
Development of Thermoresponsive Hydrogels with Mucoadhesion Properties Loaded with Metronidazole Gel-Flakes for Improved Bacterial Vaginosis Treatment
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Formulation of Metronidazole-Loaded Gel Flakes
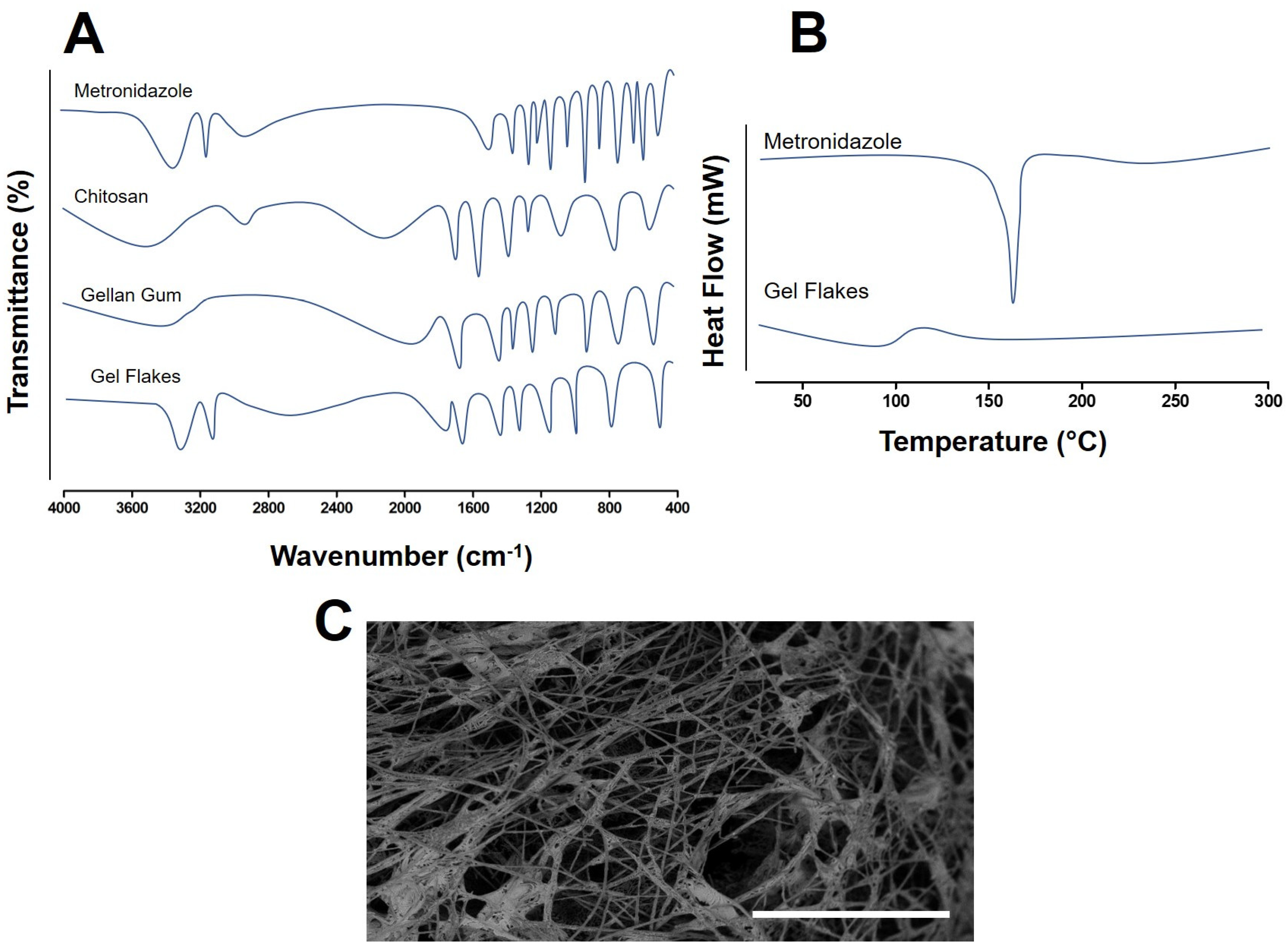
2.3. Characterization of Metronidazole-Loaded Gel Flakes
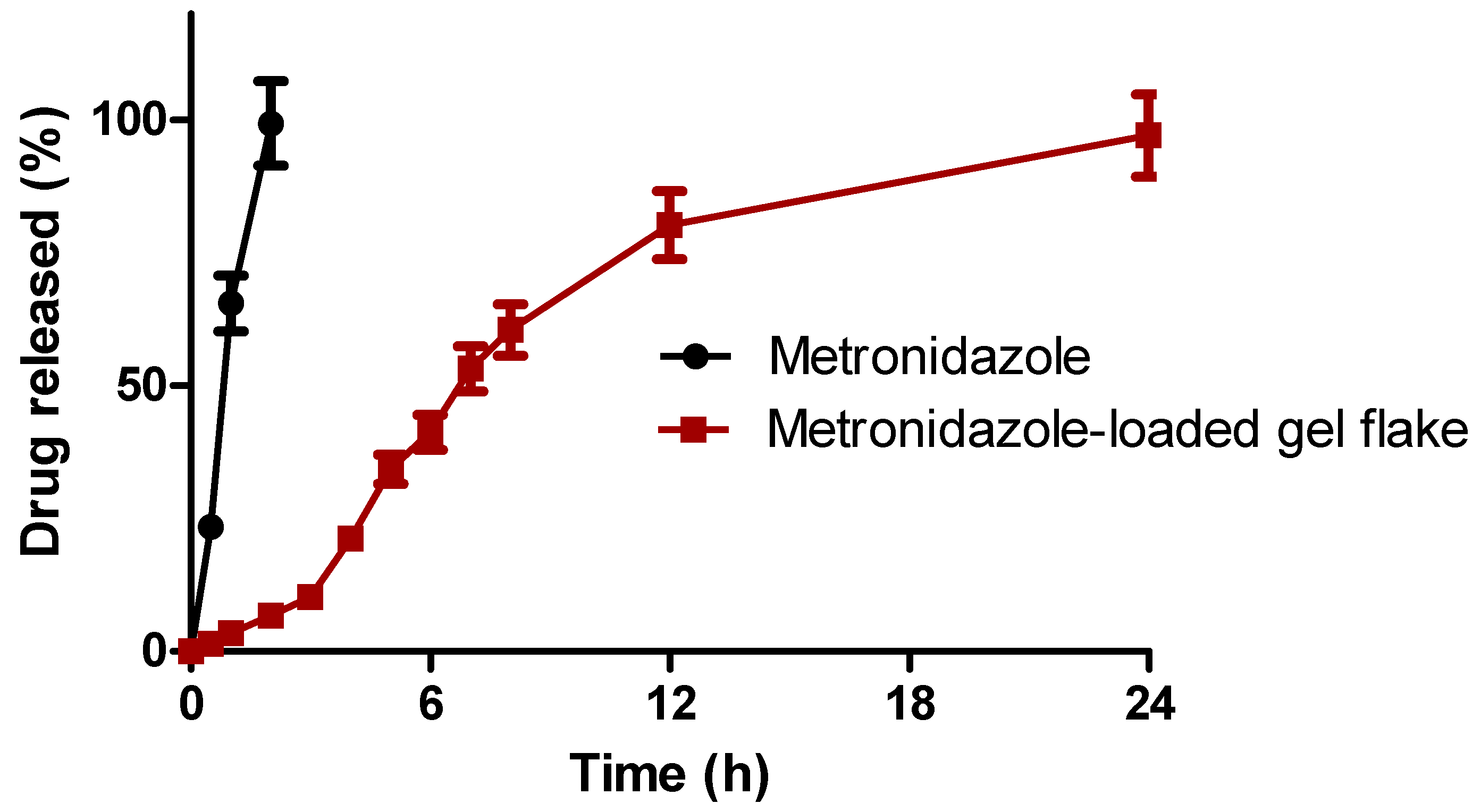
2.4. In Vitro Release Studies of Metronidazole from a Gel Flakes Formulation
2.5. Preparation of Mucoadhesive-Thermoresponsive In Situ Hydrogel Containing Metronidazole Gel Flakes
2.6. Characterization of Mucoadhesive-Thermoresponsive In Situ Hydrogel Containing Metronidazole Gel Flakes
2.6.1. The Determination of Gelation Temperature (Tsol-gel)
2.6.2. Mucoadhesion Strength
2.6.3. Mucoadhesion Time
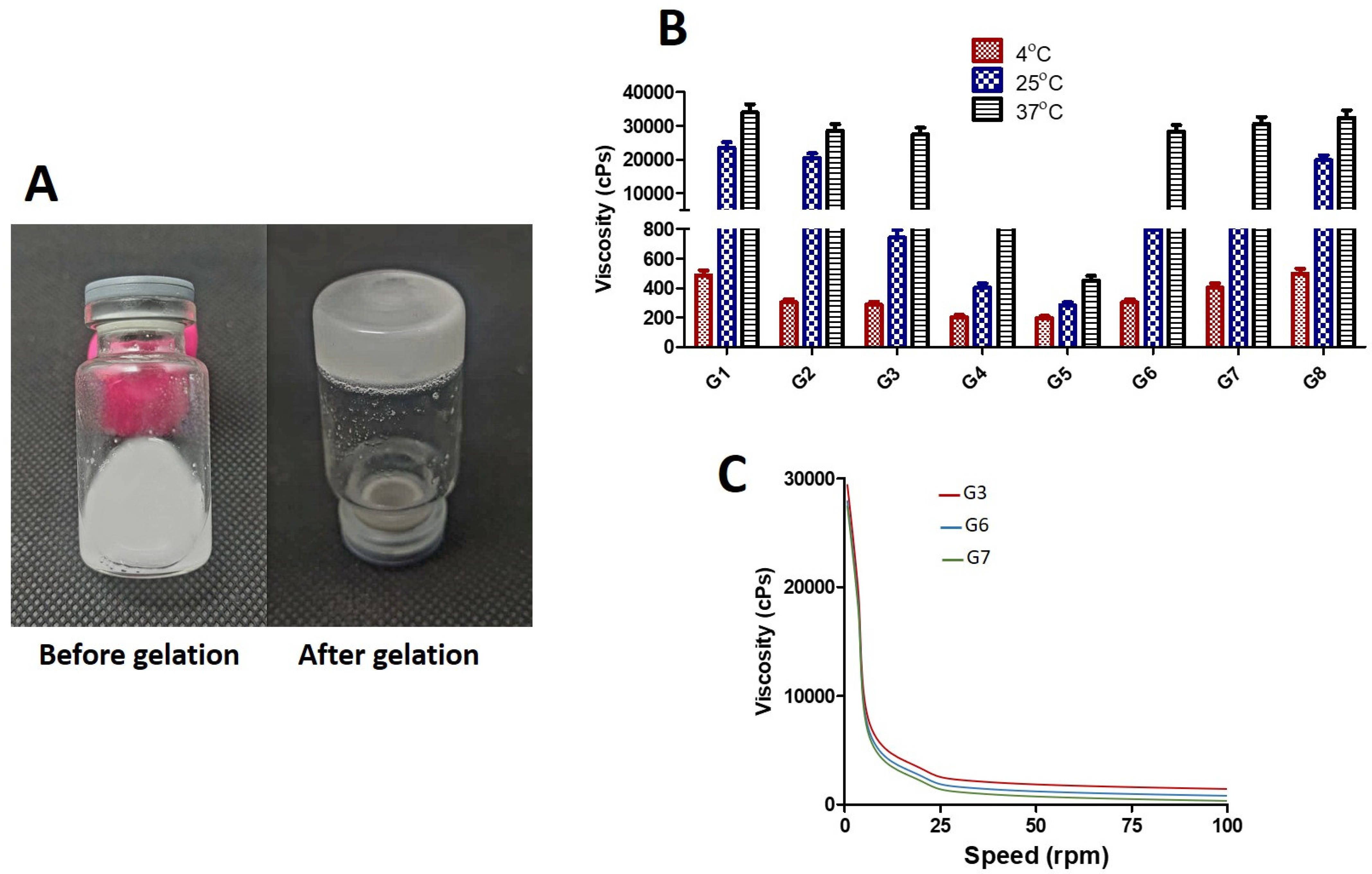
2.6.4. Investigation of Viscosity and Rheological Properties
2.6.5. Determination of pH and Drug Content Analysis
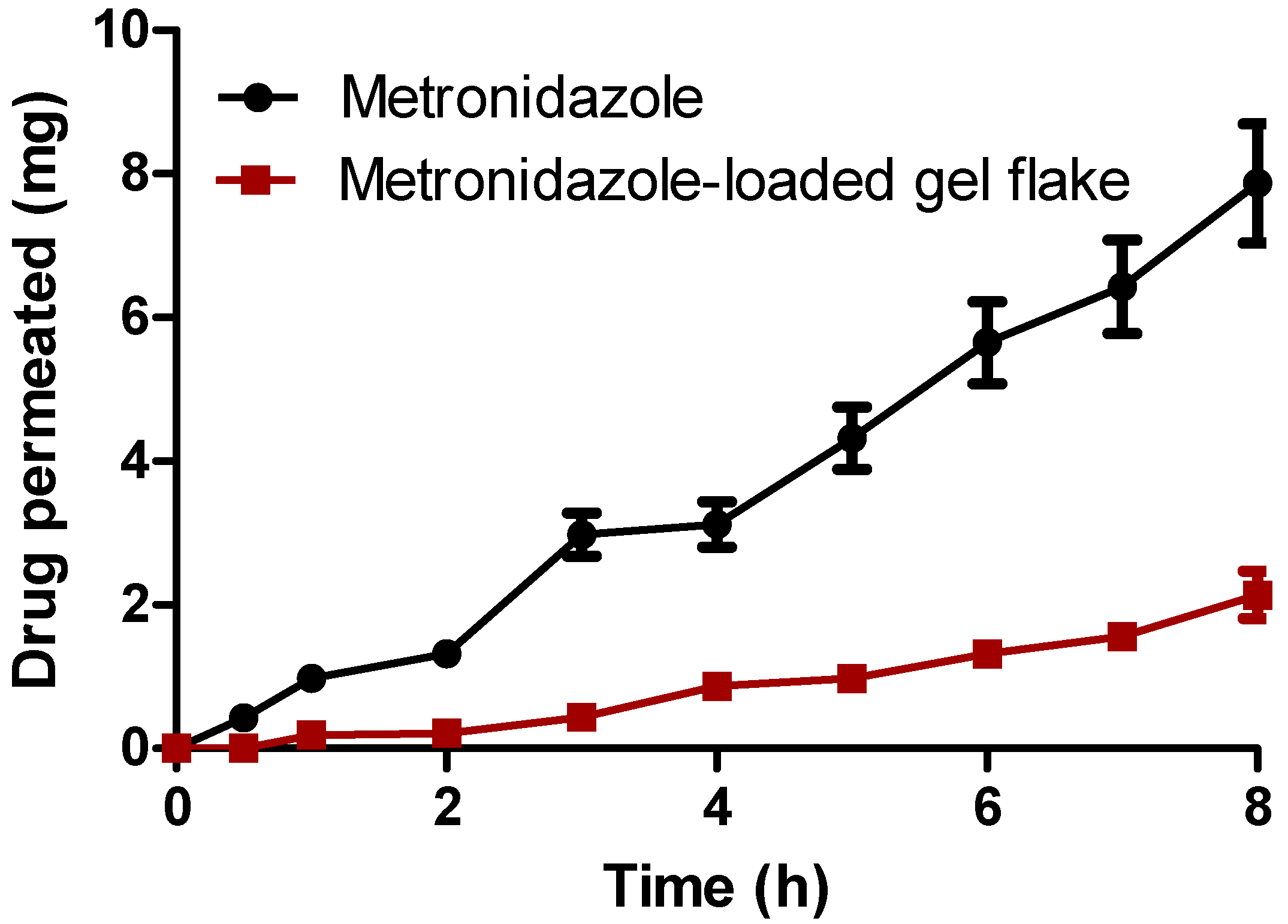
2.7. Ex Vivo Permeation Studies
2.8. Ex Vivo Retention Determination
2.9. In Vivo Antibacterial Activity in Model of Infection on Rat
2.9.1. Preparation of Bacterial Vaginosis Model on Rat
2.9.2. In Vivo Antibacterial Activity and Histopathology Evaluation
2.10. Statistical Analysis
3. Results and Discussion
3.1. Formulation and Characterization of Metronidazole Loaded Gel Flakes
3.2. In Vitro Release Studies of Metronidazole from Gel Flakes Formulation
3.3. Formulation and Characterization of Mucoadhesive-Thermoresponsive In Situ Hydrogel Containing Metronidazole Gel Flakes
3.3.1. Results of Gelation Temperature (Tsol-gel) Determination
3.3.2. Results of Mucoadhesion Strength and Mucoadhesion Time Determination
3.3.3. Viscosity and Rheological Study
3.3.4. pH Measurement and Drug Content Analysis
3.4. Ex Vivo Permeation Studies
3.5. Ex Vivo Retention Determination
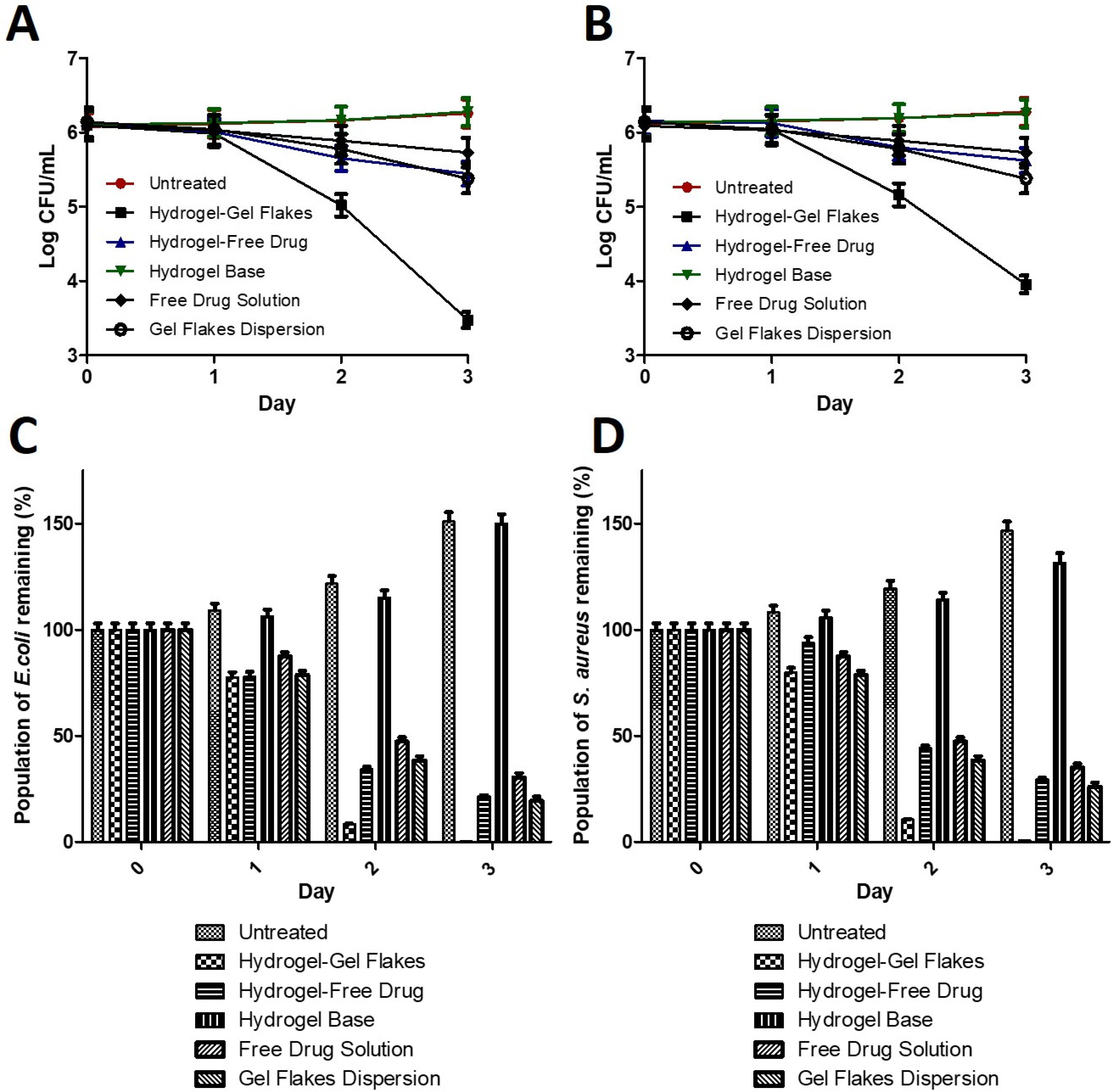
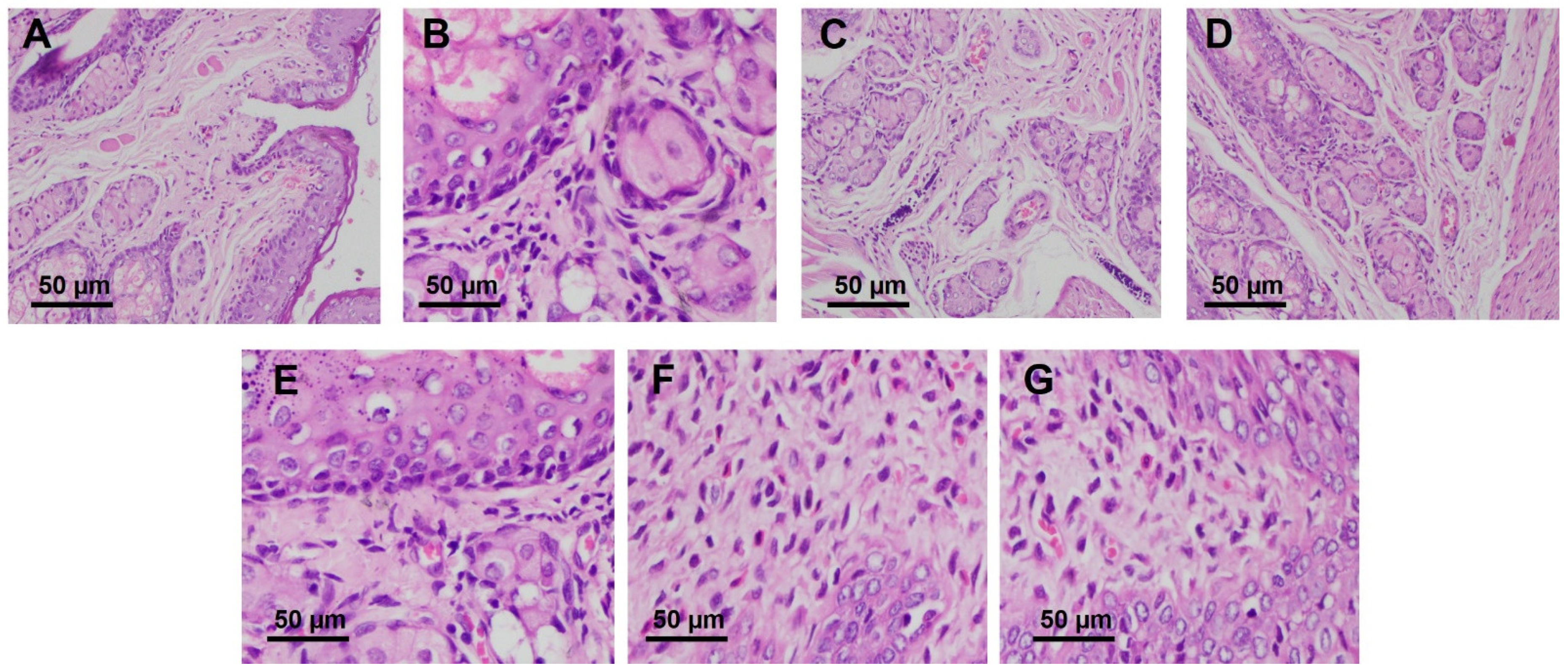
3.6. In Vivo Antibacterial Activity and Histopathology Evaluation in Model of Infection on Rat
