pharm. Sci. 2017, 105, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Hemati, M.; Haghiralsadat, F.; Yazdian, F.; Jafari, F.; Moradi, A.; Malekpour-Dehkordi, Z. Development and characterization of a novel cationic PEGylated niosome-encapsulated forms of doxorubicin, quercetin and siRNA for the treatment of cancer by using combination therapy. Artif. Cells Nanomed. Biotechnol. 2019, 47, 1295–1311. [Google Scholar] [CrossRef] [Green Version]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Gavage (Everyday) | Injections (Every Other Day) |
|---|---|---|
| V | Normal saline | Phosphate-buffered saline |
| Q | Quercetin | Phosphate-buffered saline |
| L | Normal saline | Blank liposome |
| D | Normal saline | Doxorubicin |
| LD | Normal saline | Liposomal doxorubicin |
| DQ | Quercetin | Doxorubicin |
| LDQ | Quercetin | Liposomal doxorubicin |
| Liposome Type | Particle Size (nm) | PDI | Zeta Potential (mV) |
|---|---|---|---|
| Empty liposome | 96.3 ± 2.2 | 0.189 ± 0.02 | −19.3 ± 1.5 |
| Liposomal doxorubicin | 98.8 ± 2.5 | 0.204 ± 0.03 | −18.1 ± 2.2 |
| Stored liposomal doxorubicin p-value | 101.9 ± 3.1 0.10 | 0.222 ± 0.03 0.42 | −21.4 ± 2.6 0.24 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dorostkar, H.; Haghiralsadat, B.F.; Hemati, M.; Safari, F.; Hassanpour, A.; Naghib, S.M.; Roozbahani, M.H.; Mozafari, M.R.; Moradi, A. Reduction of Doxorubicin-Induced Cardiotoxicity by Co-Administration of Smart Liposomal Doxorubicin and Free Quercetin: In Vitro and In Vivo Studies. Pharmaceutics 2023, 15, 1920. https://doi.org/10.3390/pharmaceutics15071920
Dorostkar H, Haghiralsadat BF, Hemati M, Safari F, Hassanpour A, Naghib SM, Roozbahani MH, Mozafari MR, Moradi A. Reduction of Doxorubicin-Induced Cardiotoxicity by Co-Administration of Smart Liposomal Doxorubicin and Free Quercetin: In Vitro and In Vivo Studies. Pharmaceutics. 2023; 15(7):1920. https://doi.org/10.3390/pharmaceutics15071920
Chicago/Turabian StyleDorostkar, Hamidreza, Bibi Fatemeh Haghiralsadat, Mahdie Hemati, Fatemeh Safari, Azam Hassanpour, Seyed Morteza Naghib, Mohammad Hossein Roozbahani, M. R. Mozafari, and Ali Moradi. 2023. "Reduction of Doxorubicin-Induced Cardiotoxicity by Co-Administration of Smart Liposomal Doxorubicin and Free Quercetin: In Vitro and In Vivo Studies" Pharmaceutics 15, no. 7: 1920. https://doi.org/10.3390/pharmaceutics15071920