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Utomo, E.; Domínguez-Robles, J.; Anjani, Q.K.; Picco, C.J.; Korelidou, A.; Magee, E.; Donnelly, R.F.; Larrañeta, E. Development of 3D-Printed Vaginal Devices Containing Metronidazole for Alternative Bacterial Vaginosis Treatment. Int. J. Pharm. X 2023, 5, 100142. [Google Scholar] [CrossRef] [PubMed]
- Singh, V.K.; Anis, A.; Banerjee, I.; Pramanik, K.; Bhattacharya, M.K.; Pal, K. Preparation and Characterization of Novel Carbopol Based Bigels for Topical Delivery of Metronidazole for the Treatment of Bacterial Vaginosis. Mater. Sci. Eng. C 2014, 44, 151–158. [Google Scholar] [CrossRef]
- Chen, L.; Liu, R.; Li, S.; Wu, M.; Yu, H.; Ge, Q. Metabolism of Hydrogen Peroxide by Lactobacillus Plantarum NJAU-01: A Proteomics Study. Food Microbiol. 2023, 112, 104246. [Google Scholar] [CrossRef] [PubMed]
- Persaud, K.C.; Pisanelli, A.M.; Evans, P.; Travers, P.J. Monitoring Urinary Tract Infections and Bacterial Vaginosis. Sens. Actuators B Chem. 2006, 116, 116–120. [Google Scholar] [CrossRef]
- Loquet, A.; Le Guern, R.; Grandjean, T.; Duployez, C.; Bauduin, M.; Kipnis, E.; Brabant, G.; Subtil, D.; Dessein, R. Classification and Regression Trees for Bacterial Vaginosis Diagnosis in Pregnant Women Based on High-Throughput Quantitative PCR. J. Mol. Diagn. 2021, 23, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Baig, K.; Sultana, A.; Rahman, K. A Randomized Comparative Study of Kakrasingi (Pistacia Integerrima J. L. Stewart Ex Brandis) and Metronidazole in Bacterial Vaginosis. J. Herb. Med. 2022, 36, 100609. [Google Scholar] [CrossRef]
- Mohammad-Alizadeh-Charandabi, S.; Mohammadzadeh, Z.; Farshbaf-Khalili, A.; Javadzadeh, Y. Effect of Hypericum perforatum L. Compared with Metronidazole in Bacterial Vaginosis: A Double-Blind Randomized Trial. Asian Pac. J. Trop. Biomed. 2014, 4, 896–902. [Google Scholar] [CrossRef]
- Schwebke, J.R.; Desmond, R.A. Tinidazole vs Metronidazole for the Treatment of Bacterial Vaginosis. Am. J. Obstet. Gynecol. 2011, 204, 211.e1–211.e6. [Google Scholar] [CrossRef]
- Sobel, J.D.; Ferris, D.; Schwebke, J.; Nyirjesy, P.; Wiesenfeld, H.C.; Peipert, J.; Soper, D.; Ohmit, S.E.; Hillier, S.L. Suppressive Antibacterial Therapy with 0.75% Metronidazole Vaginal Gel to Prevent Recurrent Bacterial Vaginosis. Am. J. Obstet. Gynecol. 2006, 194, 1283–1289. [Google Scholar] [CrossRef]
- Goje, O.; Shay, E.O.; Markwei, M.; Padmanabhan, R.; Eng, C. The Effect of Oral Metronidazole on the Vaginal Microbiome of Patients with Recurrent Bacterial Vaginosis: A Pilot Investigational Study. Hum. Microbiome J. 2021, 20, 100081. [Google Scholar] [CrossRef]
- Badawi, N.M.; Elkafrawy, M.A.; Yehia, R.M.; Attia, D.A. Clinical Comparative Study of Optimized Metronidazole Loaded Lipid Nanocarrier Vaginal Emulgel for Management of Bacterial Vaginosis and Its Recurrence. Drug Deliv. 2021, 28, 814–825. [Google Scholar] [CrossRef] [PubMed]
- Herold, S.E.; Kyser, A.J.; Orr, M.G.; Mahmoud, M.Y.; Lewis, W.G.; Lewis, A.L.; Steinbach-Rankins, J.M.; Frieboes, H.B. Release Kinetics of Metronidazole from 3D Printed Silicone Scaffolds for Sustained Application to the Female Reproductive Tract. Biomed. Eng. Adv. 2023, 5, 100078. [Google Scholar] [CrossRef] [PubMed]
- Ilomuanya, M.O.; Salako, B.B.; Ologunagba, M.O.; Shonekan, O.O.; Owodeha-Ashaka, K.; Osahon, E.S.; Amenaghawon, A.N. Formulation and Optimization of Metronidazole and Lactobacillus Spp. Layered Suppositories via a Three-Variable, Five-Level Central Composite Design for the Management of Bacterial Vaginosis. Pharmaceutics 2022, 14, 2337. [Google Scholar] [CrossRef] [PubMed]
- Voorspoels, J.; Casteels, M.; Remon, J.P.; Temmerman, M. Local Treatment of Bacterial Vaginosis with a Bioadhesive Metronidazole Tablet. Eur. J. Obstet. Gynecol. Reprod. Biol. 2002, 105, 64–66. [Google Scholar] [CrossRef]
- Patil, P.B.; Datir, S.K.; Saudagar, R.B. A Review on Topical Gels as Drug Delivery System. J. Drug Deliv. Ther. 2019, 9, 989–994. [Google Scholar]
- Permana, A.D.; Nurul, R.; Layadi, P.; Himawan, A.; Juniarti, N.; Kurnia, Q.; Utomo, E.; Aulia, S.; Arjuna, A.; Donnelly, R.F. Thermosensitive and Mucoadhesive in Situ Ocular Gel for Effective Local Delivery and Antifungal Activity of Itraconazole Nanocrystal in the Treatment of Fungal Keratitis. Int. J. Pharm. 2021, 602, 120623. [Google Scholar] [CrossRef]
- Soliman, G.M.; Fetih, G.; Abbas, M.A. Thermosensitive Bioadhesive Gels for The Vaginal Delivery of Sildenafil Citrate. In In Vitro Characterization and Clinical Evaluation in Women Using Clomphene Citrate for Induction of Ovulation; Taylor & Francis: Abingdon, UK, 2016; ISBN 2010134273. [Google Scholar]
- Argenta, D.F.; da Bernardo, B.C.; Chamorro, A.F.; Matos, P.R.; Caon, T. Thermosensitive Hydrogels for Vaginal Delivery of Secnidazole as an Approach to Overcome the Systemic Side-Effects of Oral Preparations. Eur. J. Pharm. Sci. 2021, 159, 105722. [Google Scholar] [CrossRef]
- Sulistiawati; Enggi, C.K.; Isa, H.T.; Wijaya, S.; Ardika, K.A.R.; Asri, R.M.; Donnelly, R.F.; Permana, A.D. Validation of Spectrophotometric Method to Quantify Cabotegravir in Simulated Vaginal Fluid and Porcine Vaginal Tissue in Ex Vivo Permeation and Retention Studies from Thermosensitive and Mucoadhesive Gels. Spectrochim. Acta Part A Mol. Biomol. Spectrosc. 2021, 267, 120600. [Google Scholar] [CrossRef]
- Enggi, C.K.; Isa, H.T.; Sulistiawati, S.; Ardika, K.A.R.; Wijaya, S.; Asri, R.M.; Mardikasari, S.A.; Donnelly, R.F.; Permana, A.D. Development of Thermosensitive and Mucoadhesive Gels of Cabotegravir for Enhanced Permeation and Retention Profiles in Vaginal Tissue: A Proof of Concept Study. Int. J. Pharm. 2021, 609, 121182. [Google Scholar] [CrossRef]
- Bouchemal, K.; Frelichowska, J.; Martin, L.; Lievin-Le Moal, V.; Le Grand, R.; Dereuddre-Bosquet, N.; Djabourov, M.; Aka-Any-Grah, A.; Koffi, A.; Ponchel, G. Note on the Formulation of Thermosensitive and Mucoadhesive Vaginal Hydrogels Containing the MiniCD4 M48U1 as Anti-HIV-1 Microbicide. Int. J. Pharm. 2013, 454, 649–652. [Google Scholar] [CrossRef]
- Yun Chang, J.; Oh, Y.K.; Soo Kong, H.; Jung Kim, E.; Deuk Jang, D.; Taek Nam, K.; Kim, C.K. Prolonged Antifungal Effects of Clotrimazole-Containing Mucoadhesive Thermosensitive Gels on Vaginitis. J. Control. Release 2002, 82, 39–50. [Google Scholar] [CrossRef] [PubMed]
- Mirza, M.A.; Ahmad, S.; Mallick, M.N.; Manzoor, N.; Talegaonkar, S.; Iqbal, Z. Development of a Novel Synergistic Thermosensitive Gel for Vaginal Candidiasis: An in Vitro, in Vivo Evaluation. Colloids Surf. B Biointerfaces 2013, 103, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Taurin, S.; Almomen, A.A.; Pollak, T.; Kim, S.J.; Maxwell, J.; Peterson, C.M.; Owen, S.C.; Janát-Amsbury, M.M. Thermosensitive Hydrogels a Versatile Concept Adapted to Vaginal Drug Delivery. J. Drug Target. 2018, 26, 533–550. [Google Scholar] [CrossRef]
- Deshkar, S.S.; Palve, V.K. Formulation and Development of Thermosensitive Cyclodextrin-Based in Situ Gel of Voriconazole for Vaginal Delivery. J. Drug Deliv. Sci. Technol. 2019, 49, 277–285. [Google Scholar] [CrossRef]
- Permana, A.D.; Utomo, E.; Pratama, M.R.; Amir, M.N.; Anjani, Q.K.; Mardikasari, S.A.; Sumarheni, S.; Himawan, A.; Arjuna, A.; Usmanengsi, U.; et al. Bioadhesive-Thermosensitive in Situ Vaginal Gel of the Gel Flake-Solid Dispersion of Itraconazole for Enhanced Antifungal Activity in the Treatment of Vaginal Candidiasis. ACS Appl. Mater. Interfaces 2021, 13, 18128–18141. [Google Scholar] [CrossRef]
- Abd Ellah, N.H.; Abdel-Aleem, J.A.; Abdo, M.N.; Abou-Ghadir, O.F.; Zahran, K.M.; Hetta, H.F. Efficacy of Ketoconazole Gel-Flakes in Treatment of Vaginal Candidiasis: Formulation, in Vitro and Clinical Evaluation. Int. J. Pharm. 2019, 567, 118472. [Google Scholar] [CrossRef] [PubMed]
- Russo, E.; Villa, C. Poloxamer Hydrogels for Biomedical Applications. Pharmaceutics 2019, 11, 671. [Google Scholar] [CrossRef]
- Tuğcu-Demiröz, F. Development of in Situ Poloxamer-Chitosan Hydrogels for Vaginal Drug Delivery of Benzydamine Hydrochloride: Textural, Mucoadhesive and in Vitro Release Properties. Marmara Pharm. J. 2017, 21, 762–770. [Google Scholar] [CrossRef]
- Al Fiqri, M.; Athiyyah, U.; Fadjar, T.G.A.; Nainu, F.; Arjuna, A.; Permana, A.D. Validation of Spectrophotometric Method for Quantification of Cefazoline in Simulated Tear Fluid and Porcine Ocular Tissue from Thermosensitive-Mucoadhesive in Situ Ocular Gel Preparation. Chem. Data Collect. 2021, 36, 100793. [Google Scholar] [CrossRef]
- Choi, S.G.; Lee, S.; Kang, B.; Ng, C.L.; Davaa, E.; Park, J. Thermosensitive and Mucoadhesive Sol-Gel Composites of Paclitaxel / Dimethyl- b -Cyclodextrin for Buccal Delivery. PLoS ONE 2014, 9, e0109090. [Google Scholar] [CrossRef]
- Cunha, S.; Swedrowska, M.; Bellahnid, Y.; Xu, Z.; Sousa Lobo, J.M.; Forbes, B.; Silva, A.C. Thermosensitive in Situ Hydrogels of Rivastigmine-Loaded Lipid-Based Nanosystems for Nose-to-Brain Delivery: Characterisation, Biocompatibility, and Drug Deposition Studies. Int. J. Pharm. 2022, 620, 121720. [Google Scholar] [CrossRef] [PubMed]
- Permana, A.D.; Mir, M.; Utomo, E.; Donnelly, R.F. Bacterially Sensitive Nanoparticle-Based Dissolving Microneedles of Doxycycline for Enhanced Treatment of Bacterial Biofilm Skin Infection: A Proof of Concept Study. Int. J. Pharm. X 2020, 2, 100047. [Google Scholar] [CrossRef]
- Permana, A.D.; McCrudden, M.T.C.; Donnelly, R.F. Enhanced Intradermal Delivery of Nanosuspensions of Antifilariasis Drugs Using Dissolving Microneedles: A Proof of Concept Study. Pharmaceutics 2019, 11, 346. [Google Scholar] [CrossRef] [PubMed]
- Mo, F.; Ma, J.; Yang, X.; Zhang, P.; Li, Q.; Zhang, J. In Vitro and in Vivo Effects of the Combination of Myricetin and Miconazole Nitrate Incorporated to Thermosensitive Hydrogels, on C. Albicans Biofilms. Phytomedicine 2020, 71, 153223. [Google Scholar] [CrossRef]
- Morsi, N.; Ghorab, D.; Refai, H.; Teba, H. Ketoroloac Tromethamine Loaded Nanodispersion Incorporated into Thermosensitive in Situ Gel for Prolonged Ocular Delivery. Int. J. Pharm. 2016, 506, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Sanz, R.; Clares, B.; Mallandrich, M.; Suñer-Carbó, J.; Montes, M.J.; Calpena, A.C. Development of a Mucoadhesive Delivery System for Control Release of Doxepin with Application in Vaginal Pain Relief Associated with Gynecological Surgery. Int. J. Pharm. 2018, 535, 393–401. [Google Scholar] [CrossRef]
- Zhang, M.; Zhuang, B.; Du, G.; Han, G.; Jin, Y. Curcumin Solid Dispersion-Loaded in Situ Hydrogels for Local Treatment of Injured Vaginal Bacterial Infection and Improvement of Vaginal Wound Healing. J. Pharm. Pharmacol. 2019, 71, 1044–1054. [Google Scholar] [CrossRef]
- Iyer, R.; Jovanovska, V.P.; Berginc, K.; Jaklič, M.; Fabiani, F.; Harlacher, C.; Huzjak, T.; Sanchez-Felix, M.V. Amorphous Solid Dispersions (ASDs): The Influence of Material Properties, Manufacturing Processes and Analytical Technologies in Drug Product Development. Pharmaceutics 2021, 13, 1682. [Google Scholar] [CrossRef]
- Chatterjee, B.; Amalina, N.; Sengupta, P.; Mandal, U.K. Mucoadhesive Polymers and Their Mode of Action: A Recent Update. J. Appl. Pharm. Sci. 2017, 7, 195–203. [Google Scholar] [CrossRef]
- Deshkar, S.S.; Patil, A.T.; Poddar, S.S. Development of Thermosensitive Gel of Fluconazole for Vaginal Candidiasis. Int. J. Pharm. Pharm. Sci. 2016, 8, 391–398. [Google Scholar]
- Bai, L.; Lei, F.; Luo, R.; Fei, Q.; Zheng, Z.; He, N.; Gui, S. Development of a Thermosensitive In-Situ Gel Formulations of Vancomycin Hydrochloride: Design, Preparation, in Vitro and in Vivo Evaluation. J. Pharm. Sci. 2022, 9, 2552–2561. [Google Scholar] [CrossRef] [PubMed]
- Walfish, S. A Statistical Perspective on the ICH Q2A and Q2B Guidelines for Validation of Analytical Methods. Bio. Pharm. Int. 2006, 19, 28–36. [Google Scholar]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Compounds | F1 | F2 | F3 | F4 | F5 | F6 |
|---|---|---|---|---|---|---|
| Metronidazole (%w/v) | 1 | 1 | 1 | 1 | 1 | 1 |
| Gellan Gum (%w/v) | 0.1 | 0.2 | 0.3 | 0.1 | 0.2 | 0.3 |
| Chitosan (%w/v) | 0.1 | 0.1 | 0.1 | 0.2 | 0.2 | 0.2 |
| Distilled water to | 100 | 100 | 100 | 100 | 100 | 100 |
| Formula | Gel Flakes (Equal to Pure Metronidazole) | PF-127 | PF-68 | Sodium Alginate |
|---|---|---|---|---|
| G1 | 1 | 20.00 | - | - |
| G2 | 1 | 17.50 | 2.50 | - |
| G3 | 1 | 15.00 | 5.00 | - |
| G4 | 1 | 12.50 | 7.50 | - |
| G5 | 1 | 10.00 | 10.00 | - |
| G6 | 1 | 15.00 | 5.00 | 0.20 |
| G7 | 1 | 15.00 | 5.00 | 0.40 |
| G8 | 1 | 15.00 | 5.00 | 0.60 |
| Formulation | EE (%) | DL (%) |
|---|---|---|
| F1 | 77.67 ± 3.43 | 79.52 ± 2.65 |
| F2 | 79.43 ± 2.12 | 72.59 ± 3.09 |
| F3 | 84.32 ± 2.61 | 67.82 ± 2.42 |
| F4 | 90.65 ± 2.34 | 75.13 ± 3.19 |
| F5 | 98.91 ± 3.43 | 74.20 ± 3.98 |
| F6 | 99.47 ± 2.98 | 66.55 ± 4.51 |
| Tsol-gel (Without Dilution) | Tsol-gel (With Dilution) | |
|---|---|---|
| G1 | 23.43 ± 2.32 | 23.91 ± 2.43 |
| G2 | 29.54 ± 2.71 | 30.87 ± 3.01 |
| G3 | 36.87 ± 3.43 | 37.43 ± 3.14 |
| G4 | 40.54 ± 4.02 | 42.32 ± 4.90 |
| G5 | 43.52 ± 4.11 | 45.41 ± 3.87 |
| G6 | 36.98 ± 3.12 | 37.94 ± 2.87 |
| G7 | 37.01 ± 3.03 | 37.98 ± 3.21 |
| G8 | 46.76 ± 3.18 | 47.65 ± 4.09 |
| Mucoadhesion Strength (dyne·cm2) | Mucoadhesion Time (h) | |
|---|---|---|
| G1 | 28.32 ± 2.31 | 3.98 ± 0.32 |
| G2 | 23.31 ± 1.98 | 3.18 ± 0.28 |
| G3 | 18.23 ± 0.93 | 2.81 ± 0.43 |
| G4 | 16.21 ± 1.87 | 2.19 ± 0.19 |
| G5 | 11.23 ± 1.02 | 2.01 ± 0.21 |
| G6 | 29.43 ± 2.32 | 6.53 ± 0.51 |
| G7 | 42.31 ± 3.82 | 8.62 ± 0.72 |
| G8 | 45.64 ± 4.01 | 8.91 ± 0.82 |
| pH | Drug Content | |
|---|---|---|
| G1 | 5.15 ± 0.39 | 98.32 ± 0.43 |
| G2 | 5.21 ± 0.41 | 97.76 ± 0.32 |
| G3 | 5.19 ± 0.54 | 98.43 ± 0.44 |
| G4 | 5.43 ± 0.33 | 98.31 ± 0.63 |
| G5 | 5.28 ± 0.13 | 99.01 ± 0.43 |
| G6 | 5.34 ± 0.34 | 98.21 ± 0.23 |
| G7 | 5.28 ± 0.27 | 99.34 ± 0.53 |
| G8 | 5.19 ± 0.32 | 99.63 ± 0.65 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Permana, A.D.; Asri, R.M.; Amir, M.N.; Himawan, A.; Arjuna, A.; Juniarti, N.; Utami, R.N.; Mardikasari, S.A. Development of Thermoresponsive Hydrogels with Mucoadhesion Properties Loaded with Metronidazole Gel-Flakes for Improved Bacterial Vaginosis Treatment. Pharmaceutics 2023, 15, 1529. https://doi.org/10.3390/pharmaceutics15051529
Permana AD, Asri RM, Amir MN, Himawan A, Arjuna A, Juniarti N, Utami RN, Mardikasari SA. Development of Thermoresponsive Hydrogels with Mucoadhesion Properties Loaded with Metronidazole Gel-Flakes for Improved Bacterial Vaginosis Treatment. Pharmaceutics. 2023; 15(5):1529. https://doi.org/10.3390/pharmaceutics15051529
Chicago/Turabian StylePermana, Andi Dian, Rangga Meidianto Asri, Muhammad Nur Amir, Achmad Himawan, Andi Arjuna, Nana Juniarti, Rifka Nurul Utami, and Sandra Aulia Mardikasari. 2023. "Development of Thermoresponsive Hydrogels with Mucoadhesion Properties Loaded with Metronidazole Gel-Flakes for Improved Bacterial Vaginosis Treatment" Pharmaceutics 15, no. 5: 1529. https://doi.org/10.3390/pharmaceutics15051529